
Abstract
Background:
The effectiveness of matrix-associated autologous chondrocyte implantation (MACI) in patients with lower limb malalignment remains debatable.
Hypothesis:
Performing MACI in patients with lower limb alignment abnormalities would result in worse postoperative outcomes than in those without alignment abnormalities.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Patients who underwent MACI using autologous cultured cartilage for traumatic chondral defects and osteochondritis dissecans across 3 institutions between February 2014 and August 2022 were reviewed. Osteotomy was recommended for patients with mechanical alignment (MA) <40% and performed on consenting patients. Evaluation included demographic and clinical variables, Lysholm Knee Score (LKS), Knee injury and Osteoarthritis Outcome Score (KOOS), International Cartilage Regeneration & Joint Preservation Society (ICRS) grade from second-look arthroscopy, and postoperative complications.
Results:
Of 96 cases, 39 showed normal alignment and did not require osteotomy, 44 showed varus alignment and underwent corrective osteotomy, and 13 showed varus alignment but declined osteotomy. All groups showed significant improvement in the LKS and KOOS at 2 years (all P < .05). At 1 year, the normal alignment group showed superior LKS (P = .01) and KOOS Activities of Daily Living (ADL) subscale (P = .04) compared with the varus group without osteotomy. The varus group with osteotomy had significantly better LKS (P = .02) and KOOS ADL (P = .04) than the varus group without osteotomy. ICRS grade–based assessments of medial femoral condylar graft sites showed no significant difference between the normal alignment group and varus group with osteotomy (mean, 10.2 vs 10.0; P = .70). However, significantly worse graft-site repair was noted in patients with MA ≥60% (P = .004), although clinical outcomes were not significantly different. Eight complications were reported in the normal alignment group, with 4 each in the varus groups with and without osteotomy.
Conclusion:
In patients with varus alignment, MACI outcomes were improved when osteotomy was performed to shift alignment toward valgus. The corrected varus group demonstrated cartilage repair status and clinical outcomes comparable with those of the normal alignment group.
Large articular cartilage defect repair is influenced by local vasculature and innervation. 16 Autologous cultured chondrocyte implantation (ACI) was first introduced by Brittberg et al in 1987, with long-term outcome data published in 1994. 5 First-generation ACI—termed periosteal ACI (pACI)—involved the injection of chondrocytes expanded by monolayer cultivation into the defect, which was then covered with an autologous periosteal flap harvested from the tibia. Matrix-associated ACI (MACI) was subsequently developed and has been supported by numerous studies reporting mostly favorable outcome.4,6,7,13,25,36,37,42,47 Indeed, a Bayesian network meta-analysis showed that MACI was associated with more favorable clinical outcomes among ACI procedures. 28 The proposed benefits of the MACI procedure include maintenance of chondrocyte phenotype during cultivation, a low risk of cell leakage, and uniform cell distribution during implantation.29,30 Ochi et al34,35 further refined this technique in 2001 35 and developed MACI covered with autologous periosteum (pMACI) by embedding chondrocytes in atelocollagen gel, which were subsequently cultured for 4 weeks, transplanted, and covered with autologous periosteum. In 2013, Japan Tissue Engineering Co Ltd's (J-TEC’s) autologous cultured cartilage (JACC) was approved by the Japanese Ministry of Health, Labor, and Welfare (MHLW) for use in pMACI for the treatment of traumatic cartilage defects or osteochondritis dissecans (OCD) in knee joints (excluding osteoarthritis) with affected areas measuring ≥4 cm2. JACC has demonstrated positive short- and midterm outcomes for treating traumatic cartilage damage; however, factors such as abnormal lower limb alignment, meniscal defects, and joint instability have been linked to poor outcomes after ACI surgery. 26 Moreover, ACI combined with lower limb alignment correction, meniscal reconstruction, and cartilage repair has been termed biological knee reconstruction, with reports of favorable postoperative outcomes. 15 Various factors influencing ACI surgery outcomes are becoming clearer 30 ; for example, postoperative results tend to be poorer when the graft area exceeds 15 cm2.
