
Abstract
Background:
Although marijuana (MJ) use is likely common among adolescents and young adults undergoing hip arthroscopy (HA) for femoroacetabular impingement (FAI), there is a dearth of literature investigating the effect of MJ use on surgical outcomes.
Purpose:
To determine the effect of preoperative MJ use on outcomes among young patients undergoing HA for FAI.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
Patients ≤25 years undergoing HA for FAI were included. Preoperative MJ use was self-reported during intake; this was used to define 2 subgroups: the +MJ subgroup and the non-MJ subgroup. Baseline and intraoperative variables were compared between the subgroups. Preoperative patient-reported outcome (PRO) scores were recorded, including modified Harris Hip Score (mHHS), International Hip Outcome Tool (iHOT-12), Patient-Reported Outcomes Measurement Information System (PROMIS) Depression, and PROMIS Anxiety scores. PROs were recorded at regular intervals over the first postoperative year and assessed to determine whether each patient achieved the relevant minimal clinically important difference (MCID) and Patient Acceptable Symptom State. PRO values were compared between subgroups at each time point. Pain levels and narcotic use before discharge were recorded.
Results:
Out of 61 included patients (65.6% male; median age, 18.6 years; range, 14.7-25.4 years), 16 (26.2%) self-reported preoperative MJ use. The +MJ subgroup and non-MJ subgroup both showed statistically significant improvements in mHHS, iHOT-12, and PROMIS Depression scores from baseline to final follow-up. Of patients with final follow-up, 87.7% achieved the MCID for both the mHHS and the iHOT-12. There were no statistically significant differences in demographic or baseline variables, surgical variables, or PRO scores between the +MJ and non-MJ subgroups.
Conclusion:
This study showed significant improvements in the year after HA for FAI in adolescents and young adults regardless of preoperative MJ use. Future work is needed to explore the potentially negative effect of heavy use or abuse of MJ.
Marijuana (MJ)—also known as cannabis—is a plant containing over 100 psychoactive cannabinoid chemicals that can be ingested by smoking, by vaping, or being taken orally. 7 Although the US Drug Enforcement Administration includes MJ on its list of schedule 1 substances (drugs with no currently accepted medical use and a high potential for abuse), its use has become less taboo in the United States in recent decades. Medicinal MJ use was first legalized on the state level in California in 1996, and it is now legal in 39 states and the District of Columbia. Meanwhile, recreational MJ use was first legalized in Colorado in 2014 and is now legal in 24 states and the District of Columbia. Recreational use has been “decriminalized” in 7 additional states. 12 The National Collegiate Athletic Association also recently removed cannabinoids from its list of banned substances in 2024. But, despite these law and rule changes, MJ use remains universally illegal across the United States for people under the age of 21.
Although studies have shown that MJ use is relatively common across a broad age range, research has suggested that rates are markedly elevated in some young patients who may receive treatment from pediatric orthopaedic surgeons. In fact, about 7% of people aged 12 to 17 years report MJ use in the past month, 2 and 43.7% of high school seniors report having tried MJ in the past. 15 People 18 to 25 years old are also likely to use MJ; previous month use was about 16% in this age group in 2004 but increased to almost 20% in 2014 and about 23% in 2019.2,9
Over the same time frame that MJ use and its legality expanded in the 1990s and 2000s, the volume of hip arthroscopies (HAs) performed in adolescents and young adults also increased significantly. One study comparing rates of HA in New York State between 2004 and 2016 found that surgical volume among adolescents (aged 10-19 years) increased by a factor of about 20, while volume among young adults (aged 20-29 years) increased by a factor of about 5. 14 Another study showed that the volume of HA increased 353% in people aged 20 to 29 years and 228% among people aged 10 to 19 years in the 7 years from 2010 to 2017. 3 Still more research has shown that the highest incidence of HA is seen in patients 15 to 24 years of age. 16
Despite the likely significant overlap in MJ users and young patients undergoing HA, there has been little research on the influence of MJ use on patient experience and outcomes associated with HA. Therefore, the purpose of this study was to assess self-reported MJ use among adolescent and young adult patients undergoing HA, report the prevalence of MJ use, and investigate any relationship between MJ use and functional outcomes for these patients over the year after surgery. A secondary aim was to assess any relationship between MJ use and pain and narcotic use before discharge.
