
Abstract
Background:
Acute anterior cruciate ligament (ACL) tears with meniscal injuries elevate posttraumatic osteoarthritis risk. While early ACL reconstruction (ACLR) remains prevalent, emerging evidence suggests that delayed intervention may enhance meniscal preservation.
Purpose:
To quantify location/morphology-specific spontaneous healing trajectories of meniscal tears and establish temporal thresholds for surgical decision-making.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Patients who underwent ACLR at a tertiary academic medical center specializing in sports medicine from January 2020 to December 2023 were included in this study. Demographic profiles and time-to-surgery intervals were extracted from electronic medical records. Patients were stratified by injury-to-surgery interval in detail: 0-1week, 1-2 weeks, 2-3 weeks, 3-4 weeks, 4-6 weeks, 6-8 weeks, 8-12 weeks, 12-16 weeks, 16-20 weeks, and 20-24 weeks. Meniscal tear characteristics were classified via preoperative magnetic resonance imaging (MRI) and intraoperative arthroscopic evaluation (location: anterior horn, body, and posterior horn; morphology: longitudinal, compound, horizontal, and radial). Spontaneous healing of the meniscus was defined as a complete fibrous union observed during arthroscopic evaluation.
Results:
A total of 2723 patients (3562 menisci) were included, including 2493 with lateral meniscal tears and 2001 with medial meniscal (MM) tears. The overall spontaneous healing rate of lateral meniscal (LM) tears is higher than that of MM tears (7.06% vs 1%; P < .001). Additionally, the highest healing rate was observed in longitudinal tears of the LM posterior horn (11.35%). The overall trend of the spontaneous healing rate of meniscal injuries in the setting of ACL tears increased over time during the first 8 to 12 weeks after the injury. The spontaneous healing rate was highest at 12 weeks and subsequently declined thereafter. Comparative analysis demonstrated a significant increase in the healing rate in the 8-12 weeks intervention group versus the delayed groups: the LM healing rate decreased from 15.87% to 9.81% (longitudinal tears: 34.04% vs 17.72%; radial tears: 22.97% vs 7.08%), and the MM rate decreased from 2.65% to 1.36%. Compared with the mean level of early intervention groups (≤8 weeks), the 8-12 weeks group showed >1.5 times increase in healing rates (LM: 15.87% vs 6.29%; longitudinal tears: 34.04% vs 9.83%; radial tears: 22.97% vs 8.65%; MM: 2.65% vs 0.86%).
Conclusion:
Delaying ACLR to 8 to 12 weeks after injury may optimize the potential for spontaneous healing in LM injuries (particularly posterior horn longitudinal and radial tears), potentially increasing meniscal healing rates by 1.5 to 2.5 times compared with early intervention (≤8 weeks). The healing potential of LM tears, particularly posterior horn longitudinal and radial tears, was greater than that of MM tears in this study.
Knee trauma frequently leads to concomitant anterior cruciate ligament tears (ACLT) and meniscal injuries, which have been shown to occur in up to 40.5% of anterior cruciate ligament reconstructions (ACLR). 21 The treatment is often ACLR and concomitant meniscal repairs or partial meniscectomies. While partial meniscectomy remains the most prevalent treatment for meniscal tears, 3 accumulating evidence highlights its association with increased osteoarthritis risk compared with meniscal repair, positioning it as a key predictor of post-ACLR degenerative changes.23,27 This recognition has driven a paradigm shift in clinical practice, leading to a marked increase in meniscal repair rates, particularly among younger patients. 4 While the benefits of meniscal repairs are well known, surgical outcomes remain unsatisfactory, as evidenced by a 10.6% revision rate within 2 years and an overall 19.1% failure rate at 5-year follow-up.4,29
Surgical timing may affect meniscal repair success and joint preservation. Current evidence suggests divergent optimal windows for ACLR and meniscal repair. Early meniscal repair (≤3 weeks after injury) significantly reduces failure rates compared with delayed procedures, 39 whereas delayed ACLR (>6 months after injury) increases risks of secondary meniscal damage and osteoarthritis.9,33,38 However, the benefits of early ACLR and the optimal time frame for ACLR remain a topic of debate. Early studies from the 1990s associated immediate reconstruction with arthrofibrosis and joint stiffness,31,38 although recent investigations report no significant differences in these complications.20,37 Paradoxically, earlier ACLR (particularly ≤3 months) correlates with increased revision risk in multiple cohorts,8,15,32 creating clinical equipoise regarding optimal surgical timing for ACLT patients with concomitant meniscal injuries.
