
Abstract
Background:
Adolescent gymnasts are at increased risk for wrist pathology due to repetitive high-impact wrist loading during the midgrowth spurt.
Purpose:
To conduct a comprehensive systematic review on the epidemiology and risk factors for wrist pain and injury in adolescent artistic gymnasts.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
Under PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, we searched MEDLINE, EMBASE, CINAHL, Cochrane, and SPORTDiscus from inception to January 2025. We included observational studies of adolescent artistic gymnasts that reported prevalence, incidence, and/or risk factors for wrist pain, acute injuries, chronic injuries (causing physeal stress or not attributable to a specific acute event), or positive ulnar variance (PUV). Where applicable, meta-analyses were conducted to estimate the pooled prevalence and proportion of new cases for each outcome using common- or random-effect models. Results from studies that were not possible to pool were also reported.
Results:
Of the 3650 records identified, 25 studies (185,107 gymnasts) were included for analysis. All evidence was deemed low to very low certainty. Nine studies suggested a pooled wrist pain prevalence of 53% (95% CI, 39%-66%), with 1 study reporting the proportion of new wrist pain cases to be 2% over 1 year. The prevalence of acute wrist injuries reported in 1 study was 34%, and the pooled proportion of new cases was 4% (n = 2 studies; 95% CI, 2%-7%) over a 2-year period. The pooled prevalence of chronic wrist injury was 36% (n = 6 studies; 95% CI, 12%-71%), and the pooled proportion of new chronic wrist injury cases was 5% (n = 2 studies; 95% CI, 3%-10%) over a 2-year period. Two studies suggested a pooled PUV prevalence of 4% (95% CI, 1%-14%), with 1 study reporting the proportion of new PUV cases to be 16% over an 18-month period in preteen gymnasts (mean ± SD age, 10 ± 2 years). Wrist pain was significantly associated with age between 10 and 14 years, increased age at training onset, training intensity, body mass index, years training, and weekly training hours.
Conclusion:
Our review demonstrated that adolescent artistic gymnasts demonstrate an alarmingly high prevalence of acute and chronic wrist pain and wrist injury. Further research on training intensity thresholds and risk reduction strategies is imperative for informing and implementing guidelines that protect the health of this vulnerable population.
Gymnasts have a high incidence of injuries, with previous reports showing rates up to 9.22 per 1000 athlete-exposures. 28 Frequently employed as a weightbearing joint, the hyperextended wrist may experience loads up to twice the gymnast's body weight and at loading rates that exceed 16 times one's weight per second. 34 However, compared with typical weightbearing joints such as the knee, the wrist comprises bones that articulate over smaller contact areas and that contain thinner articular cartilage.36,38,40,45 Consequently, wrist pain is a significant concern in gymnasts, with point and lifetime prevalence rates of 88% and 92%, respectively.33,50 Wrist injuries are also prevalent, making the wrist the most frequently injured area in male gymnasts and the sixth most injured in their female counterparts. 54
Key to the success of artistic gymnasts, specifically, is the production of high forces at the hand and wrist while performing on apparatuses such as the floor and vault. 21 However, for the artistic gymnast in the peak of one's adolescent growth spurt, repeated exposure to such loads may present several consequences to the open physis of the wrist. During this period of rapid skeletal growth, the distal radius and ulnar physes are particularly susceptible to shear and tensile forces that can result in physeal injury, disturbance in chondrocyte mineralization, and longitudinal growth disruption. 15 This overuse physeal stress injury is otherwise known as the “gymnast wrist” (GW). 41 GW has previously been cited among the most common causes of wrist pain or injury in gymnastics.14,23 GW presents in 3 stages, with stage 1 characterized by wrist pain without radiographic abnormalities. 26 Stage 2 demonstrates radiographic findings of physeal change indicating stress (chronic) injury, and stage 3 is determined by acquired positive ulnar variance (PUV) or other growth deformity. 26
Although other high-risk sports have evidence-based guidelines for promoting player safety, including the pitch count in baseball, 32 concussion guidelines in football, 52 and neuromuscular training protocols in soccer, 27 gymnastics lacks similar injury risk reduction guidelines, including that for GW. Increasing awareness of the risk factors associated with wrist pain, injury, and growth disturbances is crucial for developing effective injury risk reduction strategies that promote the health and career longevity of young artistic gymnasts. Previous studies have narratively reported on these outcomes,8,30 but a meta-analysis has yet to be conducted. We wanted to provide a comprehensive systematic review and meta-analysis of literature in this population to provide insights into specific wrist injury mechanisms and identify risk factors. The purpose of this study was to present the prevalence and incidence of wrist pain and other findings associated with wrist injury (including GW) in the adolescent artistic gymnast and to identify and evaluate the risk factors that may contribute to its development. We hypothesized that the prevalence and incidence of wrist pain and wrist injury would be high in adolescent artistic gymnasts and that the risk for these outcomes would be increased among gymnasts in the peak of their adolescent growth spurt.
