
Abstract
Background:
The tibial tubercle–trochlear groove (TT-TG) distance is a known risk factor for patellar instability, but its role in anterior cruciate ligament (ACL) deficiency is unclear. Previous studies found an increased TT-TG distance in patients with noncontact ACL tears compared with patients with intact ACLs.
Hypothesis:
The authors hypothesize that there will be a significantly increased TT-TG distance in patients with ACL injury compared with patients without ACL injury.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
All patients aged 18 to 50 years who had noncontact ACL tears between 2020 and 2021 were included in this study. Patients with ACL tears were compared with a similar cohort of patients with meniscal tears, matched for age and sex, between 2020 and 2021. Patients were excluded if preoperative magnetic resonance imaging (MRI) was unavailable. One author reviewed axial images to measure TT-TG distance. An independent 1-tailed t test was used to assess for a difference in TT-TG distance between patients with and without ACL injury.
Results:
The TT-TG distance was measured for 299 patients, of whom 159 had an ACL injury and 140 patients had intact ACLs. Patients with an ACL injury had a mean TT-TG distance of 11.3 ± 4.10 mm, and patients without ACL injury had a mean TT-TG distance of 11.9 ± 4.62 mm. There was no significant difference in TT-TG distance between the 2 groups (P = .246). The sample of patients in both groups had no significant differences in age, sex, or laterality of injury.
Conclusion:
No statistically significant difference in TT-TG distance was found between patients with and without ACL injury. The findings of this study do not support an association between TT-TG distance and ACL deficiency. Instead, TT-TG distance may vary as a result of ACL injury due to increased laxity in tibial external rotation.
Anterior cruciate ligament (ACL) tears are one of the most common injuries seen by orthopaedic surgeons, especially in young, active patients who take part in recreational and competitive sports. 8 The ACL has an integral role in providing rotational stability and preventing excessive anterior translation of the tibia in any activity. 15 Given its prevalence, research has focused on determining risk factors for ACL injury and strategies to improve outcomes after ACL reconstruction surgery.1,2 Previously identified risk factors for ACL injury include female sex, younger age, hyperlaxity, participation in soccer, history of contralateral ACL injury, and knee valgus.7,8,12,14 However, more risk factors are being investigated to better understand modifiable risk factors for ACL injury or graft failure after reconstruction surgery. More research analyzing risk factors and concomitant procedures performed during ACL reconstruction or revision will ultimately help prevent graft failure and provide better care.
The tibial tubercle–trochlear groove (TT-TG) distance, defined as the distance between the center of the trochlear groove and the center of the tibial tubercle, measured on an axial magnetic resonance imaging (MRI) or computed tomography (CT), has been identified as a risk factor for patellofemoral instability.3,6 However, its role as a risk factor for sustaining an ACL tear remains unclear. Previous studies have investigated the relationship between TT-TG distance and ACL tears, with some finding an increased TT-TG distance in knees with ACL tears compared with ACL-intact knees.16,17 TT-TG distance is primarily affected by the knee rotation angle and tibial tubercle lateralization, which is defined as how far laterally the tibial tubercle is positioned relative to the trochlear groove. 10
Increased TT-TG distance has been associated with increased rotational laxity, which can place a greater stress on the ACL, and has been associated with worse outcomes after ACL reconstruction. 16 This gives rise to questions of whether TT-TG distance is a risk factor for ACL injury and whether any concomitant procedures during ACL reconstruction, such as lateral extra-articular tenodesis, should be performed in select patients to prevent graft failure. Lateral extra-articular tenodesis can address rotational laxity in the setting of ACL reconstruction by significantly reducing anterior tibial translation and anterolateral rotary instability, in addition to reducing the force experienced by the graft when an anteriorly directed load is applied. 4
The purpose of this study is to compare the preoperative TT-TG distance between patients with confirmed ACL tears and patients without ACL tears to determine if there is a difference between the 2 groups.
