
Abstract
Background:
Recurrent tears of the rotator cuff pose a substantial problem despite advances in repair technique. Biologic augmentation via marrow stimulation or vented anchors may strengthen the suture-tendon junction and improve healing rates of native tissue, thereby enhancing outcomes of primary surgical repair.
Purpose:
To provide a focused systematic review and meta-analysis of local, intraoperative marrow-derived augmentation techniques in clinical primary rotator cuff repair.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A systematic review of PubMed, Embase, and Cochrane was conducted following PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. A total of 2131 studies from 2010 to 2022, focused on either marrow stimulation or vented anchors, were isolated and classified as either preclinical or clinical. Meta-analysis was performed for comparative marrow stimulation and vented anchor studies. Heterogeneity was tested through calculation of I 2.
Results:
A total of 13 clinical studies were included in the review. All 9 comparative studies included in the meta-analysis demonstrated high methodologic quality or a low risk of bias. The pooled retear rate across all 9 clinical studies for patients undergoing marrow stimulation was 11%. For the 5 studies in the meta-analysis, the pooled retear rates were 15% for marrow stimulation and 30% for controls. Meta-analysis demonstrated a significant difference in the overall retear rate that favored marrow stimulation (odds ratio [OR], 0.41; 95% CI, 0.25-0.66; P = .0003; I 2 = 0%). Similarly, meta-analysis of the Constant score at final follow-up demonstrated a statistically significant difference between the 2 groups that favored a higher Constant score in the marrow stimulation group (mean difference, 2.84; 95% CI, 1.02-4.66; P = .002; I 2 = 29%). Vented anchors demonstrated improved ossification and bone density at the anchor site, but no difference in outcomes or retear. Pooled retear rates were 22.5% for vented anchors and 27.8% for controls.
Conclusion:
Current evidence demonstrates that marrow-stimulation techniques may have a positive impact on healing and retear rate, while vented anchors have a muted impact relative to nonvented anchors. Although available evidence is limited and more research is needed, findings to date suggest that marrow stimulation techniques may be an inexpensive, straightforward technique to consider in qualifying patients to prevent rotator cuff retears.
Keywords
Rotator cuff repair (RCR) is a frequently performed orthopaedic procedure that improves function and reduces pain in patients with rotator cuff tears. The incidence of RCR has risen dramatically, with 1 study showing a 188% increase in total RCRs from 2007 to 2015. 8 Despite considerable advancements in technique, retear rates remain suboptimal. 5 Although the incidence of retear on magnetic resonance imaging (MRI) after RCR may be as low as 11% at the 2-year follow-up, retears of large to massive tears occur with higher frequency, with 1 study demonstrating up to 94% mechanical failure. 13,21 Additionally, multiple imaging studies demonstrate that a majority of rotator cuff retears occur within 3 to 4 months of the initial repair. 17,25 These early postoperative failures suggest that tendon healing may take longer than expected, especially in light of reported results of a failed healing response and decreased vascularity as tear size increases. 20,23 Failed RCR may result in altered glenohumeral joint kinematics, which may cause superior humeral translation, articular wear, and ultimately cuff tear arthropathy. 36
Researchers often cite insufficient mechanical strength and lack of biological healing as the primary modes of rotator cuff failure. 30 Advances in suture materials and anchors, in addition to the development of innovative surgical techniques (eg, double-row transosseous equivalent repair), have led to improved mechanical strength and lower retear rates on MRI. 3,38 That leaves the suture-tendon interface, which in an RCR construct is highly susceptible to failure. 30 This leads to suture pull-through, which is a result of reduced tissue quality and may result in tear progression. 30 Biologic augmentation may be utilized to strengthen the suture-tendon junction during surgical repair, thereby improving healing rates. The past decade has yielded many exciting, novel biological augmentation approaches that aim to increase healing rates and improve surgical outcomes, including local, procedural bone marrow augmentation via venting, microfracture, and vented anchors. Marrow stimulation via microfracture and marrow venting, as well as use of vented anchors, is a method of stimulating elution of marrow elements (eg, mesenchymal stem cells, growth factors, and chemotactic cytokines) via breaks/pores in the proximal humeral cortex at the site of RCR. 9,10 Such techniques are proposed to improve healing by recruiting healing factors from the subchondral bone to fill defects within fibrocartilage repair tissue. 1 Preclinical data show promising biomechanical and histological results when employing marrow stimulation and vented anchors in the setting of RCR. 1,16,22 Additionally, the use of complementary mechanisms that further enhance the healing response may provide synergistic benefits above those of microfracture and vented anchors alone, but require further examination. 11,16 Overall, the role of bone marrow augmentation demonstrates promise in reducing retear rates and avoiding progression to massive rotator cuff tears. 1,9,10,18,22,24,28,31 However, additional evidence is required to elucidate indications for use and enable clinical translation.