Emerging research has demonstrated that the meniscus harbors endogenous progenitor cells and intrinsic healing potential, suggesting a therapeutic window to delay ACLR and allow spontaneous meniscal healing.10,13,22,25,35 The healing capacity can vary substantially by tear characteristics. Lateral meniscal (LM) injuries, peripheral red-zone tears, and longitudinal tears are associated with higher healing rates due to enhanced vascularity and favorable biomechanical environments.6,14,17,34 This biological heterogeneity underscores the need for meniscal tear-specific temporal frameworks to guide surgical decision-making.
In this study, we characterize the spontaneous healing trajectories of meniscal tears in patients with ACLT. By correlating tear characteristics (location and morphology) with healing outcomes at specific postinjury intervals, we aimed to develop a time-sensitive framework for surgical decision-making in ACLR. We hypothesized that such an approach could potentially reduce unnecessary meniscal procedures while balancing the urgency of ACLR with meniscal preservation.
Methods
Study Population
Patients who underwent ACLR at a tertiary academic medical center specializing in sports medicine from January 2020 to December 2023 were included in this study. The study protocol was approved by the Peking University Third Hospital Medical Science Research Ethics Committee (No. M2024173). The inclusion criteria were as follows: (1) arthroscopically confirmed acute ACLT with concomitant meniscal tear; (2) injury-to-surgery interval ≤6 months; (3) no previous ipsilateral knee surgery or major trauma; and (4) availability of complete clinical/imaging records. The exclusion criteria were as follows: (1) presence of a discoid meniscus; (2) displaced bucket-handle tear; (3) having a multiligament injury; and (4) incomplete surgical documentation to determine meniscal tear characteristics. A total of 2945 patients were identified during the study period that met the inclusion criteria (Figure 1). After applying the exclusion criteria, 2723 patients (1979 men and 744 women) were analyzed, with a mean age of 29.90 ± 10.02 years (range, 12-68 years).

Flowchart of patient inclusion, exclusion, and grouping.
Meniscal Classification and Surgical Timing Stratification
Tear location was defined as anterior horn (anterior third), body (middle third including popliteal hiatus), or posterior horn (posterior third). Morphological types included longitudinal tears, horizontal tears, radial tears (including transverse and oblique tears), and complex tears. 28 In cases where a complex tear was present and composed of the combination of the aforementioned 2 types of tears, the healing situation and corresponding tear types were recorded separately. Patients were stratified into 10 intervals in detail: 0-1week, 1-2 weeks, 2-3 weeks, 3-4 weeks, 4-6 weeks, 6-8 weeks, 8-12 weeks, 12-16 weeks, 16-20 weeks, and 20-24 weeks after injury.
Data Collection
Intraoperative records were reviewed to document tear characteristics and spontaneous healing status. Preoperative magnetic resonance imaging (MRI) was cross-referenced for cases with ambiguous arthroscopic findings. One patient was excluded during analysis due to insufficient documentation.
Statistical Analysis
R version 4.2.1 for macOS (R Foundation for Statistical Computing) and Microsoft Excel version 16.43 (Microsoft Corp) were used for data organization, analysis, and plotting. Categorical variables were compared using the Pearson chi-square test, and the relationship between age and healing rate was assessed using logistic regression analysis. For all statistical analyses, P < .05 was considered statistically significant.
Results
Patient Selection and Meniscal Tear Distribution: An Analytical Overview
A total of 2945 patients initially met the inclusion criteria, of whom 222 were subsequently excluded due to discoid menisci (n = 19), concomitant injuries to other cruciate ligaments (n = 20), incomplete surgical documentation (n = 21), or displaced bucket-handle tears (n = 162). The final analysis included 2723 patients (2729 knees; 3562 menisci), with 2493 LM tears and 2001 medial meniscal (MM) tears (Figure 1). The overall incidence of LM and MM tears was 72% and 58.52% respectively, with 30.52% knees presenting with both LM and MM injuries. Among LM tears, radial tears accounted for 47.93%, followed by complex tears (29.77%), longitudinal tears (27.43%), and horizontal tears (7.79%). In contrast, the majority of MM tears were longitudinal (65.62%), with lower proportions of complex (26.17%), radial (10.27%), and horizontal tears (7.26%).
