
Abstract
Background:
The diagnostic accuracy of magnetic resonance imaging (MRI) and magnetic resonance arthrography (MRA) for detecting labral tears is well established in femoroacetabular impingement but remains unclear in dysplastic hips undergoing hip arthroscopy (HA) combined with periacetabular osteotomy (PAO).
Purpose:
To determine the sensitivity and specificity of MRI and MRA in identifying labral tears in patients with dysplasia undergoing HA combined with PAO.
Study Design:
Cohort study (diagnosis); Level of evidence, 3.
Methods:
A retrospective, real-world study was conducted at a single tertiary hip preservation center. Patients included in the analysis had undergone primary HA and PAO with available radiologist interpretation for labral assessment. Diagnostic accuracy of MRI and MRA for detecting labral tears was assessed using arthroscopic findings as the reference standard. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), positive likelihood ratio (LR+), and negative likelihood ratio (LR−) were calculated.
Results:
A total of 122 patients (mean age, 22.3 years; SD, 5.6; 90% women) were included. Radiographic measurements showed a mean lateral center-edge angle of 22.91° (SD, 6.52), an acetabular index of 8.87° (SD, 5.27), and a Tönnis grade of 0.09 (SD, 0.35). Both MRI and MRA demonstrated low sensitivity (55% and 54.1%, respectively) and low specificity (38.5% and 45.5%, respectively). The PPV was moderate (67.3% for MRI; 71.4% for MRA), and the NPV was low (27% for MRI; 31.3% for MRA). LR+ and LR− values of MRI and MRA were close to 1.
Conclusion:
This study highlights the limited diagnostic accuracy of MRI and MRA for identifying labral tears in patients with hip dysplasia undergoing combined HA and PAO. Operative decisions regarding labral treatment at the time of PAO should not be based solely on preoperative imaging.
Hip dysplasia is a common cause of hip pain that is characterized by reduced femoral head coverage, leading to overloading of the acetabular cartilage rim and labrum.11,13,23 Periacetabular osteotomy (PAO) is a well-established joint-preserving surgical procedure for correcting this acetabular deficiency with generally good to excellent short and long-term outcomes.1-3,19,20,25 However, an untreated labral tear may contribute to persistent postoperative symptoms and less-than-desirable outcomes.6-8,24,27,29 Magnetic resonance imaging (MRI) and magnetic resonance arthrography (MRA) have been shown to be accurate in identifying hip labral tears in those with femoroacetabular impingement syndrome (FAIS).28,30,31,33 However, the sensitivity and specificity of MRI and MRA for detecting labral tears at the time of surgery in patients with dysplasia undergoing combined hip arthroscopy and PAO remain unknown.
The labrum in dysplastic hips is commonly hypertrophied to compensate for bony undercoverage, potentially making it more susceptible to degeneration and tearing due to chronic shear stresses.9,14,17,22,26 Previous studies found that the incidence of labral tears in dysplastic hips treated with PAO ranged from 46% to 98% at the time of surgery.4,6,7,10,23 While many patients achieve good outcomes with PAO alone, some continue to experience unfavorable results, possibly due to an unaddressed labral tear.12,18 Recent literature supports combined hip arthroscopy and PAO as a comprehensive approach to addressing intra-articular pathology and hip dysplasia.5,9,12,18 MRI and MRA are the most common means used for diagnosing labral tears. 33 A meta-analysis by Zhang et al 33 reported pooled sensitivity and specificity of 1.5-T and 3-T MRI for diagnosing labral tear as 0.80 and 0.77, respectively, in patients with FAIS. Zhang et al also found that the sensitivity of 3-T MRI for labral tear detection was comparable to that of MRA (0.87 vs 0.89), while its specificity was superior (0.77 vs 0.69). Insurance carriers are therefore increasingly denying hip arthroscopy (HA) in the setting of PAO based solely on negative MRI or MRA findings for a labral tear. However, there are potential limitations in the accuracy of MRI and MRA in detecting labral tears in dysplastic hips due to the hypertrophied nature of the labrum, which may ultimately lead to misinterpretation.
