
Abstract
Background:
Two recent studies have shown that patients with jumping sign exhibit more pronounced lower limb torsional abnormalities and trochlear bump in recurrent patellar dislocation (RPD), suggesting that medial patellofemoral ligament (MPFL) reconstruction may not fully correct the patellofemoral relationship in patients with a jumping sign.
Purpose:
To determine whether there was an association between the preoperative jumping sign and MPFL graft failure.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
Patients who underwent primary surgery and follow-up evaluation due to RPD at our institution from 2012 to 2022 were eligible. Those who received initial combined derotational osteotomy were excluded. Patients with graft failure (postoperative patellar redislocation) were matched in a 1:2 ratio with patients who did not experience failure. Preoperative lower limb bony structural abnormalities were evaluated and combined with the jumping sign to analyze independent factors associated with graft failure. A graft failure nomogram was constructed, and model performance was examined.
Results:
A total of 129 patients (129 knees) were included, with 43 in the graft failure group. The 2 groups were comparable in terms of age, sex, number of dislocations, duration of symptoms, and primary procedures. The incidence of preoperative jumping signs in the graft failure group was significantly higher than that in the control group (69.8% vs 18.6%, P < .001). Multivariable regression analysis identified 3 independent factors associated with graft failure: jumping sign (odds ratio [OR], 4.44; 95% CI, 1.63-12.12; P = .004), increased femoral anteversion (OR, 6.23; 95% CI, 2.18-17.77; P = .001), and excessive knee torsion (OR, 3.02; 95% CI, 1.51-11.58; P = .006). After including these factors in a nomogram, the C-index of the model was 0.832, indicating reliable performance. Good concordance between the predicted risk and the actual graft failure rate was also observed.
Conclusion:
A preoperative jumping sign was present in almost 70% of patients with MPFL graft failure. This sign, combined with excessive lower limb rotational abnormalities, was identified as associated with graft failure after primary MPFL reconstruction in patients with RPD.
For recurrent patellar dislocation (RPD) requiring surgical intervention, medial patellofemoral ligament (MPFL) reconstruction (MPFL-R) is the gold standard surgical technique. Previous studies have shown that even with standardized procedures (eg, graft selection and femoral tunnel position), the incidence of postoperative patellar redislocation remains between 2% and 8%.17,19
Understandably, unaddressed risk factors from the primary surgery could be a significant cause of clinical graft failure. Previous studies have elucidated that femoral tunnel malposition was associated with a higher rate of postoperative complications8,16 and graft failure 28 after MPFL-R. In addition to surgical techniques, various bony structural abnormalities have been recognized and identified as risk factors for poor outcomes, such as increased femoral anteversion and excessive knee torsion. Zhang et al 26 reported that after MPFL-R, patients with increased femoral anteversion angle (>30°) exhibited inferior postoperative clinical outcomes, including greater graft laxity and a higher incidence of redislocation. Furthermore, they also observed that patients with excessive tibiofemoral rotation (>12.3°) were more likely to have experienced MPFL graft failure (odds ratio [OR], 13), providing further insights into the etiological mechanisms of patellar dislocation. 28 Kaiser et al 10 found that isolated MPFL-R for patellar instability is insufficient in cases of higher degrees of internal femoral torsion, highlighting the need for further investigation into abnormal indicators requiring additional surgical intervention. High-grade trochlear dysplasia demonstrates a significant effect on the positive J-sign. Even following trochleoplasty, the incidence of residual patellar maltracking remains approximately 13%. 3
A new study has shown that patients with a jumping sign exhibit rotational abnormalities consistent with a high-grade J-sign in patients with RPD. 21 This sign is also closely related to the trochlear bump. 4 This suggests that this sign may predict bony structural abnormalities or clinical outcomes of the graft. Therefore, the purpose of this study was to determine the proportion of jumping signs in patients with patellar redislocation and investigate whether it is an independent risk factor for MPFL graft failure.
