
Abstract
Background:
The aim of surgical treatment for posterolateral rotatory instability (PLRI) of the elbow is to restore the integrity of the lateral ulnar collateral ligament (LUCL), with ligamentous reconstruction being the preferred option for recurrent symptomatic PLRI. However, there is no clinical evidence demonstrating the superiority of reconstruction versus repair. Treatment options currently depend on the cause of the LUCL injury and surgeon preference.
Purpose:
To review studies comparing surgical outcomes of LUCL reconstruction versus repair in treating PLRI of the elbow.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
This review was conducted according to PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. A literature search was conducted on PubMed, Medline (via EBSCO), ProQuest, and ScienceDirect databases using the following keywords: “(lateral ulnar collateral ligament reconstruction)” OR “(lateral ulnar collateral ligament repair)” AND “(outcome).” Excluded were studies in languages other than English, those that included terrible triad injury, transolecranon fracture, radial head arthroplasty involvement, associated procedures, animal studies, and biomechanical studies. A total of 193 studies were identified after the initial search. The primary outcome measure was the Mayo Elbow Performance Score, which was compared between studies using a random-effects model.
Results:
Overall, 20 studies (N = 646 patients) were included, with 445 of 646 patients (68.8%) in the LUCL reconstruction group and 201 of 646 patients (31.1%) in the LUCL repair group. All injuries in the included studies were traumatic. The LUCL reconstruction group had a longer follow-up period compared with the LUCL repair group (72.05 ± 43.51 vs 36.86 ± 21.19 months, respectively). The postoperative range of motion arc was similar in both the repair and reconstruction groups (135.02°± 15.33° vs 133.60°± 8.84°, respectively). Both LUCL repair and LUCL reconstruction resulted in good to excellent outcomes on patient-reported outcome measures; however, a superior rate of return to activity and a lower complication rate were found after LUCL reconstruction versus LUCL repair (8.3% vs 14.9%). Ulnar nerve event (2.3%) was the most common complication in both groups.
Conclusion:
Findings indicated that LUCL reconstruction had a superior rate of return to activity and a lower complication rate compared with LUCL repair.
Posterolateral rotatory instability (PLRI) is a common form of recurrent elbow instability that was described by O’Driscoll 25 in 1994, implicating the lateral ulnar collateral ligament (LUCL) as a primary restraint for PLRI. The condition occurs as a result of axial loading, valgus force, and forearm supination. 3 This is relatively due to the internal rotation of the humerus on a fixed forearm. However, the functional anatomy of the remaining lateral elbow stabilizing structures indicates that PLRI constitutes a more complex problem. A more recent biomechanical cadaveric study suggested that damage to the lateral collateral ligamentous complex as a whole may be responsible for PLRI. 27
Although PLRI generally occurs after elbow trauma, other causes include tardy PLRI secondary to cubitus varus deformity, severe lateral epicondylitis—especially after repeated corticosteroid injections, or iatrogenic injury after lateral elbow surgery. In most cases, the mechanism involves a combination of axial load, valgus force, and supination on the forearm, resulting in the disruption of the LUCL from its humeral origin. PLRI itself gives a spectrum of mechanical symptoms, such as pain, clicking, recurrent subluxations, and dislocations. If PLRI is left untreated, posttraumatic arthritis may develop as a result of joint incongruency and cartilage damage. Establishing the diagnosis of PLRI may be difficult and is often delayed because of its variable presentation.7,30
The restoration of LUCL integrity is the main purpose of the surgical treatment of PLRI. Treatment options depend on the cause of the LUCL injury and the surgeon's preference. The choice to perform repair versus reconstruction typically depends on the chronicity of the injury and the quality of tissue available at the time of surgery. Surgical repair is more favorable for acute traumatic cases or in occasions where the tissue is still viable and has good healing potential. 24 Jones et al15, 16 showed that UCL repair with internal bracing was more resistant under fatigue loading compared with UCL reconstruction. Meanwhile, the main approach for addressing recurring PLRI involves the restoration of the LUCL. Reconstruction is the recommended surgical treatment when there is long-term weakening or a notable insufficiency in the ligament tissue, particularly among athletes performing overhead activities and persons who are engaged in strenuous manual labor. 23 There is no clinical evidence demonstrating the superiority of either LUCL repair or reconstruction.
