
Abstract
Background:
A frequent cause of exercise-induced leg pain in young individuals is chronic exertional compartment syndrome (CECS). The dominant role of a diagnostic intracompartmental pressure (ICP) measurement (ICPM) according to the Pedowitz criteria (PDWc) is criticized. The relation between number of positive PDWc and outcome after surgery for different types of lower leg CECS is unknown.
Purpose/Hypothesis:
The aim of this study was to determine whether number of positive PDWc is associated with three different outcome parameters in patients who were operated for different types of lower leg CECS. It was hypothesized that the number of positive PDWc is related to outcomes 3 and 12 months after fasciotomy for CECS.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Patients with a history and physical examination consistent with CECS of the anterior (ant-CECS) or deep posterior compartment (dp-CECS) completed a questionnaire scoring symptoms prior to an ICPM. Three PDWc were used (ICP ≥15 mmHg before the treadmill test; and ICP ≥30 mmHg and ≥20 mmHg 1 and 5 minutes after the test, respectively). Patients were grouped according to number of positive PDWc (0/1, 2, 3), and CECS type (ant-CECS, dp-CECS). In these 6 groups, outcomes—defined as symptom scores, return to sports, and operation satisfaction—were measured 3 and 12 months after a fasciotomy. Mann-Whitney U, Kruskal-Wallis, and Fisher-Freeman-Halton tests were used.
Results:
Between February 2013 and January 2025, 182 patients (313 legs; 37% male; age, 25 years [IQR, 19-36], excluding the lateral-CECS group with 5 patients) fulfilled study criteria. Group ant-CECS PDWc 0/1, PDWc 2 and PDWc 3 contained 7, 33, and 93 patients, respectively. Group dp-CECS PDWc 0/1, PDWc 2, and PDWc 3 had 10, 14, and 25 patients, respectively. Five PDWc groups demonstrated a significant drop (P < .01) in symptom scores at 3 and 12 months, but not the ant-CECS PDWc 0/1 group (P = .18; P = .37). This latter group also demonstrated lower return-to-sports rate (50%; P = .04) compared with PDWc 2 and PDWc 3 (74% and 86%, respectively). Operation satisfaction was not associated with number of positive PDWc in either ant-CECS or dp-CECS patients. dp-CECS patients tended to be more satisfied than ant-CECS patients (at 3 months 63% vs 47%; P = .07).
Conclusion:
Our study demonstrated that there is no uniform association between number of positive PDWc and outcome in patients who were operated for either ant-CECS or dp-CECS. This study can assist in future research in order to contribute to our understanding and to optimize decision making in patients with CECS who are considering fasciotomy.
Keywords
A frequent cause of exercise-induced lower leg pain in young individuals is chronic exertional compartment syndrome (CECS). 3 The exact mechanisms underlying this syndrome are poorly understood. It is generally thought that a rise in muscle compartment pressure plays a role in the pathogenesis. 15 CECS typically occurs in anterior and deep posterior compartments (ant-CECS, dp-CECS) although the lateral compartment may also be affected (lat-CECS). 25 Commonly reported symptoms are pain and tightness during and after running.
A dynamic intracompartmental pressure (ICP) measurement (ICPM) is advised as an objective tool confirming the diagnosis. 5 Most sports physicians managing CECS rely on ICP criteria proposed by Pedowitz (PDWc). 14 In 1990, they reported that a ≥15-mmHg rest ICP and/or an ICP ≥30 mmHg 1 minute after completing a standard treadmill test and/or an ICP ≥20 mmHg 5 minutes later reflected CECS. At present, sensitivity and specificity of these diagnostic PDWc are challenged.8,13,16 Moreover, whether a set of PDWc predicts success after treatment is largely unclear. One retrospective study suggested an association between number of positive PDWc and outcome following a fasciotomy for ant-CECS. 13
The aim of this study using prospective data is to determine whether the number of positive PDWc is associated with 3 different outcome parameters in patients who were operated for different types of lower leg CECS. We hypothesized that patients with more positive PDWc would have better outcomes after fasciotomy.
