
Abstract
Background:
Renewed interest in anterior cruciate ligament (ACL) preservation has led to increased focus on tear location within the knee joint in treatment decisions, with primary ACL repair reserved for proximal tears. Retrospective studies have reported varying tear locations in adults when assessed on magnetic resonance imaging (MRI), with few studies comparing tear location on MRI versus intraoperative findings.
Purpose:
To prospectively determine the distribution of ACL tear location assessed on MRI versus intraoperative evaluation to test the hypothesis that <15% of ACL tears are proximal type avulsions.
Study Design:
Cohort study (Diagnosis); Level of evidence, 2.
Methods:
A total of 174 patients with clinically confirmed full-thickness ACL tears between August 2022 and March 2024 were identified and enrolled. Patients with partial tears, chronic injuries, recurrent ACL tears, or multiligamentous injuries were excluded. ACL tear locations were classified on preoperative MRI and intraoperatively using the modified Sherman classification. Patient demographic characteristics, injury mechanism, and surgical details were recorded. Analysis of variance and chi-square and Fisher exact tests were used for analysis, with significance set at P < .05.
Results:
ACL tear location based on MRI was as follows: 9.8% type I, 22.4% type II, 67.2% type III, and 0.60% type IV, with no type V tears. Arthroscopic tear location distribution was as follows: 26.4% type I (proximal avulsion), 44.8% type II (proximal), 25.8% type III (midsubstance), and 3.4% type IV (distal), with no type V tears. There was 43% agreement between arthroscopic and MRI evaluation overall, with 95.5% agreement when classifying type III tears. Type I tears were more common in older patients, whereas type III tears were more common in younger patients. No significant correlations were appreciated based on patient sex, body mass index, or injury mechanism.
Conclusion:
Poor agreement was found between imaging and arthroscopic assessment of ACL tear location, as MRI predicted intraoperative ACL tear location in less than half of cases. However, very good agreement was noted when classifying type III tears. Tear pattern was associated with patient age, with more type I tears in older patients and more type III tears in younger patients.
Anterior cruciate ligament (ACL) tears are among the most common knee injuries, affecting >200,000 people in the United States each year and entailing direct and indirect costs >$7 billion annually.11,19,20,23 The current gold standard operative treatment is ACL reconstruction (ACLR), which carries a graft failure rate of 6% at 5 years and 9% at 25 years. 21 Before reconstructive techniques evolved, ACL injuries were commonly treated with primary repair. This method came under scrutiny after one study reported a 53% reinjury rate after 5 years, 9 and primary repair was later abandoned after randomized, prospective trials showed improved results with ACLR. 28
Despite this evidence, renewed interest has arisen in primary repair of ACL tears over the last 15 years. This interest is partially based on a 1991 study by Sherman etal 22 on primary ACL repair that stratified patients and their outcomes by tear location. This study found that patients with proximal ACL tears had better outcomes compared with patients who had midsubstance tears. Considering these results along with advancements in arthroscopic techniques, DiFelice etal 8 hypothesized that primary repair in a select group of patients with proximal tears (types I and II) and good tissue quality could have successful outcomes while maintaining the proprioceptive properties of the natural ACL with decreased graft donor site morbidity. DiFelice etal reported a failure rate of 9% at 3.5 years in 11 patients, and Jonkergouw etal 10 later published a failure rate of 10.7% at 2 years in 56 patients undergoing ACL repair. In addition to repair of these proximal tears, the use of bridge-enhanced techniques to repair midsubstance injuries has attracted interest. 18
With increased interest in ACL repair, appropriate identification of tear location has become essential. Multiple retrospective studies have measured the distribution of different tear types in adults on magnetic resonance imaging (MRI) with varying reported incidences of tear location. § However, only 2 of these studies compared MRI with intraoperative findings.17,23 As such, the primary objectives for the current study were to prospectively determine the distribution and accuracy of ACL tear location on preoperative MRI compared with intraoperative evaluation. Potential correlations between tear location, patient demographic characteristics, and injury mechanism were also examined. Based on prior studies, it was hypothesized that <15% of ACL tears would be verified as proximal avulsions. ¶
Methods
Study Design and Enrollment
A prospective cohort study was approved by the institutional review board (No. 202206104) at the senior author's institution (R.H.B.). Using a sample size calculation for descriptive studies as reported by Charan etal, 5 we calculated sample size using 95% CI, estimating type I proximal avulsion tear prevalence of 0.15 and precision of 0.05. Based on this calculation, a minimum of 139 patients were determined to be sufficient, with a goal of 160 patients to account for exclusion criteria. A total of 174 patients were ultimately enrolled between August 2022 and March 2024 by 4 fellowship-trained sports medicine orthopaedic surgeons at a single institution (R.H.B., M.J.M., M.V.S., and D.M.K.). Inclusion criteria were patients 14 years or older with full-thickness ACL tears undergoing ACLR with MRI obtained at the participating institution. Exclusion criteria consisted of patients with partial tears, those with recurrent ACL graft tears requiring revision surgery, patients with ACL tears occurring >1 month from MRI, patients with multiligamentous knee injuries, and any patients undergoing MRI at an outside facility.