The purpose of this study was to provide a focused, updated systematic review and meta-analysis of intraoperative marrow stimulation techniques in the clinical setting. We hypothesized that both marrow stimulation techniques and vented anchors would demonstrate improvements in retear rates and functional outcomes, given preclinical evidence suggesting improvement in biomechanical and histological parameters with intraoperative marrow-elution techniques. 1,16,22
Methods
Literature Search and Study Selection
A systematic review was performed using the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. 27 Relevant paper selection was performed by 2 independent reviewers (M.O. and A.C.), with the senior author (S.S.) acting as an arbiter for any disputes. The search utilized the PubMed central database in February 2022 and the Embase and Cochrane databases in August 2022. The search terms used were ((((microfracture) OR (vented anchors) OR (crimson duvet) OR (platelet rich plasma)) OR (amnion)) OR (adipose tissue)) OR (bone marrow aspiration concentrate)) OR (nandrolone)) OR (augmentation)) OR (biologics)) OR (growth factors)) OR (gene therapy)) OR (stem cells)) OR (tissue engineering)))) AND (((rotator cuff repair) OR (single-row repair)) OR (double-row repair))), with filters as follows: date range of January 1, 2010, to January 31, 2022; and English language. The initial search resulted in 2131 titles (1201 titles on PubMed, 758 on Embase, and 172 on Cochrane), to which the following criteria were applied. Papers that focused on RCR and augmentation techniques in peer-reviewed journals were included. Review articles, systematic reviews, editorials, technique articles, papers that lacked patient-reported outcomes or the appointed outcome surrogates, and case reports were excluded. After application of the exclusion criteria, 306 titles (260 titles on PubMed, 34 titles on Embase, and 12 on Cochrane) remained for abstract review. Duplicates were removed and the abstracts of the articles were then reviewed.
Excluded were case series with <15 patients; review articles not previously eliminated; articles not related to primary RCR; studies focused on augmentation that did not address either bone marrow, injectable biologics, or grafts/scaffolds; studies with a minimum average follow-up of <24 months; and those without an accessible abstract. At this step, a total of 80 articles were excluded, leaving 199 (195 on PubMed, 3 on Embase, and 1 on Cochrane) for full-text review. Full-text inclusion criteria were studies with a clearly reported healing rate; any patient-reported outcome measure; and clearly reported load-to-failure, load-to-gap, gap size, and stiffness for preclinical augmentation titles. Additionally, final selection was focused exclusively on clinical marrow induction techniques or vented anchors; thus, studies with a focus on graft/scaffolds or injectable biologics as well as preclinical studies were excluded. The full-text review resulted in the inclusion of 13 studies, of which 9 were focused on marrow stimulation methods and 4 on vented anchors. The 13 clinical studies comprised 3 level 1, 3 level 2, 3 level 3, and 4 level 4 studies. A graphical description of the search methodology has been provided (Figure 1).
