
Abstract
Background:
Patient-reported outcome measures (PROMs) are essential for assessing knee function; however, their complexity can hinder efficiency. The subjective knee value (SKV) offers a simple alternative, but lacks distinction between daily activities and sports.
Purpose:
We propose the SKV for daily activity (SKV-d) and sport (SKV-s). This study aimed to validate the SKV-d and SKV-s as simple and accurate tools for assessing knee function.
Study Design:
Cohort Study (Diagnosis); Level of evidence, 3.
Methods:
A total of 79 consecutive athletic patients (mean age, 39 years; 49% women) with knee-related issues were included and categorized into 4 groups between September and November 2024. PROMs were collected according to clinic standards: knee osteoarthritis (n = 21), Knee Society Clinical Rating System (KSS) (Knee Score and KSS Function), anterior cruciate ligament injury (n = 19), International Knee Documentation Committee subjective knee evaluation form (IKDC-S), patellar instability (n = 12), Kujala Anterior Knee Pain Scale (AKPS), and focal cartilage lesion or isolated meniscal tear (n = 27). Patients completed the SKV, SKV-d, and SKV-s, along with the validated scores mentioned above. Validity, reliability, floor/ceiling effects, and differences among the 3 single-item scores were assessed.
Results:
The SKV-s correlated strongly with the AKPS (rs = 0.71), moderately with the IKDC-S (rs = 0.64) and the KSS Knee Score (rs = 0.45), and weakly with the KSS Function (rs = 0.28). The SKV-d correlated moderately with the IKDC-S (rs = 0.65) and the AKPS (rs = 0.50), and weakly with the KSS Knee Score (rs = 0.15) and the KSS Function (rs = 0.22). The SKV strongly correlated with the SKV-s (rs = 0.83) and the SKV-d (rs = 0.81). The SKV-s was significantly lower than the SKV (46.8 ± 27.8 vs 66 ± 20.7; P < .001) and the SKV-d (46.8 ± 27.8 vs 73.7 ± 23.3; P < .001). The SKV-d was higher than the SKV (73.7 ± 23.3 vs 66 ± 20.7; P < .001). Reliability was good for the SKV (intraclass correlation coefficient [ICC], 0.80), the SKV-s (ICC, 0.86), and the SKV-d (ICC, 0.81), with no significant floor/ceiling effects except for the SKV-d.
Conclusion:
The SKV-d and SKV-s demonstrated acceptable validity with the SKV, the IKDC-S, and the AKPS, and were reliable, with significant differences between each other and the SKV. Both the SKV-d and the SKV-s may help distinguish between daily activities and sports and for assessing knee function in athletes; however, they should not replace commonly used PROMs.
Knee joint injuries and degenerative changes frequently lead to disability, significantly impairing patients’ quality of life.6,8,33 Therefore, evaluation of the knee joint is crucial, not only for improving the patient's symptoms but also for guiding treatment decisions and assessing return-to-sport potential.
Traditionally, physician-based scoring systems that emphasize the clinical component have been widely used.19,22 However, patient-centered assessment tools, which reflect the patient's perspective, have become increasingly important, offering a more direct and meaningful evaluation of knee function.5,9,11,21
Numerous scoring systems and patient-reported outcome measures (PROMs), such as the Knee Society Clinical Rating System (KSS), the International Knee Documentation Committee subjective knee evaluation form (IKDC-S), and the Kujala Anterior Knee Pain Scale (AKPS), have been validated and utilized to assess knee function and treatment effectiveness.1,10,12,13,17 Nevertheless, the implementation of these PROMs can be challenging because of their complexity and survey length.25,28 Thus, to address this issue and reduce the administrative load, single-item values, such as the subjective shoulder value (SSV), the subjective elbow value (SEV), and the Single Assessment Numeric Evaluation (SANE), although mostly for upper extremities, have been introduced and proven to be responsive, valid, and effective across various pathologies.7,24,29,32,34,35 Specifically for the knee joint, recent studies in the literature have demonstrated the subjective knee value (SKV) and the simple knee value as valid single-item tools for assessing knee function.20,26 In the original publication, patients were asked to rate their knee joints, with a completely normal knee representing 100% and a completely nonfunctional knee representing 0%.