Methods
Study Design
This study was approved by the Ethics Committee of Beijing Jishuitan Hospital (Ethics Number: 01-07-2018). All patients signed an informed consent form upon admission. Retrospective screening was conducted on patients who underwent surgical treatment for recurrent patellar dislocation at our institution from January 2012 to September 2022. Clinical examination and imaging data were collected. Patients with the following criteria were included: (1) MPFL-R, with or without tibial tuberosity osteotomy and trochleoplasty procedures; (2) postoperative follow-up data (>2 years); (3) preoperative and postoperative documentation of patellar tracking; and (4) preoperative hip-knee-ankle scan in the standard position (patient supine with patella facing upwards). Exclusion criteria involved (1) revision cases, (2) cases combined with femoral or tibial derotational osteotomy, (3) unclear determination of preoperative patellar tracking, (4) nonstandard preoperative scan, (5) history of ipsilateral knee joint fractures, and (6) limited knee extension. The flowchart of patient selection is shown in Figure 1. This study was conducted and reported in line with the Strengthening the Reporting of Observational Studies in Epidemiology checklist.
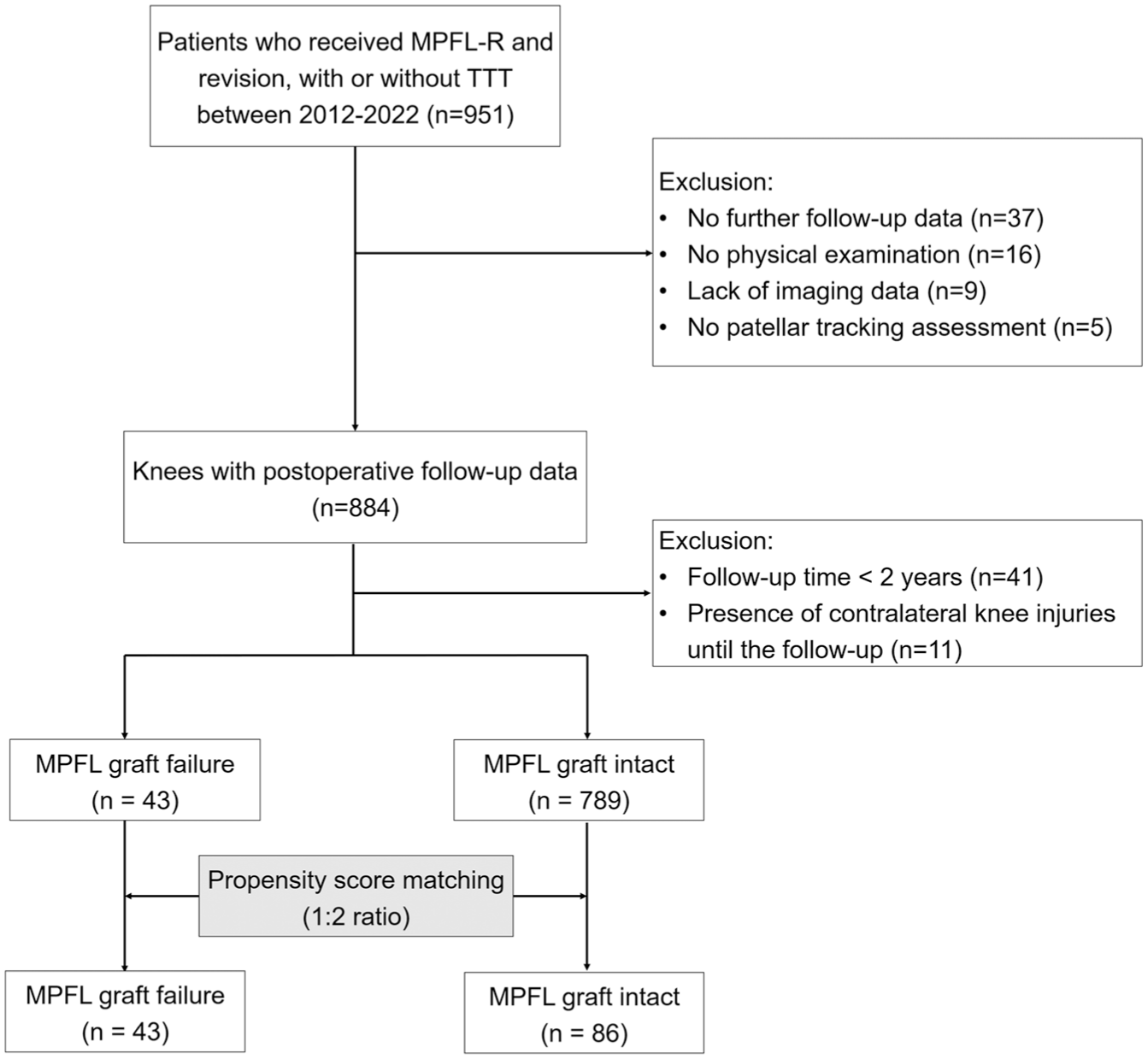
Flowchart of patient selection. MPFL-R, medial patellofemoral ligament reconstruction; RPD, recurrent patellar dislocation.
