
Abstract
Background:
Medial patellofemoral ligament reconstruction (MPFLR) is widely used for treating recurrent lateral patellar instability, with advancements such as artificial tapes and anchor fixation aiming to improve biomechanical stability and recovery outcomes compared with traditional autograft techniques. However, limited research exists on the outcomes of simultaneous bilateral MPFLR.
Hypothesis:
The time to return to sports (RTS) is longer for bilateral MPFLR than for unilateral MPFLR.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Patients were divided into bilateral and unilateral MPFLR groups. RTS rates, time to RTS, and postoperative Knee injury and Osteoarthritis Outcome Score (KOOS) were assessed.
Results:
A total of 45 knees were analyzed, including 21 in the unilateral group and 24 in the bilateral group. Their mean ages were 15.2 ± 1.9 years and 15.2 ± 2.1 years, respectively, with a minimum 2-year follow-up including evaluations at 1, 2, 3, 6, 12, and 24 months postoperatively. Both groups demonstrated favorable postoperative KOOS values across all subscales, with no significant differences between them (pain: 92.3 ± 7.9 vs 89.2 ± 10.3; symptoms: 92.3 ± 8.7 vs 87.4 ± 11.9; activities of daily living: 88.9 ± 15.3 vs 94.2 ± 8.5; sports: 98.2 ± 3.2 vs 85.4 ± 15.5; quality of life: 91.6 ± 12.3 vs 81.4 ± 16.9; all P > .05). RTS rates were 92% for the bilateral group and 76% for the unilateral group, whereas the mean times to RTS were 6.1 ± 2.6 and 5.3 ± 2.4 months, respectively, showing no significant differences. Factors preventing RTS included knee pain, loss of interest, and lifestyle changes such as retirement to pursue higher education.
Conclusion:
Bilateral MPFLR achieved comparable functional outcomes, recovery time, and RTS rates to unilateral procedures. This study suggests that bilateral MPFLR with FiberTape and knotless SwiveLock anchors is an effective treatment for young athletes, offering excellent postoperative knee function and a high RTS likelihood. Further prospective studies with larger cohorts are recommended to validate these results and assess long-term outcomes.
Keywords
Medial patellofemoral ligament reconstruction (MPFLR) is widely used to treat recurrent lateral patellar instability.16,19,27 The MPFL is crucial for stabilizing the patella against lateral displacement, and its dysfunction significantly impairs knee function, especially in active and athletic individuals. 17 Traditional reconstruction techniques, often involving autografts and allografts, have shown favorable outcomes. Allograft tendons avoid donor site morbidity and reduce operative time. However, their use may be associated with a higher risk of graft laxity or failure due to slower biological incorporation compared with autografts.1,15,29
Advances in surgical techniques have introduced the use of artificial tapes combined with anchor fixation as alternatives to traditional graft-based approaches.8,25 This technique aims to strengthen initial stability, 30 minimize donor site complications, and potentially accelerate functional recovery. However, their clinical efficacy, particularly in restoring symmetrical knee function, remains unknown.
Contralateral patellar dislocation occurs in 5% to 9% of patients after an initial dislocation.4,5 Patients who underwent bilateral MPFLR returned to sports at a rate of 62% compared with 72% for those who underwent unilateral reconstruction. 12 However, most studies focus on clinical outcomes after unilateral MPFLR and second-stage bilateral MPFLR; studies on simultaneous bilateral MPFLR for bilateral patellar instability are limited.
In this study, we evaluated the efficacy and safety of using FiberTape and anchors for MPFLR, comparing the outcomes between bilateral and unilateral cases. We aimed to investigate differences in postoperative functional outcomes and return to sports (RTS) rates. We hypothesized that the time to RTS is longer for bilateral MPFLR than for unilateral MPFLR.