Additionally, a patient's knee function following an injury or in the setting of degenerative change may be sufficient for activities of daily living but inadequate for participation in sports. Therefore, as recently demonstrated for the shoulder joint, a single-item scoring system that focuses on knee function during sports activities, as well as one separate for activities of daily living, could be beneficial, especially for recreational or professional athletes. 4
This study aimed to introduce the subjective knee value for daily activity (SKV-d) and for sports (SKV-s) as assessment tools for patients with knee disorders and to validate them against established PROMs used in clinical settings. We hypothesized that the SKV-d and SKV-s would yield distinct results from the SKV and also would differ from each other.
Methods
Study Design and Patient Selection
The local ethics committee approved this study (Zurich Cantonal Ethics Commission, BASEC-Nr. 2024-01722). Informed consent was obtained from each patient or their legal representatives. The research was performed entirely at the authors’ institution. A prospective clinical study was conducted—including all consecutive patients who visited our outpatient clinic for a knee-related issue between September 2024 and November 2024. The inclusion criteria were patients who (1) visited our outpatient clinic for the first time for 1 of the following knee problems, without having received any previous treatment: (a) knee osteoarthritis, (b) anterior cruciate ligament (ACL) injury (with or without accompanied ligamentous injuries), (c) patellar instability with or without history of dislocation, and (d) focal cartilage lesion or isolated meniscal tear; (2) regularly participated in sports at a recreational, competitive or professional level; (3) had no other knee surgeries on the affected knee; and (4) were able to complete simple questionnaires. The exclusion criteria included patients with (1) documented decline for data inclusion or no signed informed consent; and (2) musculoskeletal (other than knee disorders) or other health conditions that could significantly impair their ability to participate in sports.
Patients were categorized into 4 groups according to their diagnosis based on clinical and radiographical findings: (1) knee osteoarthritis; (2) ACL injury (with or without accompanying injuries); (3) patellar instability (with or without history of dislocation); and (4) focal cartilage lesion or isolated meniscal tear.
To determine the SKV, SKV-d, and SKV-s, all patients were asked to rate the condition of their affected knee on a scale from 100% (indicating no issues) to 0% (indicating a completely nonfunctional knee). Based on the questions originally used for the shoulder joint—both for daily activities 7 and sports 4 —the patients were verbally asked to answer the following questions: (1) “What is the overall percent value of your knee joint if a completely normal knee joint represents 100% and a completely nonfunctional knee joint represents 0%?” for SKV; (2) "Regarding the daily activities, what is the overall percent value of your knee joint, if a completely normal knee joint represents 100% and a completely nonfunctional knee joint represents 0%?" for SKV-d; and (3) “Regarding sports participation, what is the overall percent value of your knee joint, if a completely normal knee joint represents 100% and a completely nonfunctional knee joint represents 0%?” for SKV-s. In patients with chronic bilateral knee pathology, who had difficulty understanding “a completely normal knee joint,” the question was adapted to refer to another joint of the body that the patient felt was functioning normally. For example, (1) “What is the overall percent value of your knee joint if, for example, a completely normal elbow joint represents 100%?” To evaluate the reliability of the SKV, SKV-d, and SKV-s, all patients were asked to answer these questions twice: first during the initial consultation and again 2 weeks later by phone. Only patients whose clinical condition remained unchanged were included in the reliability analysis.