Previous studies have reported ACI outcomes in patients with lower limb alignment abnormalities, with certain studies suggesting improved outcomes when ACI is combined with high tibial osteotomy (HTO) compared with that when ACI is used alone.9,30 In contrast, other studies found no significant difference in clinical outcomes between HTO alone and HTO combined with ACI. 8 Moreover, specific evidence for MACI in patients with lower limb abnormalities remains lacking.
Therefore, this study aimed to compare the postoperative results of MACI in patients with normal alignment and those with varus alignment and evaluate the advantages of additional osteotomy in patients with varus alignment. We hypothesized that performing osteotomies in patients with varus alignment would improve postoperative outcomes and produce results comparable with those obtained with preoperative normal alignment.
Methods
Participants
Ethical approval for this study was obtained from the ethics committee of Fukuoka University. Informed consent was obtained through an opt-out process on the website. Overall, 111 knees underwent evaluation through re-arthroscopy between 1 and 2 years after JACC transplantation for traumatic cartilage defects or OCD across 3 institutions (Fukuoka University Hospital [n = 52], Fukuoka Sanno Hospital [n = 41], and Fukuoka Rehabilitation Hospital [n = 18]) from February 2014 to August 2022. The principal inclusion criterion was presence of a traumatic cartilage defect or OCD of the knee joint, in which the defect area was ≥4 cm2. Defect size was measured using a ruler after cleaning the cartilage before transplantation. The measured value reported is the sum of the area of each knee. We excluded patients with osteoarthritis, a history of hypersensitivity to antibiotics or animal-derived ingredients, a known history of autoimmune disease, a positive preoperative allergy test for fetal bovine serum and atelocollagen used in the manufacturing process of JACC, or preoperative valgus mechanical axis (MA). Evaluation parameters included age, sex, diagnosis, height, weight, transplant area, and MA measured using plain radiograph (Figure 1). MA measurements were performed within a month before surgery and at the 1-year postoperative follow-up. Clinical scores, including the Lysholm Knee Score (LKS) and Knee injury and Osteoarthritis Outcome Score (KOOS), were assessed by board-certified orthopaedic surgeons (A.M., K.S.) preoperatively and at 1 and 2 years postoperatively. The degree