
Abstract
Background:
An altered tibial position is still present despite anterior cruciate ligament (ACL) reconstruction. It has been demonstrated that an abnormal tibial position after an ACL injury may play a role in subsequent injuries to the meniscus, which can lead to early cartilage degeneration.
Purpose:
To determine changes in both the tibial position and the meniscal matrix present before and after ACL reconstruction as well as to evaluate the association between these 2 variables in ACL-injured knees 3 years after reconstruction.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
Bilateral knee magnetic resonance imaging (MRI) of 32 patients with unilateral ACL injuries was performed before reconstruction; 13 control participants also underwent MRI. Follow-up MRI was performed up to 3 years after surgery. Tibial position, internal tibial rotation, and T1ρ and T2 values of the menisci were calculated using an in-house MATLAB program. Student t tests and multiple linear regression were used to compare differences between injured, uninjured, and control knees as well as to assess correlations between the tibial position at 3 years and 3-year changes in quantitative MRI meniscal relaxation values.
Results:
The tibial position of injured knees was more anterior than that of uninjured knees at baseline, 6 months, and 1, 2, and 3 years (P < .05 for all). The T1ρ and T2 values of the menisci of injured knees were greater than those of uninjured and control knees in the posterior lateral and posterior medial horns up to 1 and 2 years after surgery, respectively (P < .05 for all). The tibial position at 3 years was associated with increased T2 values from baseline to 3 years in the posterior medial horn (β = 0.397; P = .031) and anterior medial horn (β = 0.360; P = .040).
Conclusion:
Results of the current study indicate that there is a persistently altered tibial position after ACL reconstruction. Initial preoperative meniscal abnormalities show prolonged but gradual improvement. Additionally, correlations between the tibial position and changes in the medial meniscal matrix suggest that the tibial position may play a role in the increased susceptibility to medial meniscal tears seen after reconstruction. The development of newer surgical techniques must address a persistently altered tibial position. Quantitative MRI is an effective instrument to evaluate meniscal matrix changes and can serve as an early radiological tool for meniscal injuries.
Although anterior cruciate ligament (ACL) reconstruction is a commonly performed procedure, the outcomes from long-term follow-ups of patients who have undergone this procedure are still concerning, with up to 50% of patients developing radiographic osteoarthritic changes. 21,23 The current literature reports that the rate of meniscal tears after primary ACL reconstruction is 8.5% for medial meniscal tears and 1.3% for lateral meniscal tears. 19,22 In a cohort of 6576 patients, Dunn et al 11 demonstrated a 2 times higher rate of meniscal reoperations after an ACL tear for those treated nonoperatively versus operatively. However, a recent systematic review by Delincé and Ghafil 10 found that there was not enough evidence to recommend systematic surgical reconstruction of all ACL-deficient patients to prevent further meniscal lesions and subsequent degeneration of the joint.
The exact mechanism of how ACL reconstruction affects the status of the meniscal matrix is still unclear. Despite success on certain clinical outcome measures, results from more objective measures such as motion analysis and magnetic resonance imaging (MRI) assert that there are persistent alterations in tibial position after ACL reconstruction, leading to altered mechanical loading of the knee. ∥ Changes in the meniscal load distribution can increase the in situ forces in the meniscus. 1 Increases in meniscal shear forces are thought to play a role in the subsequent development of meniscal damage. 24 Meniscal damage has been associated with cartilage loss and joint degeneration. 17,41
The meniscal fibrocartilage structure is a dense extracellular matrix composed primarily of water (72%), collagen (22%), and proteoglycans (<1%). 12,36 Meniscal damage has been previously linked to histological alterations in the collagen-proteoglycan matrix. 25 Recently, quantitative MRI (qMRI) comprising T1ρ and T2 protocols has been used to detect early signs of cartilage and meniscal degeneration. 26,27,34,38,40 In addition, a persistently altered tibial position after ACL reconstruction has been associated with elevated qMRI relaxation values of cartilage, suggesting that these changes may be indicative of future cartilage injuries. 2,43 To date, no longitudinal analysis has been performed on meniscal qMRI as it correlates to tibial position.