Methods
This was a retrospective study of patients who underwent HA for femoracetabular impingement (FAI) between October 2020 and December 2022 in a tertiary care pediatric hospital system. Data were obtained from a single site and single surgeon (Y.-M.Y.), collected as part of a multicenter prospective registry. The cohort included patients who were ≥10 years old and <26 years old on the day of surgery. All patients had regional anesthesia (fascia iliaca block) with general anesthesia. Muscle paralysis was used during central compartment work. No preoperative pain medication regimen was utilized. Ropivicaine was infiltrated around the hip capsule and portals at the end of the case. A cryotherapy sleeve was routinely applied to the hip postoperatively. Baseline data analyzed included demographic information, preoperative Numeric Rating Scale (NRS) pain scores, laterality affected, and preoperative patient-reported outcome (PRO) scores. PROs analyzed included the 12-item International Hip Outcome Tool (iHOT-12), modified Harris Hip Score (mHHS), and Patient-Reported Outcomes Measurement Information System (PROMIS) Depression and Anxiety scores. Self-reported preoperative MJ usage, which was queried as part of enrollment, was used to assign patients to the +MJ or non-MJ subgroup. The Child Opportunity Index (COI)—a composite index capturing inequality in regional wealth and social determinants of health 1 —was recorded for each patient based on home zip code. Social Deprivation Index (SDI) is a similar metric that was also recorded. 11 Preoperative radiographic variables including lateral center-edge angle, femoral and acetabular version, and more were recorded. These measurements were performed by an attending radiologist as part of the prospective registry. Other recorded variables included morphine milliequivalents (MMEs) of narcotic pain medication administered intraoperatively, MME given postoperatively in the postanesthesia care unit (PACU), traction time, type of nerve block used (single shot versus indwelling catheter), procedures done at surgery, and number of anchors used for labral repair (if performed). All procedures were done using a post distraction technique. The length of the procedure was calculated as the time elapsed from the anesthesia-ready mark to dressing placement.
Postoperative PROs (mHHS, iHOT-12, PROMIS Depression, and PROMIS Anxiety) were captured at 3 months, 6 months, and 1 year postoperative during in-person visits. For each PRO score, the final value was considered to be that for the 1-year time point. If there was no recorded 1-year value, the 6-month value was substituted. If neither was available, the data were considered missing. The change in PRO score (delta) for each instrument was calculated by subtracting the baseline value from the final value.
The minimal clinically important difference (MCID) and Patient Acceptable Symptom State (PASS) values for the mHHS were set at 8 and 74, respectively, based on previous literature. 13 Similarly, the MCID and PASS for the iHOT-12 were set at 13 and 63, respectively.10,13 MCID values for the PROMIS Depression and Anxiety scores were set at −4 and −6, respectively. These last 2 values were based on literature pertaining to hand surgery and spine surgery because of an absence of published research on these figures for patients undergoing HA.5,6 PASS values were not available for the PROMIS Depression and Anxiety scores, so achievement of PASS was not considered for these PROs. Other than the noted exceptions, each PRO delta was compared with the relevant MCID, and each final PRO value was compared with the appropriate PASS value to determine whether these criteria were achieved.
NRS pain scores were recorded in the PACU based on institutional nursing practice. Values were grouped according to time from surgery completion: 0-1 hours, 1-2 hours, 2-3 hours, and 3-4 hours postoperatively. Pain scores in each postoperative time frame were averaged for each patient to yield 4 successive pain scores over these time frames. The amount of narcotic (MME) administered in the PACU before discharge was also recorded.
