
Abstract
Background:
A novel retropatellar tendon implant (LIFT) that is fixed deep to the patellar tendon proximal to the tibial tubercle may provide patellofemoral offloading benefits.
Purpose/Hypothesis:
The purpose of this study was to analyze the patellofemoral contact pressures from 0° to 60° of knee flexion in 3 states: (1) intact knee, (2) knee with the implantation of a retropatellar tendon implant, and (3) knee with a 45° anteromedialization tibial tubercle osteotomy (TTO). It was hypothesized that the implant would significantly reduce the contact pressure between the patella and trochlea compared with the intact state and produce a similar offloading effect as an anteromedializing TTO.
Study Design:
Controlled laboratory study.
Methods:
Trochlear pressure sensors were placed in 7 cadaveric knees (6 donors). Patellofemoral contact area, contact pressure, peak force, and center of force were measured using a model for native quadriceps force on the patella. On each specimen, measurements were taken in an intact state, after implantation of a novel retropatellar tendon implant, and after a 45° anteromedializing TTO. Force data were collected from 0° to 60° of flexion in 15° increments and normalized to each specimen's intact state.
Results:
Compared with the intact and implant groups, the TTO reduced the contact area at 30°, 45°, and 60° of flexion. TTO reduced contact pressure compared with intact from 15° to 60° of flexion, and reduced contact pressure at 15° when compared with the implant. The implant reduced the contact pressure compared with the intact state at 30° and 45° of flexion. For peak force, TTO reduced the force seen in 15° to 60° of flexion compared with the intact condition, while outperforming the implant at 15° of flexion. The implant reduced the peak force compared with the intact condition at 30° of flexion. Center of force analysis revealed that the implant medialized the center of force at 45° and 60° of flexion.
Conclusion:
The main finding from our biomechanical cadaveric study was that the novel retropatellar tendon implant did not reduce patellofemoral contact area, contact pressure, and peak force as much as a 45° anteromedializing TTO. The implant does reduce peak and contact pressures in early degrees of knee flexion compared with native states.
Clinical Relevance:
An implant that allows for offloading patellofemoral contact pressures without the morbidity, complication profile, or postoperative rehabilitation associated with a TTO may aid in the treatment of patellofemoral chondral lesions and retropatellar knee pain.
Keywords
Focal cartilage defects in the knee are a common source of debilitating pain, especially in the young, active population. 10 In the patellofemoral region, joint reactive forces can reach up to 6.5 times body mass in flexion. 12 For symptomatic lesions, nonoperative treatment is typically pursued first, which includes a combination of bracing and physical therapy.
If nonoperative management of patellofemoral defects fails, surgical treatment is typically individualized based on skeletal maturity, lesion characteristics, and the chronicity of the condition. Options for operative management include chondroplasty, microfracture, patellofemoral arthroplasty, and cartilage restoration procedures, such as osteochondral allografts, matrix-induced autologous chondrocyte implantation, or a concomitant offloading tibial tubercle osteotomy (TTO).5,9,11,21,23 An anteriorizing TTO offloads the patellofemoral joint by reducing the sagittal force vector produced by the patellar tendon on the patella by anteriorizing the tibial attachment of the patellar tendon.1,7,8,14,25 Direct anteriorization is often performed with the Maquet technique, 16 elevating the tibial tubercle with a bone graft to offload the patellofemoral and medial-sided patellar defects in patients with nonpathologic tibial tubercle to trochlear groove (TT-TG) distances. 24 Most anteriorizing TTOs are accompanied by some component of medialization, with the most common Fulkerson technique sliding the osteotomy along a predetermined anteromedializing plane. Anteromedialization is performed to preferentially offload the distal lateral patellofemoral joint in patients with increased lateral pressure. In a previous in vitro biomechanical test, Lamplot et al 14 demonstrated decreased patellar contact pressure in the 40° to 70° of flexion after the addition of an anteromedializing TTO in a simulated model of trochlear dysplasia. 14 Similarly, Beck et al 1 measured the change in trochlear contact pressure with a Fulkerson osteotomy, also finding a decrease in contact pressure after osteotomy.