The objective of this study was to determine changes in both the tibial position and the meniscal matrix present before and after ACL reconstruction as well as to evaluate the association between these 2 variables in ACL-injured knees 3 years after reconstruction.
Methods
Participants
This longitudinal prospective study included 2 groups of patients. The ACL group was composed of 32 patients with a unilateral ACL injury who underwent “anatomic” single-bundle ACL reconstruction by 1 of 4 sports medicine fellowship–trained orthopaedic surgeons at a single institution. The control group was composed of 13 participants without a history of knee injuries, surgery, or clinical symptoms of osteoarthritis. The participant characteristics are detailed in Table 1. Exclusion criteria included previous injuries or surgery to either knee, history of inflammatory arthritic disease, injuries to other ligamentous structures needing a surgical intervention, concomitant meniscal repair, and concomitant cartilage resurfacing procedures performed at the time of surgery. ACL-injured patients had both injured (ipsilateral) and noninjured (contralateral) knees scanned at baseline before surgery and then again at 6 months, 1 year, 2 years, and 3 years after reconstruction. Patients in the control group had both knees scanned at baseline, 1 year, and 3 years. This study obtained institutional review board approval, and written informed consent was obtained from all enrolled participants.
Demographic Information for the ACL and Control Groups a

a ACL, anterior cruciate ligament; BMI, body mass index; N/A, not applicable.
Surgical Procedure
In the ACL group, single-bundle ACL reconstruction was performed using either a hamstring tendon autograft (n = 22) or posterior tibial tendon allograft (n = 10) with femoral tunnels drilled using anteromedial portal drilling. Additionally, 6 patients in the ACL group underwent concomitant partial meniscectomy: medial sided in 1 patient, lateral sided in 4 patients, and both medial and lateral in 1 patient. All patients underwent similar postoperative rehabilitation programs at the same institution’s sports medicine clinic.
MRI Protocol
Bilateral knees were scanned using a 3-T MRI scanner (GE Healthcare) with an 8-channel phased array knee coil (Invivo) at all time points. Patients were instructed to rest for 30 minutes before image acquisition in a seated, unloaded state. Imaging protocols included (1) high-resolution 3-dimensional (3D) fast spin echo (CUBE) (repetition time [TR]/echo time [TE] = 1500/25 milliseconds; field of view [FOV] = 16 cm; matrix = 384 × 384; slice thickness = 1 mm; echo train length = 50; bandwidth = 50 kHz; number of excitations = 0.5), (2) sagittal 3D T1ρ and T2 quantification sequences (TR/TE = 9/3 milliseconds; FOV = 14 cm; matrix = 256 × 128; slice thickness = 4 mm; views per segment = 64; time of recovery = 1.2 seconds; spin-lock frequency = 500 Hz; ARC [Autocalibrating Reconstruction for Cartesian imaging] phase acceleration factor = 2; time of spin lock [TSL] = 0/10/40/80 milliseconds for T1ρ; preparation TE = 0/13.7/27.3/54.7 milliseconds for T2), and (3) sagittal T2-weighted 3D fast spin echo (TR/TE = 4000/49.3 milliseconds; slice thickness = 1.5 mm; spacing = 1.5 mm; FOV = 16 cm; matrix = 512 × 512; echo train length = 9). The first 2 sequences were acquired with the knee unloaded; the third sequence was acquired with the knee extended and flexed (∼30°) with 25% body weight applied axially as previously explained. 15 This third sequence was used for tibial position and internal tibial rotation analysis. The combined time for acquisition of the T1ρ and T2 sequences was 9 minutes and 37 seconds, with the total time for 1 knee scan, including setup, being less than 1 hour.
qMRI Meniscal Analysis
All image postprocessing was performed with a MATLAB program (MathWorks) developed in-house.
