
Abstract
Background:
Surgical management of ulnar collateral ligament (UCL) tears in nonthrowing athletes is less commonly performed, and the outcomes of that management have not been thoroughly described.
Purpose:
To describe the clinical outcomes of surgical management of UCL injury in nonthrowing athletes.
Study Design:
Case series; Level of evidence, 4.
Methods:
A retrospective review was conducted on all patients who underwent UCL reconstruction or repair across a 10-year period (2010-2020), with nonthrowing athletes who had >2-year follow-up being specifically identified. Demographic variables such as age, sport participation, concomitant procedures, and graft type, as well as postoperative outcomes such as complications, patient satisfaction, return to play (RTP), and patient-reported outcomes (PROs), were recorded for the whole cohort as well as stratified by repair and reconstruction group. Data were presented as mean with standard deviation or median with range and odds ratio calculated as appropriate.
Results:
A total of 19 nonthrowing athletes undergoing either UCL reconstruction (n = 12) or repair (n = 7) met the inclusion criteria for the study. Sport participation included 5 cheerleaders, 4 wrestlers, 4 gymnasts, 2 lacrosse players, 1 boxer, 1 mixed martial arts fighter, and 1 football player (offensive lineman). The mean age for these patients was 20.1 ± 7.3 years with 52.6% of patients being female. The majority of tears were proximal (72.2%). Overall, 68.4% were able to RTP (58.3% UCL reconstruction; 85.7% repair) after 9.5 months (9.86 months UCL reconstruction; 9.0 months repair) with 76.9% (10/13) of the athletes returning to the same or higher level of competition.
Conclusion:
This study demonstrates that surgical management via either UCL reconstruction or repair can result in high rates of good-to-excellent PROs, high levels of patient satisfaction, and time to RTP that is earlier, albeit with a slightly lower overall rate of RTP, than that generally described in throwing athletes.
Keywords
Injuries to the ulnar collateral ligament (UCL) are commonly described in overhead throwing athletes participating in sports such as baseball, softball, and javelin. Surgical management of UCL injuries was popularized after Dr. Frank Jobe performed the first reconstruction in 1974. 14 Prior to Jobe's landmark work, UCL injuries were often career ending for many competitive throwing athletes. Over the years, surgical management of UCL tears has been refined and high rates of good-to-excellent results are regularly seen in throwing athletes 19 with reported return to pitching at the major league level nearing 90%. 10
UCL injuries are not exclusive to throwing athletes. 26 Small case reports and epidemiological studies have described these injuries in numerous nonthrowing athletes including National Football League players, combat athletes/martial artists, and gymnasts.11,17,24,33 Much of this existing literature on nonthrowing cohorts describes definitive nonoperative treatment, with surgical management less frequently performed than in their throwing athlete counterparts. Rothermich et al 29 were the first to share their promising results for both UCL repair and reconstruction in a series of 40 nonthrowing athletes. However, only a handful of other studies have reported outcomes for surgical management of UCL tears in nonthrowing athletes—all of which were included as subgroup analyses in studies primarily focused on throwing athletes; therefore, the unique facets of caring for the UCL-injured nonthrowing athlete has not been appropriately emphasized.5,7,23
Thus, the purpose of this study is to describe the clinical outcomes of surgical management of UCL injury performed at a single institution in nonthrowing athletes, including both UCL reconstruction and UCL repair. Our hypothesis is that nonthrowing athletes will achieve a high rate of return to play (RTP) that is earlier than what is reported in the literature for throwing athletes.3,13,16,20,25,31
Methods
After approval by our institutional review board, a retrospective review was conducted on all patients who underwent UCL reconstruction or repair (Current Procedural Terminology codes 24345 and 24346) from 2010 to 2020. Each procedure was performed by 1 of 6 fellowship-trained sports medicine (M.G.C., S.B.C., C.C.D.) or hand, elbow, and upper extremity surgeons at our institution. Manual chart review was performed to determine which patients could be considered nonthrowing athletes. After cohort identification, information regarding patient characteristics (age, sex, sport, level of competition), presence of preoperative ulnar neuritis and elbow range of motion (ROM) as assessed by the primary attending surgeon, and magnetic resonance imaging (MRI) characteristics of the tear (location, extent, tissue attenuation/ligamentous degeneration) and stress ultrasound (SUS) results (widening with stress of injured side and comparison with contralateral side) as interpreted by musculoskeletal radiologists were collected through patient chart review and imaging analysis. Postoperative patient-reported outcomes (PROs) including the short version of the Disabilities of the Arm, Shoulder and Hand score (QuickDASH), 12 Timmerman-Andrews elbow score, 32 and American Shoulder and Elbow Surgeons (ASES) 27 scores as well as sport-related outcomes such as RTP status, timing, and competitive level of RTP were collected through telephone questionnaires administered by dedicated research personnel at approximately 2 years postoperatively. Patients were excluded if they were a throwing athlete (ie, baseball player, softball player, football quarterback, javelin thrower), had <2-year follow-up, or if they had additional bony or ligamentous injury to the elbow at the time of reconstruction or repair (ie, traumatic elbow dislocation with lateral ligament injury, fracture, etc).