Although TTO can help offload patellofemoral cartilage pathology,4,21 the procedure involves an osteotomy and extensive rehabilitation, with a risk of postoperative complications such as hardware irritation, postoperative stiffness, osteotomy nonunion, periosteotomy fracture, or infection.2,19,28 Alternative methods to avoid an osteotomy while simultaneously offloading the patellofemoral joint would reduce the morbidity and postoperative rehabilitation process for these patients. One proposed alternative solution is a retropatellar tendon implant (LIFT; ZKR Orthopedics) that is fixed proximal to the tibial tubercle, deep to the patellar tendon, thus lifting the patellar tendon and potentially reducing the sagittal force on the patella in a manner similar to an anteriorizing TTO. Clinical results for this implant are not yet available; however, the implant's potential to decrease patellofemoral contact pressures makes it an intriguing option.
This study aimed to analyze the patellofemoral contact pressures from 0° to 60° of knee flexion in 3 states: (1) intact knee, (2) knee with the implantation of the retropatellar tendon implant, and (3) knee with a 45° anteromedialization TTO. We hypothesized that there would be no difference in the effects of the implant and TTO on patellofemoral contact pressure measurements and locations.
Methods
Specimen Preparation
Institutional review board approval was not required for this study due to the use of deidentified cadaveric tissue. Seven cadaveric knees (6 donors) from mid femur to toe tip, and a mean age of 68 ± 15.5 years old were obtained. The exclusion criteria included metastatic cancer, traumatic injury or surgery of the lower limbs, and grade 4 cartilage defects in the patellofemoral joint. Metastatic cancer was excluded for bone quality purposes, and grade 4 cartilage defects were excluded due to concerns that they might confound our pressure-sensing model. Each knee underwent a computed tomography (CT) (BrightSpeed; GE Healthcare) scan in the axial, coronal, and sagittal planes. The quadriceps were tensioned before scanning using a Krackow stitch through the rectus femoris connected to a 1-kg sandbag suspended over the end of the imaging table. The knees were placed in extension in the CT scanner with the foot fixed to the base of the bed, ankle in neutral dorsiflexion, and the great toe pointed directly vertical. 13 TT-TG and sagittal TT-TG were measured on CT and found to be within nonpathologic range at a mean of 15.9 ± 3.3 mm and 5.9 ± 2.4 mm, respectively, with a positive sagittal value denoting the tibial tubercle to be anterior to the trochlear groove.3,15 All specimens were stored at −20°C and thawed at room temperature before imaging and testing.
After scanning, the skin and subcutaneous fat were dissected from the mid femur to the tibial tubercle. Further dissection was performed to isolate the vastus medialis, vastus intermedius, vastus lateralis, and rectus femoris as previously described in the literature. 26 Once isolated, all other musculature proximal to the joint line was transected off the femur and removed. Care was taken to leave the joint capsule intact. For each quadriceps muscle, a No. 5 suture was used to perform a Krakow stitch with 3 throws on each side, and the free ends were left proximally for loading each quadriceps muscle individually. The rectus femoris and vastus intermedius were sewn together and prepared with 1 Krakow stitch.
Each specimen was placed in a custom jig with a clamp on the mid-femur, securing the knee in place so that the femoral intercondylar axis was parallel to the floor. To provide 3-vector loading of the extensor mechanism, the free ends of the Krakow sutures were each tied to 16-pound weights, which were draped over a horizontal wood rod acting as a fixed pulley, applying 71.17 N of force to each of the 3 heads of the quadriceps vectors as previously described.26,29 The ankle was dressed and casted, fixing the ankle in neutral dorsiflexion. The foot was allowed to rotate freely in an internal/external motion, and the thigh-foot progression angle was measured after the tibia was restrained in 15° increments of flexion from 0° to 60°. Flexion angles of 0° to 60° were chosen to include the full range of patellar engagement into the trochlea before losing the distal contact force seen with further flexion. All flexion angles were measured with a handheld goniometer.
Patellofemoral Contact Measurement
Patellofemoral joint contact pressures were measured using the K-Scan 4000 sensor (Tekscan). The K-Scan 4000 is a thin-film pressure sensor designed specifically to obtain pressures in the knee and includes 2 separate sensors (33 × 27.9–mm each, with a sensel density of 62 sensels/cm2) with simultaneous recording. Before testing, each sensor underwent 2-point calibration per the manufacturer's recommendation. The sensors were rated for a 1500 psi range and calibrated at the midpoint of the 2 levels.
To secure the pressure sensors on the trochlea, a lateral retinacular release was performed to evert the patella, thereby gaining access to the trochlea. The 2 sensor pads were placed adjacent to each other along the deepest aspect of the trochlear groove, with the most proximal aspect of the sensors aligning with the proximal trochlea. These sensors were fixed using 2 staples proximally through the osseous aspect of the femur and 2 staples distally through the cartilaginous condyles. Care was taken to ensure that both the medial and lateral sensors lay flat against the medial and lateral trochlea with minimal overlap at the trochlear groove (Figure 1). The lateral release was not closed at any point and was left unrepaired throughout all tests.