of cartilage repair during second-look arthroscopy was assessed by board-certified orthopaedic surgeons (A.M., K.S.) using the International Cartilage Regeneration & Joint Preservation Society (ICRS) grading system: grade 0 indicates normal cartilage, grade 1 indicates abnormal cartilage, grade 2 indicates partial-thickness cartilage defects, grade 3 indicates full-thickness cartilage defects, and grade 4 indicates damage extending to the bone and cartilage unit. Moreover, postoperative complications such as infection, thrombosis, and limited range of motion were monitored for 2 years.
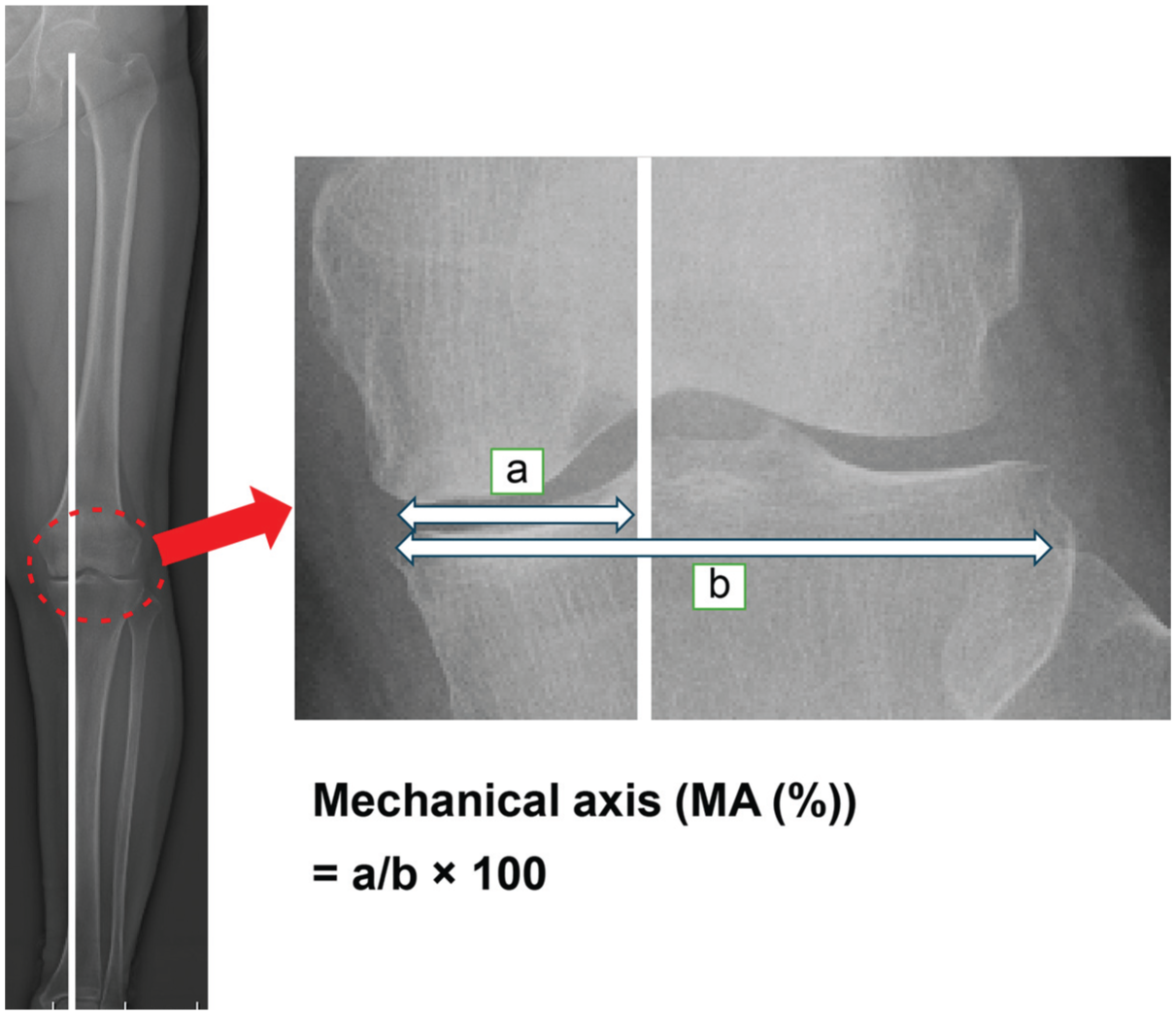
The %MA is calculated as the ratio of the horizontal distance from the medial edge of the tibial plateau to the intersection of the MA. a: Distance from the medial edge of the tibial plateau to the intersection of the MA, b: Distance from the medial edge to the lateral edge of the tibial plateau. The right panel is an enlarged view of the red dotted circle on the left panel.
Surgical Techniques
JACC is approved by the Pharmaceuticals and Medical Devices Agency. Approximately 0.4 g of cartilage tissue was harvested from the nonweightbearing area of the patient's knee during arthroscopic surgery and sent to J-TEC. Cartilage processing was conducted at a cell culture facility that complies with the Good Gene, Cellular and Tissue-based Products Manufacturing Practice established by the MHLW. Cartilage fragments were briefly enzymatically digested, and the isolated chondrocytes were embedded in atelocollagen gel and cultured in 3 dimensions for 4 weeks. After passing strict shipping inspections, JACC was delivered to the hospital under controlled temperature conditions for surgery.
The cartilage defect site was prepared during transplantation by removing any brittle tissue and calcified layer. Any irregularities in the subchondral bone were smoothed using a surgical bur, and degenerated cartilage surrounding the defect was excised to ensure direct contact between the transplanted cultured cartilage and normal articular cartilage. The JACC graft was placed at the defect site and covered with either periosteum or a collagen membrane (ChondroGide; Geistlich Pharma AG), with collagen membranes being used from September 2020 onward. The membrane was sutured to the surrounding normal cartilage at 2-mm intervals using a 6-0 nylon thread and suture anchors (Appendix Figure A1). In the case of multiple-site transplants, the surgery began with the largest area first.