Evaluation of Patellar Tracking
All patients underwent video recording of knee flexion-extension at least 5 times preoperatively (with legs naturally hanging down, then actively extending the knee). This study adopted a newly proposed method for patellar tracking 21 : during dislocation or reduction of the patella, a jumping motion is referred to as the “jumping sign.” In contrast, the gliding dislocation or reduction of the patella is defined as the “gliding sign” (Appendix 1; see the online Video Supplement for this technique).
Surgical Interventions
MPFL Reconstruction
The MPFL was reconstructed using a semitendinosus tendon autograft (all patients). Based on the method described by Schöttle et al, 15 the femoral tunnel position was determined under intraoperative fluoroscopy. Two double-loaded suture anchors were inserted into the proximal one-third and equatorial regions of the patella, respectively. The graft was first fixed on the patellar side, and the free end of the graft was then pulled into the femoral tunnel and fixed with a bioabsorbable interference screw at 20° to 30° of knee flexion.
Additional Procedures
Patients demonstrating a tibial tuberosity–trochlear groove (TT-TG) distance ≥20 mm underwent Elmslie-Trillat medialization osteotomy for TT-TG normalization (target: 10-12 mm). Those with patella alta (Caton-Deschamps index [CDI] ≥1.2) received additional tibial tubercle distalization to restore patellar height to 1.0. Trochleoplasty was performed when arthroscopic evaluation revealed persistent patellar maltracking during trochlear engagement after MPFL-R with a concomitant tibial tubercle osteotomy (if indicated).
Clinical MPFL Graft Failure
In this study, MPFL graft failure was defined as patellar redislocation after the primary surgery, which was confirmed during outpatient visits with the patients.
Measurement of Bony Structures
Standard hip-knee-ankle computed tomography scans (Figure 2A) were conducted preoperatively for all patients. Three-dimensional reconstruction of the lower limb bones was carried out using Mimics 20.0. Rotation parameters of the lower limb were assessed following the methodology outlined in previous studies.18,22

(A) Standard computed tomography scan of the hip-knee-ankle and measurement of lower limb torsion parameters. (B) Femoral anteversion. (C) Knee torsion. (D) Tibial torsion.
Femoral Anteversion
The center points of the femoral head and neck were identified through a circle-fitting method. Femoral anteversion (FAA) is defined as the angle formed between line 1, which connects the femoral head and neck, and line 2, which links the posterior condyles of the femur (Figure 2B).
Knee Torsion and Tibiofemoral Rotation Angle
For knee rotation measurement, the reconstructed tibia was used to establish the posterior-anterior view, after which the model was adjusted to align the posterior edge of the tibial plateau horizontally. Knee torsion was defined as the angle between the posterior tibial plateau tangent (line 3) and line 2 (Figure 2C).
Tibial Torsion Angle
The measurement relies on the rotational angle of the proximal tibia in relation to the distal tibia. The posterior tibial plateau was kept horizontally aligned. The center point of the distal tibia and fibula was identified, and line 4 was drawn accordingly. Tibial torsion angle was defined as the angle between lines 3 and 4 (Figure 2D).
