
Abstract
Background:
Certified athletic trainers (ATs) are the primary source of sideline coverage for high school athletic events, providing an essential role in student-athlete health. However, there is a paucity of literature evaluating the existence of state requirements regarding the presence of ATs and mandatory sideline medical coverage of high school athletic events.
Hypothesis:
It was hypothesized that there is significant variation among state policies on sideline medical coverage and AT requirements for high school athletic events.
Study Design:
Cross-sectional study
Methods:
A 17-question survey was emailed to the executive directors (or analogous position) of the state high school athletic associations for all 50 states and the District of Columbia. The survey was conducted to assess current state regulations regarding the provision of sideline medical coverage for high school athletic events and the employment of ATs in the United States from 2023 to 2024. We also sought to determine if any state based its requirement for sideline medical coverage on the perceived risk of injury. “Risk-independent” referred to a sideline medical coverage mandate irrespective of the perceived risk of injury, whereas “risk dependent” referred to coverage that was provided for those sports with a higher perceived relative risk of injury. We used descriptive statistics and compared states using odds ratios (ORs) and Fisher exact test.
Results:
Of the 51 high school athletic associations, 48 responded to the survey. Of the 48 responders, 11 (23%) had sideline coverage mandates: 3 states (6%) had risk-independent sideline coverage mandates, while 8 states (17%) had risk-dependent sideline coverage mandates. Of the 48 responding associations, 37 (77%) had no sideline coverage mandate. No state required the presence of an AT at high school athletic events. On average, states with more high schools were 95% less likely to have mandated sideline coverage than those with fewer high schools (OR, 0.05; 95% CI, 0.00094-0.54; P = .003). Overall, 92% of high schools in the United States are in states without a formal requirement for sideline medical coverage.
Conclusion:
This study highlights the widespread absence of state policies mandating sideline medical coverage or the presence of an AT for high school athletic events, which may contribute to disparities in the care and safety of student-athletes. These findings underscore the need for statewide policies to improve access to trained health care professionals, such as ATs, at sporting events, especially for high-risk sports such as football.
According to the National Federation of State High School Associations, >7.8 million students participated in high school sports during the 2022 to 2023 school year. 12 This substantial participation underscores the critical need for adequate athletic trainer (AT) coverage to ensure the health and safety of these student-athletes. Previous studies have revealed that 2 million injuries, 500,000 doctor visits, and 30,000 hospitalizations occur each year among high school athletes. 9 Despite so many students participating and incurring injuries in high school sports, only 66% of US secondary schools have certified ATs, available part-time or full-time, to provide medical services to their student-athletes. 7 This means that approximately 5.9 million high school students are participating in sports without access to an AT. 7
Perhaps the most important function of an AT is to provide sideline medical coverage for sporting events, including practice and games. This is critical because ATs at the high school level are often the first to respond to serious injuries such as fractures, dislocations, or concussions. 13 In emergencies such as cardiac arrest or heat stroke, their immediate intervention can be lifesaving, ensuring rapid assessment and stabilization until further medical help arrives. 3 ATs perform an essential role in injury recovery and prevention, and they act as liaisons between the student-athlete and the health care system. 2 The effect of ATs on orthopaedic injuries in high school athletes has been described in previous literature, highlighting their significant role in improving athlete safety and outcomes. In 2018, Pierpoint et al 13 showed that the overall injury rate in girls’ soccer was significantly higher in high schools without ATs (40.00 injuries per 10,000 athlete exposures) compared with high schools with ATs (23.07 injuries per 10,000 athlete exposures). For high school athletes suspected of having sustained a concussion, McGuine et al 11 found that student-athletes with high availability of ATs were 3.33 times more likely to have reported sustaining a sports-related concussion and more likely to have postconcussion evaluations than those with low availability of ATs.