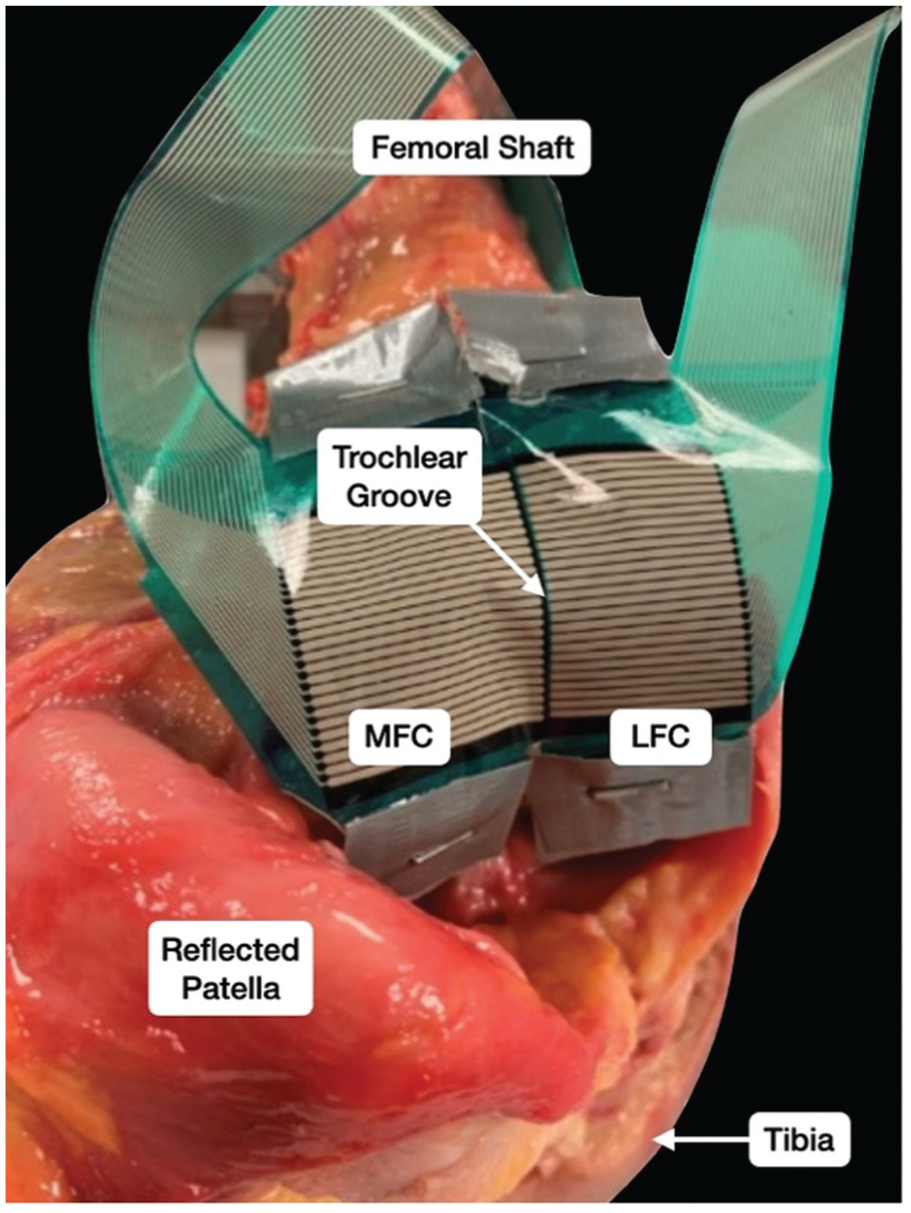
Placement of the retropatellar pressure sensors secured to the trochlea with staples. The edges of the 2 sensors meet directly over the trochlear groove. LFC, lateral femoral condyle; MFC, medial femoral condyle.
Testing Procedure
To initiate testing, each specimen was passively moved to 0° of flexion and secured with a transverse rod under the tibia to maintain full extension. Specimens were allowed to rest in a natural internal/external rotation state, and the direction of the muscle loading vectors was confirmed to be anatomically accurate with respect to the quadriceps muscles. Pressure data were subsequently recorded and saved using I-Scan software (Tekscan, Inc). After recording at 0°, the knee was passively moved through 60° of flexion, stopping at each of 15°, 30°, 45°, and 60° of flexion for data collection in a similar manner. After testing 1 complete round through a full range of motion, the knee was passively moved back to 0° for 2 more complete range of motion trials, for a total of 3 test series on each specimen.