Surgical Indications and Technique
All patients undergoing surgery had clinical and radiographic signs of UCL injury. Physical examination findings included pain/tenderness along the UCL and a positive milking maneuver and/or moving valgus stress test. The majority of patients undergoing surgery had an MRI (with or without contrast) of the elbow demonstrating signs of either partial or complete tear of the UCL. Additionally, SUS was performed in many cases to further confirm diagnosis when clinically indicated, such as in cases of partial tear. Our institution has demonstrated high accuracy as well as inter- and intraobserver reliability when combined MRI and SUS is utilized for assessment of UCL injuries. 28 When clinically appropriate, a trial of nonoperative management consisted of rest, bracing, and physical therapy, with or without injection. The decision to proceed with surgical management (ie, reconstruction or repair) was dependent on a combination of clinical and radiographic findings, failure of nonoperative management, intraoperative findings of ligament quality and tear pattern, and patient as well as surgeon preference. 6 While indication for UCL reconstruction versus repair was made on a case-by-case basis involving shared decision making between the patient and surgeon, patients were generally indicated for UCL repair when they had proximal or distal tears with adequate quality of the remainder of ligamentous tissue. Patients with midsubstance tears and/or those with degenerative ligamentous changes seen on MRI or in the operating room were not considered candidates for UCL repair and thus underwent UCL reconstruction.
All procedures were performed with the use of an upper extremity tourniquet. An 8- to 10-cm incision was made just anterior to the medial epicondyle for reconstruction whereas a slightly smaller, distally based incision was often made for UCL repair given the lack of humeral tunnel drilling. Identification of the medial antebrachial cutaneous nerve as well as the ulnar nerve was performed. A muscle-splitting approach through the flexor-pronator mass was utilized by all surgeons. All reconstructive procedures utilized either the docking or the modified Jobe technique. Graft choice was made based on individual surgeon preference and included ipsilateral palmaris or ipsilateral or contralateral gracilis autograft. When UCL repair was performed, the native ligament was repaired to its origin/insertion and was most commonly augmented with a collagen-coated suture tape (Internal Brace; Arthrex Inc), which was secured using bioabsorbable suture anchors (SwiveLock; Arthrex Inc) in the sublime tubercle and the medial epicondyle. There was 1 case of proximal tear repair with the use of a suture anchor (GII QUICKANCHOR; DePuy Synthes) without suture tape augmentation. The decision to perform subcutaneous ulnar nerve transposition was based on the presence of preoperative ulnar neuritis and/or instability as diagnosed by clinical examination, nerve conduction study, and SUS observations of instability.
Postoperative Rehabilitation
Our preferred postoperative rehabilitation protocol for nonthrowing athletes differed between UCL reconstruction and UCL repair. For UCL reconstruction, the general postoperative rehabilitation protocol was as follows:
0-2 weeks: splint or brace locked at approximately 90° of flexion
3-4 weeks: transition any splint to hinged brace (progress to 20°-90°) to remain on at all times
Progress passive ROM exercises
Begin gentle grip strengthening in brace
5-8 weeks: progress hinged brace 0°-120° to remain on at all times
Begin formal physical therapy to emphasize full elbow ROM (0°-120°)
Gentle stretching, forearm and rotator cuff strengthening
9-12 weeks: discontinue brace, begin forearm resistance exercises
When full elbow ROM is achieved, discontinue brace and begin forearm resistance exercises
Continue advancing rotator cuff and scapular strengthening
13-16 weeks: initiate swinging activities (ie, golf club, racquet) and gradual return to sport-related activities
24-30 weeks: return to sport participation
For UCL repair, the general postoperative rehabilitation protocol was as follows:
0-2 weeks: splint or brace locked at approximately 90° of flexion
3-4 weeks: transition any splint to hinged brace (progress to 20°-90°) to remain on at all times
Progress passive ROM exercises
Begin gentle grip strengthening in brace
5-6 weeks: progress hinged brace 0°-120° to remain on at all times
Begin formal physical therapy to emphasize full elbow ROM (0°-120°)
Gentle stretching, forearm and rotator cuff strengthening
7-10 weeks: discontinue brace, begin forearm resistance exercises
When full elbow ROM is achieved, discontinue brace and begin forearm resistance exercises
Continue advancing rotator cuff and scapular strengthening
11-12 weeks: initiate swinging activities (ie, golf club, racquet) and gradual return to sport-related activities
Gentle valgus loads can be initiated at approximately 12 weeks
13-16 weeks: begin plyometric program and aggressive upper extremity strengthening
17-24 weeks: return to nonthrowing sport participation
However, it should be noted that specific details regarding timing, speed of progression, and return to activity and full sport participation are variable and should be made on a case-by-case basis.