In the present review, we aimed to compare studies on the surgical outcome of LUCL reconstruction versus repair in treating PLRI of the elbow. Based on the existing literature, we hypothesized that the results of LUCL reconstruction and LUCL repair would be comparable and that outcomes would depend on the patients’ circumstances—such as injury severity and time from injury to treatment.
Methods
Search Strategy and Study Selection
This study was conducted in accordance with the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA), 28 and the study protocol was registered in the PROSPERO International Prospective Register of Systematic Reviews (CRD42023418856). We searched 4 databases—including PubMed, Medline via EBSCO, ProQuest, and ScienceDirect—from inception until September 2022 for relevant studies using the following keywords, which conformed to MeSH (Medical Subject Headings) and Emtree: “(Lateral ulnar collateral ligament reconstruction) OR (Lateral ulnar collateral ligament repair) AND (outcome).” As the number of studies investigating LUCL injury and treatment was limited, we made no restrictions with respect to specific surgical techniques, publication status, or study period. After eliminating duplicate studies, 2 independent reviewers (M.A. and L.C.S.) screened the titles and abstracts for relevant studies according to the inclusion and exclusion criteria.
Inclusion and Exclusion Criteria
All included studies were original research publications in the English language. Studies that included diagnosis, imaging, or treatment with open or arthroscopic LUCL repair or reconstruction for PLRI were included. The exclusion criteria included studies that included terrible triad injury, transolecranon fracture, radial head arthroplasty involvement, associated procedures at the time of surgery, and animal and biomechanical studies. Conference abstracts were also excluded.
Quality Appraisal and Risk-of-Bias Assessment
Two authors (M.A. and L.C.S.) independently performed data extraction and quality assessment. Discrepancies between the authors were resolved by reassessment and discussion with a third author specializing in elbow surgery (E.K.). The level of evidence of each included study was assessed using the guidelines of the Oxford Centre for Evidence-Based Medicine. 14 Quality appraisal and risk of bias were assessed using the Methodologic Index for Non-randomized Studies 1 (MINORS). The MINORS consists of a 12-item checklist comprising 8 items for noncomparative studies, with 4 additional items for comparative studies. Each item is scored from 0 to 2, with a maximum of 16 points for noncomparative studies and 24 points for comparative studies. Since the scoring system has no predefined cutoff, we considered the studies as high quality if the MINORS score was >60% (9/16 for noncomparative studies).
Data Extraction and Analysis
Data were extracted from the texts, figures, tables, and associated supplementary files and comprised (1) patient characteristics; (2) preoperative characteristics (eg, radiological findings); (3) intraoperative characteristics; and (4) postoperative outcomes (eg, functional outcomes, rate of return to work or sport, patient satisfaction, and complications). Collated data were summarized in tables using Excel (2013; Microsoft Corp). A qualitative assessment was performed to produce a narrative report. Treatment modalities were compared using subgroup analysis. Statistical analysis was conducted using OpenMeta-Analyst software (Brown University CEBM). The I2 value was used to identify the heterogeneity between studies.
The primary outcome measure was the functional outcome of the patients as measured using the Mayo Elbow Performance Score (MEPS). MEPS values were provided as scores from 0 to 100 or as categories: poor (<60), fair (60-74), good (75-89), or excellent (90-100). The secondary outcomes were the visual analog scale (VAS; 0-10) for pain, as well as postoperative complications. The MEPS values across relevant studies were assessed using a random-effects model, with forest plots used to identify outcomes. Statistical significance was set at P < .05.
Results
Included Studies
Overall, 20 studies met the inclusion criteria; 18 were level 4 case series, and the remaining 2 were level 3 retrospective cohort studies. †† Figure 1 shows the PRISMA 27 flow diagram of the study inclusion process.

PRISMA flow diagram of the study inclusion process. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Quality Assessment
The mean MINORS score for all 20 studies was 10.1 (Figure 2). Overall, all but 1 study 34 were considered high-quality studies with a low risk of bias.