Postoperative Rehabilitation
A lightweight brace was used for postoperative immobilization of the knee for 2 weeks, followed by continuous passive movements, in line with previous studies.34,35,40,41 An exception was made for patellofemoral lesions, where motion was restricted for up to 4 weeks. Partial weightbearing was introduced 3 weeks postoperatively and gradually increased to full muscle training by 8 weeks depending on each individual institution's protocol and other factors such as defect size, defect location, and existence of concomitant procedures.
Concomitant Osteotomy
Osteotomy was recommended for patients with MA measuring <40% and performed only in patients who provided consent. In cases where concomitant osteotomy was performed, a biplanar osteotomy was conducted on the tibia. A locking plate (Tris plate; Olympus Terumo Biomaterials) was used in all the cases. The target postoperative lower extremity alignment was 62%. Follow-up treatment for osteotomy cases adhered to the same protocol as that for cases wherein cultured cartilage transplantation was performed alone.
Statistical Analysis
Paired-samples t tests were employed to compare the LKS and KOOS preoperatively and at 6 months, 1 year, and 2 years postoperatively. Student t tests or Welch t tests were used to analyze patient background variables (age, body mass index, preoperative/postoperative mechanical axis [%MA], graft area, and mean re-arthroscopy period), LKS and KOOS pre- and postoperatively (6 months, 1 year, and 2 years), score changes between groups, and ICRS grade (degree of cartilage repair). Fisher exact test was utilized to compare patient background factors (sex, disease, complications, concomitant surgery, graft site, and number of graft sites) between groups. Pearson correlation coefficient was used to evaluate the relationship between postoperative %MA and ICRS (medial femoral condyle) and between postoperative %MA and LKS and KOOS. Post hoc power analysis confirmed that the sample size was sufficient to detect differences in postoperative ICRS grade with 80% power at a significance level of .05. Given the limited sample size and the number of covariates, a multivariate analysis was not feasible and thus not performed.
Data were imputed using the method of last observation carried forward, and all statistical analyses were performed using EZR Version 1.68, 20 a modified version of R commander with added statistical functions frequently used in biostatistics. Statistical significance was set at P value <.05.
Results
Table 1 presents the patients’ backgrounds, and Table 2 details their concomitant surgeries. In those undergoing concomitant surgeries, 1 (2.6%) of the 39 patients in the group with normal preoperative lower extremity alignment underwent meniscectomy and 3 (7.7%) underwent meniscal suture. In the group of 13 patients with preoperative varus lower limb alignment who did not undergo osteotomy, 1 (7.7%) underwent meniscectomy and 1 (15.4%) underwent meniscal suture. In the group of 44 patients with preoperative varus lower limb alignment who also underwent osteotomy, 12 (27.3%) underwent meniscectomy, 2 (4.5%) underwent meniscal suture, and 1 (2.3%) underwent lateral release.
Patient Background According to Grouping Variables a

Data are presented as either mean ± SD (min-max) or n (%). Bold values indicate was statistically significant. BMI, body mass index; MA, mechanical axis.
Welch t test.
Student t test.
Fisher exact test.
