
Abstract
Background:
Chronic exertional compartment syndrome (CECS) causes exercise-induced leg pain. The diagnosis is confirmed by intramuscular pressure (IMP) measurements. Fasciotomy has been demonstrated to be a successful treatment for CECS; however, few studies have examined postoperative IMP and long-term outcomes.
Purpose:
To evaluate long-term outcomes and postoperative IMP in patients surgically treated for anterior CECS, and to identify possible preoperative or postoperative factors associated with overall satisfaction with treatment at follow-up.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
A consecutive series of 209 patients who underwent fasciotomy of the anterior compartment for CECS between 2009 and 2019 and had at least 1 year of follow-up were approached for inclusion. A total of 144 patients (69%), with a follow-up time of 1 to 11.5 years, were ultimately included. All patients underwent preoperative and postoperative 1-minute postexercise IMP measurements of the anterior compartment and completed a questionnaire covering pain and activity parameters at both time points. The follow-up questionnaire included an additional question on overall satisfaction with treatment, and surgical details were collected from the patient’s medical records.
Results:
The median IMP was significantly lower at follow-up than at baseline (17 mm Hg [range, 5-91 mm Hg] vs 49 mm Hg [range, 25-130 mm Hg]; P < .001). The overall satisfaction rate was 77%, and 83% reported a decreased pain level. The group of patients who were satisfied with the treatment included more men and had a higher ΔIMP and a lower revision rate (P < .05). Among the 16 patients (11%) who had undergone revision fasciotomies before follow-up, the satisfaction rate was 56%, and 64% reported a decrease in pain level.
Conclusion:
Fasciotomy significantly reduced 1-minute postexercise IMP in patients with CECS and resulted in satisfaction and decreased pain in more than three-quarters of the patients at long-term follow-up. The male sex and a significant decrease in IMP were both positively associated with treatment satisfaction. Patients who underwent revision surgery before the follow-up had lower satisfaction rates and less pain reduction than the overall group.
Keywords
Lower leg chronic exertional compartment syndrome (CECS) presents as activity-related pain and is mainly diagnosed by elevated intramuscular pressure (IMP) elicited by activity. Patients are usually asymptomatic during rest and there are few pathological findings at physical examination, so clinicians can easily miss the diagnosis. 22 Therefore, the majority of patients have a history of long-standing symptoms before receiving a CECS diagnosis. 31 Athletes are over-represented in cohorts of patients with CECS; runners are the most common among participants in individual sports, and soccer players are the most common among participants in team sports. 3 CECS can affect all 4 muscle compartments of the lower leg, but isolated CECS of the anterior compartment is the most common engagement. 2,3,15
Although the exact mechanism of CECS is unknown, it is generally accepted that the condition is characterized by pathologically elevated IMP during and immediately after exercise, which is related to a relatively stiff musculofascial compartment. In addition to an elevated postexercise IMP—preferably assessed via a 1-minute postexercise measurement—the patient’s history and a clinical examination are important to confirm the diagnosis. 1,11
Treatment options of CECS can be divided into nonoperative and operative management. Adjustment of activities, with an overall decrease or omission of the most provocative exercises, has been shown to reduce the symptoms. However, most patients with CECS are unwilling to give up their preferred sporting activities. In a few studies, modifications of the overall running technique and of the foot-strike pattern, in particular, have been suggested to play a role in the nonoperative management of CECS. 4,8,9 These 3 studies were all case series of military personnel, and the suggested intervention programs have not, to our knowledge, been evaluated in athletes with CECS. Intramuscular injections of botulinum toxin A (Botox) have been suggested to decrease IMP and reduce pain in limited case series of patients with CECS. 12,13 However, patients treated with Botox injections often experience muscle weakness, which is an unacceptable adverse effect.
Fasciotomy of the affected compartments is the gold standard surgical treatment for CECS and is usually successful. 5,16 A recent systematic review reported that fasciotomy resulted in an 85% patient satisfaction rate and an 80% rate of return to activity. 35 However, in a study on military personnel who had undergone fasciotomy of the anterior, lateral, and/or posterior compartments, 45% of the patients reported symptom recurrence, 28% were unable to return to full activity, and 16% were suffering from surgical complications. 36
Most studies evaluating the results after fasciotomy are of retrospective design and comprise relatively small cohorts, and the parameters evaluated vary among them. 6,17,23,30,35 Further, many fasciotomy evaluation studies lack objective outcome measures and long-term outcomes. IMP measurements have been considered to be a useful objective measure for evaluation of the surgical outcome. 5 Since there are anatomical differences between the 4 compartments of the lower leg, and the median postexercise IMP values are known to vary between the compartments, 15 the IMP values in the different compartments should be evaluated separately. However, few studies have focused solely on 1 specific compartment when comparing preoperative and postoperative IMP values; moreover, in previous studies of anterior compartment postoperative IMP, the majority of the patients were men. 26,32,34
In the present study, we assessed the long-term outcomes of a large cohort of patients with CECS who underwent anterior fasciotomy using postoperative IMP measurements and patient-reported outcome measures, including satisfaction with treatment results, level of pain, and physical activity level. In addition, we aimed to identify possible preoperative or postoperative factors affecting satisfaction with treatment results at long-term follow-up.