Given the implications for clinical decision-making and insurance coverage, a better understanding of diagnostic accuracy for MRI and MRA in patients undergoing HA combined with PAO is essential. This study aimed to determine the sensitivity and specificity of MRI and MRA for the identification of a labral tear in patients undergoing HA combined with PAO presenting to a tertiary care hip preservation center. It was hypothesized that both MRI and MRA would demonstrate acceptable sensitivity and specificity for detecting labral tears in patients undergoing HA combined with PAO.
Methods
A retrospective, real-world design study was conducted at a single tertiary hip preservation center. This study was approved by Mount Carmel Institutional Review Board (180731-3). Patients included in this study were those undergoing primary HA and PAO with an available radiologist interpretation for labral assessment between January 1, 2021, and November 27, 2023. The surgeon (T.J.E.) always performs HA in conjunction with PAO. All patients had signs and symptoms positive for a labral tear—including a positive flexion-adduction-internal rotation test, and reported painful clicking, popping, or catching. The clinical signs for a labral tear were assessed by the treating surgeons (T.J.E. or R.C.K.), and the official radiology report was used to determine the presence or absence of a labral tear. Radiographic measurements were collected to evaluate acetabular morphology and joint degeneration—including the lateral center-edge angle, acetabular index, and Tönnis grade—as assessed by the 2 treating surgeons (T.J.E. and R.C.K.). Patients were excluded if they had undergone revision HA or PAO or if their MRI or MRA findings for labral tear were unknown. MRIs and MRAs were obtained from a referral base spanning 4 states. All MRIs and MRAs had been previously interpreted by board-certified radiologists. MRI diagnosis was performed using a 1.5-T scanner in 64 patients and a 3-T scanner in 22 patients. MRA was performed using a 1.5-T scanner in 26 patients and a 3-T scanner in 10 patients. A total of 98 (80.3%) MRI and MRA images were interpreted by fellowship-trained radiologists in musculoskeletal imaging from different radiology centers across a 3-state region.
Surgical Procedures
All patients had labral status determined intraoperatively as part of combined HA and PAO procedures. One surgeon (T.J.E.) performed all arthroscopies. HA was performed in the modified supine position utilizing a post-free technique with a saline arthrogram, as previously described in the literature. 21 Standard anterolateral, modified mid-anterior, and distal anterolateral portals were used for arthroscopic access. Acetabuloplasty, femoroplasty, and/or labral repair were performed as indicated, and the hip capsule was closed in all patients. After HA, patients were transferred to the flat-top position for PAO, as previously described. 32
Statistical Analyses
The diagnostic accuracy of MRI and MRA for detecting labral tears was assessed using arthroscopic findings as the reference standard. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), positive likelihood ratio (LR+), and negative likelihood ratio (LR−) were calculated using the software R Version 4.4.3 (R Core Team), with true-positive, true-negative, false-positive, and false-negative results classified accordingly. LR+ and LR– were interpreted as follows: LR+ >10 or LR– <0.1 indicated strong evidence to rule in or rule out a diagnosis; LR+ of 5–10 or LR– of 0.1–0.2 indicated moderate evidence; LR+ of 2–5 or LR– of 0.2–0.5 indicated small evidence. 16
Results
During the study period, 157 patients underwent concomitant PAO and HA. Nineteen were excluded because of the absence of MRI or MRA magnet strength information, and 16 were excluded because of the lack of radiologist reports. A total of 122 patients were included in the study, with an age range of 14 to 40 years and a mean age of 22.3 years (Table 1). Radiographic measurements demonstrated a mean lateral center-edge angle of 22.91° (SD, 6.52), an acetabular index of 8.87° (SD, 5.27), and a Tönnis grade of 0.09 (SD, 0.35). The patients consisted of 111 women (90%) and 11 men (9%). The numbers and proportions of labral tears reported on MRI/MRA—confirmed arthroscopically and treated with labral repair—are summarized in Table 2. The accuracy, sensitivity, specificity, PPV, NPV, LR+, and LR– of MRI—compared with arthroscopy and the surgeon's intraoperative decision—are presented in Table 3.
Demographic Characteristics a

LCEA, lateral center-edge angle; MRA, magnetic resonance arthrography; MRI, magnetic resonance imaging.