Concomitant Surgeries a
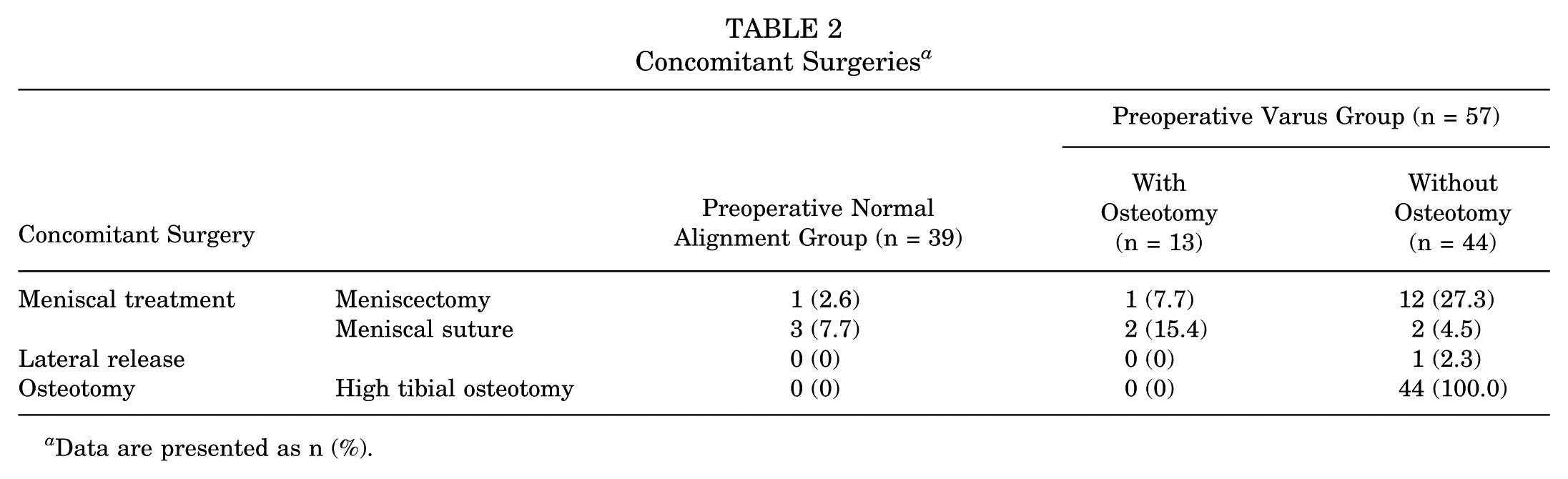
Data are presented as n (%).
MA was categorized as follows: <45% as varus alignment, 45% to 55% as normal alignment, and >55% as valgus alignment. Among 57 patients with varus alignment, 44 (77.2%) underwent osteotomy (Figure 2). A total of 16 postoperative complications were observed (8 in patients with normal alignment, 4 in those without osteotomy, and 4 in those with osteotomy in the varus group). In the normal alignment group, complications included joint contracture (n = 4 of 39; 10.3%), joint effusion (n = 1; 2.6%), quadriceps weakness with delayed (>1 month) recovery (n = 1; 2.6%), keloid (n = 1; 2.6%), and superficial infection (n = 1; 2.6%). In the varus group without osteotomy, osteoarthritis progression (n = 2 of 13; 15.4%), postoperative complications including joint contracture (n = 1; 7.7%), and joint effusion (n = 1; 7.7%) were reported. In the varus group with osteotomy, these complications included joint contracture (n = 2 of 44; 4.5%), quadriceps weakness with delayed (>1 month) recovery (n = 1; 2.3%), and joint effusion (n = 1; 2.3%). Appendix Table A1 and Appendix Figure A2 illustrate the clinical outcomes for all cases, demonstrating significant improvements in all scores at 2 years postoperatively compared with preoperative scores. The degree of repair at the transplant site during the second-look evaluation is summarized in Figure 3 and Table 3.

Overview of the groups analyzed in the current study. ICRS, International Cartilage Regeneration & Joint Preservation Society; Pre-op, preoperative.

International Cartilage Regeneration & Joint Preservation Society cartilage repair grade. The left pie chart shows the distribution of grades according to the number of knees and the right pie chart according to the number of transplanted sites. In cases of multiple-site transplants, the lower score was used.
ICRS Grade at the Second-Look Evaluation a

ICRS, International Cartilage Regeneration & Joint Preservation Society.
In cases of multiple-site transplants, the lower score was used.