The survey included specific scoring systems according to our hospital's standards: the KSS for the knee osteoarthritis group, the IKDC-S for the ACL group, and the AKPS for the patellar instability group. Per institutional protocol, no full-length questionnaire was used for patients with a focal cartilage lesion or an isolated meniscal tear. The KSS, IKDC-S, and AKPS are routinely collected at our hospital either as part of the medical history or for quality control purposes. The KSS incorporates both clinical (KSS Score) and subjective components (KSS Function), with a total score ranging from 0 to 100, where 100 indicates normal knee function and 0 represents severe knee impairment.12,18 The IKDC-S assesses subjective knee function in patients with various knee conditions, with scores ranging from 100 (absence of symptoms) to 0 (severe symptoms).2,13,14 The AKPS is a subjective tool that evaluates symptoms and functional limitations related to anterior knee pain, with a score ranging from 100 (no pain or limitation) to 0 (severe pain and disability).3,17
Statistical Analysis
The primary objective of this study was to assess the validity of the SKV, SKV-d, and SKV-s by correlating them with validated knee-specific PROMs in the patient groups described above. Using the Fisher z approximation (2-sided α = .05; power = 0.80), a total of 79 patients provides the sensitivity to detect a correlation of approximately 0.31 (Spearman rank correlation = rs). The smaller sizes in each subgroup yield higher minimum detectable correlations (rs≈ 0.58 for the knee osteoarthritis group, rs≈ 0.60 for the ACL group, rs≈ 0.73 for the patellar instability group, and rs≈ 0.52 for the focal cartilage lesion or isolated meniscal tear group).
The collected data were analyzed using IBM SPSS 29 (IBM Corp). P < .05 was considered statistically significant. Frequency rates, means, and ranges were used to describe the baseline characteristics of patients. The normality of the distribution was tested using the Shapiro-Wilk and Kolmogorov-Smirnov tests, as appropriate.
To test the validity of the SKV-d and SKV-s, their correlation with the SKV—a previously validated score 26 —was assessed using the Spearman correlation coefficient, given the fact that these scores were not normally distributed. The correlations between the SKV, SKV-d, and SKV-s with the scores used in the subgroups (KSS for the osteoarthritis group, the IKDC-S for the ACL group, and the AKPS for the patellar instability group) were evaluated using the Spearman correlation coefficient. The correlation strength was interpreted based on the rs value as follows: extreme if the rs value was between 0.90 and 1, strong if it was between 0.70 and 0.89, moderately strong if it was between 0.40 and 0.69, weak if it was between 0.10 and 0.39, and negligible if it was between 0 and 0.10. 30
The Wilcoxon signed-rank test was used to compare the SKV, SKV-d, and SKV-s.
To assess reliability, a test-retest analysis was conducted. Patients were asked to answer the SKV, SKV-d, and SKV-s questions at their initial consultation (t0) and again after 2 weeks (t2w) via a phone call, assuming their knee condition remained unchanged. The intraclass correlation coefficient (ICC) (2-way random effects, absolute agreement, single measurement, 2,1) was calculated for the SKV, SKV-d, and SKV-s between t0 and t2w and interpreted according to Portney. 27
Floor and ceiling effects were assessed by calculating the proportions of responders who scored the lowest (0%) and highest (100%) possible values, respectively. A floor or ceiling effect was considered significant if >15% of the patients scored 0% or 100%, respectively. Proportions between 10% and 15% were considered moderate but acceptable, 5% to 10% minor, and <5% negligible.15,16
To calculate the threshold value of change in the SKV, SKV-d, and SKV-s that is considered clinically meaningful, the minimal clinically important difference (MCID) was determined using a distribution method. 23
Results
A total of 79 athletic patients (40 men, 39 women) participating in recreational or competitive sports, with a mean age of 39 years (range, 15-79 years), were included (Figure 1). Two patients were unavailable at the 2-week follow-up. No patient reported any change in their knee condition during the 2 weeks, as no therapeutic interventions were performed between the 2 assessments. According to their initial diagnosis, 21 patients (27%) were categorized into group 1 (knee osteoarthritis), 19 patients (24%) into group 2 (ACL injury), 12 patients (15%) into group 3 (patella instability), and 27 patients (34%) into group 4 (focal cartilage lesion or isolated meniscal tear). A sample size of 79 patients (2-sided α = .05, power = 0.80, using the Fisher z approximation) is sufficient to detect a correlation of approximately 0.31 across the entire cohort. Due to the smaller numbers of patients in each subgroup, the minimum detectable correlation was higher (rs≈ 0.58 for the knee osteoarthritis group; rs≈ 0.60 for the ACL group; rs≈ 0.73 for the patellar instability group, and rs≈ 0.52 for the focal cartilage lesion or isolated meniscal tear group). Baseline descriptive data and the SKV, SKV-d, and SKV-s values are demonstrated in Table 1.