Spontaneous Healing of Concomitant Meniscal Tears with ACL Injuries
Spontaneous meniscal tear healing rates varied significantly by tear morphology and location. (Tables 1 and 2). For LM tears, longitudinal tears exhibited the highest healing rate (10.72%), followed by radial (6.61%), complex (6.21%), and horizontal tears (1.12%). LM posterior horn tears showed higher healing rates (11.35%) compared with body (2.26%) and anterior horn tears (0.98%). In MM tears, healing rates were substantially lower overall when compared with LM tears (0.10% vs 7.06% for LM; P < .001). MM radial tears exhibited the highest healing rate (1.58%), followed by longitudinal (1.30%) and complex tears (0.39%), with no healing observed in horizontal tears. Similar to LM, MM posterior horn tears showed superior healing (1.36%) compared with the body (0.27%). However, MM anterior horn tears showed an abnormal healing rate (5%), which may be due to the limited sample size (n = 20). Notably, longitudinal tears of the LM posterior horn demonstrated the highest spontaneous healing rates (14.17%).
Spontaneous Healing Rates of Lateral Meniscal Tears With Varying Locations and Morphologies

Spontaneous Healing Rates of Medial Meniscal Tears With Varying Locations and Morphologies

Temporal analysis revealed a dynamic healing trajectory. For concomitant LM tears with ACLT, spontaneous healing rates increased progressively, peaking at 8 to 12 weeks after injury (15.87%), followed by a decline (Figure 2). Posterior horn LM longitudinal tears reached a maximum healing rate of 34.04% at 8 to 12 weeks before decreasing (Figure 3), while posterior horn LM radial tears peaked at 22.97% but declined more rapidly (Figure 4). MM tears showed a similar temporal pattern but with substantially lower healing rates at all time points (peak 2.65% at 8-12 weeks, Figure 5).

The spontaneous healing trajectory of LM tears combined with ACLR. ACLR, anterior cruciate ligament reconstruction; LM, lateral meniscal.

The spontaneous healing trajectory of LM longitudinal tears combined with ACLR. ACLR, anterior cruciate ligament reconstruction; LM, lateral meniscal.
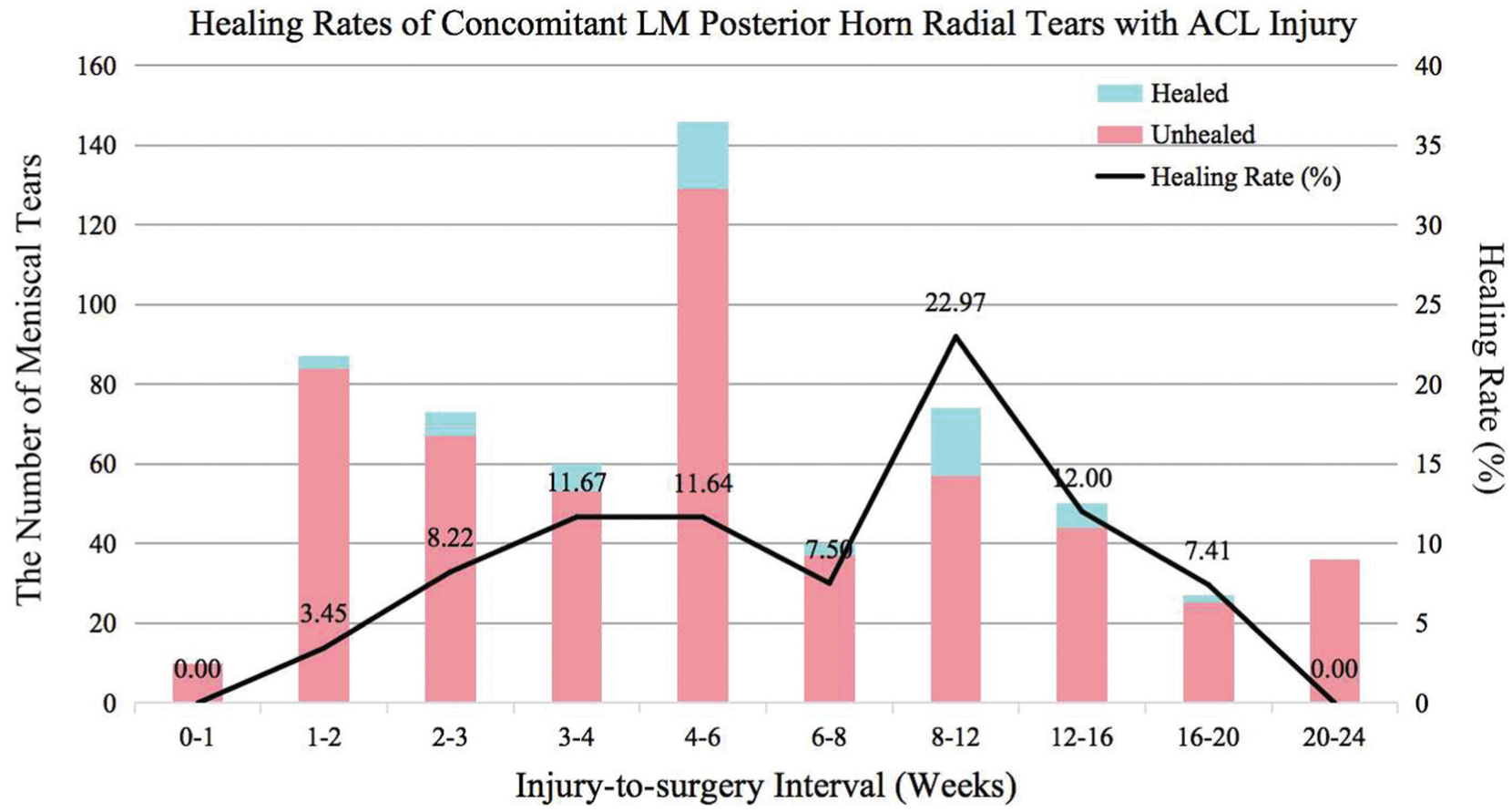
The spontaneous healing trajectory of LM radial tears combined with ACLR. ACLR, anterior cruciate ligament reconstruction; LM, lateral meniscal.

The spontaneous healing trajectory of MM longitudinal tears combined with ACLR. ACLR, anterior cruciate ligament reconstruction; MM, medial meniscal.
Comparative analysis demonstrated significantly higher spontaneous meniscus healing rates in the 8-12 weeks ACLR after injury window versus more delayed ACL injury groups. The LM healing rate decreased from 15.87% to 9.81% (longitudinal tears: 34.04% vs 17.72%; radial tears: 22.97% vs 7.08%), and MM rates from 2.65% to 1.36%. Compared with the mean level of early intervention groups (≤8 weeks), the 8-12 weeks group showed a 1.5-to-2.5-fold increase in healing rates (LM: 15.87% vs 6.29%; longitudinal tears: 34.04% vs 9.83%; radial tears: 22.97% vs 8.65%; MM: 2.65% vs 0.86%).
Discussion