Data Collection and Statistical Analysis
Demographic variables, sport participation, concomitant procedures, graft type, complications, patient satisfaction, RTP, and PROs were recorded for the whole cohort and stratified by repair and reconstruction groups. Kerlan-Jobe Orthopaedic Clinic shoulder and elbow scores were not included because of the emphasis placed by this tool on primarily throwing and other overhead athletes (ie, How much has your velocity, control, and endurance been affected due to your arm?). 1 Categorical data are presented as incidence with percentages. Continuous data are presented as the arithmetic mean with standard deviation or median with interquartile range when the data features statistical outliers. Odds ratios were calculated and reported with 95% CIs. Values were reported with statistical significance set at P < .05. Given that this was not a comparative study, no power analysis was performed.
Results
Overall Cohort Characteristics and Outcomes
Upon initial query, 427 patients undergoing primary UCL reconstruction or repair were identified. The substantial majority of these included baseball and softball players as well as javelin throwers. Thus, after careful chart review, a total of 19 nonthrowing athletes that underwent either UCL reconstruction or repair met the inclusion criteria. A total of 12 patients underwent UCL reconstruction and 7 underwent UCL repair. The nonthrowing sport participation of these patients included cheerleading (5), wrestling (4), gymnastics (4), lacrosse (2), boxing (1), mixed