Comparisons were made in the LKS and KOOS between 39 patients in the preoperative normal alignment group and 13 patients in the preoperative varus alignment group who did not undergo osteotomy, with the results presented in Appendix Table A2 and Appendix Figures A3 and A4. Compared with the preoperative scores, the preoperative normal alignment group showed improvements in all score items at 2 years postoperatively, whereas the varus group without osteotomy demonstrated improvements in LKS, KOOS Symptoms, Pain, and Quality of Life (QOL) 2 years postoperatively, without improvements in KOOS Activities of Daily Living (ADL) and Sport/Recreation subscale scores. The preoperative normal alignment group had higher LKS at 1 year postoperatively (P = .01) and higher KOOS ADL at 6 months (P = .04) and 1 year postoperatively (P = .04) compared with the varus group without osteotomy. However, no significant differences were observed between the 2 groups (preoperative normal alignment and varus group without osteotomy) in any score items at the 2-year mark (Appendix Table A2).
Furthermore, Appendix Table A3 and Appendix Figures A5 and A6 present a comparison of the LKS and KOOS between the preoperative varus groups with (n = 44 cases) and without (n = 13 cases) osteotomy. Compared with preoperative scores, the varus group without osteotomy exhibited improvements in LKS, and KOOS Symptoms, Pain, and QOL at 2 years postoperatively; however, the KOOS ADL and Sport/Recreation subscale scores did not show improvement. Meanwhile, the varus group with osteotomy demonstrated improvements in all score items at the 2-year follow-up relative to preoperative scores, except for KOOS Sport/Recreation scores (Appendix Table A3). The varus group with osteotomy had higher LKS (P = .02) and KOOS ADL (P = .045) than the varus group without osteotomy at 1 year postoperatively. Nonetheless, no significant differences were observed between the 2 groups in any score items at the 2-year mark (Appendix Table A3).
A comparison of the ICRS grades between the 39 patients in the preoperative normal alignment group and those in the preoperative varus alignment group who did (n = 44) and did not (n = 13) undergo osteotomy is shown in Table 4. No significant differences in ICRS grades for the trochlea were observed when comparing the preoperative normal alignment (9.8 ± 1.5) and varus group without osteotomy (7.5 ± 3.3) or when comparing the varus groups (with vs without osteotomy; 8.3 ± 2.8 vs 7.5 ± 3.3; both P > .05); however, the ICRS grades for the trochlea were significantly higher in the preoperative normal alignment group than in the varus group with osteotomy (9.8 ± 1.5 vs 8.3 ± 2.8; P = .015) (Table 4). The ICRS grades for the medial femoral condyle were significantly higher in both the preoperative normal alignment group (10.2 ± 1.7) and the varus group with osteotomy (10.0 ± 2.2) than in the varus group without osteotomy (6.8 ± 3.7) (P = .009 and P = .013, respectively) (Table 4), indicating a higher degree of cartilage repair in the normal and osteotomy group. No significant difference was noted in the ICRS grades between the preoperative normal alignment and varus group with osteotomy (P > .05).
ICRS Grade at Second-Look Evaluation Between the Normal and Varus (with and without osteotomy) Groups a

ICRS, International Cartilage Regeneration & Joint Preservation Society. Bold values indicate was statistically significant.
Welch t test.
Appendix Figures A7 and A8 illustrate the results of the analysis examining correlations among clinical outcomes 2 years postoperatively, the degree of repair of the graft site (medial femoral condyle), and postoperative lower limb alignment (%MA) in 44 patients from the osteotomy group who underwent osteotomy after preoperative varus alignment to achieve valgus alignment. A weak negative correlation was found between the LKS 2 years postoperatively and postoperative %MA (r = −0.35; P = .044). Additionally, a negative correlation was observed between postoperative %MA and the degree of repair at the graft site (medial femoral condyle) (r = −0.43; P = .009). Correlations were noted between alignment and ICRS grades and clinical scores after %MA reached 60%. Comparisons of the 2 groups at 2.5% increments beyond the postoperative %MA of 60% revealed a significant difference in the degree of repair of the graft site (medial femoral condyle) at %MA of 65%; nevertheless, no significant differences were observed in clinical outcomes (Appendix Table A4). No changes in the MA were observed during the study follow-up period.