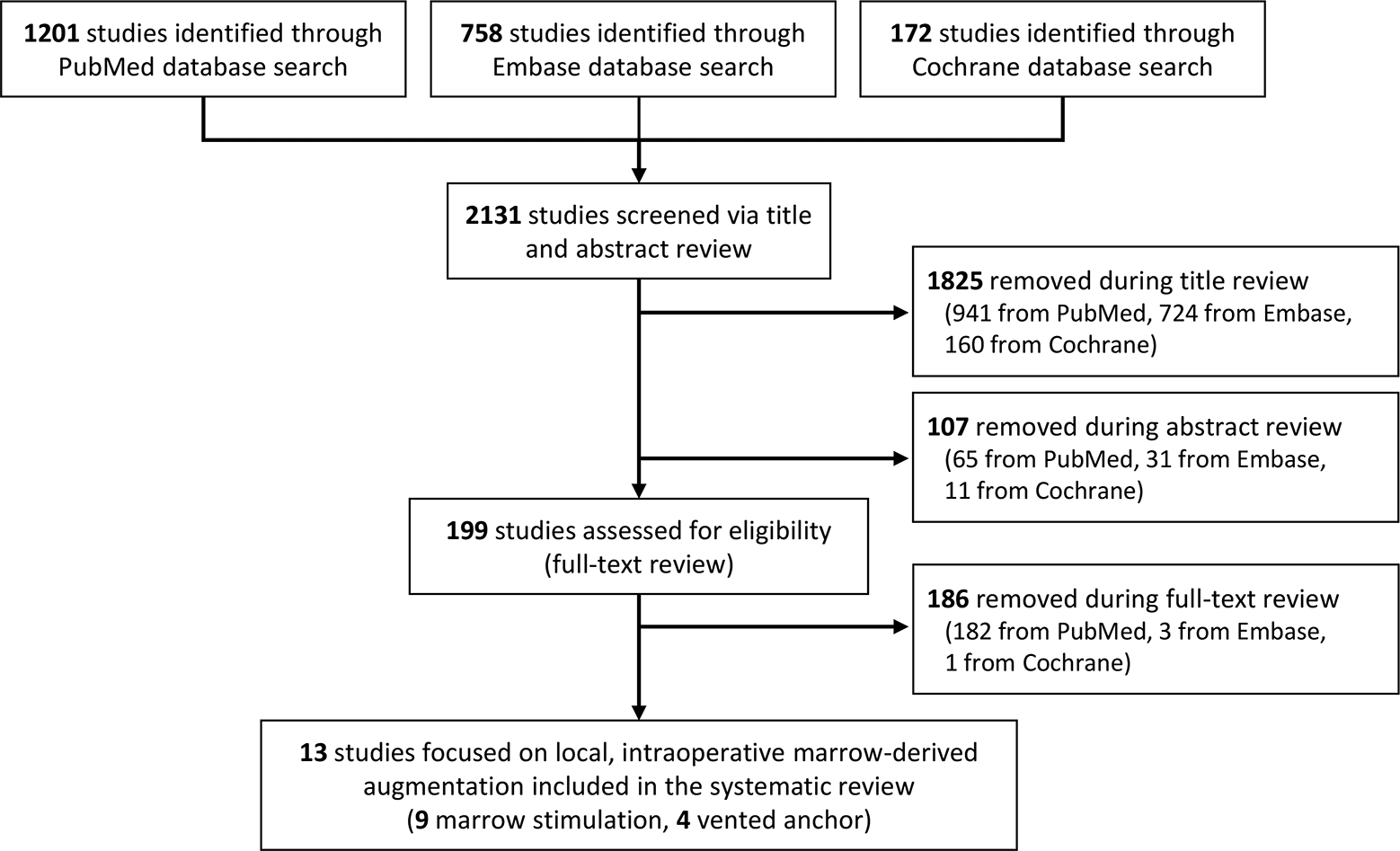
Flowchart of systematic review performed according to PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines.
Outcomes and Statistical Analysis
The 13 included studies were reviewed by 3 independent medical student reviewers (S.L., O.B., A.M.) for data on study size, mean age, sex, interventions, follow-up, and outcomes, with all disputes and final results reviewed by the principal investigator (S.S.S.). Five marrow stimulation and 3 vented anchor studies were identified to be appropriate for inclusion in the meta-analysis. Studies without comparators or low levels of evidence were not included in the meta-analysis but included in the overall study. Retear rate and Constant score were imported into Review Manager 5.4 (The Cochrane Collaboration) for analysis. For all meta-analysis studies, heterogeneity was tested through calculation of I 2.
Methodologic Quality Assessment
Assessment of the quality and risk of bias of all studies included in the meta-analysis was performed by an independent reviewer (S.L.). The Checklist to Evaluate a Report of a Non-Pharmacological Trial (CLEAR-NPT) was used to evaluate the 6 randomized controlled trials included in the study (3 marrow stimulation and 3 vented anchor). 2 A high CLEAR-NPT score (>7 points on a 10-point scale) is indicative of high methodologic quality. The methodologic index for nonrandomized studies (MINORS) was used to determine risk of bias in the 3 nonrandomized comparative studies (2 marrow stimulation and 1 vented anchor). 36 For comparative studies, 24 is considered an ideal score and given a grade of “A.” Studies with a score from 21 to 23 are given the grade “B” but are also considered to be of high quality. A score <21 is considered to have a high risk of bias and is graded as “C.” The MINORS criteria were also used to evaluate risk of bias in 4 nonrandomized, noncomparative marrow stimulation studies. For noncomparative studies, 16 is considered an ideal score. Studies with a score from 13 to 15 are given a grade “B,” while studies with a score <13 are given the grade “C.”
Results
Characteristics of All Included Studies
There were 13 articles (9 marrow stimulation and 4 vented anchor) included in the review for analysis, of which 9 were comparative studies. ¶ The studies comprised 1116 patients (515 male, 601 female). Repair techniques were reported in 1051 (94.2%) patients. Single-row repair techniques were performed in 768 (73.1%) patients, while double-row repair techniques were performed in 283 (26.9%).