Distribution of MINORS Score in the included studies. MINORS, Methodologic Index for Non-randomized Studies.
Included Patients
A total of 646 patients (n = 646 elbows) with PLRI were included in 20 studies (Table 1). There were 367 elbows in men (56.8%) and 279 elbows in women (43.2%). The dominant extremity was affected in 27.8% of patients (180/646). The mean waiting time was 18.1 months (range, 3 weeks-51.3 months); the mean follow-up was 4.5 years (range, 1-19 years).
Characteristics of the Included Studies (N = 20) a

LOE, level of evidence; NR, not reported; Retrosp, retrospective; US, United States.
Time from injury to surgery.
Preoperative Characteristics
The preoperative characteristics are shown in Table 2. Most patients experienced pain at rest (475; 73.5%) and instability symptoms (532; 82.3%). The most common instability test performed was the pivot-shift test, which was found positive in 40.2% (260/646) of patients, followed by the varus stress test (104/646; 16%) and posterolateral drawer test (56/646; 8.6%). Other instability tests performed include the chair push-up test (29/646; 4.4%) and the tabletop relocation test. The preoperative range of motion (ROM) was only available in 338 patients (52.3%), with limited ROM found in 24 patients (3.7%). All patients underwent standard elbow radiographs; other imaging modalities such as magnetic resonance imaging and computed tomography were performed on 455 (70.4%) and 31 (4.7%) patients, respectively.
Preoperative Characteristics of the Included Studies a
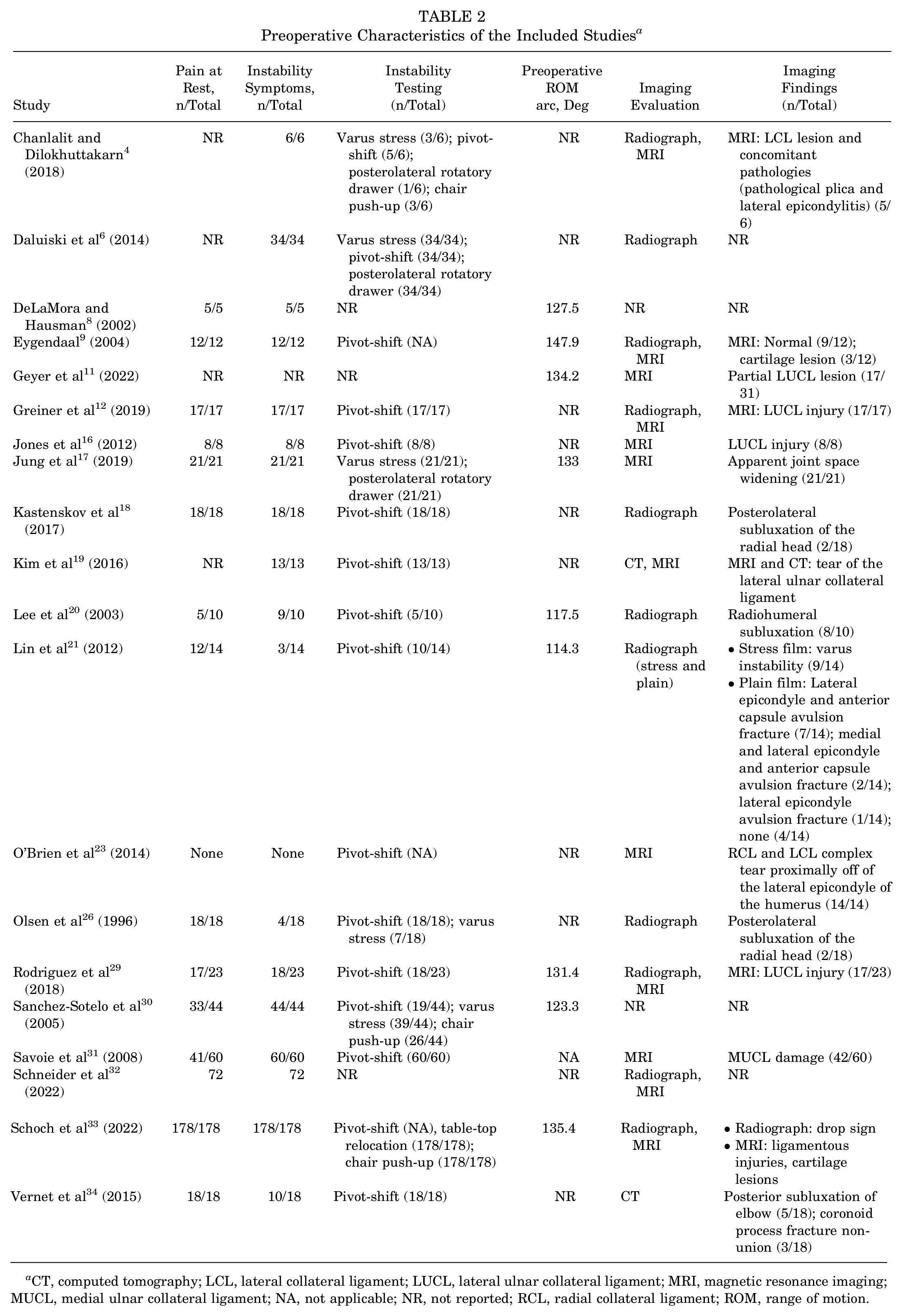
CT, computed tomography; LCL, lateral collateral ligament; LUCL, lateral ulnar collateral ligament; MRI, magnetic resonance imaging; MUCL, medial ulnar collateral ligament; NA, not applicable; NR, not reported; RCL, radial collateral ligament; ROM, range of motion.
Intraoperative Characteristics
The intraoperative characteristics of the studies are summarized in Appendix Table A1. Overall, 68.8% (445/646) of patients underwent LUCL reconstruction and 31.1% (201/646) of patients underwent LUCL repair. For the reconstruction procedure, the most common graft used was the triceps tendon autograft (342/445; 76.8%) followed by palmaris tendon autograft (72/445; 16.1%). The other grafts were gracilis tendon autograft (13/445; 