
Abstract
Background:
The COVID-19 pandemic significantly disrupted elective orthopaedic sports procedures, including anterior cruciate ligament (ACL) reconstructions, meniscal surgeries, and rotator cuff repairs. These disruptions also extended into athletics, likely resulting in reduced injury rates in athletes leading to decreased surgical volumes.
Hypothesis:
It was hypothesized that the COVID-19 pandemic led to an initial decline in ACL reconstructions, meniscal surgeries, and rotator cuff repairs, with a gradual recovery in surgical volumes during the later pandemic years.
Study Design:
Descriptive epidemiology study.
Methods:
A retrospective analysis of the American College of Surgeons’ National Surgical Quality Improvement Program database was conducted from 2015 to 2022. Patients undergoing ACL reconstruction, knee meniscectomy or repair, knee foreign body removal, and rotator cuff repair were identified using Current Procedural Terminology codes. Surgical volumes and demographics from 2015 to 2019 served as a baseline for comparison with 2020 to 2022 data. Primary outcome was surgical volume change; secondary outcomes included patient demographics and operative-related factors. Chi-square tests were used for categorical variables and Student t tests for numerical variables, with nonparametric corrections and substitutions as needed. Significance was set at P < .05.
Results:
Overall, a total of 200,511 cases (N = 200,511 patients) were identified in our database search. From 2019 to 2020, surgical volume decreased by 25.48%, followed by a 10.32% rebound in 2021 and a 2.17% decrease in 2022. All 2022 volume remained below 2019 levels, except for knee meniscal repair. Postpandemic data showed a 5.66% increase in diabetic patients (P < .001), 14.64% increase in total operative time (P < .001), 71.43% increase in pneumonia incidence (P = .02), and 48.48% increase in inpatient surgeries (P < .001). There was a 21.38% decrease in current smokers (P < .001) and 5.12% decrease in patients with insulin-dependent diabetes (P < .001). No change in hospital length of stay was observed (P = .52).
Conclusion:
The study showed that orthopaedic sports surgery volumes declined in 2020 because of the COVID-19 pandemic and had not fully returned to prepandemic levels by 2022. Surgeries postpandemic were more commonly inpatient, required longer operative times, and involved patients with shifting demographic and comorbidity profiles. Understanding and reporting changes in surgical volume, setting, and patient profiles postpandemic may better prepare surgeons and health care institutions for future resource disruptions or impaired elective surgical capabilities.
Keywords
Orthopaedic sports medicine is a subspecialty of orthopaedic surgery that aims to restore patients to their preinjury functional state with nonsurgical therapies as well as surgical options including anterior cruciate ligament (ACL) reconstructions, meniscal repairs, and rotator cuff repairs. 36 Knee injuries are common in the United States with roughly 250,000 people rupturing their ACL each year and another 850,000 requiring meniscal procedures annually.3,14 Rotator cuff pathology is the most common shoulder condition, and the surgical repair of tears boasts a >90% success rate in many instances. 34 These procedures represent some of the most common surgeries performed by orthopaedic sports medicine physicians. 36
The outbreak of COVID-19 in March 2020 and the need for social distancing disrupted athletic activities, with <40% of surveyed athletes able to continue sport-specific activities in the first few months of the outbreak, likely leading to a decrease in sports-related injuries. 37 In the early stages of the pandemic, surgical volume plummeted, with sports medicine physicians reporting a mean procedural volume decrease to 13.8% and clinic appointments to 17.9% of prepandemic levels along with 1853 fewer pediatric ACL repairs performed in March 2020 than would have been expected.8,20 Another driver of this decreased surgical volume was public apprehension about elective surgical procedures. 28 In May 2020, a survey found that 61% of respondents were concerned with contracting COVID-19 during the encounter and only 27% felt comfortable undergoing an elective procedure within the first month of health systems reopening. 28 This apprehension, along with the suspension of elective surgeries during March of 2020 delayed care for procedures that were deemed nonessential. 6 Phase 1 allowed for the reintroduction of certain elective surgeries in April 2020, but the associated delays resulted in increased pain ratings, analgesic use, and psychosocial stress in orthopaedic patients.4,5
Speculation on the future of sports medicine in the early stages of the pandemic predicted that both surgical and research volume would decrease in the years to come, while others predicted an increase in elective volume due to a backlog of cases and the implementation of COVID-19 monitoring protocols in sports leagues.24,30,38 An initial decline in surgical volume during the early stages of the pandemic has been well reported; however, the effects of the pandemic on case volume in the years after the 2020 COVID-19 pandemic are not widely published. Understanding how surgical volume recovered following the COVID-19 pandemic is useful in preparing for future periods of limited resources or disrupted surgical capabilities. The purpose of this study is to quantify the decrease in orthopaedic sports medicine–focused surgical volume during the early stages of the COVID-19 pandemic, determine if that volume has returned to prepandemic levels, and investigate changes in various patient demographic and case-related factors through 2022. We hypothesize that the COVID-19 pandemic led to a substantial decline in ACL reconstructions, rotator cuff repairs, and knee arthroscopies in 2020, with a gradual recovery of surgical volume to prepandemic levels by 2022.