Despite these data showing the positive effect ATs have on high school student-athletes, there remains a relative lack of ATs employed within high schools.7,14,15 This shortage is often attributed to funding constraints, limited awareness of their importance, and policy gaps that fail to mandate their presence in all secondary schools.15,16 This results in millions of student-athletes with little to no access to immediate medical care for their sports-related injuries. 7 Previous studies have evaluated the variety and extent of AT services within secondary schools and the effect of these services on student-athlete health.2,5,7,9,11,13 However, there is currently no federal mandate requiring such sideline medical coverage. Furthermore, little is known about the individual state requirements that exist for the presence of ATs, or other health care professionals, at high school athletic events. The purpose of this study was 3-fold: (1) to determine the existing state-specific requirements for the provision of sideline medical coverage at high school athletic events, (2) to determine the existing state-specific requirements for AT services within high schools, and (3) to analyze the regional variation in sideline medical coverage across the United States. We hypothesized that there is significant variation among state policies on sideline medical coverage and AT requirements for high school athletic events.
Methods
A survey-based study was conducted between November 2023 and July 2024 to define the number of states with mandates for sideline medical coverage during high school sporting events and to qualify the nature and extent of these mandates. In collaboration with the AOSSM, a 17-question electronic questionnaire was distributed to the executive director—or equivalent position, such as associate director—of each state high school athletic association across the United States (see Appendix). Contact information for each state director was obtained from publicly available sources.
The study included all 50 states and the District of Columbia. A follow-up email was sent to all state associations that did not respond within 3 weeks. For those that did not respond after 2 attempts, phone calls were made directly to the executive director or his or her designee. If the state association failed to respond after attempted emails and phone calls, the survey was forwarded to the corresponding state representatives of the National Athletic Trainers’ Association (NATA) via email (Figure 1).

Flow diagram depicting data collection process. NATA, National Athletic Trainers’ Association.
Primary Analysis
Two primary variables were collected via the survey: (1) general sideline medical coverage requirements and (2) mandatory AT employment within the states’ high schools.
Sideline Medical Coverage
The primary variable was the presence or absence of a state mandate for general sideline medical coverage during high school sporting events. For those states with a sideline coverage mandate, the state associations were asked if the mandate varied based on specific factors (eg, student enrollment, student sex, geographic region, athletic conference, and private vs public school). If a state mandate was based on the perceived relative risk of injury, it was defined as “risk-dependent.” If there was no distinction based on perceived risk of injury, it was defined as “risk-independent.” The state associations were also asked which health care providers could satisfy the mandate (eg, ATs, emergency medical technicians, physical therapists, physicians, etc).
AT Employment
The primary variable was the presence or absence of a state mandate that specifically required ATs to be employed at each high school. If such a mandate existed, the state associations were asked to specify the level of employment required to satisfy the mandate (eg, full-time employment vs event-specific coverage). Additionally, the state associations were questioned regarding any variation in mandatory AT employment between public and private high schools.
Statistical Analysis
All responses were treated as independent observations for analysis. Response options included binary choices (yes/no), open-ended questions, and “select all that apply” lists. The data were analyzed using descriptive statistical methods. We also compared the presence of sideline coverage mandates between states with a lower (<25th percentile) and a higher (>65th percentile) number of high schools by calculating odds ratios (ORs) with 95% CI and assessed statistical significance using Fisher exact test.
Results
The overall response rate from the high school athletic associations across all 50 states and the District of Columbia was 94% (48/51). Of the 48 responders, 44 (92%) were from athletic association staff, while the remaining (8%) were from state NATA presidents (Figure 2).

Flow diagram for respondents who participated in the sideline coverage survey. The total of 51 includes the District of Columbia (asterisk). NATA, National Athletic Trainers’ Association.
The median number of high schools governed by all of the athletic associations was 354 (IQR, 302.75). The number of high schools governed by an athletic association ranged from 56 (Delaware) to 4412 (New York). The athletic associations used specific methods to classify schools into divisions or classes.