Methods
General Study Information
The study was conducted at Máxima Medical Center (MMC), Veldhoven, the Netherlands. This hospital harbors a national center of expertise for leg exertional pain syndromes. Patients are referred from hospitals across the country. Study procedures complied with the 1964 Declaration of Helsinki and its amendments. The independent medical ethical review board at MMC concluded that the rules laid down in the Medical Research Involving Human Subjects Act did not apply to this study.
Diagnostic Procedures for CECS and Study Criteria
Patients ≥16 years with possible CECS who were scheduled for an ICPM between February 2013 and January 2025 in MMC were eligible for the study. Prior to a physical appointment at the outpatient sports medicine department, each patient completed a standard questionnaire containing a range of queries on previous medical history and symptoms related to lower leg discomfort. If CECS appeared to be a possibility, patients were evaluated by 1 of 3 sports physicians. A physical examination was then performed to assess the likelihood of CECS of the lower leg compartments. If anterior compartment palpation provoked symptoms, and other syndromes were ruled out, the patient underwent an ICPM in a manner previously described. 20
As per protocol, ICPM values were obtained during rest, then immediately, 1 minute, and 5 minutes after a provocative treadmill test. If rest values were already increased or 1-minute values were high, the provocative treadmill test was aborted or pressure measurements were prematurely terminated in some patients, arbitrarily decided by the attending sports physician. In these patients, additional ICP values were therefore not obtained but were by default considered elevated (positive PDWc). Similarly, if resting and 1-minute values were low, the measurement protocol was in some cases prematurely ended assuming that the 5-minute value remained low (negative PDWc).
The sports physician evaluated patient history, physical examination, and ICPM results to determine whether CECS was present. The patient was counseled regarding treatment options. If unresponsive for at least 12 weeks to prior nonoperative treatment, the patient was briefly informed on surgical options. Mostly within a month patients were counseled by a surgeon on the specifics of a fasciotomy of the affected compartments. 25 After oral and written consent, some weeks later surgery was performed as previously reported.19,25 Patients were excluded if they continued nonoperative treatment or if they underwent a surgical procedure including multiple-leg compartment fasciotomy. Also excluded were patients who did not complete the 3-month follow-up questionnaire or who did not undergo an ICPM.
Study Groups Based on CECS Type and Number of Positive PDWc
At first, patients were grouped according to number of positive PDWc (≥15 mmHg during rest and/or ≥30 mmHg and/or ≥20 mmHg at 1 and 5 minutes after treadmill testing, respectively). By doing so, 3 groups were constructed (PDWc 0/1, PDWc 2, and PDWc 3). Patients were randomly combined with 0 or 1 positive PDWc into a single group, as both categories contained a limited number of patients. Moreover, the diagnosis CECS in some patients having 0 or 1 positive PDWc may have been predominantly based on patient history and physical examination rather than on an ICPM. 21 PDWc 2 contained 2 positive criteria, and PDWc 3 contained 3.
Next, patients were grouped according to type of operated lower leg compartment (ant-CECS, dp-CECS, or lat-CECS). As the number of lat-CECS patients was too low, they were excluded from analysis, leaving a total of 6 groups.
Questionnaires Before and After Fasciotomy
A standard baseline questionnaire for each patient evaluated for exercise-induced lower leg pain was introduced across 17 Dutch medical institutes around 2013. 21 It covered general patient information, previous treatments, severity and frequency of symptoms, and influence on daily activities and sports. Five essential lower leg symptoms (pain, tightness, muscle weakness, cramps, and tingling/numb feeling) were scored. Intensity of symptoms was rated as none (1 point), mild (2 points), moderate (3 points), severe (4 points), or extremely severe (5 points). Frequency of symptoms was rated as never (1 point), sometimes (2 points), half of the time (3 points), most of the time (4 points), or always (5 points). For each symptom, a score was calculated by multiplying intensity with frequency (range, 1-25 points). A total symptom score was calculated as the sum of all 5 symptom scores (range, 5-125 points). Scores were obtained at rest and during exertion. The overall symptom score was the sum of total scores at rest and during exertion (range, 10-250).