Methods
Participants
This study was a retrospective cohort analysis aimed at evaluating the outcomes of MPFLR using artificial tapes and anchor systems. We identified 147 patients who underwent MPFLR between December 2016 and December 2022 from the institutional database. Patients who were not engaged in any sports activities before surgery were excluded, as this study focused on postoperative RTS. Of the 147 cases, we excluded 33 patients who did not engage in any sports activities, 23 aged >30 years, 16 without computed tomography (CT) data, and 4 without KOOS data. During follow-up, we excluded 1 patient who developed a surgical site infection (bilateral case). Overall, we included 21 patients in the unilateral group (those who underwent unilateral MPFLR) and 24 in the bilateral group (those who underwent bilateral simultaneous MPFLR) (Figure 1). Institutional review board approval was obtained before data collection. Preoperative demographics (age, sex, and body mass index [BMI]) were retrospectively collected from medical records.
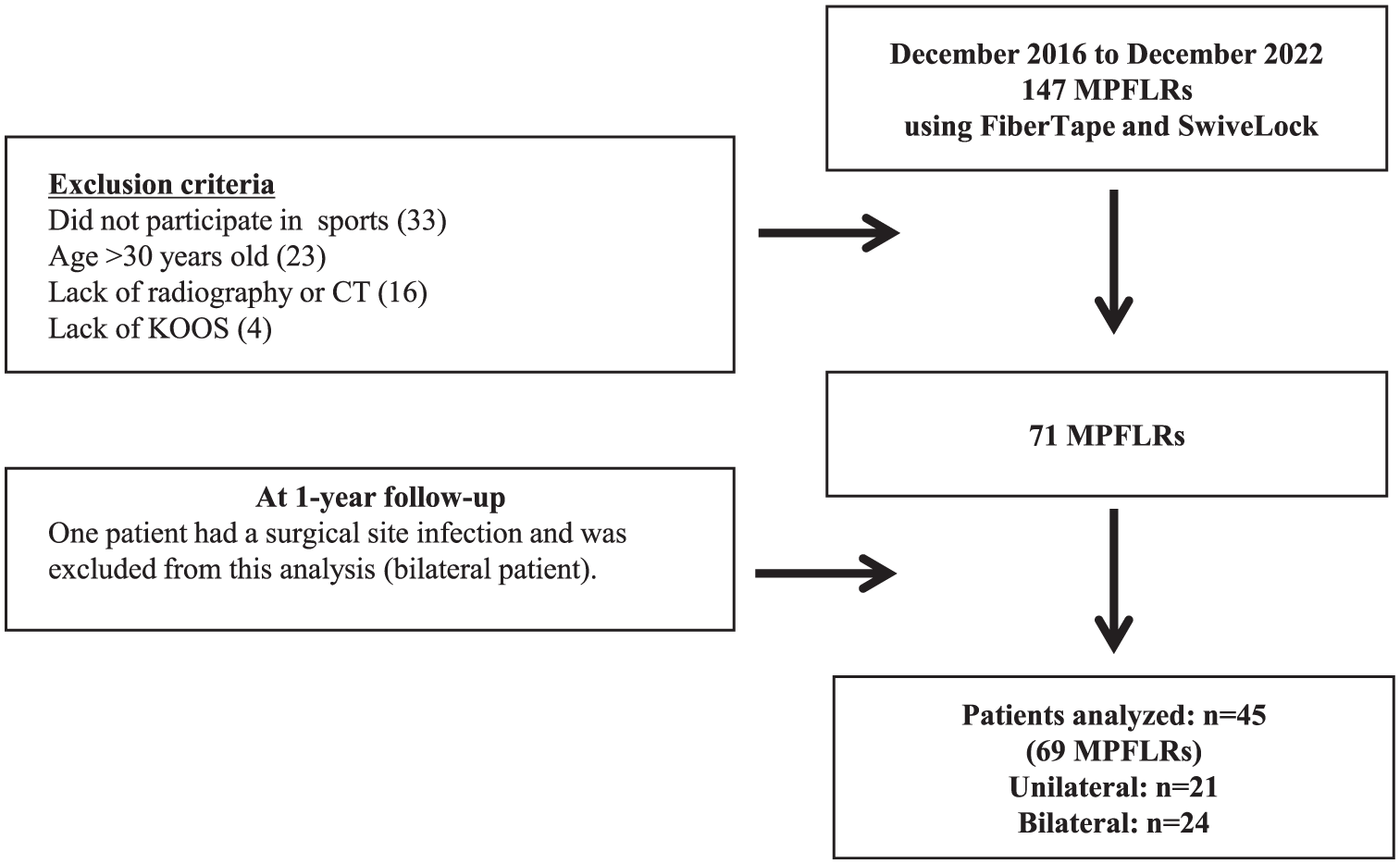
Flowchart of included patients. KOOS, Knee injury and Osteoarthritis Outcome Score; MPFLR, medial patellofemoral ligament reconstruction.