TT-TG
The distance was determined by superimposing the trochlear level and tibial tuberosity level on the computed tomography cross-sectional image. The lowest point of the trochlea and the midpoint of the tibial tuberosity were identified and marked. These points were then projected onto the line connecting the posterior condyles of the femur, with the measured distance between them representing the TT-TG distance.5,21,22
Patellar Height
The CDI is commonly used to evaluate patellar height.6,12,23 It can be measured on the lateral view, with 30° of the knee. 21
Trochlear Dysplasia
Trochlear dysplasia was evaluated based on the Dejour classification method using the true lateral view of the knee. Patients were classified into one of the following categories: normal or Dejour type A, B, C, or D. Severe trochlear dysplasia was defined as types B and D. 5
Based on established thresholds, the bony structures were categorized into normal and abnormal groups. 21 To be specific, (1) FAA >30° indicates excessive femoral anteversion, associated with significantly worse clinical outcomes 26 ; (2) knee torsion >12° indicates excessive knee torsion, significantly increasing the risk of graft failure (OR, 13) 28 ; and (3) CDI >1.2 and TT-TG >20 mm indicate patella alta and excessive tibial tuberosity lateralization, respectively. 5 These categorizations are summarized in Table 1.
Bony Abnormalities Associated With Recurrent Patellar Dislocation and Their Classification Criteria a
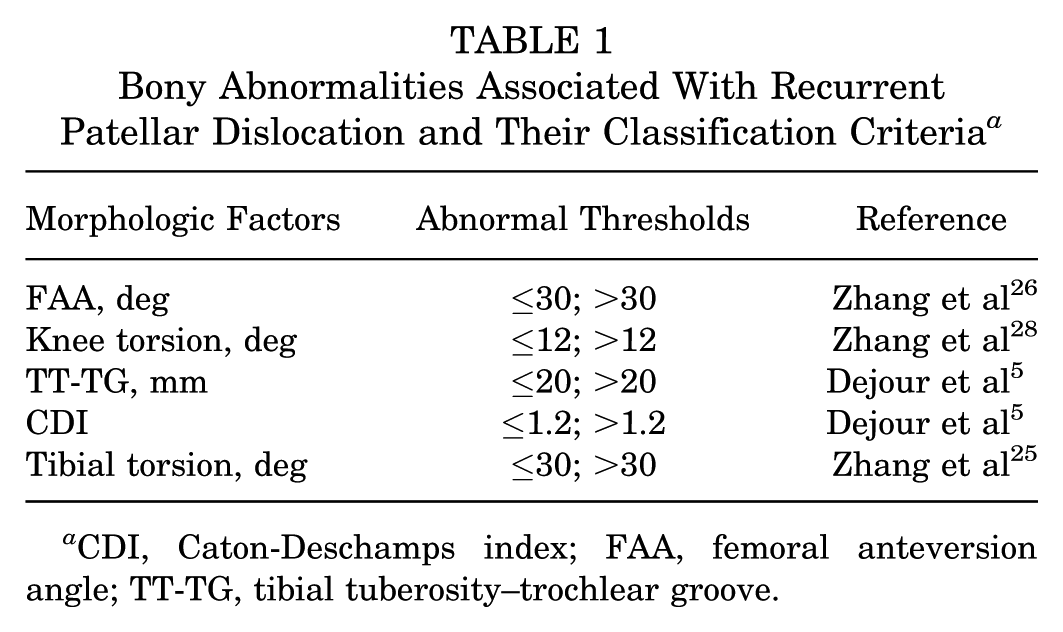
CDI, Caton-Deschamps index; FAA, femoral anteversion angle; TT-TG, tibial tuberosity–trochlear groove.
Sample Size, Reliability, and Statistical Analysis
This study aimed to develop a predictive model for MPFL-R failure using preoperative clinical variables through regression analysis. For multivariable analyses such as multiple regression, logistic regression, and factor analysis, the estimation of the sample is often 5-, 10-, or 20-fold the number of variables of interest. 14 Here, we included 7 variables (preoperative jumping sign, trochlear dysplasia, FAA, knee torsion, TT-TG, CDI, and tibial torsion); hence, a minimum of 35 patients in the graft failure group was required to ensure the representativeness of the sample.