Three and 12 months after fasciotomy, patients were asked to complete follow-up questionnaires on residual symptoms using the previously described score, their return to sport timeline, and their operation satisfaction. Return to sports was classified as “Yes, at the level before complaints”; “Yes, although at a lower level than before complaints”; “Yes, but another type of sport”; or “No.” Operation satisfaction was classified as “excellent,”“good,”“fair,”“poor,” or “bad.”
Study Outcomes
The primary study outcome was the association between the number of positive PDWc and outcomes 3 months after the fasciotomy. Three different parameters reflecting outcome were studied: decrease in symptoms, return to sports, and operation satisfaction. Baseline and 3-month symptom scores were compared on a linear scale. Return to sports was scored dichotomously as possible return to sports of any type with answer yes or no. Operation satisfaction was analyzed dichotomously as good or excellent versus fair, bad, or poor. Outcome parameters were studied in the 3 different populations (ant-CECS, dp-CECS, and lat-CECS).
Secondary study outcomes assessed at 12 months were PDWc group differences regarding symptom scores, return to sports, and operation satisfaction.
Statistical Analysis
Data were analyzed using SPSS statistics software for Windows (Version 29; IBM Corp). Data were checked for normality using kurtosis (between −1.0 and 1.0), skewness (between −1.0 and 1.0), and Shapiro-Wilk test. As data were not normally distributed, they were depicted as median (IQR) (25th-75th percentile). Mann-Whitney U tests and Kruskal-Wallis tests were used to compare continuous data between groups. An alpha of .05 was considered significant. A Bonferroni correction was applied for multiple comparisons. Differences between data at baseline versus 3 or 12 months were significant at P = .025, and for cardinal symptoms at P = .005. The chi-square test was used to compare nominal data between groups. For small sample sizes in nominal data, the Fisher-Freeman-Halton test was used for the 2 × 3 distribution using the most conservative P value. 10