The retropatellar tendon implant was then placed by the senior author (A.B.Y.) using a lateral parapatellar tendon approach (Figure 2). The same size implant was used for all specimens. A 3-cm incision was made just lateral to the patellar tendon and just proximal to the tibial tubercle. A custom device inserter (ZKR Orthopedics) was fastened to the implant and used to guide the implant between the tibia and patellar tendon. The implant was placed with its distal edge adjacent to the proximal ridge of the tibial tubercle. The lateral edge of the patellar tendon was aligned with the apex of the angled implant. Guide pins secured the implant to the tibia while 3 drill guide holes were made, 2 laterally and 1 medially. The implant was then secured in this position with three 2.9-mm screws. The lateral parapatellar tendon approach was not closed after implant placement. The testing was then repeated 3 times through the same flexion range as the intact group. The implant was removed, and the senior author then used a commercial guide (Arthrex T3 AMZ) to perform a 45° TTO with the foot in 0° of external rotation. The TTO was then translated anteromedially 10 mm along the 45° osseous cut and fixed with two 4.5-mm bicortical screws for anteromedialization of the tubercle (Figure 3). A translation of 10 mm was chosen to match the 10-mm apex of the retropatellar tendon implant, as well as to match a common translation and degree of anteromedialization used in the senior author's clinical practice. Testing was again repeated through 3 complete cycles, collecting contact pressure maps at all degrees of flexion.

(A) Extensive soft tissue release with no tension on the quadriceps vectors to visualize the placement of the implant directly proximal to the tibial tubercle with the knee in 90° of flexion. (B) Anterior-posterior view of the implant with tension on the quadriceps during testing state with the knee in 90° of flexion. Note that the lateral edge of the patellar tendon is aligned with the lateral apex of the angled implant, and no additional soft tissue disruption is needed compared with TTO. (C) Lateral view of the implant with the necessary soft tissue release for pressure sensor placement with the knee in 15° of flexion.

A left knee after a 45° anteromedializing osteotomy translating the tibial tubercle 10 mm anteromedially and fixed with 2 bicortical 4.5-mm headed screws.
Each set of pressure maps was analyzed for contact pressure, contact area, peak force, and center of force produced by the patella contacting the pressure sensors on the trochlea. Pressures produced from soft tissue effects were omitted from the analysis. The mean of the 3 tests at each degree of flexion was calculated for each specimen at each stage. To account for specimen variability, these mean values from the implant and TTO states were normalized with respect to their corresponding intact value. Thus, results were presented as percentages of the implant and TTO compared with the intact state of the specimens.
Statistical Analysis
All statistical analyses were performed in R Studio (RStudio; Version 2024.09.1; Posit). Contact area, contact pressure, and peak force data were obtained for each specimen in each of the 3 states. Measurements were taken 3 times each, averaged, and normalized as a percentage of the intact state for final analysis. Repeated measures analysis of variance (ANOVA) was performed to elucidate differences between states and at each flexion angle with respect to contact area, contact pressure, peak force, and center of force of the patella on the trochlea. When significance was achieved, a post hoc Tukey test was used to determine differences between states. Normalized values are presented as a percentage change ± standard deviation from the specimens’ intact state.
Results
Seven specimens from 6 donors underwent tests to measure patellofemoral contact pressures through 0 to 60° of flexion in 3 states: (1) intact, (2) with a retropatellar tendon implant, and (3) after a 45° 10 mm anteromedialization TTO. The mean donor age and body mass index were 68 ± 15.5 years and 22.7 ± 1.7 kg/m2, respectively. The mean TT-TG and sagittal TT-TG measured on pretesting CTs were 15.9 ± 3.3 mm and 5.9 ± 2.4 mm, respectively. Of the 7 specimens, 6 were from male donors and 4 were left knees. All knees were examined to confirm the absence of grade 4 patellar and trochlear cartilage defects.