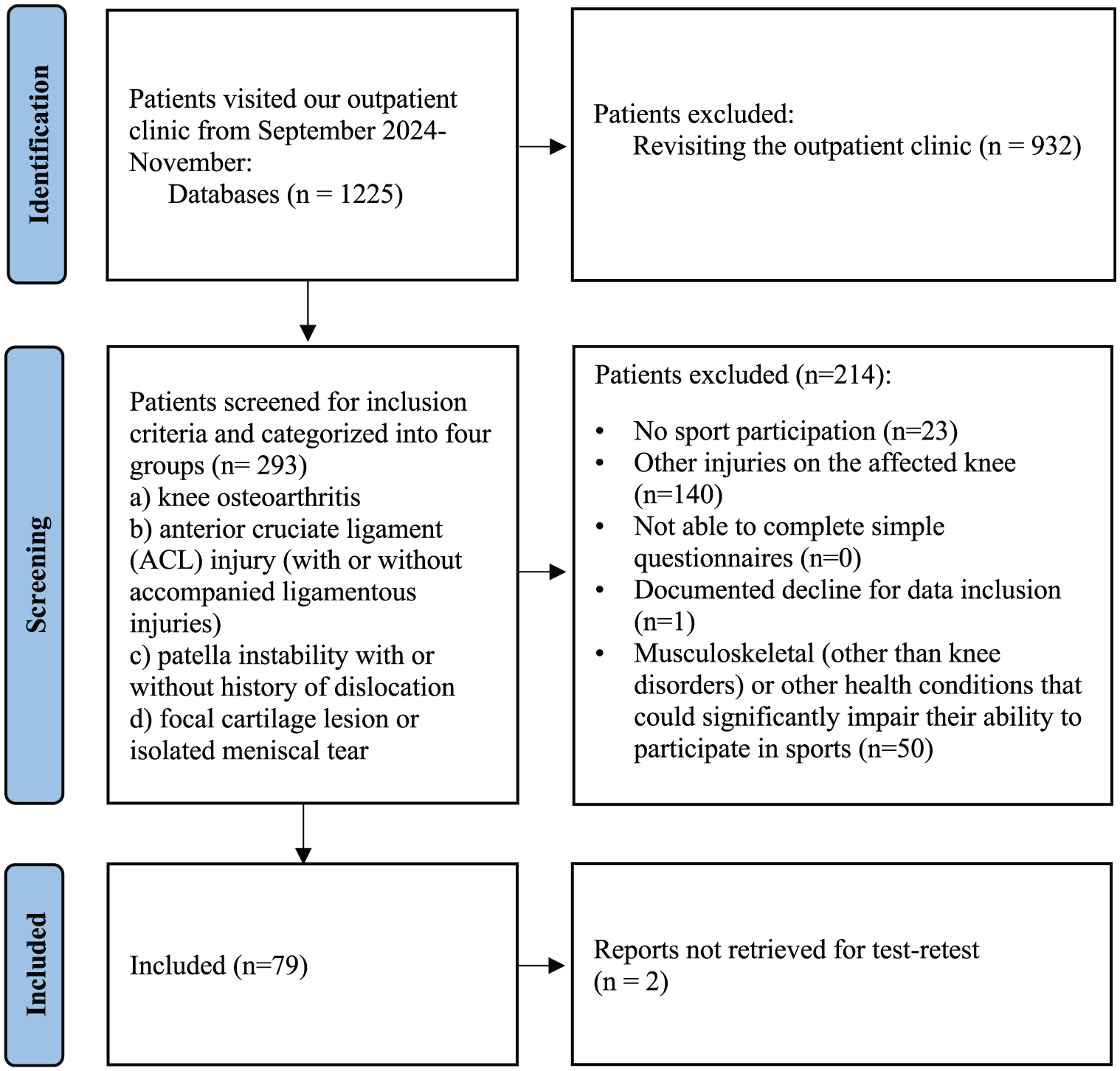
Flow diagram showing selection of patients.