Methods
Standards for Meta-Analysis of Observational Studies and PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines were followed.
Literature Search and Study Selection
A literature search was conducted in collaboration with a librarian using MEDLINE, EMBASE, CINAHL, Cochrane, and SPORTDiscus (Appendix Table A1, A -E). All databases were searched from inception to January 2025 and no limits were applied. Reference lists of eligible studies and related reviews were reviewed for additional articles. The finalized reference list was imported to an online screening platform (Covidence 2024). Two authors (S.D.F.D, E.D.) independently screened the title and abstract to assess studies’ eligibility for inclusion. These 2 authors then independently screened the eligible studies according to their full text. Conflicts present at either stage were resolved by a third author (A.N.).
Eligibility Criteria
We included observational studies that enrolled an adolescent (≤19 years) artistic gymnast population and reported ≥1 of the following outcomes: prevalence, incidence, and/or risk factors for wrist pain, acute and/or chronic injuries, or PUV in gymnasts. To distinctly evaluate the prevalence and incidence of wrist pathology, studies that reported pain or injury attributed to both the wrist and the hand together or combined acute and chronic types of injuries were excluded. We excluded studies examining adult gymnasts only (>19 years), randomized controlled trials, small case series (N < 20), laboratory-based studies, reviews, posters, or abstracts. We also excluded studies that observed other gymnastic disciplines only (ie, rhythmic, aerobic, acrobatic, or trampoline).
Data Extraction and Risk-of-Bias Assessment
Two reviewers (S.D.F.D. and E.D.) independently extracted study characteristics, gymnasts’ information (competitive level, start age, weekly training hours, total years training, whether pain/injury affected training, apparatuses causing pain/injury), and reported outcomes among eligible studies. If prevalence rates were not reported directly, the number of gymnasts reported to have pain, injury, or PUV was divided by the total number of gymnasts. The proportion of new cases of wrist injury was collected per total number of gymnasts. Studies that reported the outcomes per total number of injuries were reported separately. Wrist pain was defined as the presence of any type of pain in the wrist not attributed to a specific traumatic event or diagnosed injury at the time of data collection. This definition captured overuse-related or idiopathic pain and was considered distinct from wrist injury, which was defined as a discrete diagnosis. Injuries were categorized as acute or chronic based on the definition provided in the respective study. Acute injuries were those described as either sudden onset injuries resulting in time lost from sport or medical treatment or reports of acute wrist sprain, strain, and/or fracture. Chronic injuries were those described as either overuse physeal stress injuries (ie, GW) or diagnosed injuries not attributable to a specific acute event (with or without time lost from sport). For the second objective, we extracted data related to significant risk factors identified via a regression model.
We evaluated the risk of bias in the eligible studies using the following criteria 11 : (1) the representativeness of the study population—considered high risk if participant recruitment was inadequately described or convenience sampling was used; (2) the validity of the outcome assessment—considered high risk if unvalidated/unreliable instruments (eg, self-report questionnaires) were used; and (3) the amount of missing data—considered high risk if >20% of data were missing at follow-up. For studies that reported risk factors, we also assessed the risk of bias using the following criteria 11 : the control of confounding variables—considered high risk if the study did not adjust for ≥3 potential covariates and the method of statistical analysis—considered high risk if the study did not use a standard method of analysis to reduce bias. The same 2 independent reviewers assessed the risk of bias and discussed with a senior author (A.N.) if discrepancies were raised. The overall risk of bias for each study was summarized as high if any one of the criteria was determined to be high risk.