5,8
CUBE images were rigidly registered onto the first T1ρ-weighted image (TSL = 0) and subsequently used for meniscus segmentation at the baseline time point. Menisci were segmented by a single trained user on registered baseline CUBE images into 4 regions: anterior horn (AHLAT) and posterior horn (PHLAT) of the lateral meniscus and anterior horn (AHMED) and posterior horn (PHMED) of the medial meniscus (Figure 1). Three consecutive segmentations were used in each region. For all time points after baseline, a process of auto-segmentation was performed. For auto-segmentation, a longitudinal nonrigid registration was adopted to align the follow-up image on the baseline scan. The registration deformation field was computed in the T1ρ-weighted image with TSL = 0 characterized by a higher signal-to-noise ratio and then applied on all the later echoes. T1ρ and T2 maps were then computed voxel by voxel by fitting the monoexponential decay:

Segmentation images of meniscal horns: (A) anterior horn of the medial meniscus (AHMED), (B) posterior horn of the medial meniscus (PHMED), (C) anterior horn of the lateral meniscus (AHLAT), and (D) posterior horn of the lateral meniscus (PHLAT).
The menisci of patients who underwent partial meniscectomy were segmented at 6 months by a single trained user (A.R.M.), and for all the later time points, the same previously mentioned auto-segmentation process was adopted to align the follow-up image on the 6-month scan.
All auto-segmentations were quality checked by 2 trained users (A.R.M. and J.K.). Each auto-segmentation was evaluated and manually changed if it did not capture >80% of the meniscal area. Auto-segmentations alone correctly defined >90% of all segmentations used in this analysis. Intraclass correlation coefficients (ICCs) were calculated to determine the presence of interobserver bias between T1ρ and T2 relaxation times generated from auto-segmentations corrected by the 2 trained users. The ICCs of 0.961 (95% CI, 0.927-0.980) for T1ρ and 0.960 (95% CI, 0.924-0.979) for T2 relaxation times were comparable with results reported in the current literature on segmentation reproducibility. 9,42
qMRI Tibial Position and Internal Tibial Rotation Analysis
To determine the tibial position and internal tibial rotation, tibia and femur manual segmentations of the baseline contralateral knee were used to establish a coordinate system using an in-house MATLAB program previously described and demonstrated to have good reproducibility. 7,8,20 An iterative closest point registration technique was used to fit 3D cloud points obtained from segmentations. 30 The 3D nature of the registration allowed us to calculate the tibial position (the distance between the tibial and femoral coordinate systems) and internal tibial rotation (rotation of the tibia with respect to the femur), with a more positive tibial position corresponding to a more anterior position and a more positive internal tibial rotation corresponding to a more internally rotated knee.
Statistical Analysis
Statistical analysis was performed using R version 3.4.0. Means and standard deviations of T1ρ and T2 values, tibial position, and internal tibial rotation were calculated at all time points for injured, contralateral, and control knees. To assess for variability of T1ρ and T2 values longitudinally in our comparison groups, 2-tailed Student t tests were used to compare T1ρ and T2 values of control and contralateral knees between time points within a given meniscal region. For cross-sectional analysis, 2-tailed Student t tests were used to compare T1ρ and T2 values, tibial position, and internal tibial rotation of ipsilateral knees with contralateral knees (paired t tests) and control knees (unpaired t tests).
Multiple linear regression was used to assess the correlations between the tibial position of ipsilateral knees at 3 years and 3-year changes in either T1ρ or T2 values of all 4 meniscal regions of ipsilateral knees. Valid regression models met the following criteria: (1) studentized residuals were normally distributed, (2) there was nonmulticollinearity of variables, (3) there was a significant F statistic (P < .05), (4) there was demonstrated independence of residuals, and (5) the data were nonheteroscedastic. Age, sex, and body mass index were not included in the models. Although some of these factors have been previously shown to affect T1ρ and T2 in cartilage, the same effect has not been documented in meniscal qMRI analysis. 2 Additionally, the decision to look at individual changes in T2 from baseline to 3 years acted as an internal control for any physiological differences in T1ρ or T2. Significance was defined as P < .05 for both the Student t test and the regression analysis.