Results
Selection and Group Characteristics
Figure 1 depicts the flow chart for the 1539 patients with lower leg pain who filled out a baseline questionnaire. As 1352 patients did not meet study inclusion criteria for reasons depicted in Figure 1, a total of N = 187 patients (312 legs) were studied and included in this analysis. The lateral compartment group did not qualify for analysis as the group size was too small (n = 5; 8 legs). Baseline characteristics of ant-CECS and dp-CECS patients are shown in Table 1.
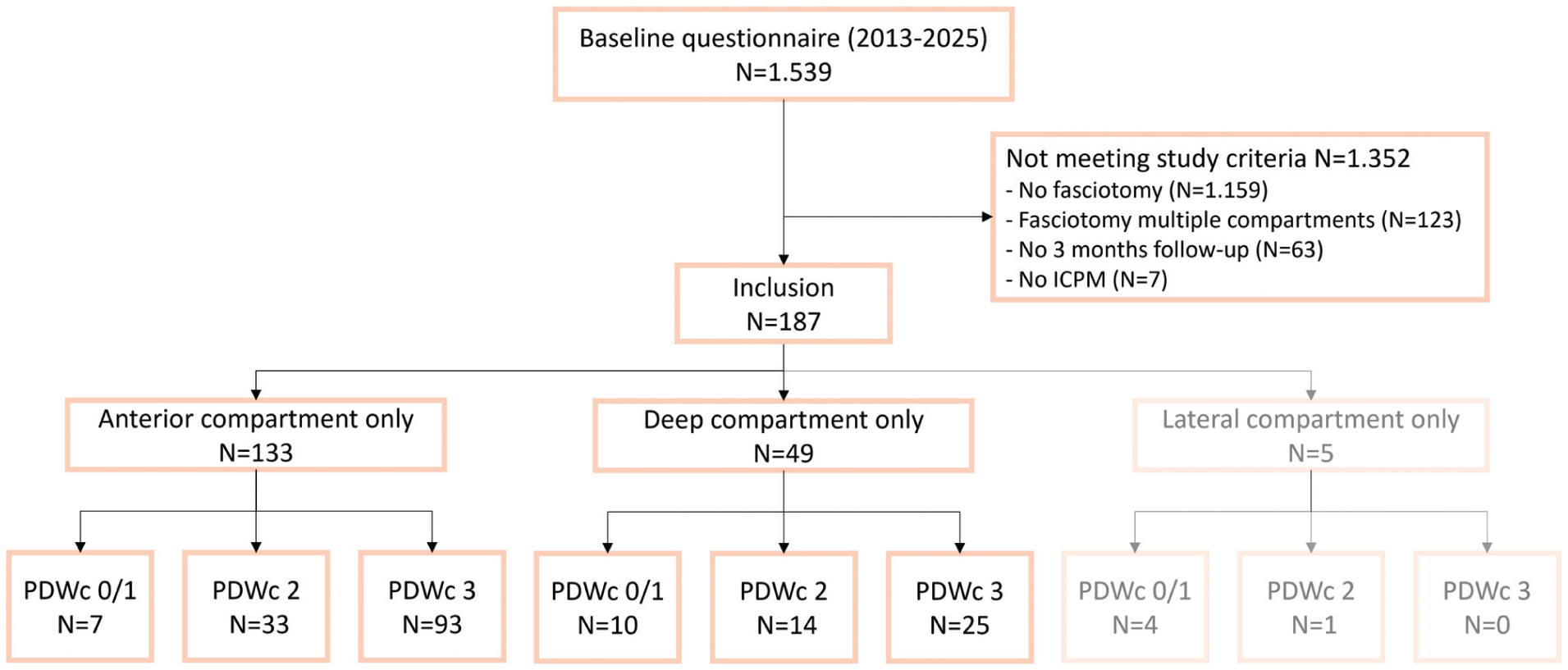
Study flowchart. The lateral compartment group values are grayed out, as the small size of this subcohort disqualified it from analysis. ICPM, intracompartmental pressure measurement; PDWc 0/1–3, number of positive Pedowitz criteria.
Characteristics of Patients Undergoing Fasciotomy for ant-CECS or dp-CECS and Number of Positive PDWc a

Data are reported as median (IQR) unless otherwise indicated. Bold P value indicates significant difference <0.05. BMI, body mass index; ant-CECS, anterior chronic exertional compartment syndrome; dp-CECS, deep posterior chronic exertional compartment syndrome; PDWc, Pedowitz criteria.
Symptoms at Follow-up
Figure 2A illustrates total symptom scores at baseline and 3 and 12 months after a fasciotomy for ant-CECS. Compared with baseline (130 [IQR, 78-145]), scores were unaltered in group PDWc 0/1 at 3 months (51 [IQR, 38-149]; P = .18) and 12 months (115 [IQR, 45-149]; P = .37). In contrast, patients in group PDWc 2 (baseline, 91 [IQR, 67-110]) and PDWc 3 (baseline, 90 [IQR, 70-116]) demonstrated significantly reduced symptom scores at both 3 months (PDWc 2, 42 [IQR, 20-65] and PDWc 3, 32 [IQR, 22-57]) and 12 months (PDWc 2, 42 [IQR, 32-56] and PDWc 3, 39 [IQR, 23-66]) compared with baseline (P < .01). Between each time point separately, there were significant differences only between PDWc 0/1 and PDWc 3 at 12 months (P = .02).