Results of the Methodologic Quality Assessment
Nine comparative studies were evaluated for quality of methodology. 4,18,19,24,28,31 –33,37 All 6 randomized controlled trials included in the study achieved a good score based on the CLEAR-NPT criteria. 4,19,24,28,33,37 All 3 nonrandomized comparative studies included in the meta-analysis achieved a “B” rating, according to the MINORS criteria, indicating a low risk of bias. 18,31,32 Four noncomparative studies were evaluated using the MINORS criteria. All 4 studies achieved a “B” rating, indicating a low risk of bias. 9,10,12,14
General Study Characteristics for Clinical Studies of Marrow Stimulation
Nine studies evaluated the impact of marrow stimulation in the clinical setting (Table 1). The studies comprised 756 patients (373 male, 383 female). The frequency-weighted age of the patients across all studies was 59.44 years (range, 56-64 years). Repair techniques were reported in 730 (96.6%) patients. Single-row repair techniques were performed in 527 (72.2%) patients. Double-row repair techniques were performed in 203 (27.8%).
Clinical Results of Marrow Stimulation Studies a

a LOE, level of evidence; MCID, minimal clinically important difference; NA, not applicable; NR, not reported; VAS, visual analog scale for pain.
b Study evaluated patients with partial-thickness tears that were completed intraoperatively.
The 5 studies 18,24,28,31,37 included in the meta-analysis comprised 500 patients (219 male, 280 female, 1 not reported). A total of 229 patients underwent bone marrow stimulation, while 271 served as controls. The frequency-weighted age was 59.47 years (range, 57.8-63.1 years). Single-row repair techniques were performed in 297 (59.4%) patients, while double-row techniques were used in 203 (40.6%).
Results From Clinical Studies of Marrow Stimulation
In summary, the 9 studies # focused on marrow stimulation had no reported adverse effects related to the technique and high rates of rotator cuff healing. The pooled retear rate across all 9 studies for patients undergoing marrow stimulation was 11% (50/445). For the 5 studies in the meta-analysis, the pooled retear rates were 15% (33/214) for the interventional group and 30% (74/249) for the control group. 18,24,28,31,37 The meta-analysis of the 5 studies using a fixed-effects model demonstrated a statistically significant difference in the overall retear rate that favored marrow stimulation (odds ratio [OR], 0.41; 95% CI, 0.25-0.66; P = .0003; I 2 = 0%) (Figure 2). 18,24,28,31,37 Similarly, meta-analysis of the Constant score at the final follow-up demonstrated a statistically significant difference between the 2 groups that favored a higher Constant score in the marrow stimulation group (mean difference [MD], 2.84; 95% CI, 1.02-4.66; P = .002; I 2 = 29%) (Figure 2). 18,24,28,31,37 Positive factors associated with MRI-confirmed rotator cuff healing included low levels of fatty infiltration (Goutallier grades 0-2). 10,24 Negative factors for healing included higher patient age, duration of symptoms, amount of tendon retraction, and area of tendon rupture; these were reported in 2 studies. 24,37

Meta-analysis of marrow stimulation techniques in rotator cuff repair (RCR). (A) Meta-analysis of retear demonstrates a statistically significant improvement in retear rate in the marrow stimulation group. (B) Meta-analysis of the Constant score at the final follow-up demonstrates a statistically significant increase in the Constant score in the marrow stimulation population. IV, inverse variance; M-H, Mantel-Haenszel.
Two level 1 evidence studies 24,28 and 1 level 2 evidence study 37 demonstrated variable effect of microfracture as a form of marrow stimulation at the humeral footprint of RCRs. A randomized controlled trial (n = 57) noted reduced pain and improved patient-reported functional scores at 3 months after microfracture RCR, but no significant difference in ROM, functional score, patient-reported outcomes, or return to preinjury sports activity at an average final follow-up of 29 months. 28 A separate level 1 study (N = 73) demonstrated high failure rates in both the microfracture group (34.3%) and the standard repair group (47.4%) and no significant difference in function or patient-reported functional outcomes between the 2 groups at a mean final follow-up of 28.1 months. 24 However, a subanalysis of large 2-tendon tears showed a greater healing rate in the microfracture group (60% vs 12.5%; P < .04). A level 2 evidence study (N = 123) demonstrated no significant difference in healing or functional outcomes at the 6-month follow-up for patients undergoing microfracture. 37 Of note, loss to follow-up was high in this study (22%) and may have affected findings.