Data Collection
The following patient demographic characteristics were collected: patient age, sex, height, weight, smoking status, and diabetes. Injury details including date and mechanism of injury were recorded. Operative details collected included date of surgery, graft type, performance of any concomitant procedures, and ACL tear location as assessed arthroscopically. Mechanism of injury was defined as noncontact, indirect contact (contact to another body part above or below the knee), or direct contact (to the knee). 4 The modified Sherman classification was used to classify tear location on both arthroscopy and MRI. Type I tears are characterized by a femoral avulsion with >90% of the distal ACL left intact; type II, proximal tear with 75% to 90% of the distal ACL left intact; type III, tear in the middle 50% of the ACL (midsubstance); type IV, distal tear with 10% to 25% of the distal ACL left intact; and type V, tibial avulsion with <10% of the distal ACL left intact at the tibial insertion.6,8,27
Intraoperative tear location was assessed using a 30° arthroscopic view from a standard anterolateral portal, further defined using an arthroscopic probe from an anteromedial portal. Assessment was performed by 1 of 4 fellowship-trained sports medicine surgeons performing the operation and was recorded using a data collection form at the conclusion of the procedure. Preoperative MRI tear location was independently assessed by 2 fellowship-trained musculoskeletal radiologists (J.C.B. and K.B.N.) using the MRI measurement protocol outlined by van der List etal. 30 All MRI examinations were performed on either a 1.5- or 3.0-T scanner using a dedicated extremity coil. All examinations included the following: sagittal proton density; coronal T1-weighted; and axial, sagittal, and coronal T2-weighted, fat-suppressed sequences. Disagreements between radiologists were resolved by the senior author, who retrospectively reviewed the blinded MRI scans to select which tear location would be used. The radiologists were blinded to arthroscopic tear location. The surgeons were blinded to the separate assessment of ACL tear location by the musculoskeletal radiologists; however, the surgeons were not blinded to the MRI scans or the initial clinical radiology reports that usually did not comment on ACL tear location.
Statistical Analysis
Statistical analyses were conducted using the R programming language (R Core Team, 2024). Descriptive statistics, including means, standard deviations, frequencies, and percentages, were used to summarize the baseline characteristics of the study participants. Arthroscopic and MRI ACL tear location distributions were described across various demographic factors such as sex, body mass index (BMI), and mechanism of injury. Mean age was calculated across tear types. The 95% CI was calculated for each proportion. Chi-square tests were used to evaluate for significant differences in overall tear location distribution between categorical variables, whereas analysis of variance was used for continuous variables. Fisher exact tests were used to evaluate for pairwise differences in individual tear types among categories. Differences between groups were considered statistically significant at P < .05. When data distributions did not meet the assumptions for parametric tests, nonparametric alternatives were considered. Interobserver reliability for ACL tear location by the radiologists was assessed using Cohen kappa. Interpretation of kappa values was based on guidelines outlined by Landis and Koch. 15 Ordinal logistic regression was used to further investigate the relationship between age and tear type.
Results
A total of 181 patients meeting inclusion criteria were initially enrolled in the investigation. Two patients were excluded because of inability to reliably determine ACL tear location arthroscopically, and 5 additional patients were excluded because of missing MRI scans or reads. As a result, 174 patients were included in the final analysis (Table 1). We found that 54% (n = 94) of patients were female, and the overall mean age was 25.4 ± 11.9 years (range, 14-66 years). The mean BMI was 25.7 ± 4.6 kg/m2 (range, 17.8-42.4 kg/m2). The mean time from injury to surgery was 50.2 ± 78.7 days (range, 8-783 days). The most common mechanism of injury was noncontact, reported in 62.1% (n = 108) of patients. Surgery was performed on the left knee in 55.2% (n = 96) of cases.