Continuous data were tested for normality before statistical comparisons. Nonparametric data were summarized using median and range, while parametric data were summarized using mean and standard deviation. Categorical data were presented in descriptive fashion along with percentages. Baseline variables, surgical variables, and outcome variables were compared between the 2 subgroups. Nonparametric data were compared using Wilcoxon rank-sum tests while parametric data were compared using unpaired t tests. Categorical variables were compared using Fisher exact tests or chi-square tests. Data were organized using Microsoft Excel, and all comparisons were done using Stata Version 17.0 (StataCorp LLC). Statistical significance was set at a threshold of P < .05.
Results
A total of 61 patients met inclusion criteria and were reviewed (40 male, 21 female). Demographic and baseline data, including COI and SDI, were similar between the +MJ and non-MJ subgroups (Table 1). Surgical variables were also similar between the subgroups (Table 2). All patients underwent femoroplasty, and 78.7% underwent labral repair. All patients were discharged home on the same day. While the overall proportion of patients self-reporting preoperative MJ use was 16 (26.2%), this rate was 40% among patients 18 to 19 years of age (Table 3).
Demographic and Baseline Data a
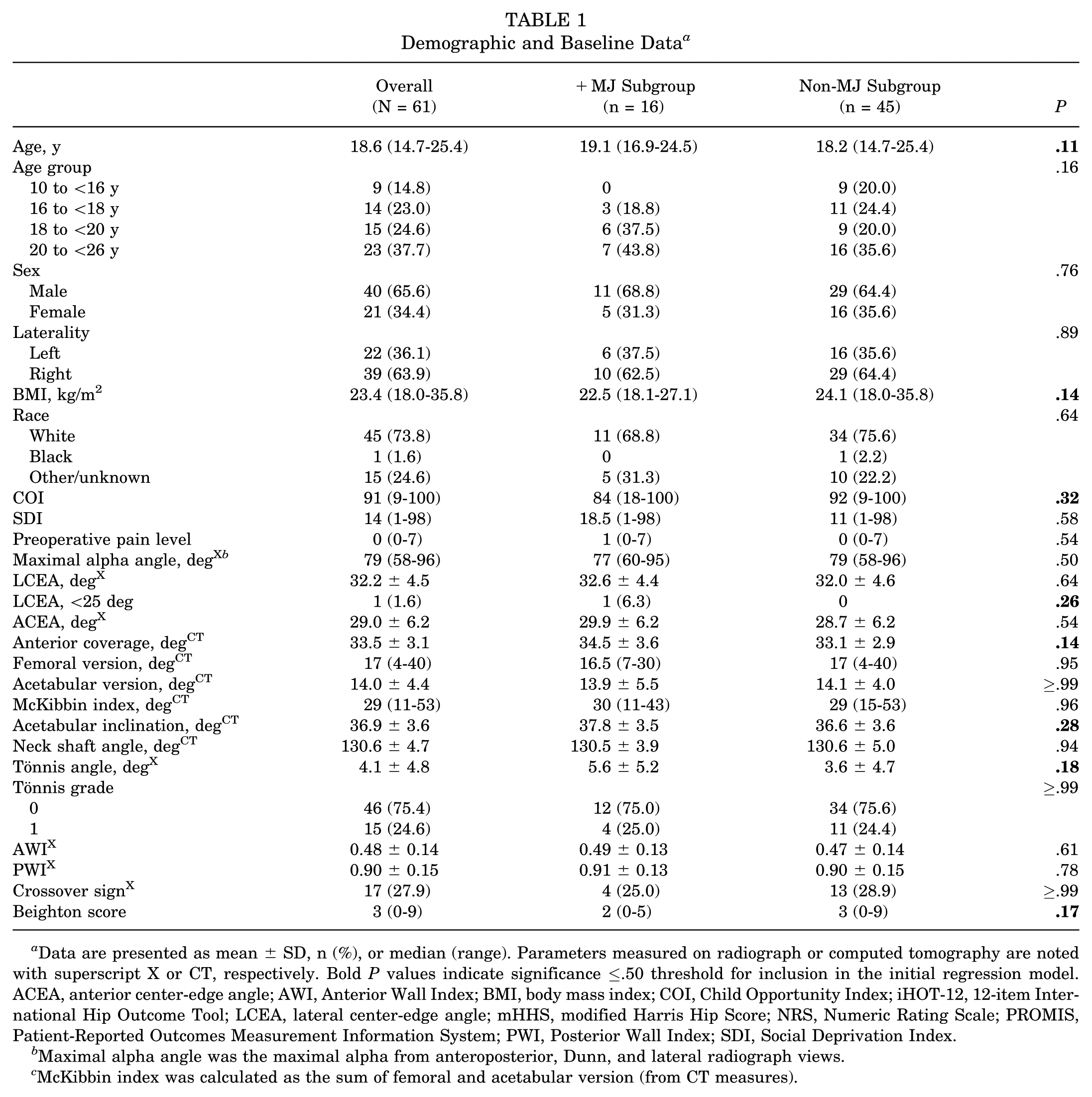
Data are presented as mean ± SD, n (%), or median (range). Parameters measured on radiograph or computed tomography are noted with superscript X or CT, respectively. Bold P values indicate significance ≤.50 threshold for inclusion in the initial regression model. ACEA, anterior center-edge angle; AWI, Anterior Wall Index; BMI, body mass index; COI, Child Opportunity Index; iHOT-12, 12-item International Hip Outcome Tool; LCEA, lateral center-edge angle; mHHS, modified Harris Hip Score; NRS, Numeric Rating Scale; PROMIS, Patient-Reported Outcomes Measurement Information System; PWI, Posterior Wall Index; SDI, Social Deprivation Index.
Maximal alpha angle was the maximal alpha from anteroposterior, Dunn, and lateral radiograph views.
McKibbin index was calculated as the sum of femoral and acetabular version (from CT measures).
Surgical Variables a

Data are presented as median (range) or n (%). MME, morphine milliequivalents.
Self-Reported Preoperative Marijuana Use a
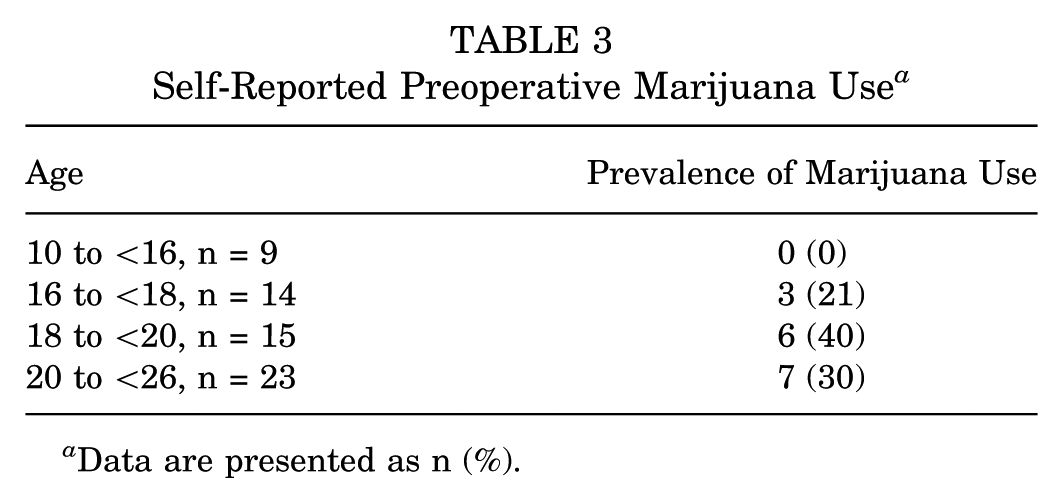
Data are presented as n (%).