martial arts (1), and football lineman (1). The mean ± SD age was 20.1 ± 7.3 years and 52.6% of patients were female (Table 1). Data from MRI evaluation was available for 18 of the 19 patients and demonstrated that a majority of the tears were proximal (72.2%). There were no midsubstance tears identified by radiology report. A majority of tears were described as partial thickness (61.1%).
Baseline Characteristics and Outcomes for Entire Study Cohort (N = 19) a
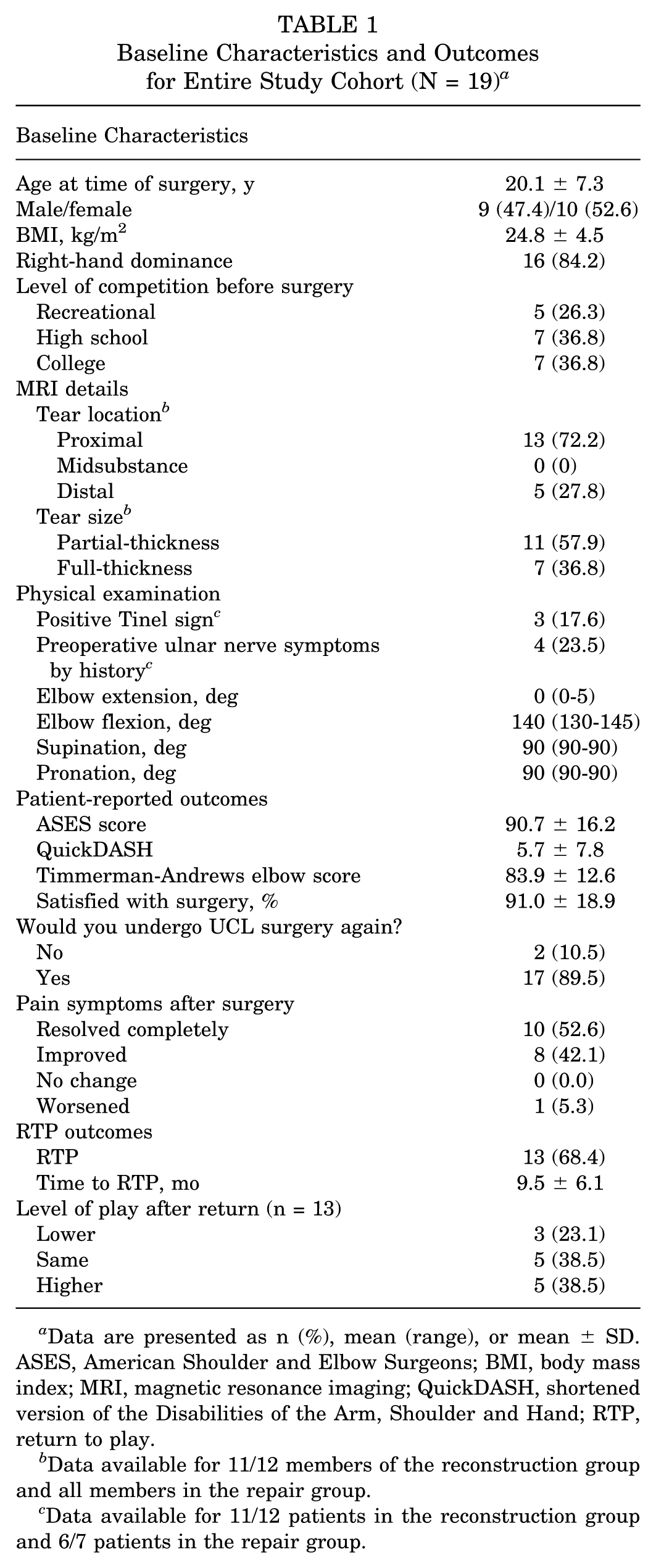
Data are presented as n (%), mean (range), or mean ± SD. ASES, American Shoulder and Elbow Surgeons; BMI, body mass index; MRI, magnetic resonance imaging; QuickDASH, shortened version of the Disabilities of the Arm, Shoulder and Hand; RTP, return to play.
Data available for 11/12 members of the reconstruction group and all members in the repair group.
Data available for 11/12 patients in the reconstruction group and 6/7 patients in the repair group.
Overall, the ASES score was 90.7 ± 16.2, Timmerman-Andrews score was 83.9 ± 12.6, and overall RTP rate was 68.4%. More specifically, 52.6% (10/19) of the athletes total athletes, including 76.9% (10/13) who reported return to competition reported returning to the same or higher level of competition.
UCL Repair and UCL Reconstruction
When evaluating the 12 patients who underwent UCL reconstruction (8 docking, 4 modified Jobe technique) and 7 who underwent a UCL repair procedure, the groups had no significant differences in baseline characteristics of age (P = .87), sex (P = .65), body mass index (P = .26), hand dominance (P > .05), laterality of procedure (P = .63), and baseline level of competition (P = .50) (Table 2).