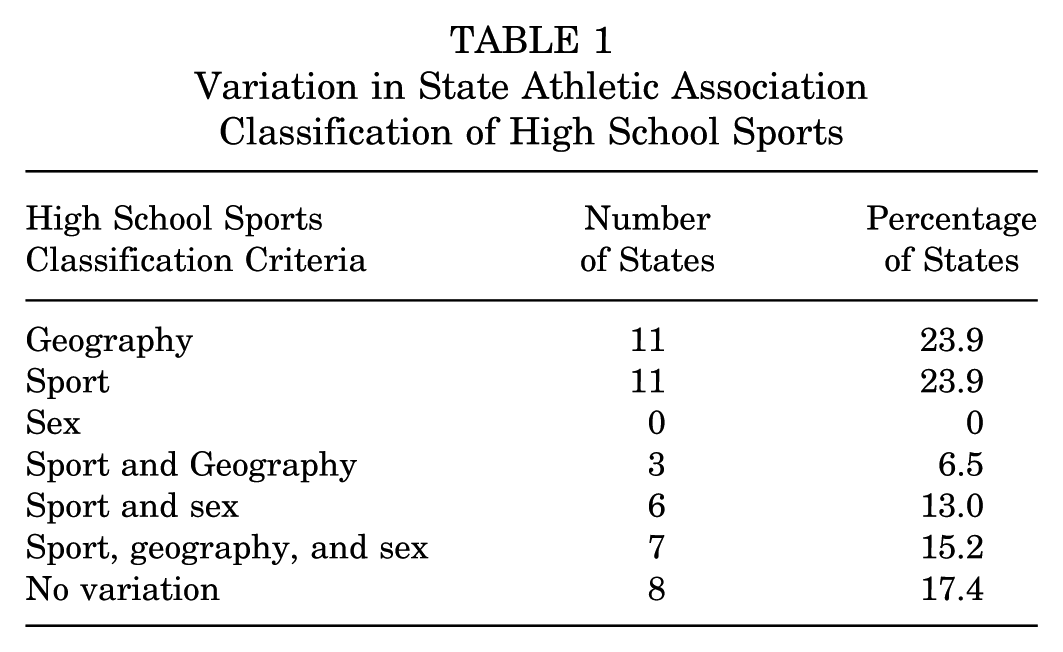
A total of 94% (44/47) of the athletic associations classified high school sports based on student population. The State of Rhode Island classified high school sports by the total number of sports, while New York State classified high school sports by total number of both students and sports. The nationwide variation in state athletic association classification of high school sports is shown in Table 1.
Variation in State Athletic Association Classification of High School Sports
Of all 48 responders, 11 (23%) reported the presence of a sideline coverage policy or mandate. Eight states (17%) had risk-dependent sideline coverage mandates, while 3 states (6%) had risk-independent sideline coverage mandates (Table 2).
Prevalence of Sideline Coverage and Athletic Trainer Employment State Mandates in the United States

Includes the 50 states and District of Columbia.
Includes full-time or part-time employment.
All 11 states with a sideline coverage mandate indicated that this requirement could be satisfied by an AT, emergency medical technician (EMT), paramedic, physical therapist, physician assistant, nurse practitioner, registered nurse, or physician. A total of 36 states and the District of Columbia (77%) had no sideline coverage mandate (Table 2). Additionally, no state required that high schools employ an AT in any capacity.
On average, states with more high schools (>65th percentile) were 95% less likely to have mandated sideline coverage than those with fewer high schools (<25th percentile) (OR, 0.05; 95% CI, 0.00094-0.54; P = .003). The mean number of high schools within states without mandated sideline coverage was 668. In contrast, the mean number of high schools within states with mandated risk-independent sideline coverage was 213, while states with mandated risk-dependent sideline coverage had a mean of 175 high schools.
The total number of high schools with no state mandates, risk-dependent mandates, and risk-independent mandates varied. The total number of high schools in states without mandated sideline coverage was 24,044. The total number of high schools in states with a risk-dependent sideline coverage mandate was 1398, while the total number of high schools in states with a risk-independent sideline coverage mandate was 640. Therefore, approximately 92% of high schools in the United States do not have mandatory sideline medical coverage for their athletic events.