Patient Characteristics a

Data are presented as mean (range) or mean (SD). ACL, anterior cruciate ligament; SKV, subjective knee value (%); SKV-d, subjective knee value for daily activity (%); SKV-s, subjective knee value for sports (%); t0, at the time of initial consultation in the outpatient clinic; t2w, at the 2-week follow-up.
Across the entire group, the SKV demonstrated a very strong and significant positive correlation with the SKV-d (rs = 0.81; P < .001) and the SKV-s (rs = 0.83; P < .001). A strong, significant positive correlation was also found between the SKV-d and the SKV-s (rs = 0.79; P < .001). Correlations of the SKV, SKV-d, and SKV-s with the KSS, IKDC-S, and AKPS are summarized in Table 2.
Correlation of the SKV, SKV-s, and SKV-d With Subgroup-Specific Scores Based on Diagnosis a

Results are presented as the Spearman correlation coefficient (P value in parentheses). AKPS, Kujala Anterior Knee Pain Scale (%); IKDC-S, International Knee Documentation Committee Subjective knee evaluation form; SKV, Subjective Knee Value (%); SKV-d, Subjective Knee Value for daily activity (%); SKV-s, Subjective Knee Value for sports (%).
For the entire study population, SKV-s values were significantly lower than both SKV (46.8 ± 27.8 vs 66 ± 20.7; P < .001) and SKV-d (46.8 ± 27.8 vs 73.7 ± 23.3; P < .001) values. Additionally, SKV-d values were significantly higher than SKV values (66 ± 20.7 vs 73.7 ± 23.3; P < .001) at the time of the initial consultation.
The SKV, SKV-d, and SKV-s showed strong reliability based on the test-retest method, both at the initial consultation and at the 2-week follow-up. Detailed information is provided in Table 3.
Reliability of the SKV, SKV-d, and SKV-s a

Data are presented as mean (SD) or mean (95% CI). ICC (2,1), intraclass correlation coefficient (2-way random effects, absolute agreement, single measurement); SKV, subjective knee value (%); SKV-d, subjective knee value for daily activity (%); SKV-s, subjective knee value for sports (%); t0, initial consultation; t2w, 2 weeks later.
Floor effects, defined as the percentage of patients with the lowest possible score (0%), were observed only in the SKV-s but were not significant. Ceiling effects, indicating the percentage of patients with the highest possible score (100%), were present in all 3 scores but were significant only for the SKV-d. Detailed results are demonstrated in Table 4.
Floor and Ceiling Effects a
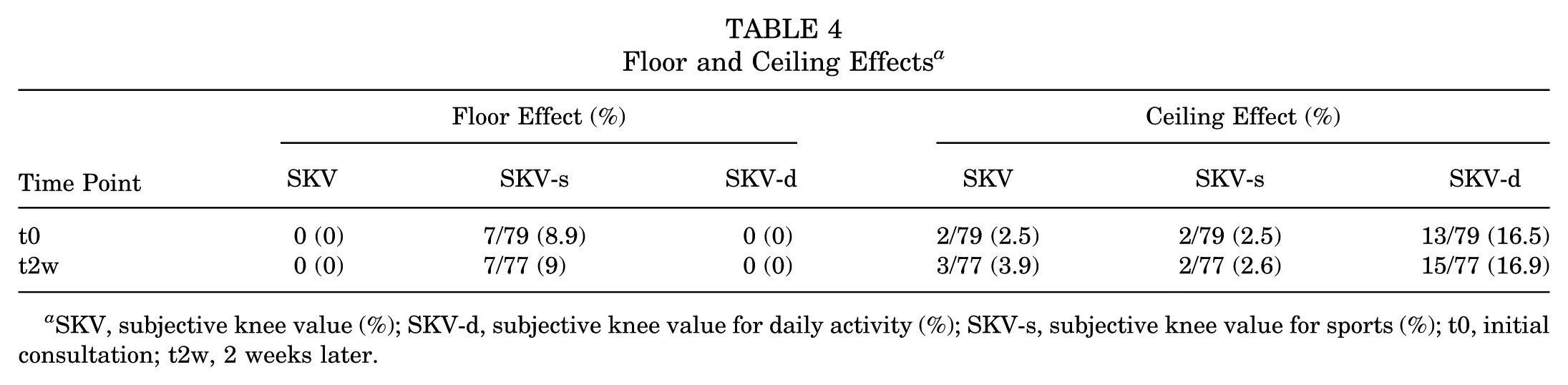
SKV, subjective knee value (%); SKV-d, subjective knee value for daily activity (%); SKV-s, subjective knee value for sports (%); t0, initial consultation; t2w, 2 weeks later.