Presurgical Evaluation of Demographic Data, MRI Results, and Physical Examination Findings Between UCL Reconstruction and Repair Cohorts a
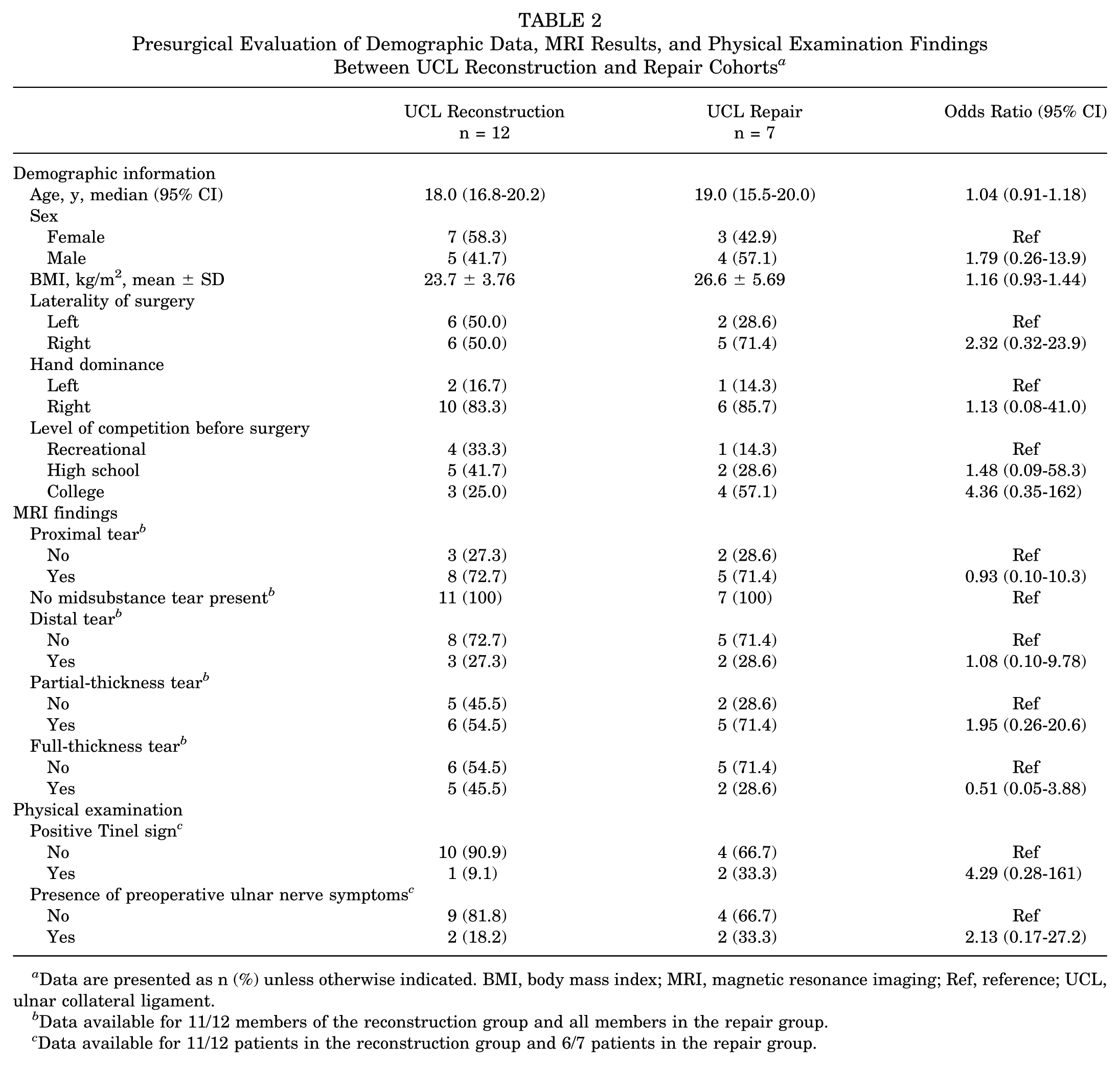
Data are presented as n (%) unless otherwise indicated. BMI, body mass index; MRI, magnetic resonance imaging; Ref, reference; UCL, ulnar collateral ligament.
Data available for 11/12 members of the reconstruction group and all members in the repair group.
Data available for 11/12 patients in the reconstruction group and 6/7 patients in the repair group.
Presurgical Evaluation and Findings
Eighteen patients (94.7%) (n = 12, reconstruction; n = 6, repair) had MRI evaluations (n = 12, MRI without contrast; n = 6, with intra-articular contrast) performed before surgery and 6 patients (31.6%) underwent preoperative SUS. One patient (5.3%) was diagnosed and indicated for surgery based on results of valgus stress elbow radiographs. Before surgery, 2 (18.2%) patients in the reconstruction group and 2 (33.3%) patients in the repair group reported ulnar nerve–related symptoms. Seventeen patients had full ROM of the elbow (Table 2), 34 with 1 patient in each group having a restricted flexion <120°. The MRI characteristics are outlined in Table 3. There was no difference between groups in the rate of tear location (proximal/midsubstance/distal) (P≥ .05, respectively) or tear completeness (partial-/full-thickness) (P = .64 for both).