Methods
Database Information
This was a retrospective observational study utilizing the American College of Surgeons (ACS) National Surgical Quality Improvement Program (NSQIP) database. The NSQIP database includes comprehensive data on patients undergoing surgery at >500 hospitals across the United States. 31 The data are obtained from patients’ medical charts by trained surgical clinical reviewers at each institution during the perioperative period and up to 30 days after the procedure. 19 NSQIP reports interrater reliability disagreements of <2%, and the database has been used to conduct >4600 studies as of 2020.25,33 The NSQIP Participant Use Data File used in the analysis of this study is freely available to staff at participating hospital systems. The number of hospitals collecting NSQIP data increased from 603 to 702 between 2015 and 2022, with small variations year to year. This study was deemed exempt by the Texas Tech Health El Paso institutional review board.
Data Collection
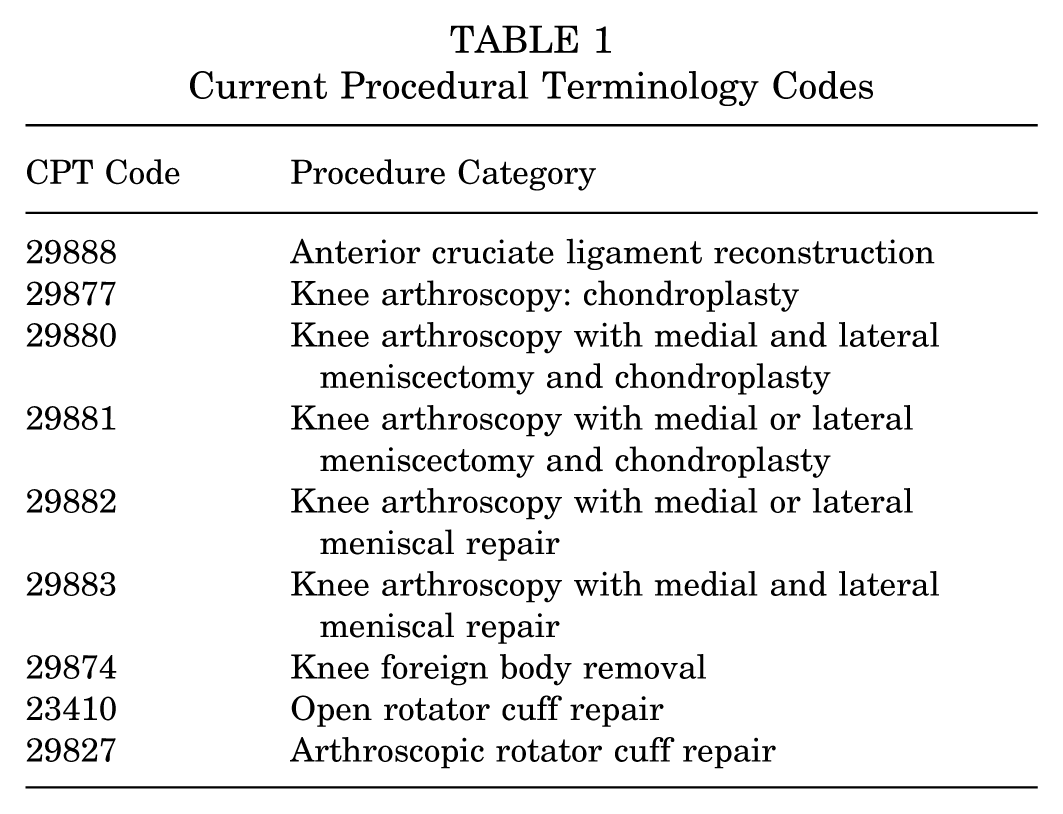
The NSQIP database was retrospectively reviewed from 2015 to 2022 to identify patients by the Current Procedural Terminology (CPT) code(s) corresponding to 6 sports medicine–focused procedures: ACL reconstruction, knee arthroscopy with meniscectomy, knee arthroscopy with chondroplasty, knee foreign body removal, and open or arthroscopic rotator cuff repair. CPT codes are standardized and widely used 5-digit codes to identify and bill for medical procedures. 12 These codes are maintained and updated by the American Medical Association on an annual basis for use by medical providers and billing staff to track and reimburse patient care. 12 The included codes and corresponding procedures are listed in Table 1. Similar procedures were grouped together for analysis. These CPT codes are listed for procedures indicated in patients with both sports-related injuries and degenerative conditions related to chronic activity, both of which would