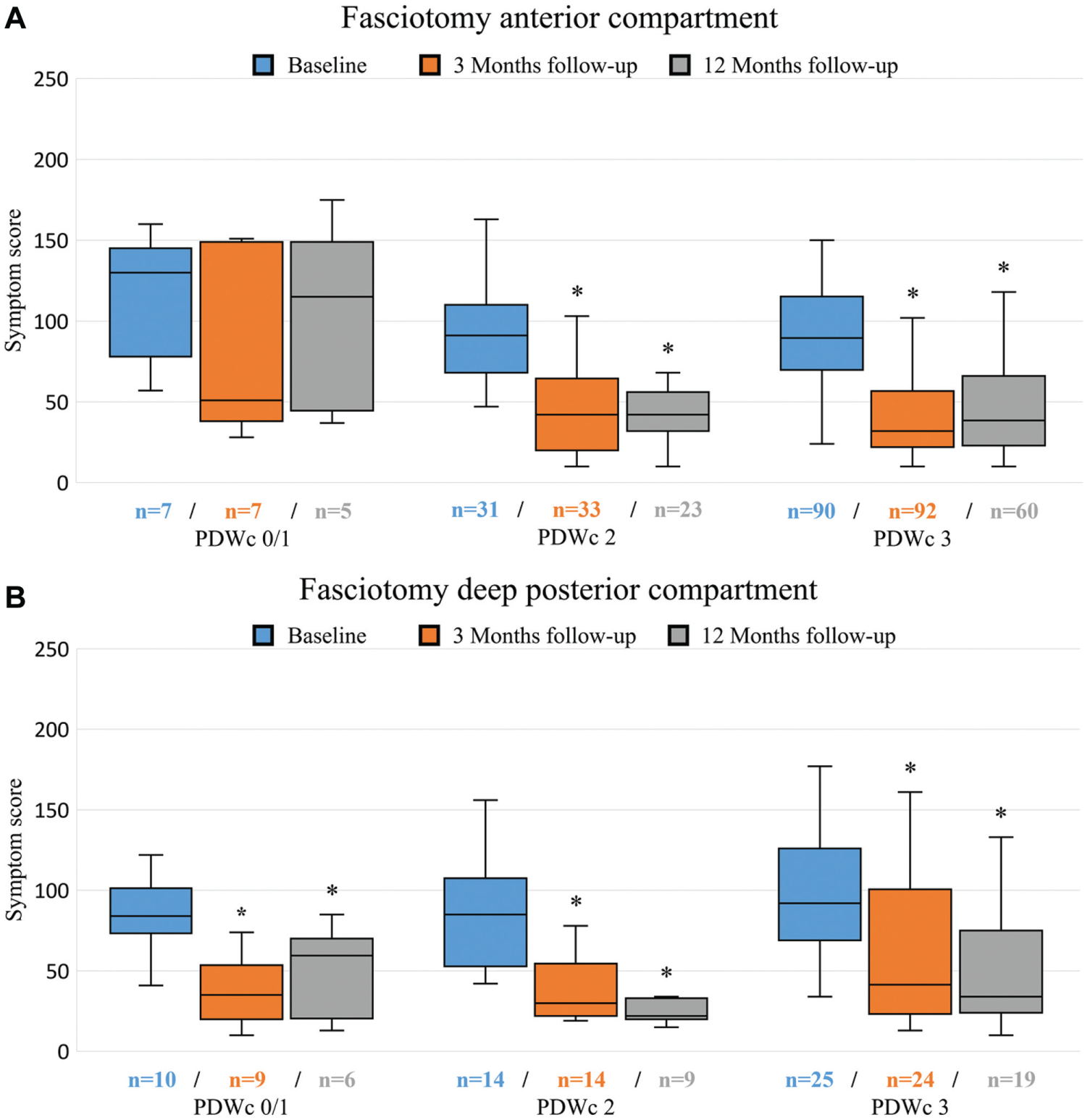
Symptom scores (range, 10-250) reflecting exercise-induced lower leg discomfort after a fasciotomy for (A) anterior or (B) deep posterior compartment syndrome. Data are shown as boxplot (median, q25-q75, minimum and maximum) with outliers (>3 times Z score) excluded from image (data not excluded from analysis). Asterisk indicates significance at P < .05 compared with baseline. PDWc 0/1-3, number of positive Pedowitz criteria.