Methods
Patients
Participants comprised 209 consecutive patients who underwent primary fasciotomy of the anterior compartment for anterior CECS between May 2009 and December 2019 at the Department of Orthopedics at Sahlgrenska University Hospital, Gothenburg, Sweden. The diagnosis of CECS was obtained before surgery based on the patient’s history, a clinical examination, and the invasive measurement of IMP after an exercise test. 14 In patients with bilateral symptoms, the clinically affected compartments were measured in the most symptomatic leg to minimize the number of invasive measurements. The IMP criteria used for the CECS diagnosis were IMP ≥30 mm Hg at 1 minute postexercise and/or IMP ≥20 mm Hg at 5 minutes postexercise. 24 At the preoperative visit, all patients filled out a questionnaire, including pain and activity parameters. The study protocol received ethics committee approval, and all patients provided their written informed consent.
All 209 patients treated during the study inclusion time were sent information about the study and an invitation to a follow-up appointment occurring at least 1 year after the primary fasciotomy of the anterior compartment. The follow-up visit included measurement of IMP of the anterior compartment after an exercise test. The patients also filled out the same questionnaire they had completed before surgery, with the addition of a question regarding satisfaction with treatment results. Information on preoperative IMP, surgical details, and eventual postoperative complications or revision surgeries was collected from the patients’ medical records.
Questionnaires
The questionnaire used at the preoperative appointment and follow-up included questions regarding the patients’ characteristics (eg, sex, age, height, and weight), duration of symptoms in months, level of leg pain during activity, and physical activity level. Response options for the question about physical activity level were as follows: no activity; recreational; club sports; and elite.
The standardized questionnaires used for all visiting patients suspected to have CECS at the present clinic were slightly changed during the study period. The purpose of the change was to improve patient care, but it also affected the pain grading in this study. Patients whose preoperative visit was before January 2018 were asked to rate their leg pain during activity on a categorical scale comprising no pain, mild pain, moderate pain, severe pain, and worst possible pain, while patients whose preoperative visit was in 2018 or later were asked to grade their pain on a numeric rating scale (NRS), ranging from 0 (no pain) to 10 (worst possible pain). At the follow-up, all patients received the same form that they had filled out preoperatively. The majority of the patients used the categorical scale, and only those patients who had answered the questions using this scale were included in between-group analyses.
The postoperative questionnaire included an additional question about satisfaction ("How satisfied are you with the treatment results after surgery?"), with the following response options: very satisfied; satisfied; uncertain; and dissatisfied. This method of assessing patient satisfaction after surgery has been used in earlier studies. 20,23 In the analyses, treatment satisfaction was dichotomized into satisfied (very satisfied or satisfied) versus not satisfied (uncertain or dissatisfied).
To examine whether follow-up time affected postoperative physical activity level, the patients were divided into 3 groups depending on follow-up time (<3 years, 3-6 years, or >6 years).
Exercise Test
Both preoperatively and at follow-up, the exercise test included running on a treadmill, followed by repeated dorsiflexion of the ankle and then heel raise in a standing position. The test was terminated when pain or fatigue hindered the patient from continuing to perform the present activity. At the follow-up appointment, the treadmill run and the dorsiflexion of the ankle were each terminated after 10 minutes if the patient did not experience pain or fatigue.
Preoperative and Postoperative IMP Measurements
The technique used for IMP measurements of the anterior compartment was the same preoperatively and at follow-up. However, the IMP was measured in all symptomatic compartments preoperatively but only in 1 leg. At the follow-up, IMP measurements were made in the anterior compartment only, but in both legs if the patient had undergone bilateral surgery—only the matched measurements are reported here. One-minute postexercise IMP values were obtained for all patients both preoperatively and postoperatively.