MRI/MRA-Reported Labral Tears, Arthroscopic Confirmation, and Labral Repairs in Patients Undergoing Concomitant PAO and HA a

HA, hip arthroscopy; MRA, magnetic resonance arthrography; MRI, magnetic resonance imaging; PAO, periacetabular osteotomy.
MRI and MRA Results Compared with Arthroscopy a
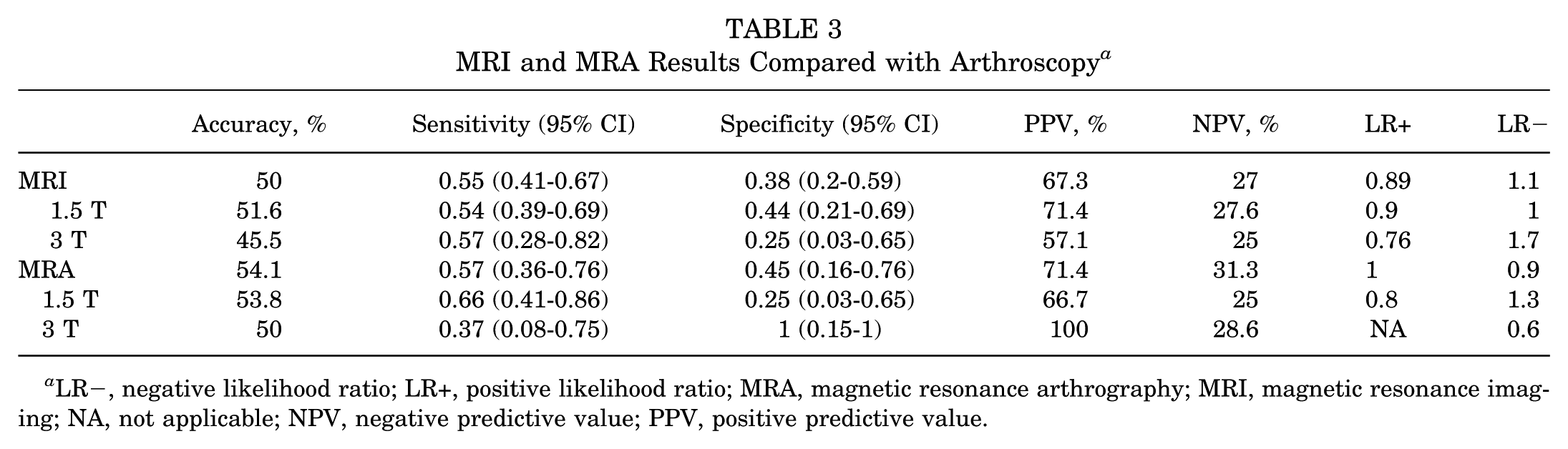
LR−, negative likelihood ratio; LR+, positive likelihood ratio; MRA, magnetic resonance arthrography; MRI, magnetic resonance imaging; NA, not applicable; NPV, negative predictive value; PPV, positive predictive value.
Discussion
The major findings of our study demonstrated that both MRI and MRA showed limited diagnostic accuracy for detecting labral tears in patients with hip dysplasia undergoing combined HA and PAO, which may reduce their utility in guiding clinical decision-making. Overall, MRI (50%) and MRA (54.1%) demonstrated low accuracy in identifying labral tears in those undergoing combined HA and PAO. Both MRI and MRA demonstrated low sensitivity (MRI, 55%; MRA, 54.1%) and low specificity (MRI, 38.5%; MRA, 45.5%) compared with arthroscopic findings. These findings suggest that MRI or MRA alone may be insufficient to accurately identify labral tears in patients with hip dysplasia undergoing combined HA and PAO. In addition, the PPVs were moderate (67.3% for MRI and 71.4% for MRA), suggesting that a positive finding may have some clinical value. However, the NPVs were low (27% for MRI and 31.3% for MRA, respectively), indicating that a negative result does not reliably exclude a labral tear. Additionally, the likelihood ratios (LR+ and LR−) for MRI and MRA were close to 1, indicating limited diagnostic value in differentiating between patients with and without labral tears. These findings highlight the challenges of using MRI or MRA for preoperative evaluation of labral tears in dysplastic hips and underscore the potential need for intraoperative assessment.