This study provides a comprehensive analysis of spontaneous meniscal healing in patients with ACLT and concomitant meniscal tears. We identified a therapeutic window for spontaneous healing, with initial healing observed as early as 1 to 2 weeks after injury, peaking at 8 to 12 weeks. Notably, healing rates declined significantly when surgery was delayed beyond 3 months. This may be attributable to the effects of prolonged recurrent knee instability on meniscal injury and healing.
Surgical Timing Dilemma
The timing of surgery for acute ACLT remains controversial. Early ACLR offers distinct advantages, including enhanced motor function, earlier return to sports, and reduced risk of secondary meniscus and cartilage injuries.9,33 However, our findings reveal that surgical intervention within the first 2 weeks after injury may be counterproductive, as it may not allow sufficient time for spontaneous healing of meniscal tears. This premature intervention may increase the likelihood of requiring concomitant meniscal procedures during surgery (eg, meniscectomies and meniscal repairs), leading to a higher risk of surgical complications and costs. 18 Additionally, early surgery has been associated with an increased risk of revision in several studies, highlighting the need to carefully balance the urgency of ligament stabilization against the potential for meniscal preservation 8,15,32
Meniscal Tear Characteristics and Healing Capacity
The healing capacity of meniscal tears has been shown to depend on tear location and morphology. In the present study, LM tears demonstrated a 7-fold higher healing rate than MM tears (7.06% vs 1%), findings that have also been reported in other clinical studies and supported by finite-element analysis.2,5,16 Posterior horn tears also showed preferential healing (11.35% vs 2.26% for body tears). This may be facilitated by compressive loading during flexion and enhanced vascular perfusion.7,16,17 In contrast, body tears near the popliteal hiatus exhibited minimal healing, which may reflect their avascular microenvironment and susceptibility to recurrent shear forces.11,19
Longitudinal tears demonstrated superior healing rates compared with horizontal and complex tear patterns, suggesting greater biomechanical stability under axial loading.16,24,26 The axial knee loads are transferred into hoop stresses via Poisson effects, resulting in significant tensile strains, which were found to be less affected in the case of longitudinal meniscal tears, allowing the torn meniscus to remain pressed together during knee flexion.16,24,26 Radial tears, including transverse and parrot-beak variants, exhibited intermediate healing potential (22.97% at 8-12 weeks), which declined precipitously beyond this window (7.08% after 3 months). Among the various classifications of meniscal tears, those designated as horizontal tears of the menisci exhibit particularly low rates of spontaneous healing. 1
Both longitudinal and radial tears achieved maximal healing at 2 to 3 months after the ACL injury despite differing biomechanical environments. However, spontaneous radial tear-healing rates declined precipitously beyond the 2- to 3-month window. While the precise mechanism remains to be fully elucidated, this precipitous decline suggests a time-limited biologic window for effective spontaneous healing of radial tears. This finding underscores the potential importance of addressing radial tear patterns within a ≤3-month window after ACL injury to align with the body's innate healing capacity.