Statistical Analysis
We conducted a meta-analysis for each outcome that was reported from 2 studies using the common-effects model (RStudio 2024, Boston, Massachusetts). Outcomes reported from more than two studies were meta-analyzed using the random-effects model. We quantified the pooled prevalence or pooled proportion of new cases along with the associated 95% CI. We conducted the meta-analysis with prevalence estimates that were transformed using the double arcsine method 6 to avoid the overestimation of weights for studies with estimates toward 100%. We also reported the results of studies that were not possible to pool.
Subgroup Analysis
We defined the following a priori subgroup hypotheses to explain heterogeneity, assuming higher rates of wrist pain/injury with (1) female versus male gymnasts; (2) smaller (<60) versus larger (≥60) studies; (3) competitive- versus noncompetitive-level gymnasts (differentiated based on whether gymnasts participated in competitions); and (4) high versus low risk of bias on a criterion-by-criterion basis. Subgroup analyses were conducted if there were ≥2 studies within each category. For all subgroup differences, significance was set at an alpha of .05.
Certainty of Evidence
We used the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach framework to assess the certainty of evidence. 44 GRADE classifies evidence as high, moderate, low, or very low based on considerations of risk of bias, indirectness, imprecision, inconsistency, and publication bias. We examined heterogeneity for all pooled estimates through visual inspection of forest plots and the I2. For subgroup analyses based on the risk-of-bias components, if no significant association was found, we included all studies and did not rate down for risk of bias. We assessed the small-study effects using Egger test when ≥10 studies contributed to a meta-analysis. One reviewer (S.D.F.D.) assessed all evaluations, and the final assessment was confirmed by the senior author (A.N.).
Results
We identified 3650 records after removing duplicates, of which 25 articles met the eligibility criteria (Appendix Figure A1). Two studies5,19 were published by the same group of authors and both involved participants from the Junior European Gymnastics Championships. As the study population overlapped, we included the most recent publication 5 only. The majority of included studies implemented a cross-sectional design (n = 14), †† followed by a retrospective design (n = 5),1,20,37,49,55 prospective design (n = 5),2,7,16,31,35 and case series (n = 1). 41
Most studies (n = 20) ‡‡ included competitive-level gymnasts. Two studies10,46 included members of a Chinese opera school who performed gymnastics-like training and three1,49,55 did not report gymnasts’ competitive level (Table 1). Seven studies3,15,16,18,22,41,50 reported the apparatuses on which gymnasts experienced pain or injury. Among the included studies, the sample size ranged from 19 to 183,139 participants and the mean female proportion was 76%. The median age of gymnasts was 12 years (IQR, 11-14). Among the 8 studies in which it was recorded,2-4,15-17,20,43 the median body mass index (BMI) was 17 kg/m2 (IQR, 17-18). Across studies, the median age at which gymnasts commenced training was 6 years (IQR, 5-7), the median hours of training per week was 17 hours (IQR, 12-22), and the median total years of training was 6 years (IQR, 5-8). Across 6 studies,3,15,16,18,22,50 wrist pain and/or injury affected training (ie, limited performance or caused time lost) for 30% to 63% of gymnasts. The method of assessing wrist pain or injury and the time that either was observed varied among the included studies (Appendix Table A2).