Figure 1 (B-D) shows that for both subgroups, 1-year mHHS, iHOT-12, and PROMIS Depression scores improved from baseline (P < .05). PROMIS Anxiety scores at the 1-year time point were not statistically different from baseline (P = .05 for the +MJ subgroup and P = .18 for the non-MJ subgroup). No statistically significant difference was found between the subgroups for any PRO score at all time points.

Box plots showing pain levels in the postanesthesia care unit (PACU) over (A) the first 4 hours after surgery as well as (B-E) patient-reported outcome scores in the year after surgery. iHOT-12, 12-item International Hip Outcome Tool; mHHS, modified Harris Hip Score; MJ, marijuana; NRS, Numeric Rating Scale; Pre-op, preoperative. Asterisk indicates a statistically significant increase from basline.
Final PRO scores were recorded for 49/61 (80.3%) patients. This consisted of 1-year follow-up data for 43/49 patients. Six-month follow-up data was substituted for 1-year data in 6 more patients who were missing 1-year data. Among patients with both 6- and 12-month follow-up, 70.5% (43/61) had 6- and 12-month scores within 9 points. Subanalysis of patients with both 6-month and 1-year PROs showed a median change of 0 points between these time periods. Delta values (difference from baseline to final follow-up) were calculated for each PRO score for the 49 patients with final scores. Analysis of achievement of MCID and PASS for the various PROs in these patients is shown in Table 4. There was no identified difference between the subgroups in rates of achievement of MCID or PASS for any of the PRO instruments.
Analysis of MCID and PASS Outcomes of Patients With Final Scores a

Data are presented as mean ± SD, n (%), or median (range).
Intraoperative opioid administration was similar between the subgroups (P = .29). Figure 1A illustrates pain scores in the 4 hours after surgery. There was no statistically significant difference between the 2 subgroups in any of these measures at any time point (P≥ .22). For both subgroups, pain levels in the 3- to 4-hour postoperative time frame were lower than those in the 0- to 1-hour time frame (P < .01). PACU narcotic consumption was similar between the subgroups (+MJ subgroup: median [range], 3.75 [0-21.5] MME; non-MJ subgroup: 7.5 [0-18] MME; P = .76).
Discussion
The current clinical study showed that regardless of preoperative MJ use, HA for FAI in adolescents and young adults was associated with marked functional improvement in the year after surgery. Patients showed increases in mHHS and iHOT-12 scores, with 87.7% reaching the MCID for both at final follow-up. Patients also showed improvements in depressive symptoms at final follow-up, with over half reaching the MCID for the PROMIS Depression score. No evidence was found that preoperative MJ use influenced these phenomena. In fact, despite examining a multitude of baseline, intraoperative, and postoperative data, this study failed to find any notable difference between patients who reported preoperative MJ use and those who denied it.
By showing that the amount of narcotic consumed perioperatively as well as pain levels in the PACU after surgery were similar between MJ users and nonusers after HA, the current study nicely complements previous work by Wood et al, 17 who showed that MJ users do not require more opioids after HA. Evidence to date suggests that although MJ use has been linked to musculoskeletal pain, surgeons can be reassured that MJ users generally do not require more narcotic pain medication perioperatively. It is recognized that the current study's evidence supporting this conclusion was gathered in a clinical situation where patients were routinely treated with regional blocks and local anesthesia regardless of MJ status. Future prospective studies may investigate pain levels and narcotic consumption in the weeks after discharge to ascertain whether MJ users consume more pain medication during the early recovery period.