2.9%), Achilles tendon allograft (6/445; 1.3%), hamstring tendon autograft (4/445; 0.89%), and flexor carpi radialis autograft (1/443; 0.22%). The most frequently used fixation type was transosseous fixation (197/646; 30.4%), followed by tenodesis screw (178/646; 27.5%), suture anchor (138/646; 21.2%), and suture tape (72/646; 11.1%). Examination under anesthesia (EUA) was performed in 33.7% of patients (218/646). The types of EUA performed were the pivot-shift test (168/218; 77%), posterior drawer test (56/218; 25.6%), and varus stress test (21/218; 9.6%). Arthroscopic examination for instability was performed in 75 patients (11.6%), with a positive result in 45.3% (34/75) of patients.
Postoperative Characteristics
The postoperative outcomes according to the study are detailed in Appendix Table A2, and the results of the subgroup analysis of LUCL repair (n = 201 patients) versus reconstruction (n = 445 patients) are shown in Table 3. The most common functional outcome tool used was the MEPS, with 15 studies including postoperative MEPS values. ‡‡ A total of 44 patients (21.8%) in the repair group and 254 patients (57%) in the reconstruction group reported excellent MEPS outcomes, and 32 patients (15.9%) in the repair group and 124 patients (27.8%) in the reconstruction group reported good outcomes. The remaining 5 patients reported fair outcomes, and 1 patient reported poor outcomes; all of these patients belonged to the reconstruction group. The mean MEPS was 91.58 ± 8.83 in the repair group and 89.8 ± 8.31 in the reconstruction group (Table 3). The VAS pain score was reported in 269 patients (41.6%), none of whom had a VAS score >3. The instability symptoms resolved in 592 patients (89.1%). Residual symptoms were observed in 28 patients (4.3%). The most common residual symptom exhibited was instability (18/28; 64.2%), followed by pain (11/28; 39.2%) and stiffness (5/28; 17.8%). Return to work or sport was reported in 8 studies,12,18,23,26,29,31,32,34 with times ranging from 7.7 to 52 weeks. Patient satisfaction was reported in 12 studies, §§ with 75 patients in the repair group and 212 patients in the reconstruction group satisfied with outcomes. The mean satisfaction rate was 94.40% ± 6.98% in the repair group and 93.69% ± 4.74% in the reconstruction group (Table 3).