Postoperative PROs and RTP Data After UCL Reconstruction and Repair a
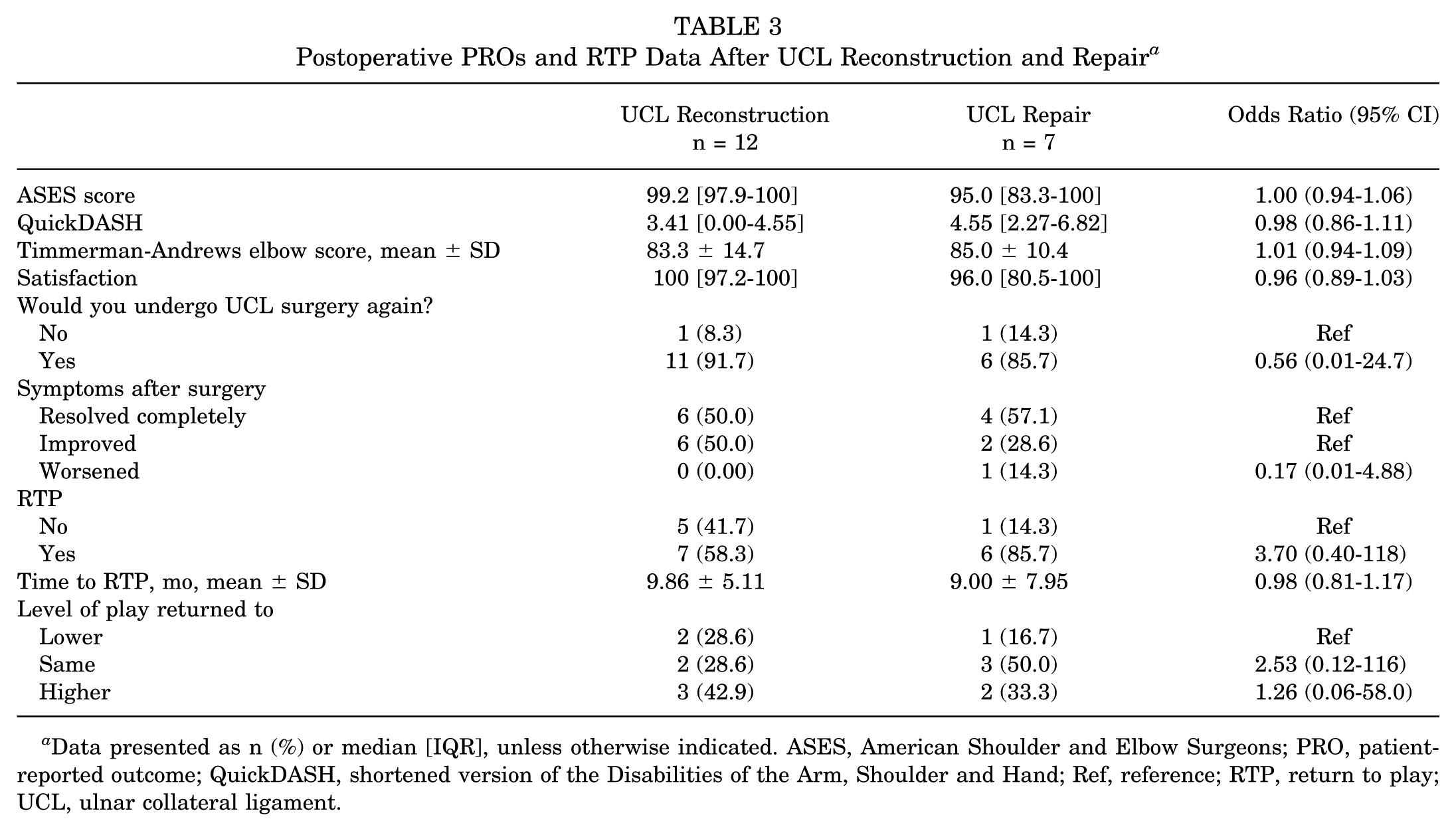
Data presented as n (%) or median [IQR], unless otherwise indicated. ASES, American Shoulder and Elbow Surgeons; PRO, patient-reported outcome; QuickDASH, shortened version of the Disabilities of the Arm, Shoulder and Hand; Ref, reference; RTP, return to play; UCL, ulnar collateral ligament.
Treatment Before Surgery and Operative Details
Before surgery, 13 patients (68.4%) attempted nonoperative treatment of their UCL injury that included formal physical therapy, rehabilitation, and bracing. Ten patients in the reconstruction group attempted nonoperative treatment with 1 also reporting having received a corticosteroid injection during nonoperative treatment. Three patients in the repair cohort reported attempting nonoperative treatment. No patients in either group elected biologic treatment (ie, platelet-rich plasma injection) before surgery.
Six reconstructions were performed utilizing a gracilis graft (5 autografts and 1 allograft), 4 were performed with palmaris longus autografts, and 2 were performed with a semitendinosus allograft. Two reconstruction patients underwent concomitant subcutaneous ulnar nerve transposition and 1 repair patient underwent an arthroscopic loose body removal and debridement. There were no intraoperative complications reported. There were no cases of postoperative infection, revision, reoperation, postoperative ulnar nerve symptoms, or need for manipulation under anesthesia.
Postoperative Outcomes
Postoperative outcome scores were similar between groups including ASES (P = .53), QuickDASH (P = .49), and Timmerman-Andrews scores (P = .78). On a scale from 0 to 100 with 100 being entirely satisfied, satisfaction with surgery was similar between groups (P = .26) as was the rate at which patients reported they would choose to undergo surgery again (P≥ .99). All patients in the reconstruction group and 85.7% of those in the repair group reported symptoms improving or completely resolving after surgery (P = .33) (Table 3). Interestingly, 55.6% (5/9) of gymnasts or cheerleaders were unable to return to their respective sport. One wrestler (25.0%; 1/4) was unable to return to sport, but all lacrosse, mixed martial arts, football, and boxing athletes were otherwise able to return to some level of sport participation.