All studies employed a small joint arthroscopic awl. Osti et al 28 described the perforations as 3 to 4 mm apart and 2 to 4 mm deep, while Milano et al 24 described their perforations as 4 mm apart, 5 mm deep, and 1.5 mm wide. Toro et al 37 described their perforations as being made at a distance of 3 mm and a depth of 3 to 5 mm. Since the publication of these studies, advances have been made aiming to deepen the channels for better delivery of marrow elements as well as to avoid compromising suture anchor fixation. 9,10,37
Deep marrow venting via multiple channeling or microfracture has been used to promote the release of marrow elements, specifically growth factors and mesenchymal stem cells, at the site of RCR. Prior work confirmed the delivery of mesenchymal stem cells to the repair footprint as a result of multiple channeling via a 2.1-mm bone punch. 18 These cells were obtained at the time of surgery, then isolated and cultured, displaying positivity for CD73, CD90, and CD105. However, the authors found no significant clinical difference at the 2-year follow-up.
Pulatkan et al 31 evaluated the effects of marrow venting via microfracture in the repair of large tears, comparing single-row repair plus marrow venting, single-row repair, and double-row repair. Single-row repair plus marrow venting had the lowest retear rate, as demonstrated by MRI at the 2-year follow-up (14% vs 33% vs 36%, respectively; P = .045). Additionally, single-row repair with marrow venting achieved significantly greater improvement in postoperative functional outcome scores (Constant and visual analog scale scores) relative to double-row repair. 31 Additional level 4 studies have demonstrated retear rates <10% after single-row repair with marrow venting, as well as excellent patient-reported outcomes. 9,10,12 In a recent level 4 study, Hill et al 14 demonstrated that only 52% of patients undergoing microfracture met the minimal clinically important difference across all patient-reported outcomes. However, their study population was small and included a combination of both acute and chronic tears.
General Study Characteristics of Clinical Vented Anchor Studies
Four studies evaluated the impact of vented anchors in the clinical setting (Table 2). The studies comprised 360 patients (142 male, 218 female). 4,19,32,33 The frequency-weighted age of the patients across all studies was 61.2 years (range, 52.0-65.3 years). The most common anchor used was the Healicoil polyetheretherketone (PEEK) anchor (3/4 studies). Repair techniques were reported in 322 (89%) patients. Single-row repair techniques were performed in 242 (75%) patients. Double-row repair techniques were performed in 80 (25%).