Characteristics of Included Studies a
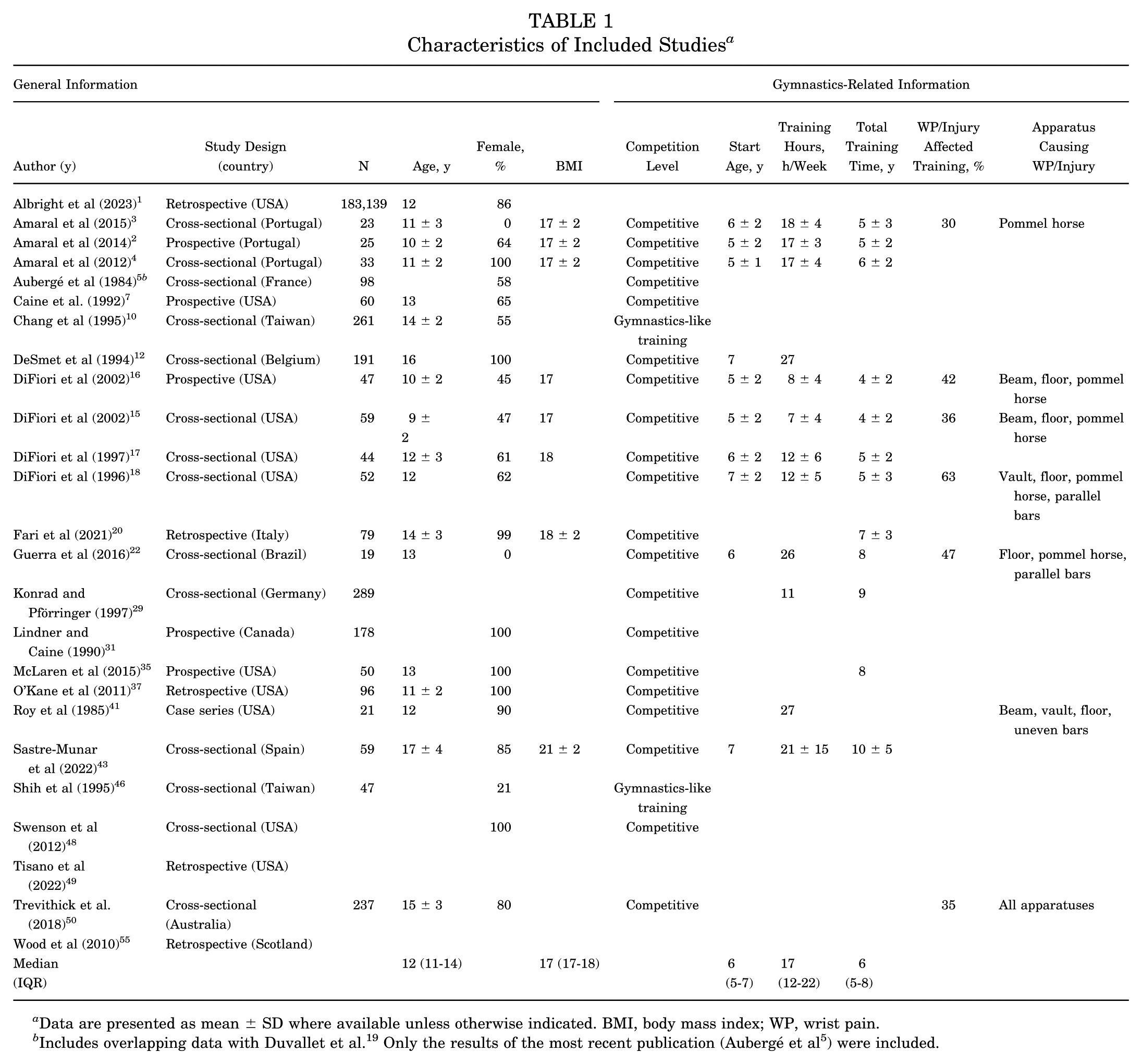
Data are presented as mean ± SD where available unless otherwise indicated. BMI, body mass index; WP, wrist pain.
Risk of Bias
Among the eligible studies, 80% (20 out of 25) §§ were considered to have a high risk of bias in ≥1 criterion. Sixteen studies ‖‖ failed to recruit a representative population, 11 studies ¶¶ did not use a valid tool for assessing outcomes, and 5 studies20,29,31,37,50 reported a high rate of missing data (Appendix Table A3). Among studies that reported risk factors, 50% (2 out of 4)20,22 were considered to have a high risk of bias, with both demonstrating high risk in each of the criteria used (Appendix Table A4).
Wrist Pain
Very low certainty of evidence from 9 studies ## (n = 839 adolescent gymnasts) suggested a pooled prevalence of wrist pain of 53% (95% CI, 39%-66%; I2 = 91%) (Table 2, Appendix Figure A2). No subgroup analyses were significant (Appendix Figure A3). Only 1 study 16 reported the proportion of new cases of wrist pain, which was 2% (1/47 gymnasts) over the 1-year study period.
GRADE Evidence Profile With Summary of Findings a

GRADE, Grading of Recommendations Assessment, Development and Evaluation; PUV, positive ulnar variance; ROB, risk of bias.
Certainty of evidence was not rated down on the basis of ROB because the subgroup analyses did not show a significant difference between each ROB component and the estimation (Appendix Figure A3, B-D).