The κ coefficient and intraclass correlation coefficient (ICC) were calculated to evaluate the reliability of the measurement method used in this study. Sample size calculation for reliability analysis was performed using PASS 2021 (NCSS).2,20 With approximately 90% confidence, it was determined that a stable consistency coefficient could be achieved with just 14 samples when 2 measurers independently assessed the same parameters using the same approach. Consequently, 20 samples were randomly selected. Two experienced researchers (H.Z. and D.W.) independently measured the patellar tracking grade and lower limb bone structure parameters (each rater performed a single assessment). The κ coefficient and ICC for interobserver reliability were calculated (κ coefficient >0.6 means adequate reliability 13 ).
Normality tests were conducted on continuous variables. If the data satisfied normality assumptions, the mean (standard deviation) was reported, and an independent samples t test was performed to compare differences between the 2 MPFL graft groups. If normality was not met, the median (interquartile range) was recorded, and the Wilcoxon rank-sum test was applied to assess group distribution differences. Categorical variables were presented as frequency (%) and analyzed using the chi-square test to evaluate differences in the jumping sign between groups. Univariate and multivariate logistic regression analyses were used to identify risk factors for graft poor outcomes. A nomogram was then created to facilitate failure prediction. The C-index of the nomogram was calculated to assess the model. P < .05 was considered statistically significant. All data analyses were conducted using the R package (R Project for Statistical Computing) and SPSS 26 (SPSS, Inc).
Results
Patient Characteristics
A total of 129 patients (129 knees) were included, with 43 in the graft failure group and 86 in the control group. The mean age of all cases was 22.4 years, with female patients accounting for 79.8% (103/129). All patients underwent MPFL-R. In addition, 64 knees (49.6%) were combined with tibial tubercle osteotomy, and 5 cases (3.9%) were combined with trochleoplasty. The average follow-up duration of all patients was 2.7 years. The 2 groups were well matched in terms of age, sex, number of dislocations, duration of follow-up, and primary procedures (all P > .05; Table 2).
Basic Characteristics of Patients and Comparisons of Key Variables Between the 2 Groups a

Values are presented as mean ± SD or number (%) unless otherwise indicated. CDI, Caton-Deschamps index; FAA, femoral anteversion angle; MPFL-R, medial patellofemoral ligament reconstruction; TTO, tibial tubercle osteotomy; TT-TG, tibial tuberosity–trochlear groove.
Time from first dislocation to surgery (months).
Abnormal proportions of bony parameters.
Reliability Analysis
The interrater reliability demonstrated highly consistent agreement (κ = 0.88) for the patellar jumping sign. For the measurement of bony structural abnormalities, the ICC was between 0.92 and 0.98 for interobserver reliability, indicating excellent measurement consistency (Appendix 2; see the online Video Supplement for this technique).
Risk Factors for Graft Failure
The incidence of preoperative jumping signs in the graft failure group was significantly higher than that in the control group (69.8% vs 18.6%, P < .001). Preoperative FAA (29.8° vs 21.5°, P < .001), knee torsion (14.3° vs 8.1°, P < .001), and TT-TG distance (21.2 vs 19.1 mm, P = .006) were greater in the graft failure group. There were no significant differences between the 2 groups in terms of trochlear dysplasia and patellar height. In addition, the number of knees with increased femoral anteversion (53.5% vs 14%, P < .001), knee torsion (62.8% vs 16.3%, P < .001), and TT-TG distance (67.4% vs 46.5%, P = .025) was also higher in the graft failure group than in the control group (Table 2).
Four variables were included in the multivariable regression analysis (Table 3). The results showed that jumping sign (OR, 4.44; 95% CI, 1.63-12.12; P = .004), increased femoral anteversion (OR, 6.23; 95% CI, 2.18-17.77; P = .001), and excessive knee torsion (OR, 4.18; 95% CI, 1.51-11.58; P = .006) were ultimately identified as independent risk factors for MPFL graft failure.