Discussion
In this study, we assessed the effectiveness of MACI in patients with lower limb alignment abnormalities. A notable finding of this study is that performing osteotomy to correct lower limb alignment to valgus resulted in a better degree of MACI cartilage repair in cases of varus alignment than in cases of maintained varus alignment without osteotomy. Moreover, in cases where osteotomy was performed and the alignment was adjusted to valgus, the degree of repair and clinical outcomes of MACI on the medial femoral condyle declined as the alignment became more valgus. Notably, the degree of cartilage repair decreased once the %MA reached the threshold of 65%.
Importantly, this effect appears to be lesion specific. Osteotomy in varus knees primarily benefits medial-sided lesions. For example, in our study, trochlear lesions showed significantly worse outcomes in the varus group with osteotomy than in the normal alignment group (Table 4) (P = .015). This difference could be attributed to increased pressure on the patellofemoral joint after valgus-producing osteotomy.
ACI is recognized as an effective treatment for articular cartilage defects; however, various factors influencing postoperative outcomes have been identified.3,18,33,43,45 Niemeyer et al 32 indicated favorable clinical outcomes in young patients, those with lateral lesions, and those with smaller lesions. Additionally, a systematic review by Goyal et al 14 highlighted that patient age and lower limb alignment were related to postoperative outcomes.
Postoperative alignment of the lower limb after high tibial osteotomy for knee osteoarthritis has been recommended to be set at a tibial plateau width of 62% to 66%, with a valgus alignment of 3° to 5°.10,12 However, recent studies proposed that alignment should be tailored according to the degree of cartilage defect.17,27 An ongoing debate remains regarding the relationship between postoperative lower limb alignment and the degree of cartilage repair, with certain studies indicating a correlation2,46 while others reporting no such correlation.19,22,23
Several reports have addressed postoperative lower limb alignment when HTO is performed with cartilage regeneration surgery, particularly in the context of medial-sided lesions in varus knees. Kim et al 24 demonstrated favorable clinical outcomes when the postoperative %MA was set at 50% to 55% (neutral alignment or valgus <3°). Correcting alignment and alleviating intra-articular pressure are crucial to achieving optimal outcomes after ACI, and evidence suggests that combining these procedures with osteotomies such as HTO may enhance treatment results. Ackermann et al 1 compared the clinical outcomes of a group with postoperative lower limb alignment set to %MA 50% to 55% and that with the conventional setting of %MA 62% to 66% among 66 cases of HTO combined with ACI. Both groups demonstrated significant improvements in postoperative functional scores and pain visual analog scale scores, with no significant differences between them. However, the reoperation rate and correct placement rate appeared to be more favorable with neutral alignment compared with valgus alignment.
Weishorn et al 44 evaluated the influence of lower limb alignment on the long-term clinical outcomes of MACI, indicating that an alignment range from −2.5° valgus to 4° varus is optimal for medial femoral condylar defects. Patients achieving alignment within this range reported high rates of satisfaction (evaluated through the Patient Acceptable Symptom State) and demonstrated favorable KOOS and magnetic resonance observation of cartilage repair tissue scores. Weishorn et al 44 noted that excessive correction should be avoided, emphasizing the importance of aiming for neutral to slight overcorrection. Careful consideration of the optimal lower limb alignment for each patient is crucial in ACI treatment, with corrective surgery performed when necessary. 39 Our study findings provide insights to this discussion by revealing that the degree of repair and clinical outcomes of ACI implanted on the medial femoral condyle decreased as alignment further shifted toward valgus in cases with valgus alignment. Additionally, cartilage repair status declined once the %MA reached 65%. These findings suggest that maintaining alignment in the neutral to 65% %MA range may yield better cartilage repair outcomes with ACI compared with varus cases or those with %MA of ≥65%.
Another important aspect to consider is the evolution of ACI techniques.5,11,31,38 The JACC used in our study constitutes a second- or third-generation ACI, whereas Kim et al 24 and Ackermann et al 1 evaluated first-generation ACIs. First-generation studies suggested that a neutral alignment was necessary for generating mechanical load on chondrocytes, which promotes cartilage maturation. Applying a biased force in association with the use of first-generation ACI, owing to its nature as a liquid suspension, increased the risk of cell leakage from the defect and uneven cell distribution, raising concerns about the effect on prognosis.29,30 In contrast, JACC utilizes a 3-dimensional culture, rather than a liquid medium, enabling the creation of a moderate mechanical load environment. This design minimizes the effects of biased mechanical loads. Weishorn et al 44 evaluated third-generation ACI, indicating that an alignment range from −2.5° valgus to 4° varus is desirable for optimizing clinical scores and grafted cartilage condition. Our study was distinguished by a direct evaluation of ICRS grading at the second look and a comparison of results with a group that did not undergo osteotomy. Future studies are warranted to assess the optimal alignment for addressing cartilage damage, particularly considering mid- to long-term alignment abnormalities.