be disrupted by the suspension of elective operations and widespread interruption of organized sports during the COVID-19 pandemic. Patient demographics and multiple operative characteristics were included in the data collection for each case. Patients were included if they were between 18 and 89 years old and underwent one of the collected procedures between January 2015 and December 2022 at an NSQIP participating facility (Figure 1).
Current Procedural Terminology Codes

Flowchart of study cohort selection, stratification, and analysis. ACS, American College of Surgeons; CPT, Current Procedural Terminology; NSQIP, National Surgical Quality Improvement Program. *CPT codes can be found in Table 1.
Statistical Analysis
Surgical volume and demographic means from cases during 2015 to 2019 were used as a baseline with comparative analysis with the 2020 to 2022 cases. More detailed analysis was conducted on a year-by-year basis for multiple associated operative-related variables. The chi-square test was used for categorical variables and the t test was used for numerical variables, with nonparametric corrections and substitutions as needed. The primary outcome is the change in surgical volume from prepandemic to postpandemic time periods. Secondary outcomes include various operative-related factors and patient characteristics. A P value of <.05 was considered significant.
Results
In total, 200,511 cases (N = 200,511 patients) were identified to have undergone one of the included procedures from 2015 to 2022. For these procedures, a 25.48% decrease in overall surgical volume was found from 2019 to 2020 with a rebound of 10.32% in 2021 and a 2.17% decrease in 2022. Overall volume in 2022 is still decreased 19.57% as compared with 2019. Only knee meniscal repairs surpassed prepandemic levels in 2022 with a 16.77% increase. Individual volume data by procedure can be seen in Figure 2 and Table 2.

Stratified case volume by year. ACL, anterior cruciate ligament.