The IMP measurements were made using a microcapillary infusion system (Hemo 4; Siemens) connected to a monitor (SC9000; Siemens) according to a previously published protocol. 14,15 An 18-gauge (1.2 × 50–mm) IMP needle with 4 side holes at its tip was connected to a transducer line (150 cm) filled with saline, which was linked to the pressure recording system. In the cases where the IMP was measured in the anterior compartment in both legs, 2 IMP needles were connected to the pressure recording system. The system was calibrated before and after each measurement. As described in previous studies, the patient was in a supine position with extended legs, positioning pads (ESWELL; Simonsen & Well) were placed under the patient’s heels and knees, the skin was first penetrated using a separate needle, a bulging of the fluid at the tip of the IMP needle was maintained, and the tip of the IMP needle was placed at heart level. 14,15
Surgery
All surgical procedures were performed at the unit specialized in exercise-induced leg pain by 1 of 3 orthopaedic surgeons (J.S, K.R, and S.L.) with several years of experience in diagnosing and treating patients with CECS. Procedures on patients with bilateral symptoms were performed either concomitantly or in stages. The anterior compartment fasciotomies were performed using a traditional open technique. First, a tourniquet was applied on the thigh, and a longitudinal skin incision of approximately 7 cm was placed 3 cm lateral of the tibial crest over the midportion of the lower leg. After blunt dissection in the proximal and distal direction, the fascia was split by long Metzenbaum scissors. If the lateral compartment was included in addition to the anterior compartment fasciotomy, the incision was placed over the septum between the anterior and the lateral compartment. Fasciotomies of the posterior compartments were performed through a separate longitudinal incision placed 3 cm medial of the medial tibia border. Resorbable sutures were used for suturing the skin.
The postoperative regimen included 2 hours of immediate leg elevation, the use of crutches for 24 hours, and compression bandaging for 48 hours. The patients were instructed to continue with normal movements of daily life after surgery, beginning with short walks after 1 week, and then gradually increasing the walking distance. They were allowed to return to sporting activities after a wound check at our clinic 3 weeks postoperatively.
Statistical Analysis
A Shapiro-Wilk test was performed and showed non-normal distributions of IMP values. Therefore, a nonparametric test was used, and the medians and ranges were used to summarize variables. Descriptive statistics are presented as medians and ranges for continuous variables and as numbers and percentages for categorical variables. Differences between the 2 independent groups were analyzed with the Mann-Whitney U test, and matched pairs (preoperative data vs postoperative data) were compared with the nonparametric Wilcoxon signed rank test. The nonparametric Kruskal-Wallis test was used to evaluate the association between IMP and pain level during activity. Categorical variables were analyzed with a chi-square test or a Fisher exact test. For all tests, P < .05 was considered statistically significant. Analyses were performed using SPSS Version 26 (IBM Corp).
Results
Patient Characteristics
A total of 144 patients of the initially identified 209 were examined at follow-up with postoperative IMP measurements taken of the anterior compartment in the same leg that was measured preoperatively. Full details of participant inclusion are given in Figure 1.

A flow chart with details of participant inclusion. CECS, chronic exertional compartment syndrome; IMP, intramuscular pressure.
The primary anterior fasciotomy was performed bilaterally and concomitantly in 69 patients (48%), bilaterally and in stages in 54 patients (38%), and unilaterally in 21 patients (15%). The median follow-up time was 3.4 years (1-11.5 years)—56 patients (39%) were observed <3 years postoperatively, 57 patients (40%) were observed 3 to 6 years postoperatively, and 31 patients (22%) were observed >6 years postoperatively.
Table 1 presents baseline patient characteristics for patients included in the present study and those who were lost to follow-up or were excluded. Similar proportions of men and women were found in the study group of 144 patients, and the median age was 26 years (range, 13-82 years). For most parameters, no differences were observed between the study group and the patients lost to follow-up; however, there were significant differences in physical activity level. The excluded group included a higher percentage of physically active patients, and the study group included a larger proportion of elite athletes.
Baseline Characteristics of the Patients Included at Follow-up and Those Excluded or Lost to Follow-up (N = 209) a

a Data are presented as percentage or median (range). The bold P value indicates a statistically significant difference between groups (P < .05). BMI, body mass index; IMP, intramuscular pressure.
There were 128 patients (89%) who had undergone anterior fasciotomy only 1 time (primary surgery group) and 16 (11%) who had undergone a primary fasciotomy and a revision fasciotomy of the anterior compartment before the follow-up (revision surgery group). The most common indications for surgical revision were persistent or recurrent symptoms together with an IMP above the cutoff value (n = 12), or painful fascia defects (n = 2). There were no significant differences in patient characteristics between the patients in the primary surgery group and those in the revision surgery group (Table 2). However, there were slightly more women in the revision surgery group than in the primary surgery group (63% vs 47%).