Compared with previous studies, the findings of this study demonstrate lower sensitivity and specificity for MRI in diagnosing labral tears. Zhang et al 33 conducted a systematic review and meta-analysis including 22 studies with 1670 patients with FAIS and found a summary sensitivity of 0.8 and specificity of 0.77 for MRI. Zhang et al 33 reported a sensitivity of 0.89 and a specificity of 0.69 for MRA. Notably, all studies included in this meta-analysis used arthroscopy as the gold standard, similar to the present study. The main difference in diagnostic accuracy between the 2 studies is likely due to differences in the population. While Zhang et al focused on patients with FAIS, this study specifically evaluated those with hip dysplasia, a population in which MRI may be limited by labral hypertrophy and altered joint morphology. Low MRI and MRA sensitivity may lead to missed true labral tears, potentially resulting in undertreatment. Zhang et al 33 also found that 3-T MRI demonstrated sensitivity values comparable with MRA (0.87 vs 0.89) and superior specificity (0.77 vs 0.69). However, this study found no significant difference in sensitivity between 1.5-T MRI (0.54), 3-T MRI (0.57), and MRA (0.57). This similarity in accuracy between 1.5-T and 3-T MRI and MRA may be due to a smaller sample size, which limits statistical power.
The lower MRI accuracy in detecting labral tears in patients with hip dysplasia compared with those with FAIS may be attributed to anatomic and pathological differences between the 2 conditions. In dysplastic hips, the labrum often becomes hypertrophied as a compensatory response to decreased femoral head coverage.14,17,22 This thickened labrum may appear hyperintense on MRI, complicating the distinction between normal adaptive changes and true pathology. 22 Conversely, labral tears associated with FAIS are typically thinner, more focal, and result from mechanical impingement, making them easier to visualize and identify on imaging. 15 Additionally, the tear patterns differ between these 2 populations. FAIS-related tears are usually located at the anterosuperior acetabular rim. This is an area where MRI is highly sensitive. In contrast, labral tears in dysplastic hips tend to be more diffuse and are often accompanied by chondral lesions. These injuries result from chronic instability and shear stress rather than acute impingement. 23 These degenerative and widespread changes may not be as readily detectable with conventional MRI sequences, further contributing to the reduced diagnostic accuracy observed in this population.
An important strength of this study is its real-world design, which reflects the variability and complexity encountered in actual clinical practice. The MRI and MRA reports were obtained from a referral spanning 4 states and had been previously interpreted by board-certified radiologists. However, as is typical in real-world clinical settings, not all scans were reviewed by musculoskeletal fellowship-trained radiologists (80.3% were), and the imaging studies varied in magnetic field strength (1.5 T vs 3 T), contributing to diversity in imaging quality. This heterogeneity mirrors everyday clinical scenarios, where patients present to a hip preservation center with externally acquired imaging of varying quality and interpretive standards, and treating physicians must make decisions based on the available information. Rather than representing a methodological limitation, this variability enhances the external validity of our findings by illustrating the diagnostic challenges inherent in routine practice. In particular, it highlights the limitations of relying solely on MRI or MRA reports for diagnosing labral tears in dysplastic hips. These findings may also help explain why insurance carriers increasingly deny authorization for hip arthroscopy in the setting of dysplasia based solely on MRI or MRA results.
Limitation
This study has several limitations. This study included variability in imaging interpretation because MRIs and MRAs were read by multiple radiologists with differing levels of musculoskeletal training. Second, the samples of patients who received MRA were relatively small, limiting the statistical power of subgroup analyses. Third, selection bias may be present, as all included patients underwent both HA and PAO, representing a specific surgical population that may not be generalizable to all patients with hip dysplasia. These factors should be considered when interpreting the diagnostic performance of MRI and MRA in this context.
Conclusion
This study highlights the limited diagnostic accuracy of MRI and MRA for identifying labral tears in patients with hip dysplasia undergoing combined HA and PAO. Operative decisions regarding labral treatment at the time of PAO should not be based solely on preoperative imaging, but rather on direct intraoperative arthroscopic evaluation.
Footnotes
Final revision submitted September 22, 2025; accepted October 8, 2025.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Mount Carmel Institutional Review Board. (reference number IRB No. 180731-3).