Operative Volume a
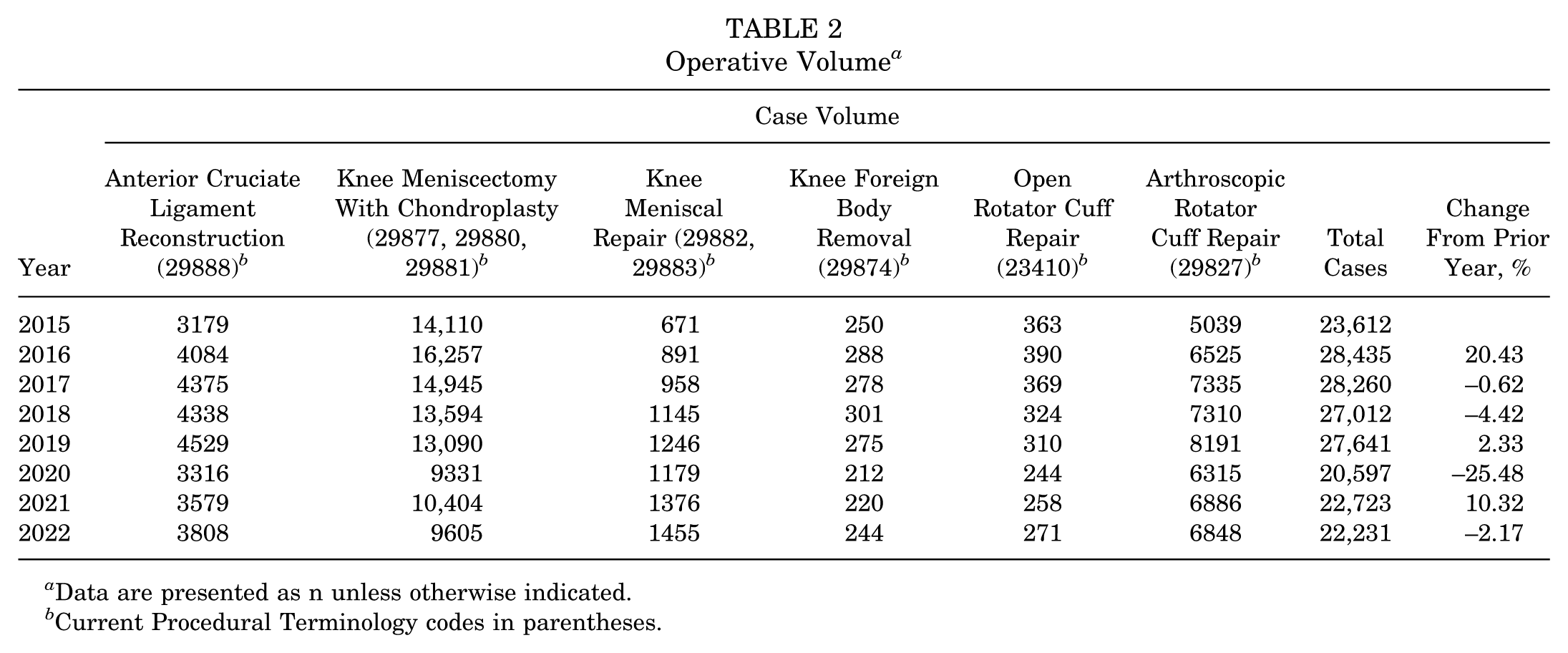
Data are presented as n unless otherwise indicated.
Current Procedural Terminology codes in parentheses.
Demographic characteristics of patients were collected, and the differences were calculated as 2015 to 2019 compared with 2020 to 2022, unless otherwise stated. The proportion of male patients significantly increased from 57.4% to 58.0% (P = .01). Race and ethnicity were calculated as significantly different between the 2 time periods; however, multiple new categories were included in the 2020s, likely confounding the results. Mean patient body mass index (BMI) increased 0.52% from 31.01 to 31.17 (P = .001). A stratification of patients with diabetes was also found to be significantly different, with a 5.66% increase in diabetic patients from 10.6% to 11.2% (P < .001). Within the diabetes group, those on oral medication increased 10.48% and those requiring insulin decreased 5.12% (P < .001). The proportion of patients smoking within the past year was also significantly decreased (21.38%, from 15.39% to 12.1%; P < .001). Demographics of the overall patient sample can be seen in Table 3.