Methods
Institutional review board approval was obtained (Thomas Jefferson University, study #21E.511) to perform the retrospective study. A query for patients with ACL tears between 2020 and 2021 was conducted using the International Classification of Diseases, 10th Revision (ICD-10) codes for ACL tear (S83.511 and S83.512). All patients aged 18 to 50 years who had acute ACL tears between 2020 and 2021 and had available preoperative MRIs in the institution's Picture Archiving and Communications System (PACS) were included in this study. Patients with ACL tears were matched based on age, sex, body mass index (BMI), and date of surgery to a cohort of patients aged 18 to 50 years with meniscal tears, identified using ICD-10 codes S83.231, S83.221, S83.232, or S83.222, between 2020 and 2021. Those who sustained an ACL tear were compared with the control group, which included those who sustained a meniscal tear. Patients with meniscal tears were included if they also had a preoperative MRI available in the institution's PACS software. Patients were excluded if no preoperative MRI was available or if the MRI was of such poor quality that TT-TG could not be reliably calculated.
MRI was taken with the patient supine and the knee positioned in slight flexion within the knee coil. TT-TG distance was measured from the center of the trochlear groove to the tibial tubercle on axial images, as described by Brady et al 5 and Erickson et al 9 (Figure 1). One author (A.J.C.), neutral to the study question and blinded to the study purpose and the patient's injury, reviewed the available axial images to measure TT-TG distance. Knee flexion angle (KFA) was also determined to assess whether it influenced TT-TG distance. KFA was measured using the method described by Summers et al, 18 where the slice with the greatest patellar height in view was identified. The nearest available image where the anterior and posterior cortices of the distal femur and proximal tibia was used. The angle was measured using the lines from the anterior cortices of the distal femur and proximal tibia. 19

The tibial tubercle–trochlear groove (TT-TG) distance was measured on magnetic resonance imaging. The axial slice with the most proximal view of the complete trochlear cartilage was used. A line was drawn from the deepest aspect of the trochlear groove perpendicular to the posterior femoral condylar line. The tibial tubercle (A) was measured at the most distal insertion of the patellar tendon, and a parallel line was drawn. The horizontal distance between the 2 lines was measured to calculate TT-TG distance (B).
Statistics
Categorical descriptive statistics were reported as number (%), and continuous descriptive statistics were reported as mean ± standard deviation or mean (range). A Shapiro-Wilk test was performed to confirm that parametric statistical analysis was appropriate. An independent 1-tailed t test was used to assess for a difference in TT-TG distance between patients with and without an ACL injury. Independent 1-tailed t tests were also used to assess for differences in age and knee flexion angle between patients with and without an ACL injury. Chi-square tests were used to assess for differences in sex and laterality between patients with and without an ACL injury. Two bivariate linear correlations were performed, one with age as the independent variable and the other with KFA as the independent variable, while both used TT-TG distance as the dependent variable. P values less than .05 were deemed significant.
Results
A total of 159 patients with an ACL tear met the inclusion criteria and were compared with a similar cohort of 140 patients without an ACL injury, matched for age and sex. All patients had preoperative MRI available, and TT-TG distance was measured for 299 patients. The mean age of the population studied was 31.3 ± 9.6 years; 57.2% were male (n = 171). There were no significant differences in age (P = .25), sex (P = .89), or laterality (P = .99) between patients with an ACL injury and patients without an ACL injury (Table 1).
Patient Characteristics and Preoperative TT-TG Distance a

Data are presented as mean (standard deviation) unless otherwise noted. ACL, anterior cruciate ligament; KFA, knee flexion angle; TT-TG, tibial tubercle–trochlear groove.
Patients with an ACL injury had a mean TT-TG distance of 11.3 ± 4.10 mm, and patients without an ACL injury had a mean TT-TG distance of 11.9 ± 4.62 mm (Table 1). There was no significant difference in TT-TG distance between the 2 groups (P = .246). Patients with an ACL injury had a mean KFA of 22.7°± 7.47°, and patients without injury had a mean KFA of 23.4°± 7.23°. There was no significant difference in KFA between patients with and without an ACL injury (P = .066).
There was no significant difference measured in TT-TG distance between male and female patients included in the study (P = .09) (Table 2). For patients with an ACL injury, TT-TG distance did not differ significantly between male and female patients (P = .19). Similarly, for patients without an ACL injury, TT-TG distance did not differ significantly between male and female patients (P = .26).