Baseline and Operative Characteristics a

Data are expressed as mean ± SD (range) or n (%).
ACL Tear Location
Arthroscopic evaluation revealed that the most frequent tear type was type II (proximal) in 44.8% of patients (78/174; 95% CI, 37.4%-52.2%), followed by type I (proximal avulsion) in 26.4% (46/174; 95% CI, 19.9%-33.0%) and type III (midsubstance) in 25.8% (44/174; 95% CI, 18.8%-31.8%). Distal tears (type IV and type V) were less common, observed in only 3.4% of patients (6/174; 95% CI, 0.74%-6.2%), with no distal avulsion tears (type V) recorded.
On MRI evaluation, the most frequent tear type was type III in 67.2% of patients (117/174; 95% CI, 60.3%-74.2%), followed by type II in 22.4% (39/174; 95% CI, 16.2%-28.6%) and type I in 9.8% (17/174; 95% CI, 5.4%-14.2%). Distal tears were also less common, with type IV tears in 0.60% of patients (1/174; 95% CI, 0.0%-1.7%) and no type V tears observed on MRI. The distribution of both arthroscopic and MRI tear locations is shown in Figure 1.

Distribution of anterior cruciate ligament tear location. MRI, magnetic resonance imaging.
Comparison of Arthroscopic Versus MRI ACL Tear Location
Overall agreement on ACL tear location on arthroscopic evaluation and MRI was 43.1% (n = 75/174). We noted 95.5% agreement when assessing type III tears (Table 2).
Arthroscopic Versus Magnetic Resonance Imaging Agreement by Tear Type

Interobserver reliability between the 2 radiologists was moderate, with a Cohen kappa value of 0.41 (95% CI, 0.29-0.51). The overall percentage agreement between radiologists was 71.3%. The radiologists disagreed on 50 images (28.7% of total). Of these, 36 (20.7% of total) differed by only 1 type (eg, type I vs type II) and the other 14 (8.0% of total) differed by 2 types (eg, type I vs type III).
ACL Tear Location and Sex
Female patients had a higher prevalence of type I tears on both arthroscopic and MRI distributions compared with male patients, whereas males had a higher prevalence of type III tears (Table 3). However, the differences in male and female distributions overall were not statistically significant on either arthroscopic (P = .332) or MRI (P = .477) evaluation.
Anterior Cruciate Ligament Tear Location by Sex a

Data are expressed as percentage (95% CI). MRI, magnetic resonance imaging.
ACL Tear Location and Age
Type III tears were more frequently encountered in younger patients (Table 4). Further investigation of this relationship through ordinal logistic regression demonstrated a significant negative association between age and ACL tear location (coefficient = −0.036; P = .009). As age increased, the likelihood of a tear occurring in lower ordered categories such as type I increased, whereas younger individuals had a higher probability of type II or type III tears. A similar result was seen with age and MRI tear location (coefficient = −0.05; P = .0001) where younger individuals had an even higher probability of type III tears. Type IV tears were excluded from both models due to low frequency.
Anterior Cruciate Ligament Tear Location and Age a
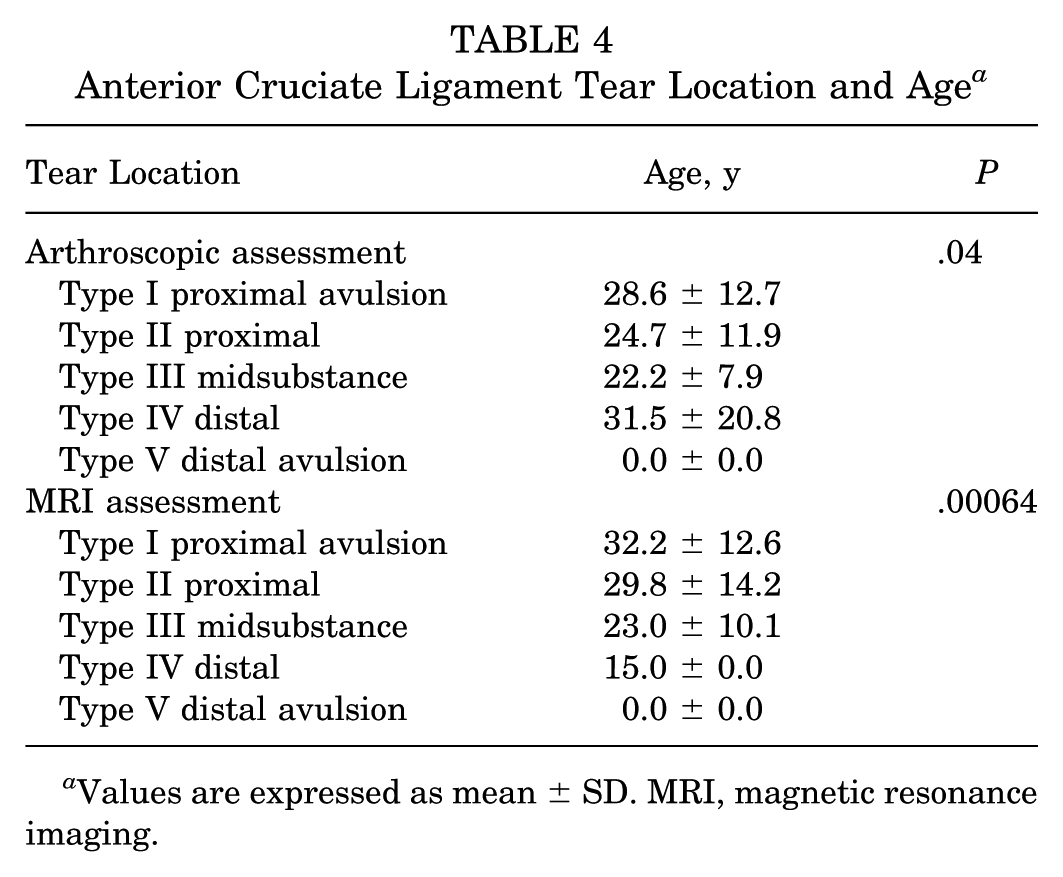
Values are expressed as mean ± SD. MRI, magnetic resonance imaging.
ACL Tear Location and BMI