Baseline Characteristics of Patients in the Primary Surgery and Revision Surgery Groups (N = 144) a
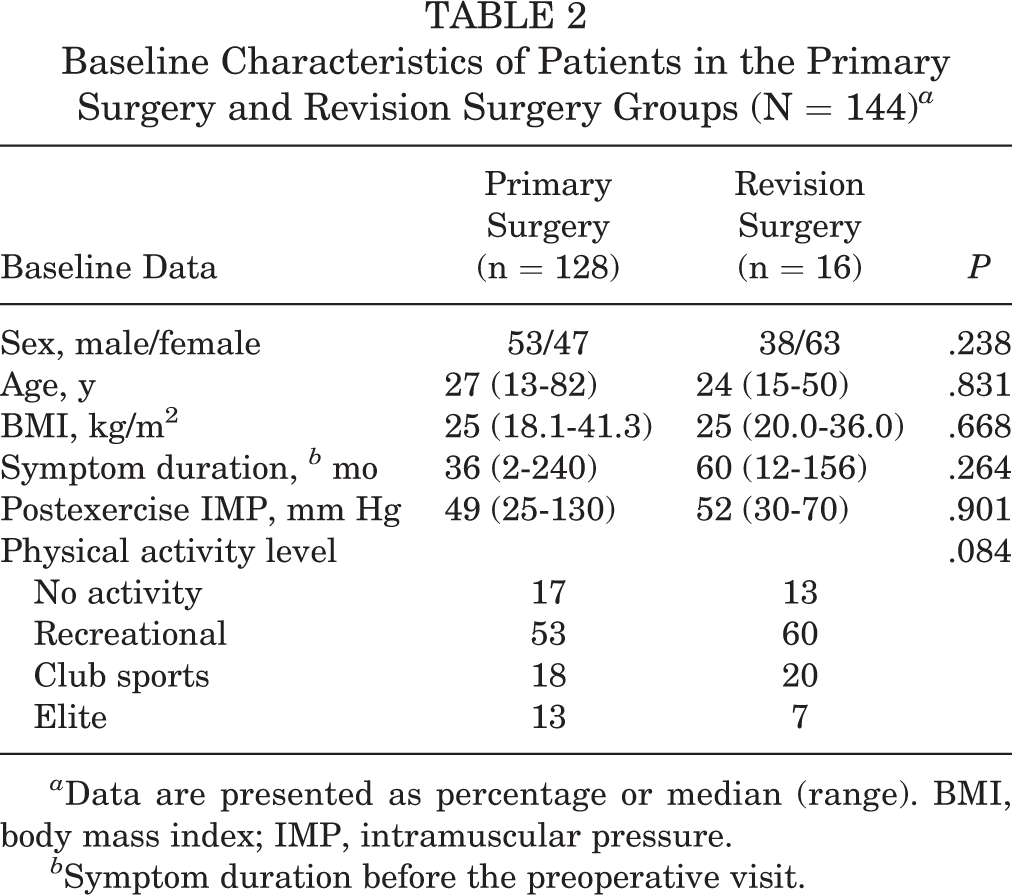
a Data are presented as percentage or median (range). BMI, body mass index; IMP, intramuscular pressure.
b Symptom duration before the preoperative visit.
The primary surgery was an isolated anterior compartment fasciotomy in 104 patients (72%), anterolateral fasciotomy in 25 patients (17%), anterolateral and posterior fasciotomy in 11 patients (7%), and anterior and posterior fasciotomy in 4 patients (3%). Table 3 shows a comparison of outcomes between patients who underwent isolated anterior fasciotomy and those who underwent fasciotomies of additional compartments. Patients in whom the primary surgery included fasciotomies of additional compartments had significantly higher preoperative IMP and ΔIMP in the anterior compartment (P = .004 and P = .020, respectively); however, no differences were found between the groups for other outcome measures.