The 3 studies 19,32,33 included in the meta-analysis comprised 320 patients (117 male, 203 female). A total of 94 patients underwent RCR with a vented anchor, while 226 served as controls. The frequency-weighted age was 62.3 years (range, 60.0-65.3 years). The technique was reported in 282 (88%) patients, with 242 (86%) patients undergoing single-row repair and 40 (14%) undergoing double-row repair.
Clinical Results of Vented Anchor Studies a
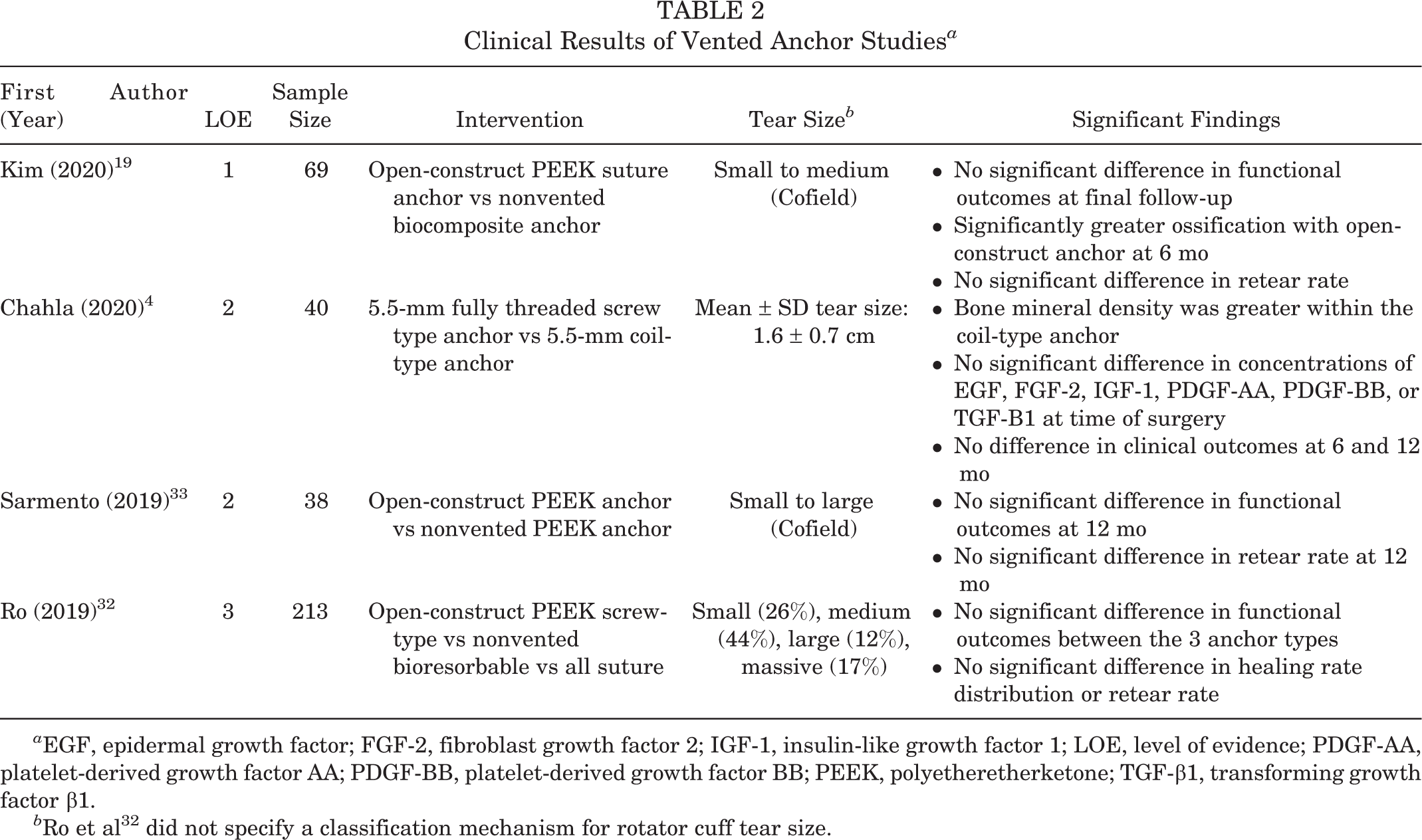
a EGF, epidermal growth factor; FGF-2, fibroblast growth factor 2; IGF-1, insulin-like growth factor 1; LOE, level of evidence; PDGF-AA, platelet-derived growth factor AA; PDGF-BB, platelet-derived growth factor BB; PEEK, polyetheretherketone; TGF-β1, transforming growth factor β1.
b Ro et al 32 did not specify a classification mechanism for rotator cuff tear size.
Results From Clinical Studies of Vented Anchors
Vented anchors are hypothesized to promote healing and superior bone ingrowth due to open-construct architecture that may be used to stimulate elution of stem cells and other marrow elements. 19,33 Four studies evaluated outcomes of RCR with various types of vented and nonvented anchors, ranging from nonvented biocomposite suture anchors to various iterations of open-architecture PEEK anchors (Table 2). Three of the 4 studies were included in the meta-analysis. 19,32,33
In summary, the included clinical studies have not demonstrated clear significant clinical benefit of vented anchors over nonvented anchors. The pooled retear rates for the 3 studies included in the meta-analysis were 22.5% (18/80) for the interventional group and 27.8% (59/212) for the control group. 19,32,33 A fixed-effects model demonstrated no statistically significant difference in the overall retear rate (OR, 0.91; 95% CI, 0.47 to 1.75; P = .28; I 2 = 21%) as well as no difference in the Constant score at the final follow-up (MD, –0.22; 95% CI, –1.40 to 0.97; P = .36; I 2 = 3%) (Figure 3). 19,32,33

Meta-analysis of rotator cuff repair (RCR) with vented anchors. (A) Meta-analysis of retear rate demonstrates no significant difference between the vented anchor and control groups. (B) Meta-analysis of the Constant score at the final follow-up demonstrates no significant difference between the vented anchor and control groups. IV, inverse variance; M-H, Mantel-Haenszel.