A higher proportion of type I tears was seen in obese patients (BMI ≥30 kg/m2) in both distributions (Table 5). Underweight and normal weight patients (BMI 17 to <25 kg/m2) had a higher frequency of type III tears when assessed on MRI (Table 5). Despite these trends, no statistically significant differences were noted in tear distribution across BMI groups for both arthroscopic (P = .64) and MRI distributions (P = .53). Additionally, we found no significant differences with pairwise comparison.
Anterior Cruciate Ligament Tear Location by BMI a

Data are expressed as percentage (95% CI). BMI, body mass index; MRI, magnetic resonance imaging.
Arthroscopic ACL Tear Location and Mechanism of Injury
For both arthroscopic and MRI tear distributions, we found no significant differences between tear location and mechanism of injury (P = .25 and .57, respectively) (Table 6). When clustering different groups, we noted a statistically significant difference between indirect contact and direct contact /noncontact injuries in the distribution of arthroscopic type III tears, with an odds ratio of 0.35 (95% CI, 0.10-0.99; P = .038), suggesting that indirect injuries were 65% less likely to result in type III tears.
Anterior Cruciate Ligament Tear Location (%) by Mechanism of Injury a

Data are expressed as percentage (95% CI). MRI, magnetic resonance imaging.
Discussion
This is the first prospective multisurgeon study reporting the distribution of ACL tear location in patients undergoing ACL surgery. Type I tears were more common in older patients, whereas type III tears were more common in younger patients. Overall, there was poor agreement between MRI and arthroscopy on ACL tear location, although type III tears appeared to be an exception with very high agreement.
In this cohort, 9.8% of patients had proximal avulsion tears identified on MRI versus 26.4% on arthroscopy. Drawing on prior literature, we hypothesized that <15% of ACL tears would be proximal type avulsions. ‖ Although the findings on MRI were in agreement with this hypothesis, the arthroscopic results were nearly double this value and toward the upper range of what was previously reported (4%-26%). # The most obvious reason for this disparity is attributable to the different identification methods, as the results in prior studies were primarily based on MRI. Some variability in surgeon assessment may be present as well. These results suggest that MRI may be less specific in diagnosing proximal ACL injuries than previously thought, given that arthroscopic evaluation should be considered the gold standard.
In contrast to an increase in proximal tears on arthroscopy, a decreased percentage of type III midsubstance tears (25.8%) was noted compared with the range previously reported (38%-62%). ** This disparity again may be largely due the classification of tear location on arthroscopy rather than MRI. Mehier etal 17 reported agreement between MRI and arthroscopy in 71% of cases versus 43% in the current study. Unlike our study, Mehier's investigation was a retrospective review of patients who underwent surgical treatment of ACL tears by a single surgeon; 30% of tears were repaired, and the study did not include patients younger than 18 years. Several factors could account for the differences in MRI tear localization, including interobserver variability in imaging and/or arthroscopic assessment along with different MRI protocols, sequences, and quality. Furthermore, scarring of the ligament and changes to ACL morphology during the time between MRI and surgery could lead to variability in tear classification.