Surgical Management
MPFLR was performed for patients who had experienced at least 2 episodes of recurrent patellar dislocation, confirmed through clinical history, physical examination, and imaging. All patients had previously received nonoperative treatments such as physical therapy and bracing but continued to experience symptoms of instability. All patients in the bilateral group had symptomatic and recurrent patellar dislocations in both knees. In cases of bilateral instability, the decision to perform unilateral or simultaneous bilateral MPFLR was based on the severity and frequency of symptoms on each side and was made through shared decision-making between the patient and the surgeons. Contraindications for this procedure included high-grade trochlear dysplasia (Dejour type D), severe patellofemoral osteochondral damage, and skeletal immaturity. Skeletal maturity was assessed using plain radiographs by confirming the closure of the distal femoral and proximal tibial growth plates. All surgical procedures were performed by 1 of 2 senior orthopaedic surgeons (Y.K., Y.I.). MPFLR was performed using FiberTape (Arthrex) and SwiveLock (Arthrex) following established protocols. 8 Briefly, with the knee flexed to 90°, a 2- to 3-cm longitudinal incision was made along the medial patellar border. The medial retinaculum (first layer) was incised, and a subcutaneous tunnel was created to access the femoral side. Two blind tunnels were drilled in the medial patellar edge—1 proximal near the quadriceps insertion and 1 in the midsection—where 3.5-mm SwiveLock anchors were placed to secure the FiberTape. For femoral fixation, a 2.4-mm Kirschner wire was inserted at the Schöttle point using imaging guidance and an MPFL guide (JBM0200-01/2; BEAR Medic Corp). 14 After confirming the isometry of the FiberTape and patellar tracking through full knee motion, the FiberTape was secured at 90° of flexion with a 4.75-mm SwiveLock anchor. Based on our previous study, it was recommended that the knee flexion angle for suture fixation could be 90° to prevent excessive contact pressure on the patellofemoral joint after MPFLR. 23 To avoid overtensioning, the FiberTape was slightly loosened within a range that prevented patellar dislocation before final fixation. A final arthroscopy examination was performed to confirm proper patellar tracking after fixation.
Postoperative rehabilitation focused on early range of motion. Muscle activation exercises, including patellar setting and straight-leg raises, were started immediately. Weightbearing activities were introduced based on pain tolerance, with jogging permitted approximately 2 months after surgery. No knee braces or other orthotic devices were used postoperatively. All patients followed the same rehabilitation protocol, with no differences between the 2 groups. RTS clearance was determined for each patient through consultations between the surgeon and the rehabilitation team. No standardized objective criteria for RTS, such as limb symmetry testing, were applied.
Alignment Parameters
Preoperative imaging assessment included weightbearing anterior-posterior views and Laurin views. The sulcus and patellar tilt angles were measured on Laurin views with the knee flexed at 30°. 6 Patellar height was assessed using the Caton-Deschamps index on lateral radiographs. 18
Femoral torsion (FT) and tibial torsion (TT) were measured using preoperative CT scans. FT was defined as the angle between a line drawn through the femoral head and neck and a line tangent to the posterior femoral condyles. 28 TT was measured as the angle formed between a line tangent to the back edge of the tibial plateau and a line connecting the centers of the medial and lateral malleoli. 22
The tibial tubercle–trochlear groove (TT-TG) distance was calculated following established methods. The deepest point of the TG was identified on axial CT slices, and its center point was marked. The most prominent point of the tibial tuberosity was also identified and marked. 11 Perpendicular reference lines were drawn from these points to a baseline along the posterior femoral condyles. The TT-TG distance was calculated as the separation between the 2 points.
Measurements were conducted using Picture Archiving and Communication System software (ShadeQuest/ViewR Version 1.24.15; Fujifilm Medical Co Ltd), with an accuracy of 0.01° and length accuracy of 0.01 mm. Alignment parameters were analyzed by 2 trained surgeons (K.I., E.S.) with >8 years of experience.