A prospective randomized trial by Kim et al 19 evaluated the radiologic and clinical outcomes of open-construct PEEK anchors as compared with nonvented biocomposite suture anchors. The grade of ossification was significantly higher in the open-construct group versus the nonvented group at 6 months. However, there was ultimately no difference between the 2 groups in the rate of cyst formation at 6 months, retear rate at 12 months, or functional outcomes at final follow-up (mean, 25.2 months). Another prospective randomized study evaluating the short-term outcomes of RCR with either vented or solid PEEK anchors demonstrated no significant difference in functional outcome improvement or retear rate at the 12-month final follow-up. 33 A third study by Chahla et al 4 evaluated a novel coil-type open-architecture anchor with a screw-type PEEK anchor. Although the study did not report retear rate, there was no significant difference in patient-reported outcomes at 6 or 12 months. However, it was noted that bone mineral density and total bone mineral mass were greater with the coil-type anchor. Finally, a retrospective comparative study evaluating all-suture, bioresorbable, and open-construct PEEK-type anchors found no statistically significant difference in functional outcomes, healing rates, or retear rates. 32
Discussion
Overall, our meta-analysis demonstrated a statistically significant improvement in retear rate (OR, 0.41; 95% CI, 0.25 to 0.66; P = .0003; I 2 = 0%) and Constant score (MD, 2.84; 95% CI, 1.02 to 4.66; P = .002; I 2 = 29%) in patients undergoing RCR with marrow stimulation. However, it failed to demonstrate improvement in retear rate (OR, 0.91; 95% CI, 0.47 to 1.75; P = .28; I 2 = 21%) or Constant score (MD, –0.22; 95% CI, –1.40 to 0.97; P = .36; I 2 = 3%) in patients undergoing repair with vented anchors.
Local intraoperative marrow-derived augmentation, such as marrow stimulation and vented anchors, demonstrates promise in RCR. Such techniques are proposed to improve healing by recruiting healing factors from the subchondral bone to fill defects within fibrocartilage repair tissue. 18,33 Preclinically, marrow stimulation techniques such as microfracture or marrow venting demonstrate improved histology (eg, thicker collagen bundles) and improved load characteristics. 1,16,22 Cells obtained at the time of surgery display positivity for CD73, CD90, and CD105, although notably the current literature lacks evidence that biologically active factors remain within the repair itself. 18 Studies exploring vented anchors demonstrate improvements in all histopathologic parameters versus untreated samples. 11 However, analysis of marrow elements released at the repair site shows no significant differences in concentrations of epidermal growth factor, fibroblast growth factor 2, insulin-like growth factor 1, platelet-derived growth factor AA, platelet-derived growth factor BB, or transforming growth factor β1) between vented and closed anchors. 4 Concomitant use of multiple augmentation modalities (eg, kartogenin-loaded hydrogel scaffolds plus microfracture or vented anchor) may synergistically improve outcomes in preclinical studies but require further evaluation. 11,16
Our meta-analysis demonstrated a statistically significant improvement in retear rate and Constant score that favored the marrow stimulation group. Marrow stimulation has most often been employed in primary repair in the setting of large tears and has demonstrated variable but positive benefit. Several studies evaluated the effect of marrow stimulation in a medialized, single-row repair with this technique, demonstrating a very high healing rate in primary RCR. 9,10,28,31 Furthermore, 1 study showed a statistically significantly lower retear rate with single row with microfracture versus single row and double row without microfracture. 31 Thus, marrow stimulation techniques may be considered as a relatively straightforward method to increase healing, reduce retear, and improve long-term functional outcomes.
All studies included in our systematic review employed a small joint arthroscopic awl. Perforations smaller and deeper into the marrow portend better marrow access. A thin and sharp awl has been shown to produce a statistically higher percentage marrow access than a beveled tip awl. 15 Using an analogous clinical scenario of cartilage repair, increased depth of subchondral penetration improves marrow access, outcomes of cartilage repair, and subchondral bone. 34 Advances have been made as well as to avoid compromising suture anchor fixation. 9,10,37 The local presence of marrow elements including growth factors and cytokines combined with autologous mesenchymal stem cells likely provides a favorable milieu for tendon healing. An additional advantage to this technique is the ability for marrow elements to elute after the conclusion of the case without dilution by arthroscopic fluid.