The multiple regression analysis evaluating associations between the tibial position at 3 years and 3-year changes in T1ρ values did not meet the validation parameters discussed above and thus was not included in this analysis.
Results
Patient Demographics
There were no significant baseline differences between the ACL group and control group with regard to age, sex ratio, body mass index, or Marx activity rating scale results.
Tibial Position and Internal Tibial Rotation
The tibial position of ipsilateral, contralateral, and control knees at all time points are displayed in Figure 2. The mean tibial position of ipsilateral knees was more anterior than that of contralateral knees at all time points (baseline: P < .001; 6 months: P = .002; 1 year: P = .013; 2 years: P < .001; 3 years: P = .015). Additionally, the mean tibial position of ipsilateral knees was more anterior than that of control knees at 3 years (P = .010). The mean internal tibial rotation of ipsilateral knees was more internally rotated than that of contralateral knees at baseline only (P = .034). There were no significant differences found between the mean internal tibial rotation of ipsilateral knees and that of control knees at any time point. Additionally, in the ACL group, there was no significant difference in the tibial position or internal tibial rotation between those who underwent partial meniscectomy and those who did not or between those who received an allograft and those who received an autograft at any time point.

Mean tibial position (TP) of ipsilateral (Ipsi), contralateral (Contra), and control knees at all time points. Ipsilateral knees were significantly (P < .05) more anterior than contralateral knees at all time points and control knees at 3 years only. Error bars = ±1 SD.
T1ρ and T2 Meniscal Relaxation Times of Injured Versus Noninjured Knees
The T1ρ and T2 relaxation times of the PHLAT and PHMED in ipsilateral, contralateral, and control knees at all time points are displayed in Figure 3. The mean T1ρ and T2 meniscal relaxation times of ipsilateral knees were higher than those of contralateral knees in the PHLAT at baseline, 6 months, and 1 year (baseline T1ρ: P = .001; baseline T2: P = .003; 6-month T1ρ: P = .030; 6-month T2: P = .047; 1-year T1ρ: P = .002; 1-year T2: P = .020) and in the PHMED at 6 months and 1 year (6-month T1ρ: P = .003; 6-month T2: P = .003; 1-year T1ρ: P = .008; 1-year T2: P = .005). Additionally, the mean T2 of ipsilateral knees was higher than that of contralateral knees in the AHLAT at baseline (P = .010) and in the PHMED at baseline and 2 years (baseline: P = .009; 2 years: P = .026). There were no significant differences found between the mean T1ρ or T2 in the AHMED of ipsilateral knees compared with the mean T1ρ or T2 in the AHMED of contralateral knees.

Mean relaxation values of all knees: (A) posterior horn of the lateral meniscus (PHLAT) T1ρ, (B) PHLAT T2, (C) posterior horn of the medial meniscus (PHMED) T1ρ, and (D) PHMED T2. Error bars = ±1 SD. *Ipsilateral (Ipsi) vs contralateral (Contra): P < .05. ⁁Ipsilateral vs control: P < .05.
T1ρ and T2 Meniscal Relaxation Times of Injured Versus Control Knees
The mean T1ρ and T2 meniscal relaxation times of ipsilateral knees were higher than those of control knees in the PHLAT at baseline and 1 year (baseline T1ρ: P < .001; baseline T2: P < .001; 1-year T1ρ: P = .009; 1-year T2: P = .003) and in the PHMED at 1 year (T1ρ: P = .012; T2: P = .003). Additionally, the mean T2 of ipsilateral knees was higher than that of control knees in both the AHLAT at baseline (P = .018) and in the PHMED at baseline (P < .001). Unexpectedly, the mean T1ρ in the AHMED of ipsilateral knees was significantly lower than the mean T1ρ of control knees at baseline (P = .047); this significant difference was not seen in the T2 meniscal relaxation values. Additionally, in the ACL group, there was no significant difference in T1ρ or T2 values between those who underwent partial meniscectomy and those who did not or between those who received an allograft and those who received an autograft in any meniscal region at any time point.