Subgroup Analysis of LUCL Repair Versus Reconstruction Patients a
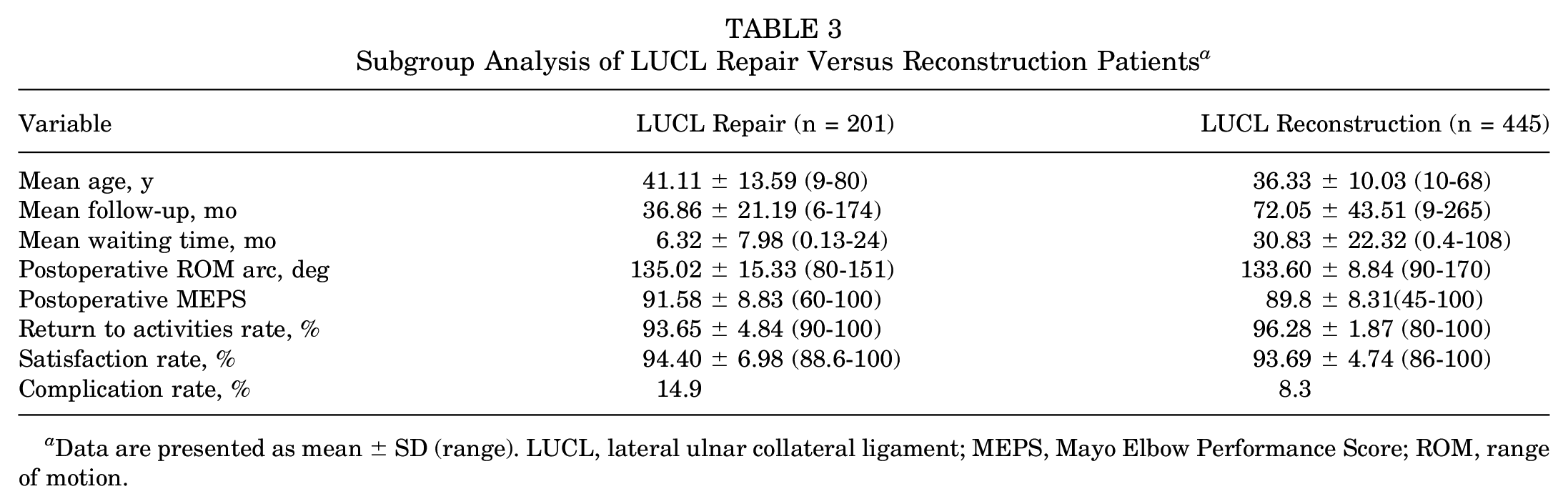
Data are presented as mean ± SD (range). LUCL, lateral ulnar collateral ligament; MEPS, Mayo Elbow Performance Score; ROM, range of motion.
Complications were observed in 54 patients (8.3%), with ulnar nerve event being the most common complication (2.3%). Postoperative complications were grouped into wound problems (1.8%)—including hematoma, wound infection, stitch abscess, pin-site irritation, and suture granuloma; ulnar nerve event (2.3%)—including persistent ulnar nerve symptoms, postoperative ulnar nerve injury, cubital tunnel syndrome, and ulnar nerve neuritis; joint problems (2.1%)—including contracture, heterotopic ossification, posttraumatic osteoarthritis, and arthrofibrosis; instability (1.8%)—including medial collateral ligament and flexor pronator tear, graft insufficiency, mild radiocapitellar opening, and reruptured ligament; and other (0.3%)—including deep vein thrombosis and nonunion. A comparison of complications between the reconstruction and repair groups is shown in Figure 3.