Nationwide, there was regional variation in state sideline coverage mandates. Based on PearlDiver's regional map of the United States, the Midwest had no states with a sideline coverage mandate. The West, Northeast, and South did not demonstrate significant variation regarding the type of mandatory sideline medical coverage, including risk-independent and risk-dependent sideline coverage. The West region had 3 states with sideline coverage mandates (AZ, UT, HI), while the South (WV, NC, MS, DE) and Northeast (VT, NH, MA, RI) each had 4 states with sideline coverage mandates. The Northeast had the highest prevalence of risk-dependent sideline coverage mandates (n = 4) (Figure 3).

Map of the United States depicting the states with no sideline coverage mandates, risk-dependent sideline coverage mandates, and risk-independent sideline coverage mandates.
A total of 29 respondents answered the item assessing whether sideline medical coverage requirements differ between public and private schools (n=29). Among these respondents, three states (10%) established a difference in sideline medical coverage between public and private schools: New Hampshire, Utah, and North Carolina. In contrast, 25 states and the District of Columbia (90%) reported no difference in sideline medical coverage between public and private schools. Of note, 20 of the 29 respondents did not have a sideline coverage mandate.
Discussion
The major findings of our survey-based study revealed that 77% of states do not mandate any form of sideline medical coverage for high school athletic events. Consequently, approximately 92% of high schools in the United States have no requirement for sideline medical coverage of their athletic events. These findings align with previous literature on the current state of AT services within the country. In their 2019 study, Huggins et al 7 demonstrated that one-third of secondary schools have no access to an AT. Similarly, Pryor et al 17 found that 30% of public secondary schools did not have AT services and Pike et al 14 found that 42% of private secondary schools lacked AT services.
The effect of inadequate sideline coverage and lack of AT mandates extends beyond the field of play. ATs are commonly the first medical point of contact for high school athletes, and they serve as liaisons between student-athletes, parents, and the rest of the medical community. 2 Their presence provides many downstream effects beyond merely triage and immediate first aid of injured athletes. Preparticipation physical exams, referral to medical specialists, rehabilitation before and after surgery, clearance to return to sport, injury prevention, and patient education are all within the purview of ATs.5,13
Our study underscores how the absence of state policies may be a factor in the lack of AT coverage in secondary schools. It should be noted that the absence of a formal policy within a state does not necessarily mean that high schools within that state do not have some degree of sideline medical coverage. However, the absence of a formal mandate makes sideline coverage dependent on school-specific factors including financial resources, geographic location, socioeconomic status, available medical personnel willing to provide such coverage, perceived risk of injury, perceived malpractice risk, and sports played, among others.
Of the states with mandated sideline coverage, the requirement could be fulfilled by a variety of trained health care providers such as ATs, EMTs, paramedics, physical therapists, physician assistants, nurse practitioners, registered nurses, or physicians. In some communities, a physician-parent of a high school athlete may volunteer to provide sideline medical coverage for their sons’ or daughters’ games. While this would appear to be an ideal solution for those schools with no other coverage options available, a physician-parent’s medical expertise may not be applicable to sports-related traumatic or medical conditions experienced by high school athletes. In addition, a physician-parent may not be able to provide completely unbiased medical objectivity in terms of return-to-play decisions or the provision of emergency medical care.
In our study, no states required high schools to employ an AT in any capacity. Interestingly, we found that states with more high schools within their athletic association were less likely to have mandatory sideline medical coverage. These findings have a direct implication for the timely reporting and management of sports-related injuries for a significant number of high school student-athletes, which may, in part, be attributable to the absence of consistent state policies. Furthermore, our study found that 90% (n = 29) of the responders reported no policy differences between public and private school sideline coverage. These findings differ from existing literature, showing differences in sideline coverage presence between public and private schools.8,15 In the State of Illinois, a greater number of ATs were present on the sideline of private high schools than public high schools. 8 In a nationwide analysis, Pike et al 15 demonstrated that a higher percentage of public secondary schools had ATs who provided sideline coverage. Therefore, both public and private school coverage is likely more dependent on individual school resources than state policy.