Logistic Regression Analysis on the Risk Factors of Graft Clinical Failure a
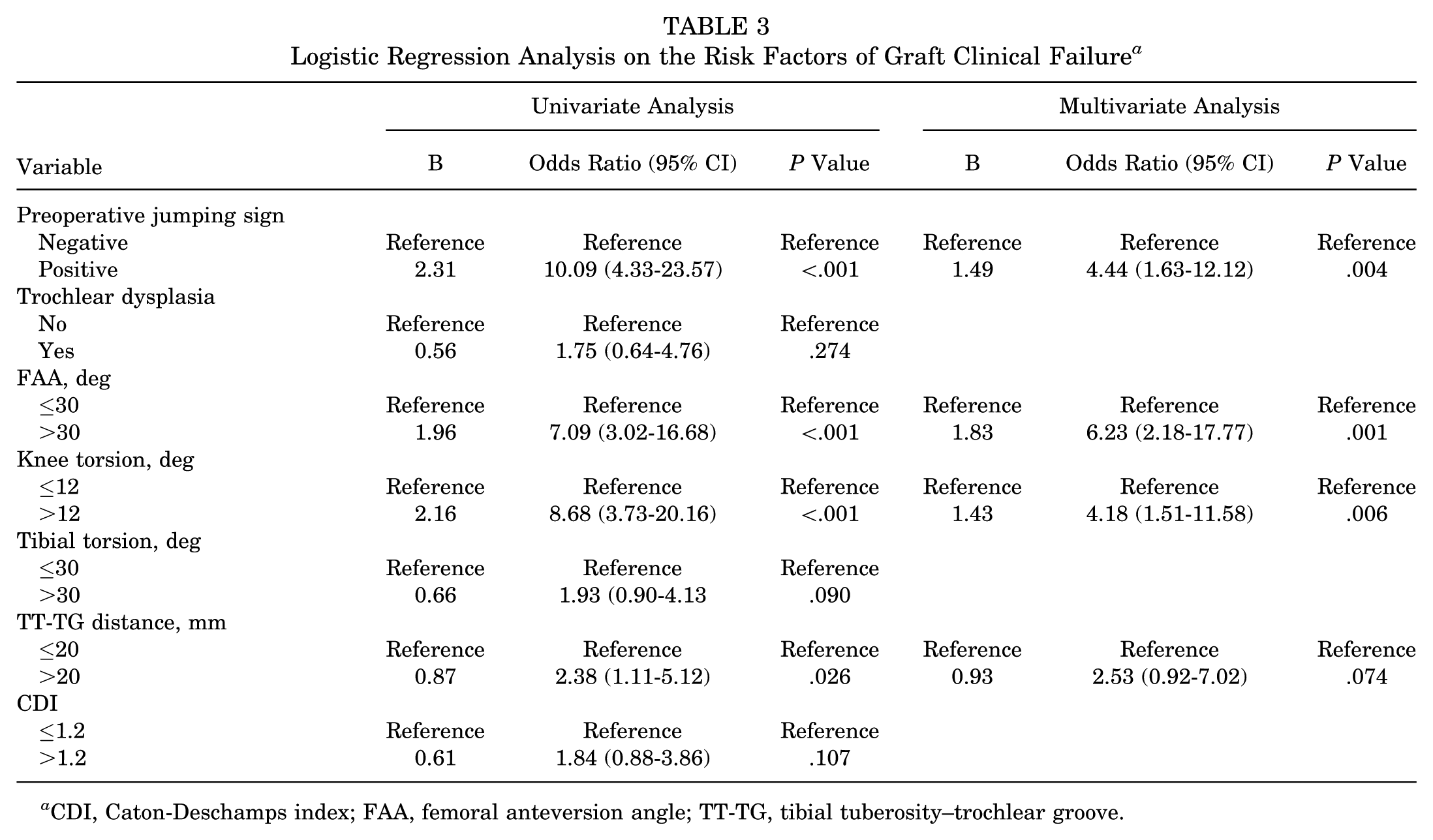
CDI, Caton-Deschamps index; FAA, femoral anteversion angle; TT-TG, tibial tuberosity–trochlear groove.