Demographic Data a
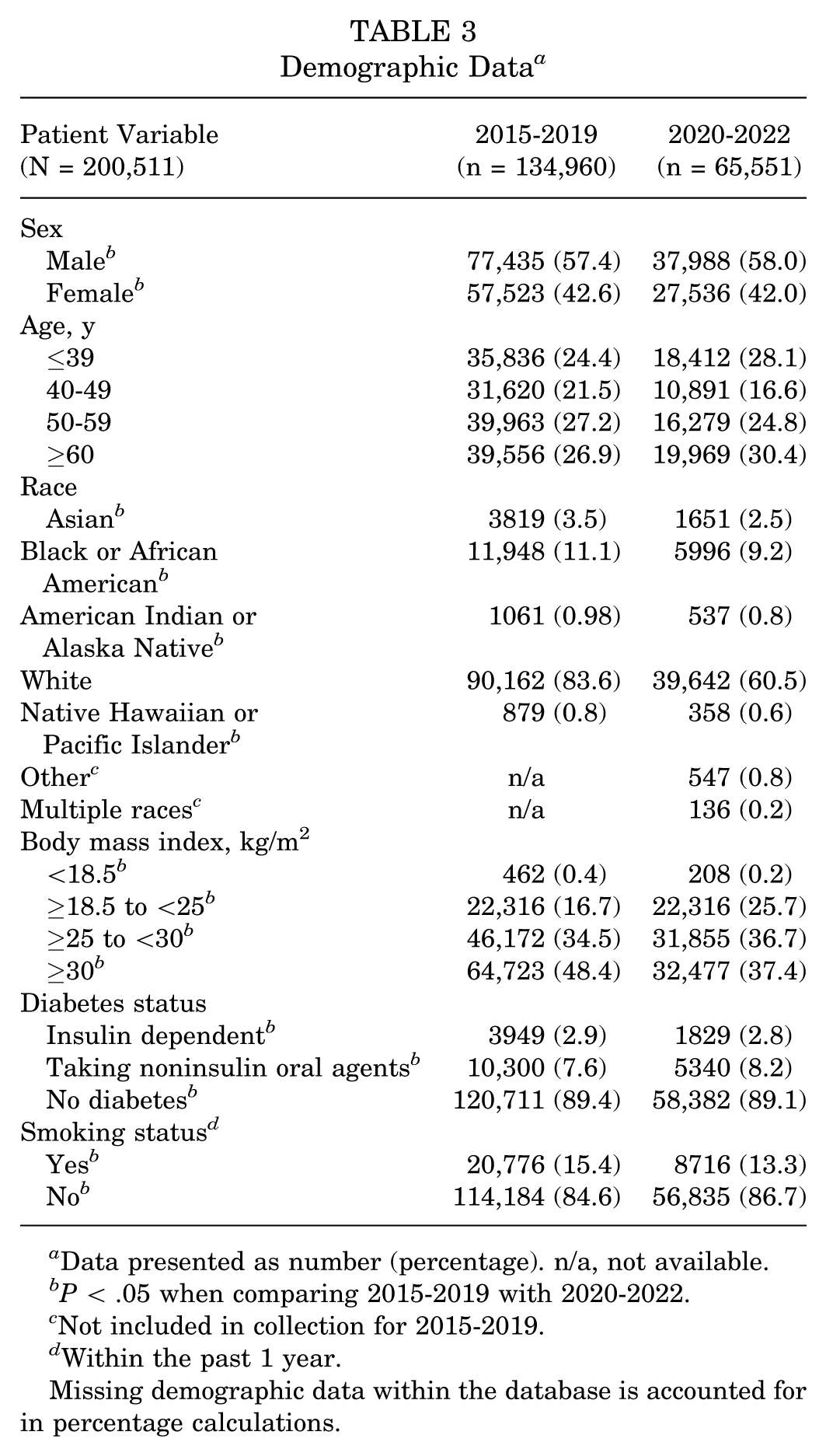
Data presented as number (percentage). n/a, not available.
P < .05 when comparing 2015-2019 with 2020-2022.
Not included in collection for 2015-2019.
Within the past 1 year.
Missing demographic data within the database is accounted for in percentage calculations.
This analysis found significant differences in many operative-related factors when comparing a 2015 to 2019 baseline with 2022. Mean total operative time increased 14.64% from 59.21 minutes to 67.84 minutes in 2022 (P < .001) (Table 4). American Society of Anesthesiology (ASA) scores were analyzed and it was found that scores of 1 and 2 had decreased 3.71% with a corresponding 11.11% increase in scores of 3 and 4 (P < .001). The proportion of surgeries performed in the inpatient setting moved from 3.3% to 4.9% in 2022, a 48.48% increase from prepandemic levels (P < .001) (Table 4). Total hospital length of stay was not found to be statistically different (P = .52).
Operative/Complication Factors a

Data are presented as percentage of N. ASA, American Society of Anesthesiology.
P < .05 when compared with 2015-2019.
P < .05 when compared with 2020.
Percentage within year.
Within 30 days of operation.