Preoperative TT-TG Distance by Sex a

Data are presented as mean (standard deviation) unless otherwise noted. ACL, anterior cruciate ligament; TT-TG, tibial tubercle–trochlear groove.
Regression analysis showed no true relationship between the age or KFA and the dependent outcome of preoperative TT-TG distance (Table 3).
Relationship With Tibial Tubercle–Trochlear Groove Distance
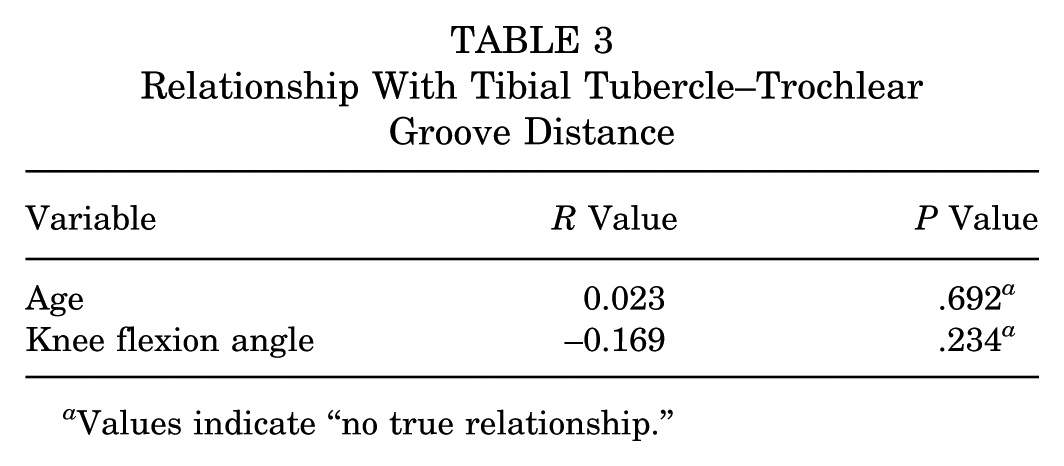
Values indicate “no true relationship.”
Discussion
This study found no significant difference in the mean preoperative TT-TG distance between individuals with and without an ACL injury. The findings of this study do not support an association between ACL injury and TT-TG distance.
The utility of TT-TG distance as a risk factor for ACL injury remains unclear. This study differs from the findings of Saper et al 16 and Shen et al, 17 who found a significant difference in mean preoperative TT-TG distance between patients with and without an ACL injury. Similar to previous studies, there were no differences in age or sex between cohorts with and without an ACL injury. Our study population was older (mean age 29.0 years) than that of Saper et al 16 (mean age 17.4 years) but similar to that of Shen et al 17 (mean age 27.8 years). Both this study and Shen et al 17 found no true relationship between age and TT-TG distance. This study has a larger cohort of patients with (n = 159) and without (n = 140) an ACL injury to compare preoperative TT-TG distances. Despite differences in methodology, the varying results between this study and previous studies demonstrate that there is inconsistent evidence to conclude that preoperative TT-TG distance is a risk factor for ACL injury. Saper et al 16 also acknowledge that while they found a statistically significant difference in mean preoperative TT-TG distance, the clinical significance remains unknown. Future biomechanical studies may help elucidate whether the force experienced by the ACL varies by TT-TG distance and determine whether an increase in tension across the ACL predisposes it to tears when TT-TG distance is increased. Shen et al 17 found a significant difference in preoperative TT-TG distance between patients with and without an ACL injury but alluded to the possibility of it being caused by increased rotational laxity after an ACL injury.