Comparison of Outcomes Between Patients After Isolated Anterior Fasciotomy vs Fasciotomies of Additional Compartments a
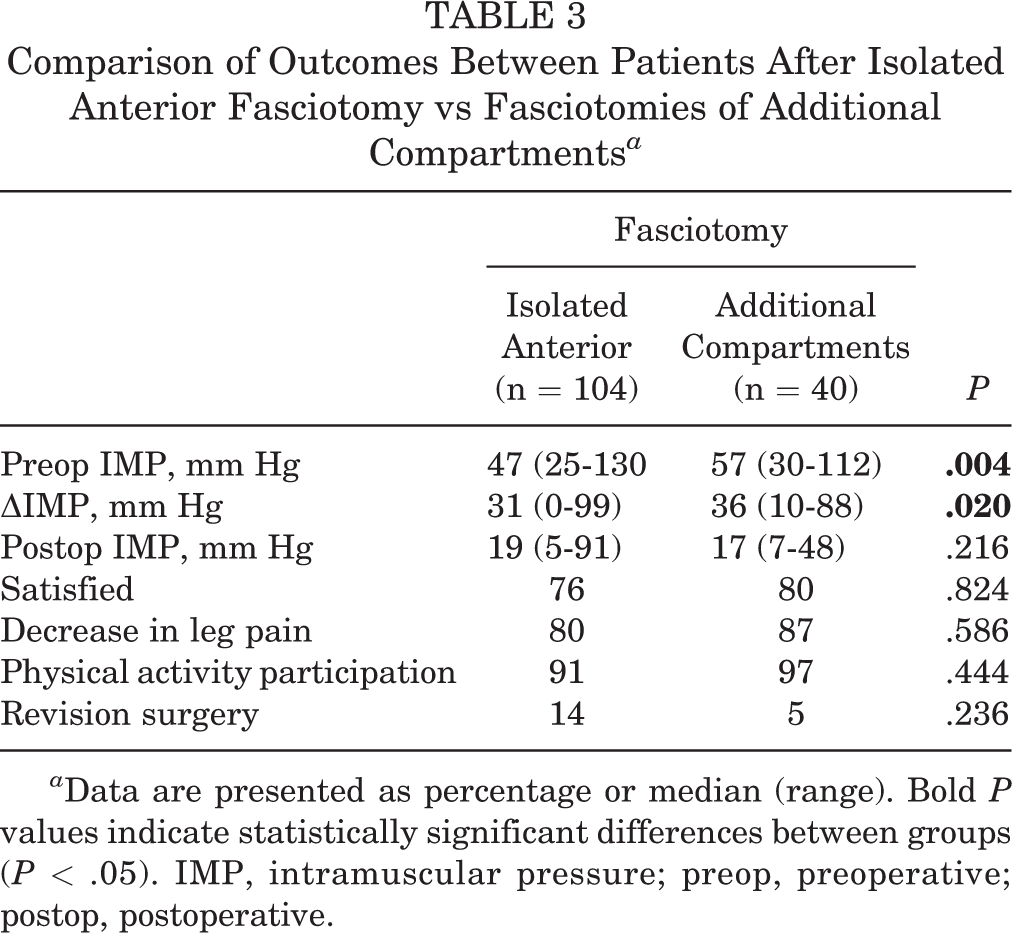
a Data are presented as percentage or median (range). Bold P values indicate statistically significant differences between groups (P < .05). IMP, intramuscular pressure; preop, preoperative; postop, postoperative.
Intramuscular Pressure
At follow-up after fasciotomy, 143 of the 144 patients had a lower 1-minute postexercise IMP in the anterior compartment compared with their preoperative measurements, and 1 patient had no change in IMP (30 mm Hg). For the study group overall, the median 1-minute postexercise IMP was 17 mm Hg (range, 5-91 mm Hg) at follow-up, which was significantly lower than the preoperative median 1-minute postexercise IMP of 49 mm Hg (25-130 mm Hg) (P < .001). The primary surgery group had similar median IMP values to the revision surgery group; however, the IMP showed less variability in the revision group, both preoperatively and at follow-up (Table 4).
Comparison of Preoperative and Follow-up 1-Minute Postexercise IMP Measurements Overall and by Surgery Group a

a Data are presented as median (range). Bold P values indicate statistically significant differences between groups (P < .05). IMP, intramuscular pressure.
b Paired data.
The distributions of the 1-minute postexercise IMP values preoperatively and at follow-up after fasciotomy of the anterior compartment for the total study group and the subgroups are presented in Figure 2. Eleven patients (7.6%) in the primary surgery group had a 1-minute postexercise IMP >30 mm Hg at follow-up.

Distribution of the 1-minute postexercise IMP values preoperatively and at follow-up after fasciotomy of the anterior compartment for (A) the total study group (N = 144), (B) the primary surgery group (n = 128), and (C) the revision surgery group (n = 16). Note the different scales on the y-axis. IMP, intramuscular pressure.
Patient Satisfaction
Overall, 111 patients (77%) were very satisfied or satisfied with their treatment results. When considering the subgroups separately, the rates of those describing themselves as very satisfied or satisfied were 80% in the primary surgery group and 56% in the revision surgery group (Figure 3).