A nomogram was developed for the presentation of the final model. For a patient with jumping patella and increased femoral anteversion (>30°), the nomogram-predicted risk of recurrent dislocation at 2 years postoperatively was >70% (Figure 3A; calculations are as follows: jumping patella corresponds to 97.5 points, femoral anteversion >30° corresponds to 100 points, and knee torsion ≤12° corresponds to 0 points; total points = 197.5, indicating a >70% risk of recurrent dislocation at 2 years). The model resulted in a C-index of 0.832. Furthermore, the calibration curve plotted in Figure 3B evaluated the agreement between nomogram-estimated and observed risks. Both evaluation methods indicate good discriminative performance of the model.

Use and interpretation of a nomogram. (A) Vertical lines are drawn upward from covariate values (jumping sign, femoral anteversion angle, knee torsion) to determine point contributions (Points). The sum of these points (Total Points) is then projected downward to estimate the 2-year postoperative risk of recurrent patellar dislocation (Risk). (B) Calibration curve demonstrates agreement between predicted and observed outcomes. The gray line represents ideal calibration, the green line actual performance, and the blue dotted line bootstrap-corrected estimates (1000 resamples). (Note: Model fit was also assessed using the Hosmer-Lemeshow test, where P > .05 indicates adequate calibration.)
Table 4 presents the predicted risk and actual failure rate in patients with different combinations of risk factors. Among 58 patients without any risk factors, 2 experienced graft failure (2/58, 3.4%). In 33 patients with 1 risk factor, graft failure occurred in 9 cases (9/33, 27.3%). Among the 23 cases with 2 risk factors, the graft failure rate increased to 73.9% (17/23). Furthermore, in 15 patients with 3 risk factors, all experienced graft failure (100%). There was good concordance between the nomogram-predicted failure risk and the actual graft failure rate.
Predicted Risk and Actual Failure Rate in Patients With Different Combinations of Risk Factors a

FAA, femoral anteversion angle.
Based on the nomogram result.
Discussion
This study retrospectively reviewed patients with postoperative follow-up over a continuous 9-year period, minimizing selection bias as much as possible. Moreover, cases with femoral tunnel malposition were excluded to ensure that all enrolled patients underwent standardized procedures, to obtain relatively reliable analytical results. The most important findings of this study were (1) a preoperative jumping sign was present in almost 70% of patients with MPFL graft failure; (2) this sign, combined with excessive lower limb rotational abnormalities, was identified as associated with graft failure after primary MPFL-R in patients with RPDs. This study found that approximately 20% of patients in the control group exhibited a preoperative jumping sign, suggesting that the presence of this clinical sign does not predict graft failure with 100% accuracy. These findings may help surgeons easily identify high-risk patients with MPFL graft failure before surgery.
A recent study has shown that knees with a concomitant jumping sign exhibit a higher proportion of increased femoral anteversion (40.8% vs 24.4%, P = .004), excessive knee torsion (61.2% vs 15.3%, P < .001), pronounced supratrochlear spur (73.1% vs 32.3%, P < .001), and flatter lateral trochlear inclination (81.3% vs 27.5%, P < .001). 21 Another study suggested that the trochlear bump may contribute to the pathogenesis of this sign. 4 This suggests that the jumping sign is often associated with underlying bony structural abnormalities. The present study established a clear clinical association between the jumping sign and MPFL graft failure (OR, 4.4; P = .004). Although current clinical evidence cannot confirm whether bony abnormalities cause the jumping sign, the presence of a jumping sign warrants further investigation to evaluate associated osseous abnormalities. The resulting changes in treatment decisions may affect long-term clinical outcomes. Further prospective studies, such as cohort studies, are needed to validate these findings.