For each of the 3 scores evaluated, the threshold value for a clinically meaningful change was calculated. The MCID values were 10.4 points for the SKV, 11.6 points for the SKV-d, and 13.9 points for the SKV-s, indicating that a change from 10 to 14 points on these scales would be required to detect a clinically meaningful improvement or deterioration in knee function.
Discussion
The most important finding of this study is that the SKV-d and SKV-s, as single-item tools assessing knee function in patients with knee disorders, showed a strong positive correlation with the SKV and demonstrated acceptable validity when correlated with the IKDC-S and the AKPS. However, their correlation with the KSS Knee Score and KSS Function was weak. All 3 scores—SKV, SKV-d, and SKV-s—proved to be reliable. However, all 3 scores showed a strong positive correlation with each other; the SKV-d and SKV-s yielded significantly different results both from one another and from the SKV, supporting the hypothesis that differentiation of knee function between daily activities and sports is possible and beneficial.
Assessing knee function in patients with knee disorders is essential for guiding clinical decisions, making scoring systems that capture the patients’ perspective highly valuable. A variety of self-administered PROMs have been developed, validated, and widely adopted in both clinical practice and for research purposes.1,10,12,13,17 However, the complexity and survey length of these PROMs often pose challenges, making them time-consuming and difficult for patients to complete.25,28 This, in turn, can negatively affect patients’ compliance and complicate score interpretation for physicians. To address these challenges, concise, straightforward outcome measures are desirable, highlighting the value of single-item tools developed for this purpose.7,29,34
The SANE score, specifically applied to the knee joint, has been used in patients with knee ligament injuries, showing a moderate to strong correlation with the IKDC-S and Lysholm scores,31,35,36 as well as moderate correlations with other knee-specific PROMs. 24 Most recently, the SKV, presented by Plachel et al, 26 demonstrated a strong correlation with the Knee injury Osteoarthritis Outcome Score and the IKDC-S in common knee disorders, corroborating the results of Marot et al.20,26 In our prospective study, the SKV-d and SKV-s showed a strong positive correlation with SKV and a moderately strong correlation with the well-established IKDC-S and AKPS, in contrast with the previous literature, which reported the correlation of the SKV. However, both the SKV-d and the SKV-s showed only a weak correlation with the KSS Knee Score and KSS Function. A possible explanation is that the KSS includes both a clinician-assessed component and a subjective component, potentially diluting the direct relationship with purely patient-reported outcomes. Notably, given the total sample size, the study was adequately powered to detect weak correlations in the overall cohort (rs≈ 0.31) and moderate-to-strong correlations within the smaller subgroups (rs≈ 0.58 for the knee osteoarthritis group, rs≈ 0.60 for the ACL group, rs≈ 0.73 for the patella instability group, and rs≈ 0.52 for the focal cartilage lesion or the isolated meniscal tear group). Due to smaller subgroup sample sizes, subgroup analyses had lower statistical power; thus, weaker or nonsignificant correlations may reflect limited sample sizes rather than a lack of correlation and should be interpreted cautiously.