Postoperatively, all patients underwent formal physical therapy rehabilitation (reconstruction, 5.21 ± 3.35 months; repair, 4.36 ± 3.64 months; P = .62). All had full ROM in flexion, extension, pronation, and supination, however, 1 patient had hyperextension (–20°) on physical examination after surgery (compared with 5° short of full extension preoperatively). Notably, while no patients in the reconstruction cohort reported suffering any subsequent elbow (including UCL-related symptoms) or shoulder injury after their UCL surgery, 1 patient in the repair cohort sustained a partial tear of the distal biceps tendon 3 years after initial surgery.
Discussion
The principal findings of this study are that >91% of nonthrowing athletes with UCL tear were satisfied with results after undergoing UCL reconstruction or repair. Additionally, 94% of all patients reported improvement in pain or instability-related symptoms experienced before surgery, improvement in PROs was comparable with that described by throwing athletes, and mean time to RTP was approximately 9 months regardless of repair or reconstruction. There was a slightly lower rate of RTP in this study compared with what has been frequently described in high-level throwing athletes, with 53% of nonthrowing athletes able to return to the same or higher level of sport after either UCL reconstruction or repair, however, of the 13 who were able to RTP, 77% of them did so at the same or higher level. Injuries to the UCL in the nonthrowing athlete appear to differ with regard to rehabilitation protocols and surgical outcomes compared with those in throwing athletes.
The primary UCL injury mechanism in the nonthrowing athlete involves an acute traumatic valgus load to the elbow while performing activities such as an arm bar submission in martial arts, a back handspring in gymnastics, or blocking in football linemen. 26 This comes in contrast to the repetitive valgus loads seen in the elbows of overhead athletes, which are often accompanied by ligament thickening, calcification, and hyperechoic foci within the UCL as seen on MRI and SUS, indicative of repetitive use and strain on the ligament. 4 In our cohort of nonthrowing athletes, there were no midsubstance injuries described. Instead, all injuries represented avulsion-type tears either proximally (72%) or distally (28%)—in contrast to the 86% rate of distal UCL tears found on predraft MRI in Major League Baseball pitchers described by Erickson et al. 9 These findings may have clinically meaningful implications. It may suggest that midsubstance tear patterns more commonly occur by attritional mechanisms than acute traumatic ones. The high prevalence of proximal avulsion tears seen in this cohort may portend a favorable prognosis for those athletes attempting nonoperative management given the proximal ligament's more favorable blood supply.2,26 However, when nonoperative management fails in the nonthrowing athlete, the combination of more favorable vascularity of proximal injury and an acute injury mechanism in the absence of more chronic degenerative changes to the ligament could make these injuries more amenable to treatment with repair rather than reconstruction. Ultimately, however, further study on this topic is needed to determine the optimal management strategy (reconstruction vs repair) for predominantly nonthrowing athletes.
The mean time to RTP after UCL reconstruction in the present study was 9.86 months, closely matching the 10 months reported by Rothermich et al 29 in a similar cohort of nonthrowing athletes. Time to RTP was 2 to 3 months earlier than the approximately 12 to 13 months that has been frequently described in previous studies assessing UCL injury in overhead throwers (predominantly baseball players),3,13,16,20,25,31 a finding that likely stems from the accelerated rehabilitation protocol utilized following reconstruction for nonthrowing athletes because of the lack of repetitive throwing in this cohort. However, the mean time to RTP after repair was 9 months, nearly 2 months longer than that described by Rothermich et al. There are multiple potential reasons for these differences in time to RTP. First, while not specifically reported, the latter study may have utilized a more expedient rehabilitation and RTP protocol. Additionally, given the lower frequency of this injury in nonthrowing athletes, some clinicians may favor a more conservative RTP protocol mirroring that used in throwing athletes. Given the reported 4 to 5 months spent in formal physical therapy postoperatively, it is also possible that external factors such as the date of injury and surgery in relationship to the timing of the season could have prolonged the reported time to RTP. The more likely explanation, however, stems from the small sample sizes and resulting fragility of the data in the present study (1 out of 7 patients reported a time to RTP of 24 months; median RTP was 8 months) and the study by Rothermich et al in which the mean reported time to RTP for nonthrowing athletes was surprisingly longer than the 6.7 months previously reported after UCL repair in throwing authors by the same authors. 6 Despite this, the apparent advantage of an accelerated recovery and time to RTP seen in UCL repair in throwing athletes15,22 also seems to hold true in the nonthrowing athlete when compared with UCL reconstruction.