Contact Area, Contact Pressure, and Peak Force Through Flexion
The 7 specimens were cycled from 0° to 60° of flexion 3 times each, and values were averaged and recorded. Three of the specimens exhibited no patellofemoral contact pressure at 0° of flexion after performing a TTO, with one of these specimens also exhibiting no contact pressure at 0° after retropatellar tendon implant placement. However, all had slight contact pressure in the intact state. This effect resulted in increased standard deviations at 0° of flexion, as these zero values of patellofemoral contact pressure were included in the analysis. Figure 4A demonstrates the increase in contact area through flexion. A significant increase was observed in contact area in the intact state from 0° to 30° (P = .004), 45° (P < .001), and 60° (P < .001). Likewise, there is a significant increase in contact area in the intact state from 15° to 45° (P = .001) and 60° (P < .001) of flexion. The same trends are evident in both the implant and TTO curves. Figure 4B shows the increase in contact pressure, with significant increases in the intact state, between 0° and 15° (P < .001), 30° (P < .001), 45° (P < .001), and 60° (P < .001). The TTO group demonstrated the same trends as the intact group; however, the implant group did not experience a significant increase in contact pressure through flexion. This is likely due to the increased contact pressure at 0° of flexion compared with the other groups. Figure 4C shows the increase in peak force through flexion with significant increases in the intact state from between 0° to 15° (P = .007), 30° (P = .014), 45° (P = .026), and 60° (P = .003). Again, the TTO group followed the same trends as the intact group, while the ZKR group did not have a significant increase in peak force through flexion, with a higher peak force at 0° of flexion. Figure 5 demonstrates a representative example of a typical pressure map montage, with blue indicating lower pressure and red representing the maximum pressure within the calibrated sensor range.

(A) Contact area (mm2) through 0° to 60° of flexion for all 3 groups. (B) Contact pressure (kg/cm2) through 0° to 60° of flexion for all 3 groups. (C) Peak force (N) through 0° to 60° of flexion for all 3 groups.

Representative sample of 1 specimen's pressure map. The top of each image is the most proximal aspect of the trochlear cartilage, and the bottom of each image is the distal edge of the pressure sensor. Top row: Trochlear pressure map in the intact state. Middle row: Trochlear pressure map after retropatellar implant placement. Bottom row: Trochlear pressure map after removal of the implant and a successful 45° Fulkerson osteotomy translating the tibial tubercle 10 mm anteromedially. Columns read from left to right as different flexion angles: 0°, 15°, 30°, 45°, and 60°.
Comparisons of Contact Area, Contact Pressure, and Peak Force
All specimens completed testing with 0° of flexion, demonstrating increased variability within groups due to 1 retropatellar tendon implant and 3 TTOs lacking patellofemoral contact after intervention. However, all specimens exhibited patellofemoral contact pressure in ≥15° of flexion. Each specimen was cycled through 3 rounds of testing in all 3 states. Patellofemoral contact area, contact pressure, and peak force were averaged over the 3 tests. The mean intact values for each outcome were recorded and set to 100% for each specimen. The mean implant and TTO values were normalized to each individual specimen's intact mean and expressed as a percentage increase/decrease compared with the respective intact group. This was done to eliminate inter-specimen variability in contact area, contact pressure, and peak force, as shown in Figure 4, which is likely due to specimen-specific patellofemoral geometry, cartilage health, and variations in testing.
Repeated-measures ANOVA for the normalized contact area, contact pressure, and peak force revealed significant differences across the 3 testing conditions at flexion angles of ≥15°.
Contact Area
The contact area was calculated as the total area of contact between the patella and trochlea. Due to specimen variability in intact anatomy, all values were analyzed as a normalized ratio with respect to their intact specimen value. The contact area moved distally and increased throughout flexion as the patella fully engaged with the trochlea. No statistically significant differences were found among normalized values of patellofemoral contact area at 0° or 15° of flexion. At 30°, 45°, and 60° of flexion, the TTO reduced the contact area significantly more than both the intact and implant groups. No significant differences in contact area were observed between the intact and implant groups at any degree of flexion (Figure 6).

The normalized contact area, expressed as a percentage of each specimen's intact group (100%), was averaged across specimens. Significant differences between specific groups are denoted with a line.
Contact Pressure
The contact pressure was calculated as the total force exerted by the patella on the trochlear pressure sensor, divided by the contact area, and is depicted through flexion angles in all 3 groups. The contact pressure significantly increased from 0° to 15°, then remained relatively constant from 15° to 60° (Figure 4B). No differences were found between the groups with respect to normalized contact pressures at 0° of flexion. At 15° of flexion, the TTO group exhibited lower normalized contact pressure compared with both the intact and implant groups. Both the retropatellar tendon implant and TTO groups significantly reduced normalized contact pressures compared with the intact state at 30° and 45°. At 60°, the implant trended toward significance (P = .078), while the TTO significantly reduced the normalized contact pressure compared with the intact state (Figure 7).