For a scoring system to be reliable, its results must remain consistent in patients whose condition does not change over time. 32 Our findings show that both the SKV-d (0.81 [95% CI, 0.71-0.87]) and the SKV-s (0.86 [95% CI, 0.79-0.91]), as well as the SKV (0.80 [95% CI, 0.70-0.87]), are reliable at both the initial consultation and after 2 weeks. This supports the idea that these scores remain unchanged when the knee joint condition remains constant, which aligns with existing literature on the simple knee value 20 and other studies assessing single-item scores for other joints, such as the shoulder and elbow.7,29
Floor and ceiling effects are important factors to consider when validating a scoring system. Consistent with the existing literature, both the SKV and the SKV-s demonstrated no significant floor or ceiling effects, indicating that these scores can capture variability across a patient cohort. In contrast, the SKV-d showed a significant ceiling effect at both baseline and after 2 weeks. This could be interpreted by the fact that athletic patients with knee issues may still be able to perform daily activities without difficulty, leading to an underestimation of the knee condition when only the SKV-d is considered.
Notably, the SKV does not differentiate between daily activities and sports participation, leaving it unclear how patients interpret this score and whether they assess their knee function based on daily activities, sports participation, or a mix of both. For instance, for the shoulder joint, a recent study by Descamps et al 4 highlighted a significant difference between the SSV and SSV-Sport in patients participating in recreational or competitive sports, concluding that the SSV-Sport is better suited than the SSV for assessing pre- and postoperative shoulder function in athletes. Similarly, our findings highlighted significant differences between the SKV-d, SKV-s, and the original SKV in a cohort of athletic patients. On average, the SKV-d was 7.7 points higher than the SKV and 26.9 points higher than the SKV-s, while the SKV-s was 19.2 points lower than the SKV. These results suggest that the SKV and SKV-d may overestimate knee function in athletic patients whose goal is to return to sports, where persistent knee function problems are likely to occur. The differences between the scores indicate a clear distinction between a score focusing on knee function during daily activities (SKV-d), a score emphasizing knee function during sports (SKV-s), and a more generalized or averaged assessment provided by the original SKV, which appears to integrate both aspects. This supports the idea that the SKV may serve as a global measure encompassing both domains, and the SKV-d and SKV-s could serve as its subcomponents, providing a more precise evaluation of knee function based on the different demands of daily life and sports participation.
From a practical standpoint, these differences have important implications for decision-making regarding therapeutic recommendations. For example, a patient may have a knee condition that allows them to perform activities of daily living—reflected in a high SKV-d and even SKV score—but impairs them in sports activities, leading to a low SKV-s score. Relying solely on the SKV and SKV-d in such cases, when the patient's primary goal is returning to sports, could lead to a misinterpretation of their therapeutic needs.
The present study should be interpreted in light of its potential limitations. First, while we evaluated several aspects of the validation process, we did not assess the responsiveness of the SKV-d and SKV-s. Second, we did not investigate their ability to detect changes, either improvement or worsening of the knee function after treatment. These scores may have potential as efficient instruments for tracking changes over time, offering a practical alternative when frequent use of longer PROMs is not feasible. This remains an important area for future research. Third, despite the total sample size providing adequate sensitivity to detect weak correlations, the subgroup sizes were modest, with larger corresponding minimum detectable correlations. Therefore, subgroup analyses may be underpowered for small to moderate effects and should be interpreted with caution. Fourth, the short interval between the 2 evaluations (2 weeks) used to assess test-retest reliability could have influenced the results. However, a longer interval would have increased the risk of clinical change in the patients’ knee condition due to the initiation of conservative or surgical treatment, making a reliable comparison impossible. Last, neither the SKV-d, SKV-s, nor the SKV provides information on the underlying cause of the knee condition or the reason for the consultation. As a result, these scores cannot be used alone for clinical decision-making and are not a substitute for established PROMs.
Conclusion
The SKV-d and SKV-s demonstrated acceptable validity with the SKV, IKDC-S, and AKPS, and were reliable, with significant differences between the SKV-d and SKV-s. Both the SKV-d and the SKV-s may help distinguish between daily activities and sports and for assessing knee function in athletes; however, they should not replace commonly used PROMs.
Footnotes
Acknowledgements
The authors would like to thank and acknowledge Ms Nathalie Kuehne for her dedicated work as a study nurse and for her valuable support in submitting the ethics application.
Final revision submitted October 15, 2025; accepted October 27, 2025.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical review and approval for this study were obtained from the local ethics committee (Zurich Cantonal Ethics Commission, BASEC-Nr. 2024-01722).