Complications and related factors were also found to have changed from prepandemic levels. Pneumonia occurrences after surgery were at 0.07% prepandemic and increased 71.43% to 0.12% in 2022 (P = .02). Preoperative COVID testing was positive in 0.15% of patients in 2021 and increased 53.33% to 0.23% in 2022 (P = .04). Similarly, postoperative COVID testing was positive in 0.44% of patients in 2021 and increased 513.64% to 2.7% in 2022 (P < .001). Operative-related factors and complication data can be found in Tables 4 and 5.
COVID-19 Status a

Data are presented as percentage of N. n/a, not available.
Percentage within year.
P < .05 when compared with 2021.
Discussion
The major findings of our study demonstrated that surgical volume was still 19.57% lower in 2022 than it was in 2019. As compared with the prepandemic cohort, mean BMI increased 0.52%, patients with diabetes increased 5.66%, and patients currently smoking decreased 21.38%. Case-related factors found that the postpandemic procedures took 14.64% longer, ASA scores of 3 and 4 increased 11.11%, and procedures performed in the inpatient setting had a 1.6% absolute increase; however, length of stay was unchanged.
Case Volume
The most significant finding of this study was the persistent reduction in orthopaedic sports medicine surgical volume from prepandemic levels. While the initial decrease from 2019 to 2020 was expected due to COVID-19 restrictions and cancellations of elective procedures as seen in previous studies, the persistent decline in volume through 2022 was more surprising.17,32,35 There are likely a number of contributing factors for this continued decrease in volume. First, the NSQIP database collects data from a shifting number of hospitals each year, creating variability within the sample itself; however, given the large number of institutions and relatively small changes year-over-year, this would not fully explain the decline. It could have been expected for surgical volume to increase, especially in elective surgical fields, following the pandemic as surgeons work to operate on a backlog of delayed cases. 26 One answer could be decreased sports involvement extending after the pandemic: the Aspen Institute found that youth team sports participation decreased 6% between 2019 and 2022, 2 and Doro et al 11 found that 9.7% of young adults reported decreased levels of activity since the pandemic. Decreased sports participation and decreased levels of physical activity would contribute to a decrease in sports-related injuries and their subsequent repairs. Another cause could be increased isolation precautions with patients hesitant to undergo elective operations. 28 While this trend was expected in the short term, it was not expected to persist into 2022, setting the stage for continued monitoring of elective sports case volume moving forward. The single procedure found to increase through 2022 was meniscal repairs; this procedure displayed tremendous year-to-year growth (8.8%-32.7%) before the COVID-19 pandemic, as well as a relatively shallow decline during the pandemic (5.4%) compared with the other cases. Meniscal repairs were increasing in prevalence before the pandemic and their popularity in surgical practices likely continued to increase throughout and after 2020. Although there is a near absence of published work quantifying orthopaedic surgical volume during the pandemic, Ghoshal et al 15 found that overall orthopaedic volume at their institution decreased 72% during the peak of the COVID-19 pandemic and that volume had recovered to 94% of prepandemic levels in 2022. This contradicts our findings and could be related to national database versus single institution sampling.
Demographic Characteristics
Demographic characteristics of the sports surgical patient population also changed during the pandemic. Patients who are current smokers decreased >2% from the 2015-2019 to the 2020-2022 cohorts, which is consistent with previously reported national smoking trends. 27 Another contributing factor could be surgeon or anesthesiologist preference or requirement for smoking cessation in order for patients to undergo elective procedures, especially given the newfound prevalence of COVID-19 in the population. Mean BMI increased between the 2 cohorts by 0.52%, which is also consistent with national trends indicating increasing population BMI in the United States. 22 The increase in BMI could also be expected with decreased physical activity during the pandemic and could possibly be related to increased isolation and lockdown procedures. However, it must be stated that the absolute difference between the 2 cohorts is <1% and will need to be monitored and evaluated over time as this trend is likely not unique to orthopaedic sports medicine patients.