Serious unexplained inconsistency (I2 = 75%-100%).
Acute Wrist Injury
Only 1 study 46 reported the prevalence of acute wrist injury per total number of gymnasts, which was 34% (16/47 gymnasts). Data from 3 studies29,48,55 reported that acute wrist injury accounted for between 22% and 46% of the total number of injuries.
Low certainty of evidence from 2 studies31,37 (n = 274 adolescent gymnasts) suggested a pooled proportion of new cases of acute wrist injuries over a median 2-year period of 4% (95% CI, 2%-7%; I2 = 39%) (Table 2, Appendix Figure A4A). Additionally, 2 studies not included in the meta-analysis because of insufficient data reported the proportion of new cases of acute injury as 5% over an 8-year period 1 and 10% over a 7-year period. 49
Chronic Wrist Injury
Very low certainty of evidence from 6 studies5,7,12,17,22,41 (n = 433 adolescent gymnasts) suggested the pooled prevalence of chronic wrist injury was 36% (95% CI, 12%-71%; I2 = 96%) (Table 2, Appendix Figure A5). No subgroup analyses were significant (Appendix Figure A6).
Very low certainty of evidence from 2 studies31,37 (n = 274 adolescent gymnasts) suggested a pooled proportion of new cases of chronic wrist injuries over a median 2-year period of 5% (95% CI, 3%-10%; I2 = 83%) (Table 2, Appendix Figure A4B).
Positive Ulnar Variance
Very low certainty of evidence from 2 studies3,4 that employed the Hafner Method for skeletally immature patients (n = 56 adolescent gymnasts) suggested a pooled prevalence of PUV of 4% (95% CI, 1%-14%; I2 = 0%) (Table 2, Appendix Figure A7). Across all gymnasts in these studies, the mean age was 11 ± 0.05 years, and the mean ulnar variance (UV) was −3 ± 2 mm. The remaining studies employed the method of perpendiculars 10 or the concentric circle technique, 12 both of which are more appropriate for skeletally mature individuals. Respectively, these studies reported PUV prevalence rates of 46% (mean age, 14 ± 2 years; mean UV, +0.5 ± 2 mm) and 71% (mean age, 16 years [SD not reported]; mean UV, +2 ± 1 mm). A single study among 25 gymnasts aged 10 ± 2 years reported that 16% acquired PUV after 18 months. 2
Wrist Pain Risk Factors
Four studies16,18,20,22 reported the risk factors associated with wrist pain in adolescent gymnasts (Table 3); however, their findings could not be meta-analyzed due to insufficient data. Multiple factors related to wrist pain were investigated including age, age at training onset, training intensity, BMI, years of training, and weekly training hours. Risk factors related to the chronological age of gymnasts were cited most frequently.16,18,20 Only 1 study 18 reported the adjusted odds ratio (AOR) for significant risk factors among gymnasts including age >10 years (AOR, 16.28), age <14 years (AOR, 208.51), older age at training onset (AOR, 1.97), and increased intensity of training (AOR, 1.19) (defined as the product of training hours per week and competitive level grouping). Based on these findings, the risk for wrist pain was suggested to be significantly increased in gymnasts between 10 and 14 years old. 18 Another study also reported increased BMI (OR, 1.72) and increased number of years training (OR, 1.02) as significant risk factors. 20
Significant Wrist Pain Risk Factors a

BMI, body mass index; NR, not reported.
In studies reporting on specific events,3,15,16,18,22,41,50 all gymnastics apparatuses (floor, pommel horse, balance beam, vault, parallel bars, horizontal bars, uneven bars, rings) were reported to cause wrist pain or injury (Table 1). However, the floor was the most reported apparatus used by both sexes to cause pain or injury among the studies.15,16,18,22,41,50 The pommel horse3,15,16,18,22,50 and balance beam15,16,41,50 were the most reported male-only and female-only apparatuses, respectively.
Discussion
The major finding of this systematic review and meta-analysis of 25 studies was that young gymnasts demonstrated an alarmingly high prevalence of wrist pain and wrist injury. The highest risk identified was in 10- to 14-year-olds, which corresponds to the adolescent growth spurt. Wrist pain occurred in 53% of adolescent artistic gymnasts with a proportion of new cases of 2% over 1 year. Acute wrist injury occurred in 34% with a proportion of new cases of 4% over a median 2-year period, and chronic wrist injury occurred in 36% of adolescent gymnasts with a proportion of new cases of 5% over a median 2-year period. This study also found that PUV occurred in 4%, with a proportion of new cases of 16% over an 18-month period in preteen gymnasts.