The current literature exploring the benefit of vented anchors has shown limited clinical benefit relative to their nonvented counterparts, despite a theoretical mechanism that is similar to that of marrow stimulation. Although preclinical studies demonstrated promise, the 4 clinical papers included in this study demonstrated that vented anchors provided no clear benefit over nonvented anchors in either functional outcomes or retear rate at both short-term and long-term follow-up. 4,11,19,32,33 Although 2 studies demonstrated that vented anchors improved ossification, bone mineral density, and bone mineral mass at the anchor site, this did not translate to any meaningful difference in clinically significant outcomes. 4,19 Overall, our meta-analysis demonstrated no difference in retear rate or Constant score between the vented anchor and control anchor groups. However, further evaluation is likely necessary, given the relatively low number of patients (N = 94) who were treated with vented anchors across the 3 included studies. 19,32,33
Given the comparative success of marrow stimulation techniques, the results of the vented anchor studies may suggest that current commercially available vented anchors may not achieve the marrow access necessary to induce the desired effects. Marrow access is influenced by the depth of perforation, the number of vents used in the repair, and the diameter of the anchor vent. Prior studies have demonstrated that holes with a depth of ≥4 mm are necessary to communicate with trabecular marrow cavities and that the depth of subchondral perforation influences cartilage repair outcomes. 6,15,35 However, commercially available anchors are typically 4.5 to 6.5 mm in length, suggesting that adequate depth should be achieved. 4,19 Furthermore, a close relationship has been demonstrated between the number of perforations and marrow elements eluted, with 1 study demonstrating that defects treated with 3 to 5 perforations resulted in elution of a substantially higher number of mesenchymal stem cells than defects treated with 1 perforation. 26,35 Given that the repairs in the cited studies utilized 1 to 3 anchors, use of vented anchors alone may result in a lower number of perforations versus marrow stimulation techniques, which utilize as many perforations as the exposed footprint will allow. 4,9,32,37 Finally, commercially available anchor vents may not have the optimal diameter for elution of marrow elements, as evidenced by a study that failed to demonstrate increased marrow element elution in vented anchors versus closed anchors. 4 Prior studies have established the ideal diameter of subchondral drill holes to be 1.0 mm, with larger 1.2-mm and 1.8-mm holes demonstrating reduced histological matrix staining, tissue repair quality, and subchondral bone reconstitution. 35
Despite promising results, it should be noted that the local, procedural marrow-derived augmentation techniques discussed may not be feasible in all primary cases. Osteoporosis has been demonstrated to be an independent risk factor for failure of arthroscopic RCR, potentially driven by the lower pullout strength in osteoporotic bone versus healthy bone. 7,29 Similarly, poor bone quality or small tear size may serve as barriers to implementation of microfracture techniques. In both cases, such procedures may compromise healing by weakening the bone and reducing stability at the anchor site, resulting in bone collapse or anchor loosening. 24,28
Limitations
As with all studies, there are limitations. First, only 3 comparative studies evaluating vented anchors in RCR were available for inclusion in the meta-analysis, resulting in a relatively small sample size. Of those, 1 level 3 study comprised 66% of included participants, with 80% of those patients classified as “control” patients (bioabsorbable and all-suture anchors). 32 All these patients underwent the single-row technique for repair. 32 This may create a risk of bias that could influence the overall observed effect. Additionally, there was considerable differences in repair techniques, marrow stimulation techniques (see Table 1), control anchor selection (see Table 2), and limitations on the concomitant procedures performed across the 13 included clinical studies. Heterogeneity in approach presents a double-edged sword, allowing for greater applicability of findings across patient populations, but also limiting one’s ability to draw definitive conclusions on the efficacy of specific techniques. Finally, patient comorbidities and other baseline characteristics were not specifically controlled for in this study, given the limited publication of such data in the included studies.
Nonetheless, the data from this systematic review and meta-analysis may prove valuable in terms of improving quality of care and prevention of retears. Given the onus of prevention of retear on the surgeon, surgeons must anticipate patients at risk of retear and work with payors to leverage technologies that improve healing and reduce retear rates in order to improve the value of care given. In the era of bundled payments, further consideration must be given to the relative cost-effectiveness of marrow augmentation techniques. Increased healing and reduced retear via marrow stimulation may result in cost savings through avoidance of revision repair or the development of chronic tears, despite an increased time-zero cost associated with implementation of a unique technology or technique. More research is needed in this specific area, as the available evidence for use of local, procedural marrow-derived augmentation techniques in RCR is relatively limited, with 9 clinical studies evaluating marrow stimulation techniques and 4 clinical studies evaluating vented anchors. Future direction includes larger trials with both radiographic and clinical follow-up for the evaluation of lasting treatment effects, cost-effectiveness analyses of newer marrow augmentation techniques and technologies, and clinical trials evaluating combined mechanisms of augmentation.
Conclusion
Recent advances in marrow stimulation promote the biologic milieu and demonstrate favorable outcomes and limited adverse effects in both preclinical and clinical settings. Current evidence demonstrates that microfracture and marrow-venting techniques may have a positive impact on healing and retear rate, while vented anchors have a muted impact relative to nonvented anchors. Although the available evidence is limited and more research is needed, findings to date suggest that marrow stimulation techniques may be an inexpensive, simple technique to consider in qualifying patients to prevent rotator cuff retears.
Footnotes
Notes
Final revision submitted September 30, 2022; accepted October 21, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.F. has received honoraria from DJO. K.M. has received consulting fees from Vericel. G.R. has received consulting fees from Arthrex, Stryker, and Tornier and speaking fees from Arthrex and Stryker. S.S.S. has received consulting fees from Exactech. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.