Without MRI evidence comparing TT-TG distance before and after ACL injury, it is not possible to conclude whether TT-TG distance changes as a result of ACL injury. However, a retrospective study by Liu et al 13 provides insight into how TT-TG distance compares between knees with ACL injuries and contralateral knees without an ACL injury in the same patient. Liu et al 17 measured TT-TG distance of ACL-deficient knees preoperatively and postoperatively, as well as contralateral knees. The authors found that the preoperative TT-TG distance in knees with an ACL injury was significantly greater than that in the contralateral knee with an intact ACL. 13 The results further the question of whether elevated TT-TG distance predisposed patients to an ACL injury or whether elevated TT-TG distance is a product of an ACL injury and the TT-TG distance in the contralateral intact knee is normal. The study did recommend double-bundle ACL reconstruction because it restored TT-TG distance to that of the contralateral intact knee and prevented potential patellofemoral cartilage injury. 13
Elevated TT-TG distance in knees with injury can also be explained by increased rotational laxity. Biomechanical studies of the human knee have shown that the ACL is the primary restraint for anterior tibial translation, with a secondary role in resisting internal and external tibial rotation. 18 In those with an ACL-ruptured knee, there would be an increase in anterior translation and valgus rotation of the tibia, along with an increase in lateral tilt and lateral shift of the patella, which would increase TT-TG distance. 11 This study found a mean KFA of 23.4 ± 7.2 within all MRIs reviewed, and this did not differ significantly between patients with and without an ACL injury. A systematic review by Zee et al 20 studied the differences in tibial rotation after ACL reconstruction in human patients and found reductions in tibial internal and external rotation after ACL reconstruction. The results suggest there is increased rotational laxity in ACL-deficient knees, but this has not been quantified compared with healthy knees in the literature.
The findings of this study, as well as those of previously published articles, suggest preoperative TT-TG distance has no association with ACL injury. To determine whether preoperative TT-TG distance is a risk factor for ACL injury, a prospective study would need to be designed where active patients without an ACL injury would need to have available MRI of the knee. This cohort would need to be followed through time, and any patients who develop ACL injuries would need preoperative TT-TG distance measured and compared with the MRI of their previously healthy knee. While this study design would be difficult to execute, the results would define the role of preoperative TT-TG distance as a risk factor or an outcome of ACL injuries. As more research looks to identify risk factors for ACL injury, an emphasis needs to be placed on evaluating the clinical significance of detected associations. In tandem, studies should investigate outcomes after addressing morphologic risk factors in ACL reconstruction surgery to understand whether patients benefit from any concomitant procedures.
Limitations
This study is not without limitations. This single-center retrospective study is limited by the institution's available imaging and preoperative data. This institution consists of multiple facilities, and it is unknown whether MRI protocols and parameters are consistent across all locations, which could affect TT-TG distance measurement. Although the difference in KFA between groups did not achieve statistical significance, there was a trend that may have influenced the comparisons of this study. This study did not include KFA as a variable to control for when preparing a similar cohort or performing an analysis to adjust for KFA as a potential confounder. Additionally, this retrospective study cannot differentiate whether an altered TT-TG is caused by the ACL injury itself or by anatomic variance, such as external tibial rotation deformity, true lateralized position of the tibial tubercle, or trochlear dysplasia. No data were available for patients’ knees before injury or contralateral knees, which could serve as a healthy control group to compare with.
Conclusion
No statistically significant difference in TT-TG distance was found between patients with and without an ACL injury. The findings of this study do not support an association between TT-TG distance and ACL deficiency. Instead, TT-TG distance may vary as a result of ACL injury caused by increased laxity in tibial external rotation.
Footnotes
Final revision submitted August 31, 2025; accepted September 18, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.G.C. has received a grant or contract from Arthrex and DJO LLC and is a board or committee member of the American Orthopaedic Society for Sports Medicine, Major League Baseball Team Physicians Association, and Orthopaedic Learning Center. S.B.C. has received a grant or contract from Arthrex and Slack, has received consulting fees from Conmed and Zimmer, and is a board or committee member of the American Orthopaedic Society for Sports Medicine and the International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine. M.E.B. is a board or committee member of the American Orthopaedic Society for Sports Medicine and an editorial or governing board member of the American Journal of Sports Medicine and the Video Journal of Sports Medicine. B.J.E. has received consulting fees from Arthrex; has received research support from DePuy, A Johnson & Johnson Company, Linvatec, Smith & Nephew, and Stryker; and is a board or committee member of American Academy of Orthopaedic Surgeons, American Orthopaedic Society for Sports Medicine, American Shoulder and Elbow Surgeons, and PLOS. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Thomas Jefferson University (study #21E.511).