Analysis of T1ρ and T2 of Control and Contralateral Knees as a Comparison Group
With regard to the use of contralateral and control knees as a stable comparison variable, the mean T1ρ and T2 relaxation times of contralateral knees showed no significant changes between time points in all 4 meniscal regions. The mean T1ρ and T2 relaxation times of control knees additionally showed no significant differences between time points in any of the 4 meniscal regions, except in the AHMED. The mean T1ρ relaxation time in the AHMED of the control knees at baseline was 19.1 ± 1.4 milliseconds, which was unexpectedly significantly higher than the mean T1ρ relaxation time of control knees at 1 year (17.5 ± 2.2 ms; P = .003) and at 3 years (17.6 ± 2.1 ms; P = .004).
Tibial Position and qMRI Regression
Multiple regression analysis showed that a more anterior tibial position at 3 years was associated with increasing T2 values from baseline to 3 years in the PHMED (P = .031) and AHMED (P = .040). The T2 changes from baseline to 3 years in the PHLAT and AHLAT of ipsilateral knees, also included in the same regression model, were not significant. Partial correlation plots in Figure 4 show positive associations between the significant variables.
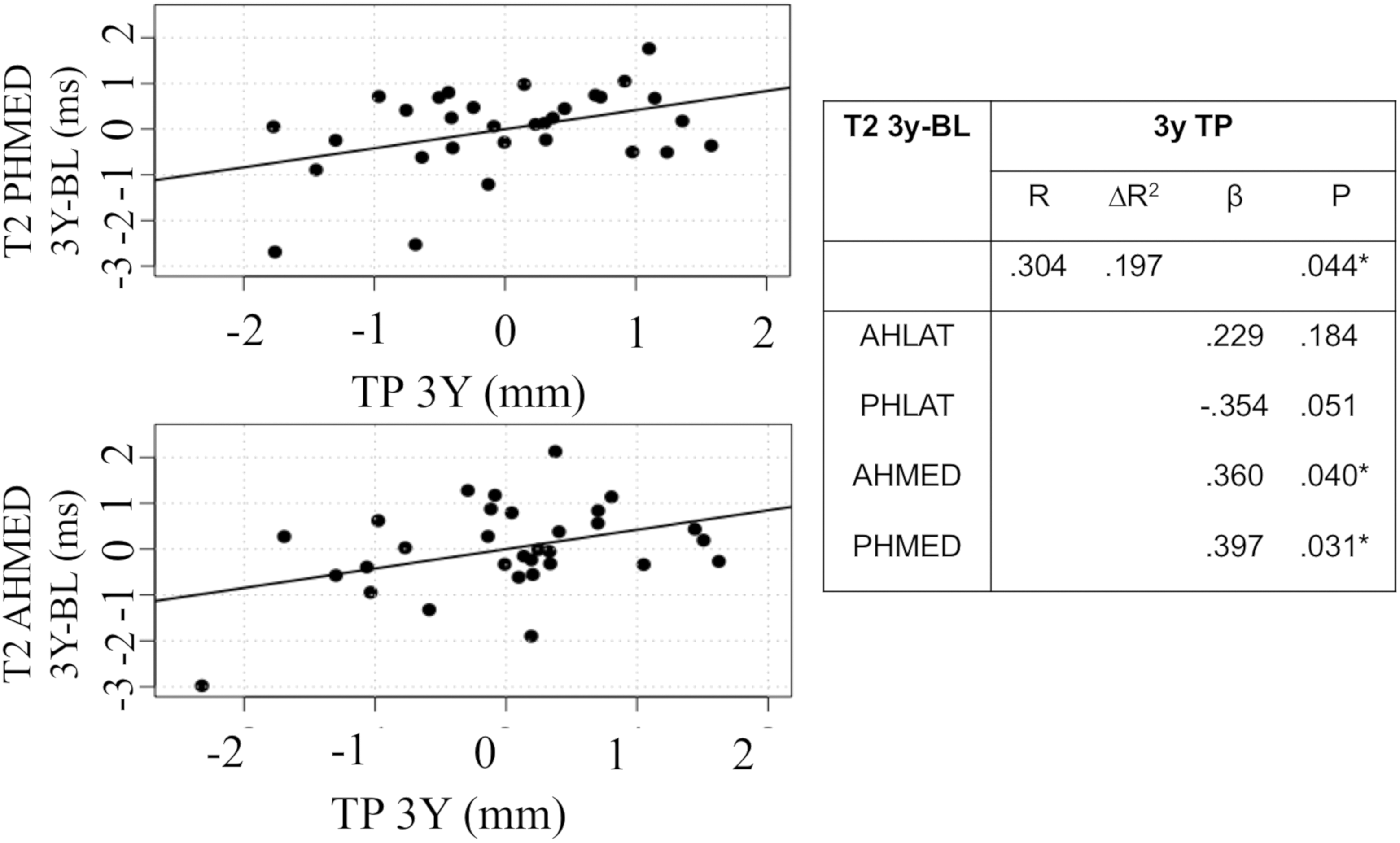
Correlation plots from multiple regression analysis of the tibial position (TP) of ipsilateral knees at 3 years and changes in T2 values from baseline to 3 years of ipsilateral knees. One data point outlier was removed because of residual significant deviation (≥2 SDs) from the mean of residuals. *P < .05. β, standardized regression coefficient, ΔR 2, adjusted R 2 value; AHLAT, anterior horn of the lateral meniscus; AHMED, anterior horn of the medial meniscus; PHLAT, posterior horn of the lateral meniscus; PHMED, posterior horn of the medial meniscus.
Discussion
Although ACL reconstruction clinically allows the restoration of normal activities 1 year postoperatively, more sensitive analysis via qMRI analyzed in this study reported a persistently altered tibial position after ACL reconstruction, as is consistent with the literature. 29 Although there are numerous studies analyzing alterations in tibiofemoral kinematics as they relate to the cartilage status, to our knowledge, this is the first study to show a correlation between the tibial position and sustained alterations in the meniscal matrix in a longer term follow-up after primary ACL reconstruction. 2,15,43