These findings collectively advance our understanding of meniscal pathobiology after ACLT and advocate for a stratified surgical timing protocol: longitudinal tears may be observed for up to 3 months to permit spontaneous healing, while radial/compound tears require intervention within this window. Given the established high failure rates of surgical repair for bucket-handle and horizontal tears—a finding now explained by our demonstration of their negligible intrinsic healing capacity—early surgical management is strongly indicated.12,30 Clinicians must balance the biomechanical urgency of ACLR against the biological potential for meniscal preservation, particularly for lateral and posterior horn injuries. This paradigm shift toward morphology-stratified, time-sensitive management protocols may improve long-term meniscal preservation and, therefore, joint outcomes in ACLT patients.
Limitations and Future Outlook
Several limitations of this study must be acknowledged. As a retrospective cohort, our findings are inherently susceptible to selection and interpretation bias despite rigorous inclusion criteria. Key confounders such as patient activity levels, rehabilitation protocols, surgeon experience, and adjunctive therapies (eg, bracing, nonsteroidal anti-inflammatory drugs) could not be controlled due to limitations in registry data collection. Furthermore, intraoperative meniscal evaluations during ACLR were not blinded to injury-to-surgery intervals, as this information was documented in surgical records. The relative rarity of anterior horn tears (<5% incidence) limited statistical power for this subgroup analysis, necessitating cautious interpretation of associated healing rates. Further studies are required to clarify the spontaneous healing of anterior horn tears or specific tear morphological subtypes occurring in the anterior horn. Our classification system, combining oblique radial, parrot-beak, and transverse tears under a single radial category, while clinically pragmatic, may obscure subtle biomechanical differences between these subtypes. Additionally, while some complex meniscal tears, such as T-shape tears or horizontal tears combined with healed longitudinal tears, were well-documented in surgical records, other records lacked sufficient detail regarding the specific occurrence and spontaneous healing of compound tears, potentially affecting the accuracy of our results. While the red-white zone classification is prognostically significant, its systematic application was precluded by 2 factors: the inaccuracy of preoperative MRI in delineating vascular zones and the primary focus of surgical records on tear repairability rather than vascular mapping.14,36 Most critically, the absence of long-term functional outcomes—such as retear rates, joint stability, and return-to-sport metrics—restricts direct translation to clinical practice. These limitations highlight the need for more precise vascular zone classification and blood supply assessment methods, as well as for future prospective studies integrating multicenter registries that track functional endpoints to validate the proposed 8- to 12-week optimal window.
Conclusion
Delaying ACLR until 8 to 12 weeks after injury may allow for the greatest spontaneous healing of meniscal tears that occur with ACL injuries. The healing potential of LM tears, particularly posterior horn longitudinal and radial tears, was greater than that of MM tears in this study. ACLR performed 8 to 12 weeks after injury has been shown to increase arthroscopically confirmed spontaneous healing rates of LM tears by up to 1.5 to 2.5 times compared with those undergoing surgery within the first 8 weeks of injury. However, careful consideration of tear morphology is necessary as certain tear patterns, such as horizontal tears, demonstrated poor spontaneous healing capacity overall. Understanding the healing timeframes of meniscal injuries associated with ACLT may inform decision-making about when to undergo ACLR, allowing spontaneous healing of the meniscal tear and minimizing the need for concomitant meniscal procedures.
Footnotes
Final revision submitted September 25, 2025; accepted October 19, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was funded by the National Natural Science Foundation of China (32471531) and the National Key Research and Development Program of China (2023YFB3812904). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Peking University Third Hospital Medical Science Research Ethics Committee (IRB00006761-M2024173).