Clinical Outcomes
All patients were followed for a minimum of 24 months postoperatively. Follow-up assessments were performed by the operating surgeon at 1, 2, 3, 6, 12, and 24 months. The incidences of redislocation and subluxation were evaluated during follow-up. Postoperative outcomes at the final follow-up were assessed using the Knee injury and Osteoarthritis Outcome Score (KOOS), which includes 5 subscales: pain, symptoms, quality of life, sports, and activities of daily living. 3
Clinical outcomes were evaluated during routine outpatient visits. Patients were asked standardized questions regarding knee stability, pain, and ability to return to preinjury levels of play. Level of play was determined based on patient self-report and categorized as return to the same or lower level or no participation in sport.
Statistical Analysis
All statistical analyses were performed using SPSS software (Version 29.0; IBM). Continuous variables are expressed as mean ± standard deviation, whereas categorical data are reported as frequency and percentage. The normality of continuous variables was assessed using the Shapiro-Wilk test. The Mann-Whitney U test was used to compare continuous variables, such as time to RTS, KOOS subscale values, and alignment parameters, owing to nonnormal distribution. Categorical variables, including RTS rates and levels of sports participation, were analyzed using the chi-square or Fisher exact test depending on sample size. Statistical significance for all analyses was set at a P value <.05.
Intrarater reliability, expressed as the interclass correlation coefficient (2.1), was 0.821 (95% CI, 0.539-0.818; P < .001) for FT, 0.793 (95% CI, 0.492-0.700; P < .001) for TT, and 0.862 (95% CI, 0.391-0.791; P < .001) for TT-TG.
Results
The mean age was 15.2 ± 2.0 years (range, 11-20 years), and the mean BMI was 23.3 ± 3.9 kg/m2, with no significant differences observed between groups (P = .595 and P = .619, respectively). No significant differences were observed for alignment parameters (Table 1).
Patient Demographic Data and Alignment Parameters a
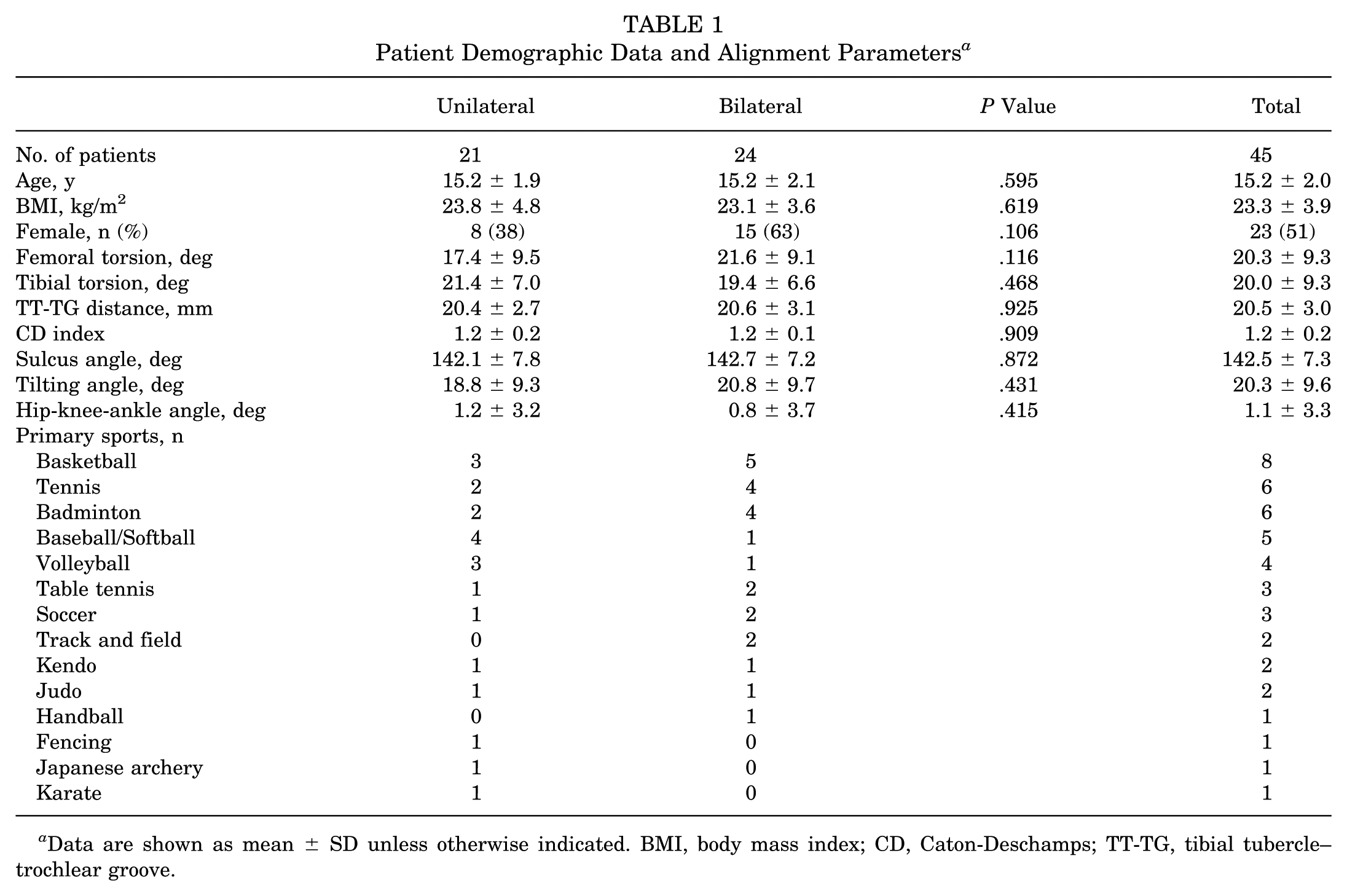
Data are shown as mean ± SD unless otherwise indicated. BMI, body mass index; CD, Caton-Deschamps; TT-TG, tibial tubercle–trochlear groove.