Tibial Position and Internal Tibial Rotation
The tibial position of injured knees was more anterior than the tibial position of noninjured knees at all time points (P < .05), as is consistent with the current understanding of the tibial position after ACL reconstruction. 2,15,43 Despite a persistently anterior tibial position, ACL reconstruction improved internal rotation of the ACL-deficient knee, as differences were only found at baseline. This finding, while consistent with previous studies conducted via qMRI, is contrary to other gait analysis studies that have demonstrated a persistently altered tibial rotation after ACL reconstruction. 2,15,28,31,37 The current literature suggests that knee kinematics can vary between low- and high-demand activities in ACL-reconstructed knees, which may contribute to dissimilarities between the results of our study and those that used gait analysis. 6,13,28
Quantitative MRI
T1ρ and T2 values of the menisci of ipsilateral knees showed prolonged elevations predominantly in the posterior portions of the meniscus: up to 1 year in the PHLAT and 2 years in the PHMED. Elevations in T1ρ and T2 were also seen before surgery with gradual improvement over time, demonstrating that there is an initial meniscal injury that persists in the short term after reconstruction, although it does improve over a longer follow-up. This gradual improvement in the meniscal status after ACL reconstruction has been demonstrated in other studies. 9,18 Chu et al 9 demonstrated in 11 patients who underwent ACL reconstruction and subsequent qMRI 2 years after reconstruction that ultrashort TE T2 values in the posterior medial meniscus decreased 17% to levels that did not significantly differ from those seen in uninjured controls. In addition, there was an unexpected finding of elevated mean T1ρ relaxation times in the AHMED of the control group at baseline, also reported in a previous analysis. 40 The same elevation was not seen in T2 relaxation times at baseline or in T1ρ or T2 relaxation times at 1 or 3 years. No differences were seen in the baseline Marx activity score of the control group, which may have helped explain this surprising observation. A separate analysis of the AHMED of noninjured participants could further elucidate this issue.