Figure 2B depicts changes in symptom scores over time in patients after fasciotomy for dp-CECS. The drop in symptoms was significant (P < .02) at both postoperative time points compared with preoperatively in all 3 PDWc groups. For each time point separately, there were no significant differences between PDWc.
Return to Sports
At 3 months, a significant (P = .04) positive association was present between number of PDWc and successful return to sports in patients who underwent a fasciotomy for ant-CECS (Table 2) but not in patients with dp-CECS (P = .73) (Table 2). Rate of return to sports was lower in ant-CECS compared with dp-CECS in the PDWc 0/1 group (50% vs 70%; P = .61) but not in PDWc 2 and PDWc 3.
Return to Sports and Operation Satisfaction in CECS Patients in Relation to Number of Positive PDWc a
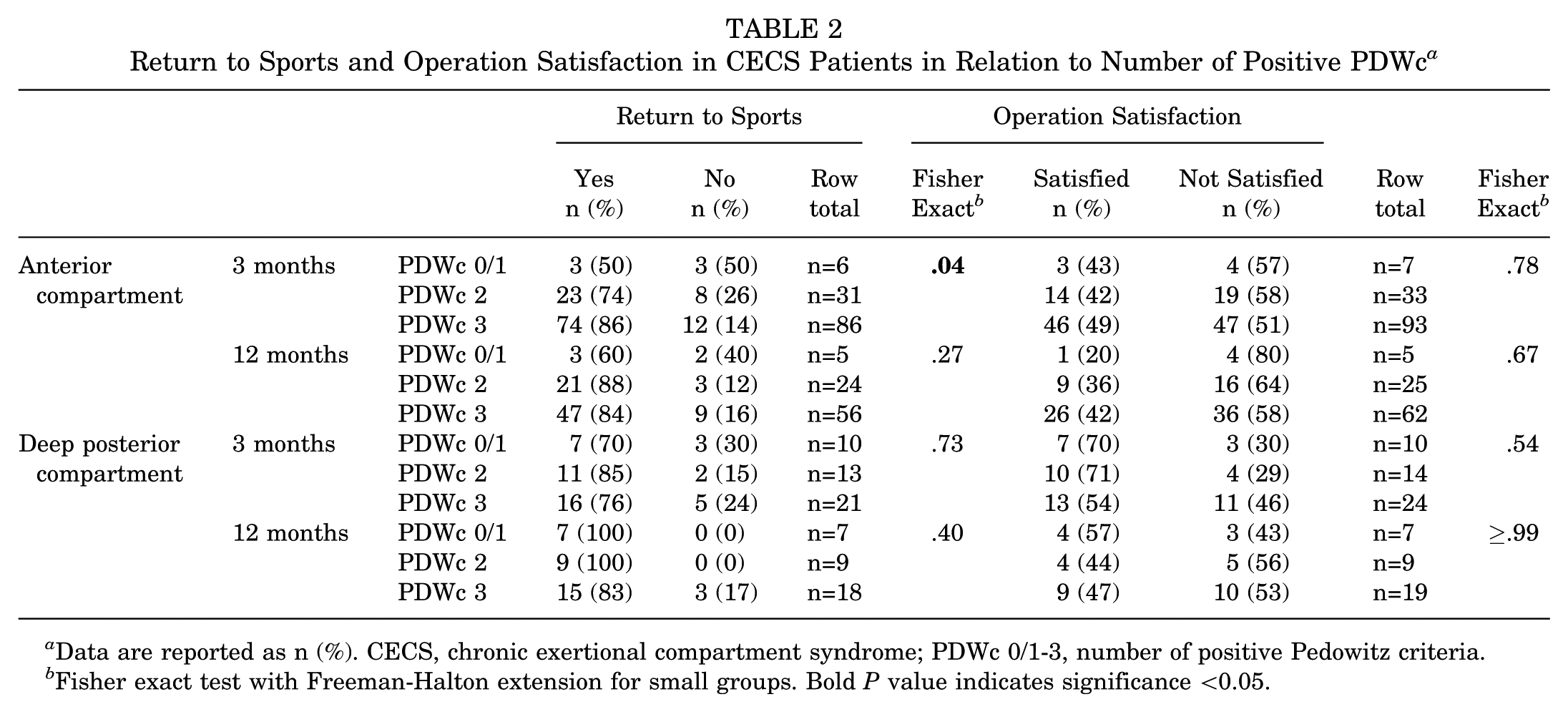
Data are reported as n (%). CECS, chronic exertional compartment syndrome; PDWc 0/1-3, number of positive Pedowitz criteria.