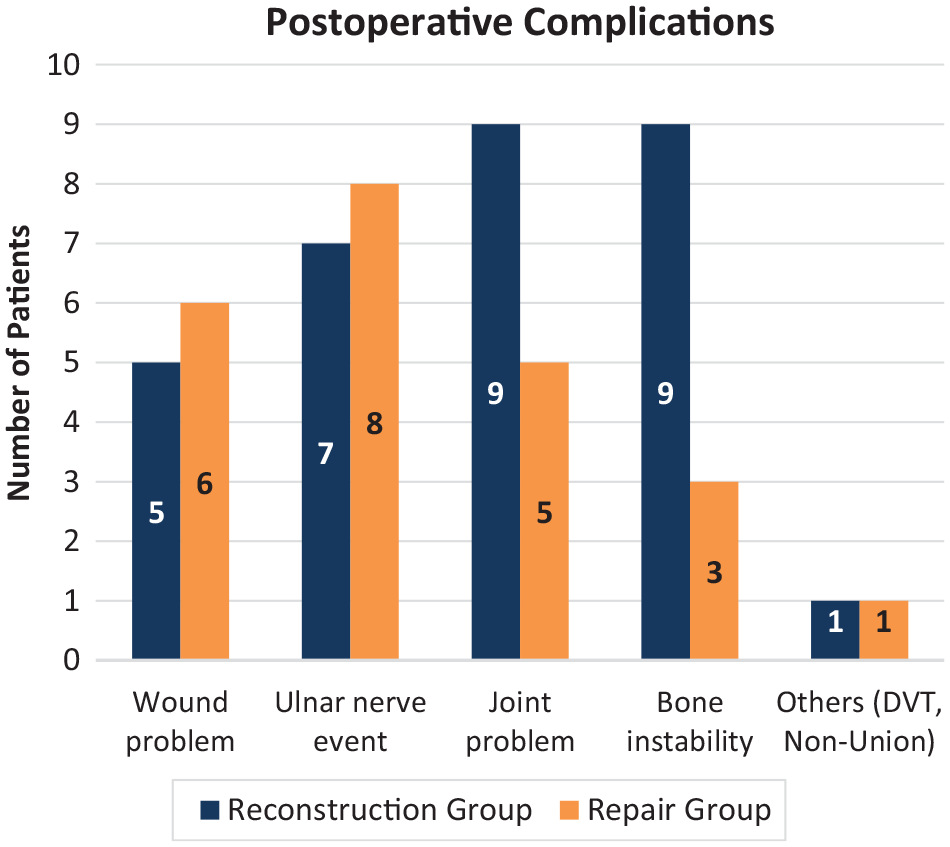
Postoperative complications after LUCL reconstruction versus LUCL repair. LUCL, lateral ulnar collateral ligament.
Functional Outcomes
Results of the meta-analysis of MEPS scores among 4 studies9,19,23,30 of LUCL repair and 11 studies
‖‖
of LUCL reconstruction indicated that the mean postoperative MEPS was significantly higher in the repair group (91.5 [95% CI, 86.8-96.2]; P = .016; I2 = 99.3%)
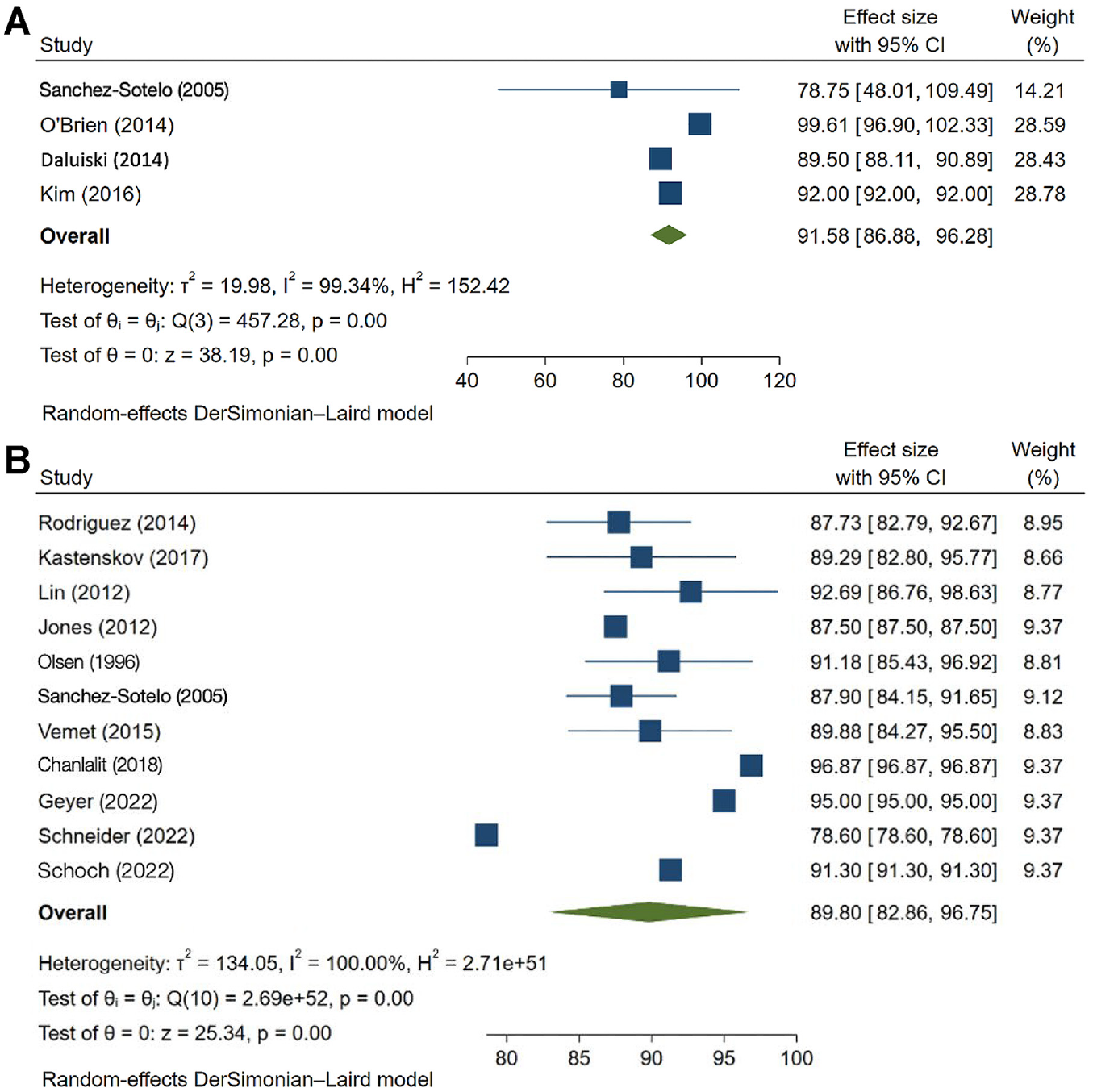
The MEPS of the (A) LUCL repair group and (B) LUCL reconstruction group. LUCL, lateral ulnar collateral ligament; MEMPS, Mayo Elbow Performance Score.
Discussion
This review and meta-analysis indicated that both LUCL repair and reconstruction surgery led to good to excellent patient-reported outcome scores. With regard to other outcome measures, LUCL reconstruction was shown to have a superior rate of return to activity and a lower complication rate compared with LUCL repair, while LUCL repair had higher postoperative functional outcomes and ROM arc.
In the acute traumatic setting, LUCL repair is an option if the soft tissues are amenable; however, given the frequent difficulty in diagnosis of PLRI, repair is often not feasible as the soft tissues are irreparable. Therefore, reconstruction of the lateral collateral ligament complex is the recommended choice to restore elbow stability in patients, especially in those with subacute to chronic PLRI. As reported by Sanchez-Sotelo et al, 31 reconstructions using a tendon graft provided better results than ligament repair, and the results did not appear to deteriorate with time, as satisfactory results were seen in 84% of patients after reconstruction.3,6,31
With regard to functional outcomes, the postoperative ROM arc and MEPS values were slightly higher in patients who underwent LUCL repair versus reconstruction (ROM: 135.02° vs 133.60°; MEPS: 90.14 vs 89.04). These results may be due to the longer waiting times in the reconstruction group (30.82 months vs 6.30 months in the repair group), since a longer time from diagnosis of PLRI to surgery will result in significant pain, dysfunction, and degenerative changes to the elbow. Concrete diagnosis of PLRI is often delayed since it requires a careful history of elbow trauma in combination with a focused physical examination as well as associated imaging. 33 Among the included studies, Lin et al 22 reported a mean time between injury and index surgery of 45 months, and Chanlalit and Dilokhuttakarn 4 reported that patients with atraumatic PLRI showed inferior results compared with patients with traumatic PLRI due to their longer waiting time.