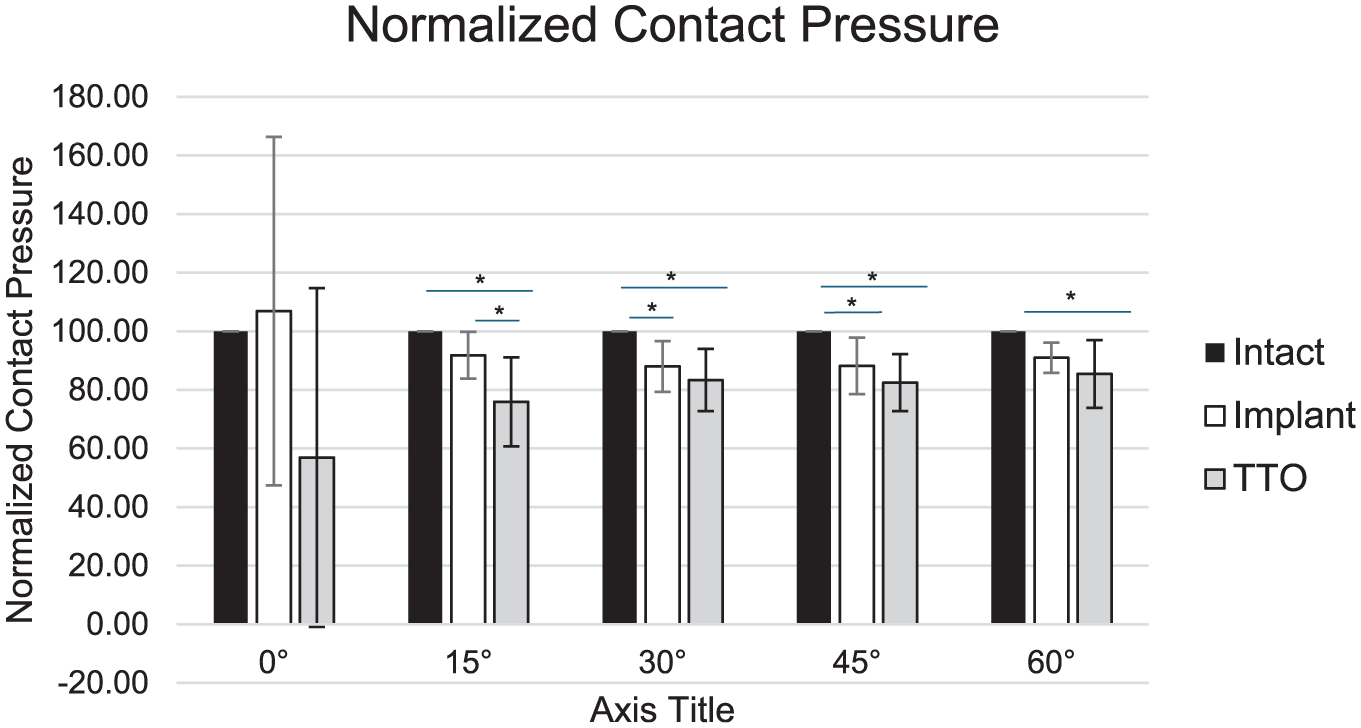
Normalized contact pressure, expressed as a percentage of each specimen's intact group (100%), was averaged across specimens. Significant differences between specific groups are denoted with a line and an asterisk.
Peak Force
The mean normalized peak force was calculated for each group at every degree of flexion and could appear anywhere on the trochlear pressure map as the patella engaged (Figure 8). The peak force was measured as the value (N) of the single voxel on the pressure sensor with the highest force. The peak force moved distally through flexion as the patella engaged in the trochlea. In early flexion, the patella generally exhibited an edge loading effect on the trochlea as it entered the trochlear groove, as seen in the intact 15° state of Figure 4. Similar to contact pressure, peak force significantly increased from 0° to 15° before staying relatively constant from 15° to 60°. Again, at 0°, there were no significant differences between the groups. The TTO group resulted in a statistically significant reduction of peak force compared with both the intact and implant groups at 15°. Both the implant and the TTO reduced the peak force compared with the intact group at 30° of flexion. At 45° and 60°, the implant did not produce a significant reduction in peak force compared with the intact group, whereas the TTO did demonstrate a significant decrease in peak force. At 45° and 60°, there was no significant difference in the peak force produced by the TTO and the implant groups (Table 1).