Fisher exact test with Freeman-Halton extension for small groups. Bold P value indicates significance <0.05.
At 12 months, there was no significant association between PDWc and return to sports in ant-CECS or dp-CECS. Again, rates of return to sports in ant-CECS having PDWc 0/1 (60%) were lower than all other categories (all >80%).
Operation Satisfaction
Operation satisfaction was not related to PDW category or type of CECS at the 3- and 12-month time points. At 3 months, satisfaction rates in patients who received a fasciotomy for ant-CECS were lower (all PDWc ≤50%) compared with the dp-CECS group (all PDWc >50%; P = .07). At 12 months, the satisfaction rate was lowest for the ant-CECS PDWc 0/1 group (17%). In all other groups, satisfaction rates ranged from 38% to 75%.
Discussion
A dynamic ICPM using PDWc is advised as an objective tool confirming the diagnosis of lower leg CECS. 5 Since the introduction of the ICPM, its test characteristics have been criticized, as predictive properties regarding treatment outcome are not univocal. 16 One retrospective study found a positive association between number of positive PDWc and outcome following a fasciotomy for ant-CECS. 13 The aim of this study was to determine with prospective data whether the number of positive PDWc were associated with 3 different outcome parameters in patients undergoing surgery for ant-CECS or dp-CECS. In general, outcomes largely depended on the type of CECS. When considering ant-CECS, patients with 0 or 1 positive PDWc did not show significant symptom relief after a fasciotomy. Additionally, the rate of return to sports was lower with a trend of less satisfaction compared with the 2 or 3 PDWc group. In contrast, outcomes in dp-CECS patients were better compared with ant-CECS and were not related to the number of positive PDWc. These results should be discussed during counseling of patients who consider surgery.
The present study is the first prospective effort investigating a potential association between number of positive PDWc and outcome after fasciotomy for CECS. Interviews by Verleisdonk et al 22 2 years after a fasciotomy in patients having symptoms suggestive of ant-CECS found that 66% with normal pressures (PDWc 0) reported success compared with 83% with elevated pressures (PDWc 1, 2, and 3). A retrospective study by Pasic et al 13 used questionnaires and interviews and found that the PDWc 3 group had an 85% success rate compared with a 67% success rate in the PDWc 0/1 and 2. The present study is unique in that data were collected prospectively, we investigated 2 types of lower leg CECS, and considered 3 different outcome parameters, which limited selection bias and recall bias. An important finding, confirming results of the aforementioned studies,13,22 is that ant-CECS patients having 0 or 1 PDWc are less likely to benefit from a fasciotomy.
Measuring outcome after a fasciotomy for CECS is not standardized. The most frequently used tools are questionnaires investigating return to daily activity or sport to reflect daily functioning.7,12,13,17 These questionnaires represent a somewhat objective measure, though it is still subject to changes in daily functioning not related to CECS. Alternatively, treatment satisfaction may be determined by interviews. 12 Answers are likely influenced by expectations and recall bias, as a baseline measurement is absent. Additionally, changes in symptom intensity and frequency may be quantified, either via elaborate scoring systems or through visual analog scale or Numeric Rating Scale scores.18,21 These techniques include a baseline measurement that prevents recall bias. However, changes in pain perception might influence these results. Finally, outcome may be evaluated using performance measures such as a standardized treadmill test, but this approach is costly and time-consuming. 21 A recent Delphi analysis on CECS suggested that an overall outcome scoring system should include a measure of return to previous levels of sport and activity along with a global perceived effect. 23 It may well be that development of such a system is hampered by the lack of consensus on the diagnosis of CECS itself. As different lower leg CECS types exist, often in combination with other exercise-induced lower leg pain syndromes, consensus on an outcome scoring system is even more crucial.