Despite the lower overall agreement between arthroscopy and MRI, we noted 95.5% agreement when classifying type III tears. One reason for higher agreement could be that midsubstance tears are easier to identify on both modalities, as more proximal tears can be obscured by other tissue within the notch or out of plane on the MRI scan. A recent study also found that MRI may overestimate the distality of tear location. 7
In regard to identifying MRI tear location, we found moderate interobserver reliability between radiologists, with a Cohen kappa value of 0.41. This agreement was in the range of prior studies that reported kappa values going from slight to substantial agreement in classifying ACL injuries on MRI.3,32 Another study found that focusing on the distal remnant length rather than using the Sherman classification to classify ACL tears led to almost perfect agreement. 33 When considering MRI evaluation of the knee overall, however, variation in radiologist interobserver reliability is common.2,13,32
Although the overall distribution of tear types between male and female patients was not statistically significant, there were notable trends. Female patients demonstrated a higher proportion of type I tears compared with male patients, whereas male patients had a greater incidence of type III tears. These trends are consistent with prior literature suggesting that anatomic and biomechanical differences between men and women may predispose them to different ACL injury patterns. 24 It has also been theorized that men experience more high-energy ACL injuries compared with women 34 and that proximal avulsion injuries are more common in lower energy injuries, whereas the ligament is more commonly disrupted in the midsubstance in higher energy mechanisms. 30
Age was found to be a significant factor in ACL tear location. The probability of type I tears clearly increased with age. Based on tear location assessed by arthroscopy, patients with type I tears were on average 6 years older than those with type III tears, whereas they were on average 9 years older when based on MRI assessment of tear location. This finding is similar to a study by van der List etal, 30 in which type I tears were significantly more frequent in patients older than 35 years compared with patients ages 18 to 35 years. Additionally, the probability of having a type III tear was significantly increased in younger patients. This result is similar to prior studies that have associated type III tears with younger adults and pediatric populations.14,30,31 This result also suggests that younger individuals, who are often involved in high-intensity sports or physical activities, may be more prone to midsubstance tears, which are typically caused by higher energy mechanisms. 30
This study is not without limitations. As the cohort was drawn from a single institution, this may limit the generalizability of the findings to broader populations located in different urban or suburban areas. Moreover, variations in patient demographic characteristics, injury mechanisms, and surgical techniques across could affect tear distribution and outcomes. Additionally, the reliance on intraoperative assessments from different surgeons for determining tear location introduces interobserver variability. Subsequent studies could assess interobserver reliability of surgeon arthroscopic evaluations using video analysis; however, arthroscopic videos were not recorded in the present study. Interobserver variability was also present on the MRI assessment of ACL tear location that led to further discrepancies in assessing tear location. Almost 30% of the MRI scans required review to reconcile discrepancies between the radiologists, although the majority of the discrepancies were within 1 type and the rest differed only by 2 types. Another limitation is the imbalance in tear type distribution, particularly the low occurrence of tear types such as distal tears. This limits the ability to draw definitive conclusions about how these tears present and how well intraoperative findings correlate with MRI evaluation. Future studies could potentially rely on recording the distal remnant length, which may be a more reproducible measure, in addition to analyzing variables such as meniscal tears, posterior tibial slope, notch width, and the extent of injury to the lateral compartment in order to further investigate any relationships with tear classification.
The findings from this study provide valuable insights into the general understanding of ACL tear patterns and their associations with various demographic and injury-related factors. With this renewed interest in ACL repair, it is important to understand tear location as it may affect surgical approach. The data highlight that MRI may not be ideal for predicting type I tears that may be amenable to surgical repair. These findings reinforce the need for further classification and study to better understand the underlying mechanisms behind different tear types and how variation in ACL injuries could influence treatment.
Footnotes
Final revision submitted October 11, 2025; accepted October 25, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.V.S. has received research support from Elite Orthopedics. M.J.M. has received consulting fees from Arthrex Inc, Osteosys, and Schwartz Biomedical and support for education from Arthrex Inc, Bregg Inc, Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Washington University School of Medicine, St. Louis, Missouri, USA (Institutional Review Board No. 202206104).