MPFL-R is the basic intervention for patients with RPD who require surgical management. Clinically, additional procedures may be performed to maintain the patellofemoral joint congruence and patellar tracking. Combined tibial tubercle osteotomy is frequently employed in cases with increased TT-TG distance, and this technique has been demonstrated to effectively reduce patellofemoral joint contact pressure and improve patellofemoral congruence.1,11 For patients with excessive femoral anteversion and high-grade patellar maltracking, distal derotational femoral osteotomy has shown superior clinical and radiologic outcomes, although it is associated with greater surgical trauma.24,27 In rare cases with severe tibial torsion, tibial derotational osteotomy has been proven to effectively improve the foot progression angle. 25 However, there is no consensus regarding the management of excessive knee torsion. A recent study reported that knee torsion showed no significant changes after femoral rotational osteotomy (10.2° vs 9.4°, P = ns), 9 suggesting that other surgical techniques should be explored to correct tibiofemoral rotation. Wang et al 22 recently found that for every 4° increase in knee torsion, there is a high likelihood of observing a higher grade of patellar maltracking. This finding indicates that additional surgical interventions could improve knee torsion by approximately 4°, thereby further optimizing patellar tracking and graft tension, potentially reducing the risk of graft failure.
The primary challenge of current patellar tracking classifications is to identify which pathologic tracking patterns require additional procedures beyond MPFL-R. A recent reliability study reported low interobserver agreement for both the quadrant method and Donnell classification (κ = 0.51 and 0.49, all <0.60). 7 This suggests that although individual observers maintain consistent standards when assessing patellar tracking, reproducibility between different observers is relatively poor, limiting the generalizability of treatment strategies based on these classification systems. The present study found that classifying patellar tracking using the jumping sign and gliding sign achieved higher interobserver agreement (κ = 0.88). This result is consistent with previous research. 21 Furthermore, this classification system encompasses a broader range of cases and provides more consistent treatment strategies, highlighting its clinical utility.
Femoral tunnel malposition is a well-established risk factor for unfavorable MPFL graft outcomes.8,16,28 To more rigorously investigate the predictive value of the jumping sign on clinical outcomes, a consistent femoral tunnel positioning method was used for all cases in this study. 15 Furthermore, all patients who actively participated in the follow-up were included, without intergroup matching, thereby minimizing the influence of selection bias on the case-control design. This study included 43 cases of MPFL graft failure over 11 years, making it the largest known retrospective study of MPFL-R failure in terms of sample size.
This study has limitations. This retrospective case-control study has inherent limitations in controlling all confounding factors between groups, particularly regarding the performance of tibial tubercle osteotomy and trochleoplasty. However, this study implemented propensity score matching to balance potential confounding variables across cohorts, thereby enhancing the reliability of findings to a meaningful degree. In addition, although this study design clearly demonstrated an association between jumping patella and graft failure, it does not allow for a definitive inference of causality.
Conclusion
A preoperative jumping sign was present in almost 70% of patients with MPFL graft failure. This sign, combined with excessive lower limb rotational abnormalities, was associated with graft failure after primary MPFL-R in patients with RPD.
Supplemental Material
sj-docx-1-ojs-10.1177_23259671251399799 – Supplemental material for Association Between Preoperative Patellar Jumping Sign and Graft Failure After Medial Patellofemoral Ligament Reconstruction for Recurrent Patellar Dislocation
Supplemental material, sj-docx-1-ojs-10.1177_23259671251399799 for Association Between Preoperative Patellar Jumping Sign and Graft Failure After Medial Patellofemoral Ligament Reconstruction for Recurrent Patellar Dislocation by Daofeng Wang, Yang Liu, Yanwei Cao, Tong Zheng, Zhijun Zhang and Hui Zhang in Orthopaedic Journal of Sports Medicine
Supplemental Material
sj-MTS-2-ojs-10.1177_23259671251399799 – Supplemental material for Association Between Preoperative Patellar Jumping Sign and Graft Failure After Medial Patellofemoral Ligament Reconstruction for Recurrent Patellar Dislocation
Supplemental material, sj-MTS-2-ojs-10.1177_23259671251399799 for Association Between Preoperative Patellar Jumping Sign and Graft Failure After Medial Patellofemoral Ligament Reconstruction for Recurrent Patellar Dislocation by Daofeng Wang, Yang Liu, Yanwei Cao, Tong Zheng, Zhijun Zhang and Hui Zhang in Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted September 15, 2025; accepted October 6, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by the National Natural Science Foundation of China (82472527). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Ethics Committee of Beijing Jishuitan Hospital (Ethics Number: 01-07-2018).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.