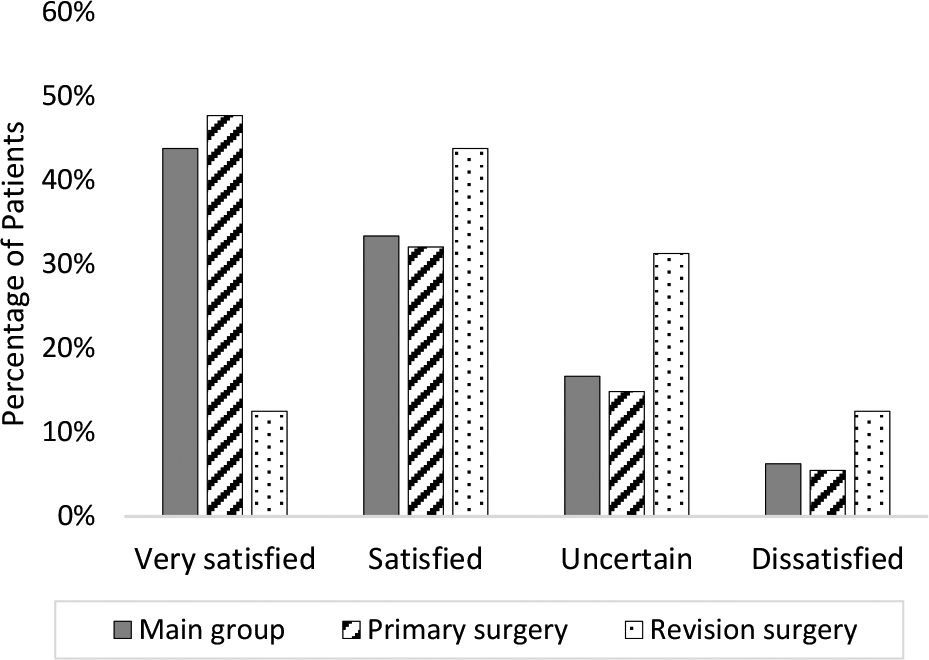
Satisfaction with the treatment results in patients at follow-up after fasciotomy of the anterior compartment for the total study group (N = 144) and the subgroups: the primary surgery group (n = 128) and the revision surgery group (n = 16).

Satisfaction with the treatment results in patients at follow-up after fasciotomy of the anterior compartment in relation to the surgical procedure (unilateral, bilateral performed in stages, or bilateral performed concomitantly) for the primary surgery group (n = 128).
Patient satisfaction with treatment was not significantly affected by the extent or the way the fasciotomy of the anterior compartments was performed (unilateral, bilateral performed in stages, or bilateral performed concomitantly) (Figure 4). Table 5 presents a comparison of patient characteristics, symptom duration, preoperative IMP, IMP at follow-up, change in IMP between preoperative and postoperative values (ΔIMP), pain level, physical activity level, follow-up time, and revision rate between the patients who were satisfied (ie, responded with very satisfied and satisfied) with the treatment result and the group of patients who were not satisfied (ie, responded with uncertain and dissatisfied). Compared with their dissatisfied counterparts, the satisfied group included a higher proportion of men (P = .049), a lower proportion of patients who underwent revision surgery (P = .035), and a significantly higher ΔIMP (P = .016). In addition, the satisfied group had a significantly lower level of leg pain at follow-up compared with patients who were not satisfied (P < .001).
Comparison of Baseline and Follow-up Variables Between Patients Who Were Satisfied vs Not Satisfied With Treatment Results a

a Data are presented as median (range) unless otherwise indicated. Bold P values indicate statistically significant differences between groups (P < .05). BMI, body mass index; IMP, intramuscular pressure.
b n = 97 satisfied; 29 not satisfied.
c n = 99 satisfied; 29 not satisfied.
d n = 99 satisfied; 27 not satisfied.
e n = 100 satisfied; 28 not satisfied.
f n = 110 satisfied; 33 not satisfied.
Level of Leg Pain
A total of 95 patients graded their level of pain during activity both preoperatively and at follow-up using the 5-step categorical scale. All groups showed a significant reduction in this measure between preoperative and follow-up values, with 83% of the patients in the total study group (P < .001), 86% in the primary surgery group (P < .001), and 64% in the revision surgery group (P =.018) reporting a decrease of at least 1 step on the scale. The NRS was used by 22 patients in the total study group to grade their level of pain during activity preoperatively and at follow-up. The median NRS score decreased significantly (P < .001) from 8 preoperatively to 5 at follow-up, and 77% of these patients reported a reduction in leg pain during exercise at follow-up compared with their preoperative self-assessment.
No association was observed between preoperative IMP and preoperative level of pain during activity; moreover, no association was found between IMP at follow-up and the level of pain at follow-up.
Physical Activity Level
Among the 127 patients who graded their level of activity preoperatively and at follow-up, 94% of the patients reported physical activity of some sort at follow-up. At follow-up, the physical activity levels had increased in 16% of the patients, remained at the same level in 61% of the patients, and decreased in 23% of the patients.
The postoperative change in physical activity level differed significantly between the 3 groups divided by follow-up time (<3 years, 3-6 years, and >6 years). Among the patients with a follow-up time of <3 years, 10% had a decreased activity level at follow-up, in contrast to 52% among the patients with a follow-up time of >6 years.