The lack of correlation between the ICRS grade and clinical outcomes observed in our study is likely reflective of the observation from previous studies that cartilage regeneration after high tibial osteotomy is not correlated with clinical outcomes at 2 years after surgery.19,22,23 However, a more recently published report has demonstrated a correlation between cartilage regeneration after HTO and clinical outcomes at 3.9 years after surgery, 46 which suggests that clinical outcomes may change with longer term follow-up. Further studies with longer follow-up are required to confirm this.
Limitations
This study has several limitations. First, the small sample size posed a challenge, particularly in the context of the subgroup analyses (comparing normal, varus with osteotomy, and varus without osteotomy groups), which would have increased the risk of a type II statistical error. The sample size along with multiple covariates also prevented the performance of robust multivariate analyses. When comparing the primary endpoint of the study—the LKS scale score—between the varus group without osteotomy and the varus group with osteotomy, a power analysis using G*Power indicated that the required sample size was 52 cases. Despite this, the ICRS variable was adequately powered. Second, 2 types of periosteum were used to secure the JACC. Previous reports have indicated that the degree of cartilage repair may be superior when employing a collagen membrane (ChondroGide), which should be considered when interpreting the results. 21 Third, this study had a relatively short follow-up period of only 2 years, and this may not capture the full advantage of long-term procedures, such as osteotomy, emphasizing the need for further investigation of clinical outcomes with long-term follow-up to assess durability and efficacy over time. Fourth, the inclusion of cases with multiple transplants presents another limitation because the degree of preoperative cartilage damage varied among patients, which may influence outcomes and should accounted for when interpreting the results. Fifth, confounding factors, including the osteotomy type, defect size, presence of meniscal injury, and the use of 2 different materials to cover the transplanted cultured cartilage could have influenced the interpretation of the results of the study. The location of the cartilage defect may have also affected the outcomes after osteotomy; however, this was not investigated in the current study. Sixth, the ICRS graders were not blinded to the osteotomy status of the cases, which may have resulted in biased outcome assessments. Finally, as a retrospective study, the results of this study could have been influenced by observer bias, as the surgeons were aware of previously performed surgeries, and attrition bias, because patients who did not undergo second-look arthroscopy were excluded.
Conclusion
This study demonstrated that cartilage repair after MACI was more successful when an osteotomy was performed to shift alignment toward valgus in patients with varus lower limb alignment compared with that in patients who did not undergo realignment. These findings highlight the importance of achieving optimal mechanical axis during MACI procedures. Future studies should investigate alignment thresholds more precisely and assess long-term outcomes to refine surgical strategies for treating cartilage lesions in malaligned knees.
Supplemental Material
sj-pdf-1-ojs-10.1177_23259671251403094 – Supplemental material for Effect of Lower Limb Alignment and Corrective Osteotomy on Clinical Outcomes After Matrix-Associated Autologous Chondrocyte Implantation for Extensive Cartilage Defects of the Knee
Supplemental material, sj-pdf-1-ojs-10.1177_23259671251403094 for Effect of Lower Limb Alignment and Corrective Osteotomy on Clinical Outcomes After Matrix-Associated Autologous Chondrocyte Implantation for Extensive Cartilage Defects of the Knee by Akira Maeyama, Kazuhiko Saeki, Tetsuro Ishimatsu, Taiki Matsunaga, Shizuhide Nakayama, Junya Hara and Takuaki Yamamoto in Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted August 20, 2025; accepted September 12, 2025.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the ethics committee of Fukuoka University (approval No. H24-07-004).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.