In a previous study, 28% of patients undergoing HA for nonarthritic conditions were noted to exhibit depressive symptoms. 8 If, in the current study, the suggested PROMIS Depression score cutoff of ≥53 was applied to classify depression as a clinical condition, 4 18 of 61 (29.5%) patients would have qualified for the diagnosis of depression before surgery. Although it is interesting that PROMIS Depression scores decreased in both subgroups in the year after HA in the current study, this finding is not novel. In fact, the idea that depressive symptoms decrease after HA has been suggested in ≥2 previous studies: one showing that insurance claims for depression medication and therapy are lower after HA surgery 19 and another showing improved PROMIS Depression scores 1 year after HA for FAI. 18
Limitations
This study has several limitations, including the single-surgeon nature of the study and the young patient age range, which may limit external validity. We also recognize that over half of the patient sample was male, and patients with borderline hip dysplasia were largely absent from the study, which may further limit generalizability. It is recognized that a reliance on self-reporting likely leads to an underestimation of true MJ use rates. This issue may be especially relevant when dealing with patients <18 years (recognizing that no one <16 admitted to MJ use in this study). This is important to note, as having a significant number of MJ users deny preoperative MJ use would have biased results toward showing no difference between the groups. Additionally, the amount of MJ regularly used and mode of ingestion was not known in this study, preventing any assessment of influence for these variables. A lack of information detailing pain levels and narcotic usage over the weeks after surgery also limited any assessment of postoperative pain to the experience before discharge. It is also noted that no data were available detailing sports participation or return-to-sport rates after surgery.
Follow-up was also limited in this study, with only 70.5% (43/61) of patients having 1-year PROs. However, a significant proportion without 1-year PROs had 6-month scores. Because the median change in mHHS between 6-month and 1-year follow-up was 0 (with 70% having 6- and 12-month scores within 9 points), the authors decided that it was reasonable to deal with missing 1-year values by substituting 6-month values whenever available. While this led to 80.3% of patients having “final follow-up,” it would have been ideal to have more consistent 1-year follow-up, as well as longer-term metrics.
Additionally, the authors recognize that the values used for MCID and PASS—although based on sound methodology in larger series—were derived from predominantly adult samples. Younger patients might be expected to have higher MCID and PASS scores, which would affect our conclusions regarding the proportions of patients achieving each threshold. However, in the absence of clearly defined values specific to adolescent and young adult patients, it was decided to proceed with the existing MCID and PASS values used.
Perhaps the most significant limitation of the current study is its limited power. Using the given sample sizes and findings, the study achieved only about 30% power to discern the observed difference in the mHHS delta and only about 11% power to discern the observed difference in the iHOT-12 delta. This lack of power means that there is a risk of Type II error in this study. However, enrollment was limited to patients from the prospective registry, so there was no reasonable alternative to counter this limitation. Moreover, not one statistically significant difference between subgroups was found throughout over 40 comparisons, which strengthens the conclusion that there is likely no notable difference between the subgroups. This many comparisons would typically require a correction to the statistical significance threshold, but this was not necessary, as none of the between-subgroup comparisons even approached the unadjusted significance threshold of p<0.05. Additionally, 12 patients (19.7%) did not have final follow-up PRO data available (no 6-month or 1-year follow-up data). Although these dropouts could theoretically influence the study's conclusions, repeat testing after removal of these patients did not affect the statistical significance of the findings presented.
Conclusion
This study is the first clinical study to assess the potential effect of preoperative MJ use on the patient experience around and outcomes after hip arthroscopy for FAI. Clinicians may be encouraged that there is no evidence that preoperative MJ use affects pain levels or narcotic requirements around the time of surgery, nor is there evidence that MJ use detracts from outcomes. In fact, adolescents and young adults showed marked improvements after hip arthroscopy regardless of preoperative MJ use. Further research is needed to test this conclusion on a larger scale and to examine whether heavy MJ use or abuse may negatively affect outcomes after surgery.
Footnotes
Final revision submitted July 22, 2025; accepted August 11, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: C.J.D. has received food and beverage from Stryker and Wishbone and support for education from Arthrex and Smith & Nephew. G.D.H. is a consultant for Medtronic. Y.-M.Y. is a consultant for Smith & Nephew and Orthopediatrics and has received food and beverage from Stryker and Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Boston Children's Hospital (No. P00041987).