Discussion
To our knowledge, this study has the largest participant groups used to investigate long-term results after fasciotomy of the anterior compartment, as well as a sex, activity, and age distribution that is in line with current everyday clinical practice. With a follow-up time of up to 11.5 years, the results show that anterior fasciotomy results in a significant reduction in median postexercise IMP, a significant reduction in leg pain during activity in 4 of 5 patients, and an almost universal (94% of patients) ability to perform some form of physical activity at the time of follow-up. However, 23% of the patients reported a decreased level of activity at follow-up. Overall, the patients had a satisfaction rate of approximately 80%; however, the satisfaction rate among the patients who had undergone a revision fasciotomy of the anterior compartment before follow-up was markedly less, at only 56%. Male sex, a large difference between preoperative and postoperative IMP value, a lower revision rate, and none or mild leg pain during exercise at follow-up were all associated with satisfaction with treatment.
Multiple studies have presented good results and relief of symptoms after fasciotomy in patients with CECS. 21,23,28 However, comparisons between studies are challenging because of differences both in the methods used to evaluate the result after fasciotomy and in the compartments investigated. Some studies evaluate solely parameters extracted from medical records, others use self-administered questionnaires, and yet others report data from face-to-face interviews. 25,28,36 Patient-reported outcomes used in previous studies include questions about satisfaction with treatment, pain scales, and activity scores. 10,17,20,23,29,30
There is a lack of long-term follow-up studies, including baseline data on patients surgically treated for CECS. In the present study, preoperative data on symptom duration, pain, and activity level were collected for 144 patients who had undergone fasciotomy for anterior CECS. These patients included similar proportions of men and women, which reflects the sex ratio seen in CECS cohorts today. The study design could be considered as retrospective; however, we used prospectively collected preoperative data in combination with prospectively collected follow-up data. The follow-up time ranged from 1 to 11.5 years, which is comparable to some of the previous studies investigating treatment results for patients with CECS. 18,21,27,28 However, these previous studies all had a completely retrospective design regarding baseline data, thus introducing recall bias to the results.
IMP has been suggested to be the most useful objective measure to assess the outcome after fasciotomy. 5 However, postoperative IMP measurement is rare in routine clinical practice, and very few studies have investigated the existence or size of the change in IMP after fasciotomy. Furthermore, since median postexercise IMP values are known to vary between the different compartments in the lower leg, studying the treatment results of each compartment separately is of high importance. 15
In the present study, the finding that fasciotomy significantly lowers the IMP confirms that fasciotomy of the anterior CECS is effective in reducing muscle compartment pressures. This finding is in line with earlier studies of the anterior compartment; however, previous studies on postoperative IMP exclusively in the anterior compartment included few patients, and 80% to 100% of the patients were men. 26,32,34 Somewhat unexpectedly, the present study showed a large variation in postoperative IMP values. Although most patients had an IMP <30 mm Hg, a small proportion of patients had relatively high IMP values postoperatively. These, however, were too few to analyze as a subgroup. The subgroup of patients who underwent repeated fasciotomy of the anterior compartment showed less variability in IMP values, both preoperatively and at follow-up. The reason for this can only be speculated on, but perhaps some of the patients had another coexisting problem that was not properly addressed. Another reason might be that different people experience pain at different IMP levels, which is supported here by the finding that the level of pain could not be linked to the IMP.
No differences were observed in satisfaction, pain decrease, or return to activities between patients undergoing fasciotomy for solely the anterior compartment and those who underwent fasciotomy for 1 or several additional compartments. However, the preoperative IMP and the ΔIMP in the anterior compartment were significantly higher in patients who had undergone fasciotomy of the anterior compartment combined with fasciotomies of the lateral or posterior compartments. These results could speculatively be caused by several reasons—the effect of increased IMP in the anterior compartment may increase the IMP in nearby compartments; and multiple compartment disease indicates a more severe form of CECS. However, the exact reason for this cannot be elucidated in the present study.
The overall satisfaction rate (77%) obtained in the present study falls within the range of earlier studies, which found patient-reported satisfaction rates 10,21,23,27 of 76% to 81%. However, these earlier studies included patients with varied combinations of compartments treated with fasciotomy for CECS; thus, the results might not be comparable. In the present study, the satisfaction rate was higher in the primary surgery group than in the revision surgery group, despite similar patient characteristics in each group. The exact cause for this is unknown; however, it falls in line with other conditions where repeated surgery often does not match up to the result of primary surgery. 7
A study of 73 patients found a higher satisfaction rate after fasciotomy in patients aged <23 years, and it also found an increased failure rate in patients who had a combined anterior-lateral fasciotomy. 21 An earlier study of 62 patients reported improved outcomes after fasciotomy with partial fasciectomy in patients with a symptom duration of <12 months. 28 Another study conducted on 16 patients found that bilateral fasciotomies performed concomitantly resulted in early return to sports and low complication rates. 25 In the present study, including a cohort of 144 patients, no relationships were found between patient satisfaction and age, involvement of additional compartments, symptom duration, or type of surgical procedure (unilateral, staged bilateral, or concomitant bilateral).