The proportion of patients with diabetes also displayed change between the pre- and postpandemic groups, with the total number of diabetic patients increasing over 5% in 2022. This trend is consistent with literature reporting an increasing prevalence of diabetes in the United States over the past 10 years. 29 While the overall prevalence of diabetic patients increased postpandemic, the number of diabetic patients requiring insulin actually decreased >5%, indicating that the disease in these patients was likely better controlled. This is further supported by an increase of >10% in those on oral diabetic medications. It appears that throughout the pandemic, while also considering the increasing baseline prevalence of diabetes in the population, surgeons were more willing to operate on diabetic patients, with a preference for those on oral medications.
This study found that the proportion of male patients undergoing these procedures significantly increased; however, the absolute increase was only 0.6%. Similar to mean BMI, while this met statistical significance there is a minimal absolute difference. It has been reported that the pandemic disproportionally affected female orthopaedic sports medicine patients regarding time to recovery and pain scores, highlighting the importance of continuing to monitor this trend in the future. 21 Our analysis also found significant differences in the proportions of patient race undergoing the selected procedures; however, given the introduction of new categories in 2020 to 2022 likely skewing the data when comparing with pre-2020 cohorts, it will require more time in the future to analyze trends within these new categories.
Case-Related Characteristics
This analysis also evaluated multiple case-related factors, including finding a nearly 15% increase in total operative time between pre- and postpandemic surgeries. This trend has not been extensively reported in the literature, but Datzmann et al 9 reported a similar increase in total operative and anesthesia time in 2020 that continued through 2022. There are many possible explanations for this trend, including increased isolation precautions during and after the pandemic, which is supported by data in this study finding a significant number of COVID-positive patients. Additionally, these patients could have been of higher complexity given the increased ASA score of patients undergoing these procedures as reported in the current study. Furthermore, the decrease in overall surgical volume for a period of time during the pandemic could have led to a decrease in experienced personnel within the operating theater, further extending operating time; however, this would likely not explain the persistence of this trend into 2022, as elective surgeries returned in late 2020 and 2021. As a final point, the proportion of each surgery during the year could shift the mean total operative time, as certain surgeries such as ACL reconstruction (mean, 89.7 minutes) or rotator cuff repair (mean, 77.7-90.65 minutes) typically require more time than other knee arthroscopies (mean, 30.4-36.5 minutes).1,10,16 Further investigation on a case-by-case basis will likely be required to fully ascertain the underlying factors.
Increased overall ASA scores in this patient population were also of particular interest. Decreased scores of 1 to 2 and increased scores of 3 to 4 in 2022 patients indicates that surgeons were operating on patients who were at higher risk of intraoperative anesthesia complications or who had higher rates of comorbid conditions. 18 This could be related to an increased prevalence of current or past COVID-19 infection or worsening of other preexisting conditions during the pandemic while these patients delayed elective procedures, among a myriad of other potential factors. Further analysis would be required to analyze the differences between these patient cohorts to find the underlying factors contributing to each individual patient's ASA score.
While the vast majority of orthopaedic sports medicine surgeries occur in an outpatient setting, this analysis found that these procedures were increasingly performed in an inpatient setting during the postpandemic time frame through 2022. Given that previous literature has reported that ACL reconstructions in the outpatient setting tend to be preferred by patients and result in decreased total operative time and cost, this postpandemic trend is significant.13,23 As the absolute increase in inpatient surgeries from 2015 through 2019 to 2022 was 1.6% and from 2020 to 2022 it was 0.6%, this could signal a continued shift in operative setting after the pandemic subsided. The data within the NSQIP database only include outpatient procedures collected by facilities that perform both inpatient and outpatient surgeries. This limited our ability to analyze many cases that could have been performed at standalone or privately owned outpatient ambulatory surgical centers (ASCs). Closure or limited capacity of ASCs during and after the pandemic is likely a contributing factor for this trend; however, this is not widely reported in the literature. Surgeon preference to perform surgery in a facility with higher resource availability is also a possible underlying cause, given the probable increase of more complex patients in the postpandemic time period. Again, more analysis will be necessary to investigate the complex resource availability, patient factors, and decision-making process underlying this change.