Tibial Position and qMRI
An altered tibial position was correlated with increasing T2 values in the medial regions of the meniscus, and given that these correlations were associated over 3 years, it is likely that these changes are related to longer term outcomes as opposed to acute responses related to the initial insult, the chronic ACL-deficient state, or the immediate postoperative recovery period after ACL reconstruction. Alterations in the tibial position leading to increased loading of the cartilage and the development of subsequent osteoarthritis are a well-researched phenomenon; however, an understanding of how alterations in loading affect meniscal abnormalities is still being elucidated. 3,4,33,35
A proposed mechanism is that with persistent anterior translation of the tibia, the PHMED acts as a secondary restraint to translation, leading to increased contact forces and subsequent meniscal injuries. In a study by Guess and Razu, 14 computational multibody models of the knee generated from the medical images and recorded passive leg motion of 2 female participants predicted that loss of the ACL increased contact and hoop forces in the medial menisci by a factor of 4 when a 100-N anterior tibial force was applied. In Markolf et al, 24 in vitro analysis of 12 fresh-frozen knee specimens demonstrated increased forces on the PHMED attachment when a joint-loaded ACL-deficient knee was subjected to a 200-N anterior tibial force while flexed between 20° and 90°. Markolf et al 24 additionally postulated that increased shear forces can lead to the development of medial meniscal tears, limiting the ability of the meniscus to act as a secondary stabilizer and leading to further joint degeneration.
Additionally, despite finding correlations between the tibial position at 3 years and 3-year changes in the meniscal status, we did not find any significant differences between the mean T1ρ or T2 between the comparison groups and the ACL group at 3 years. Although no specific longitudinal comparison analysis was performed in this study, our multiple regression analysis suggests that there are patients who have an improved meniscal matrix 3 years after reconstruction but also a solid subset of patients that worsen 3 years after reconstruction. In the regression analysis, more than half of the patients had positive residuals from T2 values in the PHMED from baseline to 3 years, suggesting that there may be additional factors contributing to worsening meniscal outcomes. Findings from this study encourage further longitudinal analyses to examine additional factors that may influence outcomes after ACL reconstruction.
Limitations
This study has several limitations. The use of static qMRI, while previously proven to be sensitive for changes in the tibial position, cannot fully evaluate tibiofemoral joint changes during motion or higher activity levels, which may present with increased laxity, rotation, or translation of the knee. Additionally, the development of meniscal abnormalities as a result of tibial position alterations may take longer than 3 years, and thus, longer follow-ups are warranted.
Conclusion
Results of the current study indicate that after ACL reconstruction, there is a persistently altered tibial position at 3-year follow-up, with an initial preoperative meniscal injury that shows prolonged but gradual improvement. Additionally, correlations between tibial position and changes in the medial meniscal matrix suggest that tibial position may play a role in the increased susceptibility to medial meniscal tears seen after reconstruction.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by a grant from the National Institutes of Health/National Institute of Arthritis and Musculoskeletal and Skin Diseases (P50 AR606752) as well as the AOSSM/Genzyme (Cartilage Initiative Grant). X.L. receives research support from Ferring Pharmaceuticals and UCB. C.B.M. receives research support from Zimmer, Histogenics, and Moximed and is a paid consultant for Stryker, Zimmer, Conmed, Valeris, and Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of California, San Francisco, Human Research Protection Program (No. 11-06734).