While this study failed to establish a direct relationship between rates of distal radial physeal stress injury (GW) and PUV, it has previously been reported that GW can result in a 10% growth disturbance rate with 3% of those affected requiring surgical correction. 25 Despite the acknowledgement for such consequences in the literature, this review identified a lack of consistent and specific reporting of the GW diagnosis across included studies. This makes it impossible to determine the true pooled rates of related complications such as pain or permanent skeletal changes.
The current review demonstrated that ages between 10 and 14 years, as well as increased age at training onset, training intensity, BMI, years of training, and weekly training hours were significant risk factors for wrist pain development in adolescent gymnasts. Risk factors related to the chronological age of gymnasts were cited most frequently.16,18,20 Only 1 study 18 quantified the AOR for this variable and observed gymnasts between 10 and 14 years old to be at increased risk. This age cohort coincides with the onset of the adolescent growth period and encompasses the period of peak growth velocity (PGV), which occurs around 11 to 12 years in girls and 13 to 15 years in boys51,53 and reflects the maximal growth during the midgrowth spurt. 51 During this period, alterations in the rate of mineralization cause temporary weakness, making the distal radial physis increasingly susceptible to injury. 18 Repeatedly exposing the wrist to high-impact loads during the vulnerable PGV period may explain the relationship between age and gymnasts’ increased risk for wrist pain. Microtraumatic changes to the distal radial physis that result from these repetitive, high-impact wrist loads may also explain the association of wrist pain/injury with increased training intensity, increased BMI, more years of training, and longer weekly training hours. 26 Furthermore, gymnasts who initiate their training at a later age may be closer to/within this vulnerable growth period, possibly increasing the risk for wrist pain/injury that is a direct result of GW. 18
Future Recommendations
Adolescent gymnasts experience high-intensity training during the period of peak skeletal growth. 13 This highlights the need for evidenced-based SafeSport guidelines that optimize long-term wrist health by minimizing injury and permanent growth disturbances. Prospective studies using validated and systematically collected outcome measures are recommended to improve the epidemiological understanding of diagnosis-specific risk factors and to clarify the influence of training volume and training intensity on pain or injury. These are necessary to inform future injury surveillance tools and establish parameters for risk reduction guidelines. Finally, studies that examine other biomechanical and morphological factors suggested to influence wrist pain and injury risk, such as wrist braces, soft mats, and joint angles,9,24,39,41 will further aid in developing guidelines that are both relevant and informed.
Strengths and Limitations
The main strengths of this study include the conducting of a comprehensive search and applying of explicit eligibility criteria, which allowed for inclusion of more studies in the current review compared with previous related reviews,8,30 as well as pooling of key outcomes. This review, however, was limited by the inclusion of studies with high risk of bias, as well as by heterogeneous definitions of pain/injury, study designs, and reported outcomes. Many studies reporting risk factors failed to present odds ratios or report on other athlete-specific and external factors previously suggested to influence GW risk. 53 Last, the failure to discriminate among specific wrist injury diagnoses including GW, as well as a general tendency for gymnasts to underreport wrist pain or injury42,47 and overconformity to sport ethics, may all contribute to an underrepresentation of the true prevalence and incidence of the reported outcomes included in this study.
Conclusion
Our review demonstrated that adolescent artistic gymnasts demonstrate an alarmingly high prevalence of acute and chronic wrist pain and wrist injury. Further research on training intensity thresholds and risk reduction strategies is imperative for informing and implementing guidelines that protect the health of this vulnerable population.
Footnotes
Appendix
The following searches were conducted on February 2, 2024, and January 14, 2025.
Final revision submitted August 15, 2025; accepted September 18, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study is supported by the Tanenbaum Institute for Science in Sport (TISS) Research Accelerator Grant. The TISS grant has supported conference fee reimbursement to present this research at the Annual TISS conference and supports the umbrella research program under which this project falls. S.D.F.D. has received funding from the Canada Graduate Scholarships–master’s program and partial funding under the TISS Research Accelerator Grant. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.