As would be expected in 2021 to 2022, there was a portion of the patient population with positive COVID-19 tests undergoing these elective procedures. This analysis found that of patients tested, only 0.23% tested COVID-positive in the preoperative setting, which is a 0.08% increase over 2021. While this did reach statistical significance, it is possible that some surgeons and anesthesiologists were more willing to operate on COVID-positive patients. Postoperatively, 0.4% of patients tested positive in 2022, a 0.01% increase over 2021. A probable cause is patients contracting COVID during their operative visit or a lack of testing before surgery. These numbers are likely skewed by the fact that many likely went untested, as this database places patients with negative and unknown test results within the same category, making analysis of this distinction unavailable.
A known postoperative complication of any surgery is pneumonia, which increased 71.43% from a prepandemic level of 0.07% of patients to 0.12% of patients in both 2020 and 2022. 7 While an increase in postoperative pneumonia could be expected due to increased COVID-19 prevalence, the continued increased of pneumonia prevalence into 2022 is striking. This would be supported by the increased postoperative COVID-positive test results also reported in this study. However, it is important to note the overall rates of postoperative pneumonia remain well below 1%, and further investigation would be needed to evaluate if this is related to COVID infection.
There are several effects that these findings have on an orthopaedic surgeon's clinical practice. As we did not find a significant correction in surgical volume, practicing physicians were likely still operating less in 2022 than they were before 2020. Additionally, given that there was a decline from 2021 to 2022, it suggests that these procedures were not on-track to continue increasing steadily into the future. The effects of a persistent decline in practice volume are significant to both institutions and private practices including decreased total reimbursement, reduced operating theater utilization, and lower total clinic visits.
Limitations
This study has limitations. The goal of the study was to analyze and report statistics and trends on a national level, which limited our ability to delve into the underlying factors behind the reported findings. Literature related to these trends was reviewed and included for broader context; however, it is our hope that this study will spur further investigation into these findings. The data included in this study are not all-encompassing and only include data from hospitals participating in the ACS's collection protocol and do not include all portions of the population, which will impart bias in the data. Given the deidentified nature of the data in the NSQIP database, no individual patient analysis was conducted and we did not report volume on a “per-facility” basis to promote generalizability. Further investigation including these characteristics would aid in providing greater insight into the trends reported here. Furthermore, additional analysis as further NSQIP data become available would provide valuable information on the evolution of these trends over time.
Conclusion
Our study showed that orthopaedic sports surgery volumes declined in 2020 due to the COVID-19 pandemic and had not fully returned to prepandemic levels by 2022. Surgeries postpandemic were more commonly inpatient, required longer operative times, and involved patients with shifting demographic and comorbidity profiles. Understanding and reporting changes in surgical volume, setting, and patient profiles postpandemic may better prepare surgeons and health care institutions for future resource disruptions or impaired elective surgical capabilities.
Footnotes
Final revision submitted August 6, 2025; accepted September 18, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: The American College of Surgeons National Surgical Quality Improvement Program and the hospitals participating in the ACS NSQIP are the source of the data used herein; they have not verified and are not responsible for the statistical validity of the data analysis or the conclusions derived by the authors. R.R. has received hospitality payments from Heraeus Medical LLC, KCI USA Inc, Linvatec Corporation, Onkos Surgical Inc, OsteoCentric Technolgies Inc, Stryker Corporation, Ultragenyx Pharmaceutical Inc, Bone Support Inc, Curasan Inc, Zimmer Biomet Holdings Inc, Bioventus LLC, DePuy Synthes Sales Inc, Orthalign Inc, Smith & Nephew, and Integra LifeSciences Corporation; consulting fees from Bone Support Inc and Daiichi Sankyo Inc; and support for education from Zimmer Biomet Holdings Inc. E.C. is a consultant for CTM and has received hospitality payments from Arthrex Inc, Embody Inc, Linvatec Corporation, OsteoCentric Technologies Inc, Rattan and Associates, Stryker Corporation, Orthofix Medical Inc, SI-BONE Inc, Zimmer Biomet Holdings Inc, Sequoia Surgical Inc, Smith & Nephew, Plyant Medical, Terumo BCT Inc, and Sequoia Surgical Inc; support for education from Rattan and Associates, Arthrex Inc, Medical Device Business Services Inc, Sequoia Surgical Inc, and Smith & Nephew; and a grant from Arthrex Inc. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study as it was deemed exempt by the Texas Tech University – El Paso Institutional Review Board.