The peak force, expressed as a percentage of each specimen's intact group (100%), was averaged across specimens. Significant differences between specific groups are denoted with a line and an asterisk.
Pairwise Comparison of Normalized Peak Force with the Tukey Test a

Bold P values indicate statistical significance. TTO, tibial tubercle osteotomy.
Center of Force
The location of the center of force (COF) of the patella on the trochlear pressure map through all degrees of flexion is demonstrated in Figure 9. As the knee moves into flexion, the patella moves its COF distally and medially. As seen in Table 2, the ANOVA analysis of medial/lateral motion throughout the flexion cycle revealed differences between the groups at 45° (P = .028) and 60° (P = .026), with a trend toward significance at 15° (P = .098) and 30° (P = .057). At 30° of flexion, there was a trend toward the TTO medializing the COF compared with both the intact group (P = .090) and the implant group (P = .089). At 45° of flexion, the TTO medializes the COF compared with the intact state (P = .047) and trends toward significantly medializing the COF compared with the implant (P = .051). At 60° of flexion, the TTO medializes the COF compared with the implant only (P = .020). There were no significant differences in the proximal-distal COF relationship between any of the 3 groups.

Center of patellofemoral force through flexion. Greater x-axis values represent greater medialization of the center of force. Lower y-axis values demonstrate distalization of the center of force.
ANOVA for Medial/Lateral Center of Force a

Data are presented as mean ± SD. Bold P values indicate statistical significance. Values indicate differences (in mm) from the intact condition. Positive values indicate a more medial position. ANOVA, analysis of variance; TTO, tibial tubercle osteotomy.
Discussion
The main finding from our biomechanical cadaveric study was that a novel retropatellar tendon implant (LIFT; ZKR Orthopedics) reduces peak and contact pressures in early degrees of knee flexion compared with native states, although at a lower capacity than a 45° anteromedializing TTO. In particular, the retropatellar tendon implant significantly reduces contact pressures at 30° and 45° of flexion compared with the same knee without an implant, and reduces peak force at 30° of flexion compared with the native state. A 45° anteromedializing TTO offloads to a larger magnitude, with significant reductions in contact area at 30°, 45°, and 60°, contact pressures at 15° to 60°, and peak force at 15° to 60° of knee flexion compared with the same knee before TTO.
The retropatellar tendon implant is fixed to the proximal tibia underneath the distal patellar tendon, just proximal to the tibial tubercle, essentially lifting the patellar tendon anteriorly, and providing a similar, albeit smaller, offloading effect as an anteriorizing TTO without the morbidity and postoperative rehabilitation of an osteotomy. While this study presents the first biomechanical data for this retropatellar tendon implant, several patellofemoral contact pressure studies have investigated the effects of an anteriorizing and anteromedializing TTO before this. Rue et al 22 performed a controlled laboratory study of 10 human cadaveric knees, and using a similar electroresistive pressure sensor and quadriceps loading method, demonstrated that a straight anteriorizing TTO of 10 mm significantly decreased mean and peak contact pressures at 30° and 60° of flexion, without significant medialization of contact force location. Beck et al 1 with a similar methodology performed an anteromedializing TTO of 60° with a 15 mm shift, resulting in anteriorization of 13.5 mm and medialization of 7.5 mm in 10 cadaveric knees. They found a mean medial shift of the center of force on the trochlea, with overall decreased mean lateral trochlear pressures at all knee flexion angles, and an overall increased mean medial trochlear pressures at all flexion angles. Mean central trochlear pressures were significantly reduced at 30° of flexion, but increased significantly at 90° of flexion. 1 By not permanently altering the osseous anatomy, the retropatellar tendon implant functions almost as an internal mechanical offloader, similar in concept to a novel medial implantable shock absorber (MISHA; Moximed). The MISHA implant is similarly fixed to the femur and tibia via unicortical locking screws, offloading the medial compartment by up to 53% in extension during the stance phase of gait. 18 The MISHA implant obtained Food and Drug Administration (FDA) approval in 2023, while LIFT obtained FDA breakthrough device designation in 2023.