As discussed previously, the absence of an AT or other health care professional providing sideline medical coverage of an athletic event can increase the risk of injury and delay the correct diagnosis and management of injuries in high school student-athletes.6,11,13 The consequences of not having access to an AT can be life-threatening, especially with medical emergencies or second-impact syndrome. 6 This has been recognized by numerous medical associations that have advocated for change. The American Medical Association and American Academy of Family Physicians (AAFP) have stated that ATs should be part of a high school's medical team.4,15 Furthermore, the AAFP recommends high schools employ a board-certified or registered/licensed AT as an integral part of the high school athletic program. 4 Despite the evidence in support of AT presence at high school athletic events, there continues to be no federal mandate for high schools to employ an AT or require a health care professional of any kind to provide medical sideline coverage.
The involvement of state legislators may offer a solution to ensure sideline coverage at high school athletic events. However, a recent study demonstrated that legislators have a limited knowledge of the AT profession, often confusing ATs with strength coaches and personal trainers. 16 In addition, only 68% of legislators recognized ATs as health care professionals. 16 These findings illustrate the need for further education of legislators and the general public on the important responsibilities that ATs have in keeping our young athletes safe. Parental demands of state legislators may be instrumental in changing or instituting state policies pertaining to sideline medical coverage. State medical societies, medical specialty groups, and physician-parents of high school athletes may all be influential in educating athletic directors, school boards, and elected officials at the local and state level, on the important role of ATs in the care of high school athletes and the need for sideline medical coverage of at least some high school athletic events.
Limitations
This study is not without limitations. The most notable is the inherent response bias of all survey-based studies. Although our survey revealed that 92% of high schools in the United States are governed by state athletic associations that do not require sideline medical coverage, many individual schools have a health care provider attend at least some of their athletic events, either through volunteering or under contract, to provide coverage for high-risk sports such as football. A survey of individual high schools would best capture this phenomenon; however, it was not feasible to survey each of the 26,727 public and private high schools in this country. 19 Additionally, the absence of a state policy requiring high schools to employ an AT (part-time or full-time) does not necessarily mean that a school does not have an AT present in some capacity. Many private schools employ a full-time AT, and a significant number of public schools have contractual arrangements with a physical therapy or other health care organization that provides an AT to cover at least some athletic events. Again, a nationwide survey of each high school would be required to determine whether an AT is present in some capacity at their school. Furthermore, these data are only applicable to the study period. Over time, state and/or federal policies may change, potentially leading to more comprehensive sideline medical coverage of high school athletic events. Last, we were only able to obtain survey results from 48 of the 50 states and the District of Columbia. Consequently, these results may have varied if 100% participation had been achieved. Nevertheless, we believe that a 94% response rate for a survey of this nature still provides valuable information regarding the nationwide requirements for mandatory sideline medical coverage and the availability of an AT for high school sports.
In lieu of a formal nationwide survey of every high school to document the presence of sideline high school sports event coverage, previous research done in Illinois, North Carolina, California, and Florida has shown both physician and AT sideline coverage to be inadequate during games and practices.1,8-10,18 Within a large urban high school district in California, Salzman et al 18 found that 70% of schools did not staff a health care professional for practices, 28% did not staff home games, and 30% did not staff away games, for any sport. In fact, a 2015 study that evaluated athletic training services in public secondary schools across the United States found that only 48% of schools provided medical coverage for all sports’ practices. 17 The large body of previous research showing a lack of routine sideline medical coverage coupled with the discrepancies in sideline coverage from state to state reflect the absence of formal nationwide mandates exposed by the current study. Therefore, we believe that statewide mandates should be considered to protect the health and safety of high school athletes most at risk for injury. We acknowledge that financial resources are likely the primary determinant of the services a high school offers its students. Nevertheless, we believe that all high schools should be required to have some degree of sideline medical coverage for its athletic events even if it is limited only to game coverage of high-risk sports such as football. Furthermore, future research should investigate the effect of sideline coverage on injury outcomes across diverse socioeconomic contexts to further advocate for policy change and help ensure the health and safety of all high school athletes.