Functional outcomes after UCL repair and reconstruction in nonthrowing athletes were excellent. Notably, ASES scores were excellent for both UCL reconstruction (99.2) and UCL repair (95.0), which appears similar to data reported in throwing athletes who RTP. 21 These outcomes are similar to those reported by Rothermich et al 29 in their cohort of nonthrowing athletes. Additionally, we found that the overwhelming majority of patients were satisfied (17/19 reported >80% satisfaction on a 100-point scale) with surgery and that nearly 90% would elect to undergo surgery again. Despite this, however, only 68% of patients were able to RTP, and of those who did RTP, 77% were able to return to the same or a higher level than before their injury. These reports are lower than the >80% reported RTP in high-level baseball players,3,13 and Erickson et al10 suggested that baseball players of a higher level (professional, collegiate) may have a higher rate of RTP than those of lower-level high school pitchers. 8 Given the predominance of recreational and high school athletes (12/19; 63.2%) in the present study compared with generally high-level (college and professional) pitchers and baseball players analyzed in much of the baseball-related UCL injury literature,30,31 it is possible that our lower reported rate of RTP stems from different baseline levels of competitiveness. Specifically, 89.5% (17/19) of athletes indicated that their elbow had little or no effect on their activity; therefore, it is reasonable to consider that this primarily recreational- and high school–level cohort elected to participate in a different sport or activity—thus affecting our reported RTP. Last, as the rate of UCL reconstruction and repair continue to rise in throwing athletes, these injuries are often viewed as a means of maintaining sport participation for competitive throwers, and thus the preoperative expectations between throwers and nonthrowers could be inherently different. Nevertheless, of the athletes able to successfully RTP, 77% were able to do so at the same or even a higher level of competition. Therefore, surgical treatment of UCL injury in nonthrowing athletes can be seen as a viable and successful option for patients who fail nonoperative treatment.
Limitations
This study must be considered with respect to its limitations. Because of the low incidence of UCL injuries in nonthrowing athletes, 18 which made up a small portion of surgical UCL injuries at our institution over a 10-year period, this study lacks sufficient power to make direct comparisons in outcomes between UCL reconstruction and repair. Furthermore, the small sample size included in the study left the reported data especially fragile, as was seen and previously described in our reported RTP after surgery. However, the only previous study focusing specifically on UCL injuries in nonthrowing athletes included only 40 patients; thus, the current study from another high-volume center treating UCL injury adds necessary data to a scant body of literature. This study is a retrospective review with a heterogeneous cohort of athletes at different levels and stages of their respective sports and seasons. Preoperative PRO scores were not collected and there is also a risk of recall bias, as is commonly seen in such retrospective questionnaire-based studies. Furthermore, data on rate and timing of RTP are heavily dependent upon timing of injury relative to athletes’ respective seasons and personal careers as well as the level of competition and pressure on the athlete to return. Because our cohort of patients was primarily recreational and high school athletes, the pressure for RTP in our cohort may not be the same as those of college- and professional-level pitchers. This factor likely contributes to our mean time to RTP of approximately 9 months despite reports of accelerated return of nonthrowing athletes after UCL reconstruction and repair. Finally, surgical management of UCL tears is subject to some selection bias, with individual surgeons making an often-intraoperative decision on whether to perform UCL reconstruction or repair.
Conclusion
Our study demonstrates that surgical management via either UCL reconstruction or UCL repair can result in high rates of good-to-excellent PROs, high levels of patient satisfaction, and time to RTP that is earlier, albeit with a slightly lower overall rate of RTP, than that generally described in throwing athletes.
Footnotes
Final revision submitted July 15, 2025; accepted September 8, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.B.C. receives royalties from Major League Baseball, is a board or committee member of the AOSSM, and is an editorial or governing board member of The American Journal of Sports Medicine and The Video Journal of Sports Medicine. M.G.C. is a board or committee member of the Major League Baseball Team Physicians Association and the Orthopaedic Learning Center. W.L.J. is a board or committee member of the AOSSM. C.C.D. receives royalties from, is a paid consultant for, and holds stock or stock options in Aevumed. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Thomas Jefferson University Hospitals (iRISID-2022-0917).