There was an overall increase in patellofemoral contact pressures with increasing flexion in our study for the intact native state and 45° TTO, while the retropatellar tendon implant had less contact pressure and peak force increase through flexion. In extension, the lowest contact pressure and contact area were observed between the patella and trochlea. In our study, after placement of the retropatellar tendon implant, 1 knee exhibited no contact force at all in extension, and 3 knees similarly exhibited no contact force at all after 45° TTO. This is because TTO slightly anteriorizes the distal pole of the patella, offloading the distal edge of the patella from the proximal trochlear groove. We chose to include these specimens and set their contact force at 0 N and contact area at 0 mm2 for analysis. We ran our analysis both with and without these 3 specimens, with no difference in results; thus, we included them for the completeness of the data. The intact native state and 45° TTO exhibited increasing contact pressures with increasing flexion, consistent with previous literature. The retropatellar tendon implant did not demonstrate a significant increase in contact pressure or peak force through flexion, likely due to the increased pressure seen at 0° of flexion. Multiple previous studies have demonstrated that various soft-tissue and osseous procedures for patellofemoral instability increase patellofemoral contact pressure with increasing knee flexion.6,17,20,27 The addition of the 45° TTO with a resultant 7.5 mm of medialization did significantly shift the center of contact force medially at 45° and 60° of knee flexion when compared with the native state and the retropatellar tendon implant. In contrast, there were no differences in medialization of the center of contact force between native states and the use of the retropatellar tendon implant. This may provide a useful clinical treatment option for medial trochlear or patellar chondral lesions that previously would have required a pure anteriorization, as opposed to the more commonly utilized anteromedialization.
The LIFT implant is not without clinical limitations and potential complications. Indications for the implant are the same for those undergoing TTO for patellofemoral chondral degeneration. While the TTO also has utility in the setting of patellofemoral instability, 24 the LIFT implant is not expected to have the same utilization; therefore, pathologically increased TT-TG distances and lateral patellar instability are contraindications to its use. An ongoing clinical trial is currently underway to investigate the clinical efficacy of the LIFT implant compared with TTO. Potential complications that need to be elucidated include irritation to the patellar tendon, with possible painful friction occurring between the implant and the tendon during dynamic activation of the extensor mechanism. Other feared complications include introduction of novel impingement in the knee joint, hardware prominence, range of motion restriction, implant loosening in the long term, and iatrogenic patellar instability. Despite these risks, the LIFT implant's rehabilitation protocol, with immediate weightbearing compared with 6 weeks of restricted weightbearing with a TTO, makes LIFT an appealing option. As always, patient education on the benefits and risks associated with this procedure will be crucial. High-quality clinical trials with long-term follow-up will be necessary to prove the clinical efficacy of LIFT.
Limitations
This study has several limitations. As with all cadaveric biomechanical studies, clinical significance remains to be determined, as patient outcomes and complications are not reported. The sample size in this study was small and may therefore be underpowered for some comparisons. Testing was performed at time zero, which does not account for soft tissue remodeling or dynamic muscle contraction that may alter time-zero contact pressures. The use of Tekscan sensors was limited to the trochlear side of the patellofemoral joint, and thus, takeaways on patellar contact pressures remain to be seen. The same size implant was used for all tests, potentially introducing a confounding variable of how well the implant fit each specimen. The methodology of our testing system utilized an open kinetic chain model through loading of the quadriceps tendon, which, although previously validated, may lead to clinical variability with closed-chain activities such as stair climbing or rising from a chair. 22 Lastly, cadaveric knee specimens of older age (mean age, 68 ± 15.5 years) were used, which may not accurately reflect the bone and soft-tissue quality of patients indicated for the retropatellar implant. We also utilized normal cadaveric knees without patellofemoral chondral lesions; theoretically, there could be a difference in the biomechanical and clinical effects of the retropatellar implant in patients with a relatively more posteriorized tibial tubercle, which may predispose patients to patellofemoral chondral lesions and retropatellar pain.
Conclusion
The main finding of our biomechanical cadaveric study was that the novel retropatellar tendon implant (LIFT, ZKR Orthopedics) did not reduce patellofemoral contact area, contact pressure, or peak force as much as a 45° anteromedializing TTO. The implant does reduce peak and contact pressures in early degrees of knee flexion compared with native states.
Footnotes
Final revision submitted August 19, 2025; accepted September 8, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: Funding for this study, including providing equipment and purchasing cadaveric specimens for testing, was provided by ZKR Orthopedics. A.B.Y. is a paid consultant for AlloSource, JRF Ortho, and Stryker; is an unpaid consultant for Patient IQ and Sparta Biomedical; has received consulting fees from Stryker, Joint Restoration Foundation, Inc, and Olympus America Inc; has received nonconsulting fees from Arthrex, Inc; has received honoraria from Joint Restoration Foundation, Inc; has received support for education from Medwest Associated; and holds stock or stock options in Patient IQ, Sparta Biomedical, and Icarus. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.