Despite the limitations of this study, this is the first study, to our knowledge, that clearly quantifies and qualifies the current state-based policies regarding sideline medical coverage of high school athletic events and the provision of AT services at these schools. Quantifying widespread lack of sideline coverage across the country is a crucial first step in identifying ways to improve and standardize the care of high school athletes. We believe that statewide policies mandating sideline medical coverage could help address health care disparities in the diagnosis, treatment, and outcomes after common sports-related injuries, particularly in high schools with limited financial resources or whose students reside in lower socioeconomic neighborhoods. Future studies exploring the effect of AT coverage on injury and reinjury rates of athletes at schools across different socioeconomic levels are needed. Understanding the relationship between student-athlete health and local policies regarding sideline coverage of athletic events is an important step toward improving the health and safety of all student-athletes.
Conclusion
This study highlights the widespread absence of state policies mandating sideline medical coverage or the presence of an AT for high school athletic events, which may contribute to disparities in the care and safety of student-athletes. These findings underscore the need for statewide policies to improve access to trained health care professionals, such as ATs, at sporting events, especially for high-risk sports such as football.
Footnotes
Appendix
High School Sideline Medical Coverage Survey 1. Name_________________________________________________________________________________ 2. Job title_______________________________________________________________________________ 3. State high school athletic association affiliation________________________________________________ 4. How many high schools are governed by your state high school athletic association?_______________________________ 5. How many classes/divisions/levels are used to classify high school sports in your state?_____________________________ 6. How are high school sports classified in your state? (Please circle all that apply). a. By total number of students b. By total number of sports c. Other (please specify)_____________________________________________________________ 7. How does high school sports classification vary within your state? (Please circle all that apply). a. By geographic region b. By sport c. By sex d. It does not vary 8. Is there a state mandate for sideline medical coverage during high school sporting events? (Please circle all that apply). a. Yes b. No c. Varies based on injury risk (ie, football, lacrosse, etc) d. Varies based on geographic region (ie, county, city, township, etc) e. Varies based on sports conference 9. If there is a state mandate for sideline medical coverage during high school sporting events, does it vary by high school classification? (Please circle correct response). a. Yes b. No 10. If there is a state mandate for sideline medical coverage during high school sporting events, does it differ between public and private high schools? (Please circle correct response). a. Yes b. No 11. If there is a state mandate for sideline medical coverage during high school sporting events, which of the following health care providers can satisfy this coverage requirement? (Please circle all that apply). a. Certified athletic trainer (ATC) b. Emergency medical technician (EMT)/paramedic c. Physical therapist d. Physician (MD/DO) e. Other (please specify)_____________________________________________________________ 12. Is there a distinction between mandated sideline medical coverage during collision sporting events in which there is an increased risk for injury (eg, football) versus sporting events that have a reduced risk for injury (eg, volleyball)? (Please circle correct response). a. Yes b. No 13. If you answered “Yes” for Question 12, please specify which sports are included. __________________________________ 14. If there is a state mandate that sideline medical coverage is required during collision sporting events in which there is an increased risk for injury (eg, football), which of the following health care providers can satisfy this coverage requirement? (Please circle all that apply). a. Certified athletic trainer (ATC) b. Emergency medical technician (EMT)/paramedic c. Physical therapist d. Physician (MD/DO) e. Other (please specify)_____________________________________________________________ 15. Is there a state mandate that certified athletic trainers (ATCs) must be employed at each high school? (Please circle correct response). a. Yes b. No 16. If you answered “Yes” for Question 15, please specify the level of employment required (Please circle correct response). a. Employed full-time b. Employed for event coverage only 17. If there is a state mandate that certified athletic trainers (ATCs) must be employed at each high school, does it differ between public and private high schools? (Please circle correct response). a. Yes b. No
Thank You!
Acknowledgements
The authors thank the members of the AOSSM Council of Delegates and the state representatives of the National Athletic Trainers Association who assisted in the distribution of the survey to all 50 states and the District of Columbia. They would also like to thank the members of the AOSSM BOLD (Boosting Orthopaedic Leaders’ Development) program who collected and assisted in the analysis of the survey data.
Final revision submitted August 3, 2025; accepted September 12, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: This research was supported by the University of Chicago Pritzker School of Medicine. M.A. has received food and lodging from the University of Chicago Pritzker School of Medicine. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Chicago Institutional Review Board (IRB24-0127).