During the minimum 24-month follow-up period, no cases of postoperative patellar redislocation or symptomatic subluxation were observed in either unilateral or bilateral MPFLR groups. Both groups demonstrated favorable postoperative outcomes with high KOOS values. KOOS subscale values are summarized in Table 2. There were no statistically significant differences between the unilateral and bilateral groups across any subscale.
Comparison Between Preoperative and Postoperative Outcomes a

Data are shown as mean ± SD. KOOS subscales were compared using the Mann-Whitney U test. KOOS, Knee injury and Osteoarthritis Outcome Score.
As shown in Table 3, there were no statistically significant differences in rates of RTS or in the time to return between the unilateral and bilateral groups.
Comparison of RTS After Unilateral and Bilateral Medial Patellofemoral Ligament Reconstruction a

Measurements between the 2 groups were compared using the chi-square and Mann-Whitney U tests. RTS, return to sports.
Reasons for not returning to sports included knee pain in 1 patient from each group, loss of interest in 1 patient in the unilateral group, and retirement to pursue higher education in 3 patients in the unilateral group and 1 patient in the bilateral group (Table 4).
Reasons for Not Returning to Sports After Medial Patellofemoral Ligament Reconstruction a

Data are shown as number of patients.
Discussion
Unilateral and bilateral MPFLR using FiberTape and SwiveLock anchors yielded excellent postoperative outcomes. Bilateral MPFLR was associated with a marginally longer time to RTS and lower KOOS values in certain subscales; however, these differences were not statistically significant. In addition, >90% of bilateral cases achieved RTS. These findings suggested that bilateral MPFLR is a viable option for young athletes, with outcomes comparable to those of unilateral reconstruction.
MPFLR is an effective treatment for patellar instability with a high RTS rate. 26 Investigations on the rate of RTS after MPFLR provide valuable insights into patient outcomes and influencing factors. A meta-analysis of 23 studies with 786 patients reported that approximately 92.8% of patients returned to sport within a mean of 6.7 months, with 71.3% achieving preinjury sports level or higher. 9 RTS rates were marginally lower for patients who underwent MPFLR combined with osteotomy (86.9%) compared with those for patients who underwent MPFLR only (95.4%). Notably, fear of reinjury was the most common reason for patients returning at a lower play level, affecting 39.7% of participants.