Patient satisfaction seems to be somewhat associated with patient sex, as significantly more men than women were satisfied with their treatment results in the present study. This might be linked to the fact that the majority of women were in the revision surgery group. A previous study of young female athletes reported a lower success rate after fasciotomy compared with studies including both male and female patients, and the authors speculated that women might respond to fasciotomy less effectively than men. 19 The male sex was an independent predictor for a positive outcome in a study of 61 patients undergoing 2- or 4-compartment fasciotomies of the lower leg. 17
In the present study, we found that the ΔIMP was significantly higher in the group of patients who were satisfied with the treatment result. Since men at a group level have higher IMP preoperatively than women, this may be a reflection of the sex's effect on satisfaction. 14 We found no association between preoperative IMP and satisfaction with treatment results after fasciotomy, which is in line with an earlier study of the lateral compartment. 33 Further, we found no association between IMP at follow-up and satisfaction with treatment results.
The revision rate of 11% in the present study is in line with rates reported in earlier studies. 5,23 The most common reason for revision surgery of the anterior compartment in our participants was recurrent symptoms combined with IMP above the cutoff value. Despite the low median IMP values (16 mm Hg) after revision surgery, the revision group had a lower satisfaction rate and a considerably larger proportion of patients with remaining pain during activity than the primary surgery group. There are several possible reasons for this decreased satisfaction and remaining pain in the revision group, including the patients being wrongly diagnosed with CECS, the occurrence of additional lower leg diagnoses, or perioperative damage to surrounding structures. Clinicians must search for other causes of leg pain in patients who do not have symptom relief after fasciotomy. There is a need for further studies on patients who undergo revision surgery.
The decreased level of leg pain at follow-up in our study group is comparable with previous work on anterior fasciotomy. 34 Most of the patients in the primary surgery group (86%) reported a lower level of pain at follow-up, compared with a somewhat smaller proportion in the revision surgery group (64%). Preoperative level of pain was not related to patient satisfaction with the treatment result; however, treatment satisfaction was found to be associated with postoperative pain relief. There was also no association between preoperative IMP and preoperative level of pain during activity and no association between postoperative IMP and level of pain at follow-up. These findings are in line with a previous study that found no relationship between the percentage of pain relief and preoperative IMP. 10
At follow-up, almost a quarter of the patients had a lower physical activity level compared with preoperatively. This result is similar to that of previous studies focusing on anterior or anterior/lateral fasciotomies. 10,30 However, in the group of patients observed after <3 years, only 10% had a lower activity level postoperatively. The follow-up time of >6 years in 31 patients might have resulted in finding a decreased activity level due to age, lifestyle change, or other factors; it is entirely possible that these patients initially increased or maintained their physical activity level postoperatively, but that this was no longer the case by the time of follow-up. Physical activity level might be difficult to use as an outcome measure when the follow-up time varies from 1 to 11 years.
Strengths and Limitations
The main strength of the present study is the large cohort of patients treated with anterior fasciotomy for CECS who underwent preoperative and postoperative IMP measurements of the anterior compartment in the same leg. Other strengths are the equal sex distribution, the inclusion of patients with different activity levels, and the fact that all patients were investigated and surgically treated by a small number of orthopaedic surgeons at a clinic specializing in patients with exertional lower leg pain. Moreover, recall bias was unlikely to be present because the questionnaires on preoperative data were distributed preoperatively.
A limitation of the study is the use of different versions of the questionnaire during the study period. However, the only change in the questionnaire that might have affected the results was the scale used to answer the question regarding pain during activity. Although most patients (69%) were included in the study, the patients lost to follow-up may have restricted our ability to determine factors associated with outcome. Some of the loss to participate in the follow-up could have been due to patients’ concern over the pain and the risks involved with invasive IMP measurements. However, patient characteristics did not differ substantially between the patients who were included and those who were lost to follow-up or excluded from the study. Another possible limitation is that the preoperative IMP values were routinely measured only in the most symptomatic patients to minimize the risks of complications and discomfort for the patients.
Conclusion
This study indicates that anterior fasciotomy significantly decreases the 1-minute postexercise IMP in a wide range of patients with anterior CECS, results in a satisfaction rate of 77%, produces a reduction in pain level in 83% of patients, and allows most patients (94%) to participate in physical activity. For patients who had undergone an anterior revision fasciotomy before the follow-up, the satisfaction rate was only 56%. Overall, patient satisfaction seems to be associated with the male sex, a large difference between preoperative and postoperative IMP (ΔIMP), and not having undergone revision surgery.
Footnotes
Final revision submitted October 13, 2022; accepted November 9, 2022.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the regional ethics commission of Gothenburg (ref No. 589-18).