Intuitively, one might expect to find an association between number of positive PDWc, the burden of the disease, and treatment outcome. The absent association can be explained in different ways. First, a discrepancy illustrates the limitations of the set of PDWc as a tool reflecting treatment outcome. 13 Zimmermann et al 26 also reported that absolute values of ICP in the anterior compartment were not associated with treatment outcome. Second, it must be acknowledged that exercise-induced pain and discomfort are subjective characteristics that may not be captured in objective tissue pressures. An earlier study demonstrated that patient satisfaction is determined by expectations. 24 Third, in the previously mentioned Delphi analysis, criteria other than that of Pedowitz should have a role in the assessment of treatment outcome. 23 The overall conclusion supported by previous literature and our study is that the PDWc are of limited use regarding treatment outcome of CECS.
The decision to counsel a patient for fasciotomy is largely guided by the clinical judgment of the treating sports physician. This approach is partially due to the limitations of ICP measurements and the rigidity of the Pedowitz cutoff values. 1 There are a number of issues limiting the credibility of an ICPM. For instance, patient positioning is crucial. It is suggested that an ICPM obtained from a standing patient rather than a lying patient allows for a proper distinction between CECS and non-CECS. 16 These uncertainties were already addressed in the original article of Pedowitz et al 14 and have resulted in various modifications of ICPM protocols. Other studies also consider an ICPM of limited value and stress the importance of a thorough history and clinical examination.2,6,26 In the present study, 18% of the excluded patients had ≥1 positive PDWc. However, based on an unconvincing history and physical examination, they were considered by their treating sports physician to not have CECS. As a consequence, surgery was not offered. In daily practice, therefore, a large group of patients suffering from lower leg pain having 1 or 2 positive PDWc are excluded from surgery because the diagnosis is unsure, possibly leading to undertreatment.
Recent studies have identified ≥3 clinically different types of lower leg CECS. 4 Nowadays, whether a patient has ant-CECS, dp-CECS, or lat-CECS (often combined) is diagnosed by a single ICPM system with fixed cutoff criteria. One study suggested that normal rest and postexercise pressures of the anterior compartment are higher compared with values of the deep posterior compartment and lateral compartment. 9 Modification of cutoff values may therefore allow for diagnosing type of CECS. Ogunlusi et al 11 studied 49 healthy participants and found that the upper threshold for rest compartment pressures is about 4 mmHg higher in the anterior compartment compared with the deep compartment. The present study found an 18-mmHg median (range, 15-23) resting value in ant-CECS patients compared with a 15-mmHg median (range, 12-19) rest value in dp-CECS patients, which is in conformity with previous studies. Future studies on outcome should take into account the type of lower leg CECS.
Limitations
The present study has limitations, including an expected limited number of patients in the PDWc 0/1 group, as well as an 18% exclusion rate and outcomes based on patient reports. Being a center of expertise, the number of complex cases is likely higher compared with a standard hospital possibly influencing outcome. The percentage of refasciotomies was not considered in the analysis. Cases with unilateral or bilateral symptoms were not analyzed separately. The decision was made to study only patients reporting symptoms in a single compartment. In practice, 30% of patients reported CECS in multiple compartments. 4 Future multicenter studies may focus on different noninvasive techniques including static versus dynamic measurements or different patient positioning.
Conclusion
Our study demonstrated that there is no uniform association between number of positive PDWc and outcome in patients who were operated for either ant-CECS or dp-CECS. This research can assist in future studies to contribute to our understanding and to optimize decision-making in patients with CECS that are considering fasciotomy.
Footnotes
Final revision submitted October 14, 2025; accepted October 15, 2025.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not required for this study.