Unilateral MPFLR has been reported to yield higher RTS rates than bilateral MPFLR. 20 Bilateral MPFLR is associated with prolonged recovery and compounded psychological barriers, such as fear of reinjury and lack of confidence, reducing RTS rates. 12 Liu et al 13 studied RTS outcomes in 91 patients who underwent unilateral or bilateral MPFLR without additional osteotomy. It was found that 94.5% of patients returned to sports, with 74% regaining their preoperative levels of play. However, the study did not include a subgroup analysis comparing unilateral and bilateral MPFLR outcomes. Li et al 12 compared RTS rates between bilateral and unilateral MPFLR cohorts with mean ages of 25 and 22 years, respectively. The RTS rates were 62% for bilateral MPFLR and 72% for unilateral MPFLR, with significant differences. Conversely, Klueh et al 9 reported a significantly lower RTS rate in patients who underwent bilateral MPFLR than in those who underwent unilateral MPFLR (69% vs 94%; P = .03). Among those who returned to sports, no significant difference was observed in the postoperative level of play achieved. Specifically, 81% of the bilateral group reached the same or a higher level of play compared with 67% in the unilateral group. These discrepancies are likely due to the difference in surgical procedures and activity levels. In the present study, the RTS rate in the bilateral group was not significantly different from that in the unilateral group, suggesting that simultaneous bilateral MPFLR may be a reasonable treatment option for patients evaluated with symptomatic instability in both knees. Therefore, when both knees fulfill the surgical indication criteria and the patient is motivated, simultaneous bilateral MPFLR may offer a practical and efficient approach without compromising short-term RTS outcomes. Furthermore, our study showed a more favorable RTS rate of 92%, in comparison with previous studies.9,12,24 Regarding patients who retired to pursue higher education, the adjusted RTS rates were 19 of 21 (90%) in the unilateral group and 23 of 24 (96%) in the bilateral group. This discrepancy between our study and previous studies may be attributed to differences in patient selection (ie, young athletes), consistent use of FiberTape and anchor fixation providing greater initial stability, and no donor site morbidity. These factors may collectively enhance early recovery and facilitate successful RTS.
Although MPFLR effectively treats recurrent patellar instability with high RTS rates, 21 some patients are unable to return to their preinjury play level. Fear of reinjury and knee instability often prevent RTS after surgery for knee injury.7,10 Bony malalignment, trochlear dysplasia, and patella alta contraindicate isolated MPFLR.2,32 Xu et al 31 reported that patients returning to sports before 9 months after surgery exhibit a high incidence of postoperative anterior knee pain, suggesting that returning too early may negatively affect postoperative outcomes. These findings suggested that careful consideration of RTS timing is crucial for optimal outcomes after MPFLR.
This study has some limitations. First, it was a retrospective study, with a relatively small sample size and no long-term data. Second, the absence of a standardized definition of RTS complicates cross-study comparisons, as some include only organized sports, whereas others consider general athletic activities. Third, there is the lack of a quantitative method for determining graft tension during MPFLR. Although we followed a standardized protocol based on intraoperative assessment of isometry and patellar tracking, final tensioning was performed subjectively by the surgeon. The inability to precisely quantify graft tension may introduce variability in postoperative outcomes. Fourth, because of the retrospective design of the study, we were unable to perform a priori sample size calculation. The limited sample size may reduce the ability to detect subtle differences between groups. Finally, we did not assess patella-specific outcome scores such as the Kujala score. Although we used the KOOS, which includes sports and symptoms subscales relevant to patellofemoral function, the addition of a validated patella- and femur-specific measure could have enhanced the clinical relevance of our findings.
Conclusion
Simultaneous bilateral MPFLR provided favorable clinical outcomes with high RTS rates. Patients with bilateral symptoms did not demonstrate prolonged time to return compared with patients in the unilateral group, suggesting that simultaneous bilateral MPFLR may be considered as a reasonable option in appropriately selected patients
Footnotes
Final revision submitted October 18, 2025; accepted October 29, 2025.
The authors declare that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto. Ethical approval for this study was obtained from Hirosaki University Hospital (No. 2014-229).