Our findings are similar to a study by Fares et al, 10 which showed that despite the delayed diagnosis, surgical outcomes after LUCL reconstruction are generally excellent, with 90% of patients reporting a mean MEPS of 89.7 at a long-term follow-up. The rate of return to activities was marginally higher in the LUCL reconstruction group compared with the repair group. Vitale et al 35 showed that LUCL reconstruction was effective in returning athletes to sports, with a rate of return of approximately 80%. This finding was also supported by Hechtman et al, 13 who reported that out of 34 athletes, 29 athletes (85%) had an excellent result, defined as the ability to return to play at or above the preinjury level. Conway et al 5 also reported that only 50% of patients undergoing a direct repair returned to their previous level of sport compared with 68% of those undergoing a reconstruction. Even worse outcomes were seen in Major League Baseball players in the United States who underwent primary repair, with only 2 of 7 players being able to return to sports. 13
We cannot conclude from the available studies whether one procedure is superior to another because of the limited number of patients and the heterogeneity of the patient characteristics and mechanisms of injury. LUCL repair may be a viable surgical option in young athletes with acute injuries, as it has excellent outcomes and allows an earlier return to play compared to LUCL reconstruction. 29 Savoie et al, 31 included in this review, showed that the results of primary LUCL repair in patients with acute injury were excellent, with 93% (56/60) of patients returning to sporting activities within 6 months. However, LUCL reconstruction may be more beneficial in patients with subacute, chronic PLRI or in older patients who may have degenerative tissue.2,17
Limitations
The main strength of this study is that our meta-analysis compares the surgical outcome of LUCL reconstruction versus repair for PLRI, comprising 20 included studies from 4 major databases after a comprehensive literature search. However, this study does have limitations. The analysis demonstrated a lower quality of evidence. However. The heterogeneity of patient characteristics and various mechanisms of injury limited the comparison of the superiority of each technique. Also, many studies did not discuss postoperative rehabilitation, and they had incomplete data as it related to return to preoperative levels of activity. Future studies into the surgical treatment of PLRI with a higher level of evidence, similar patient characteristics, and chronicity of the condition are needed.
Conclusion
This study demonstrated that LUCL reconstruction showed a superior rate of return to activity and a lower complication rate compared with LUCL repair. The patient population and the time from injury to the procedure also contributed to the outcome among the patients. LUCL reconstruction also had a lower complication rate but the ROM among these groups was similar.
Footnotes
Appendix
Postoperative outcomes of the Included Studies a

| Quantitative Assessment | Quantitative Assessment | ||||||
|---|---|---|---|---|---|---|---|
| Study | Outcome Measures | Postop ROM arc, Deg | Resolution of Instability Symptom, n/Total | Recurrence/ |
Return to Work/Sport (Time) | Patient Satisfaction, n/Total (%) | Complications (n) |
| Chanlalit Chanlalit and Dilokhuttakarn 4 (2018) | • MEPS: 97.5 • DASH: 7.6 |
136.8 | 8/8 | — | NR | NR | None |
| Daluiski et al 6 (2014) | MEPS: 89.5 | 135 | 34/34 | — | NR | NR | Postoperative stiffness (1); wound breakdown (1); postoperative arthritis (1); ulnar nerve neuritis (1) |
| DeLaMora and Hausman 8 (2002) | NR | 125 | 5/5 | — | NR | NR | None |
| Eygendaal 9 (2004) | Broberg and Morrey score: excellent (6/12), good-excellent (5/12), good (1/12) | 150.4 | 11/12 | Persistent instability (1/12) | NR | NR | None |
| Geyer et al 11 (2022) | • MEPS: 95 • PREE: 15.8 • VAS pain: 1.4 • DASH: 11.8 |
137.9 | 29/31 | — | NR | 28/31 (90.4) | Wound infection (1); persistent ulnar nerve symptoms (2); elbow stiffness (1) |
| Greiner et al 12 (2019) | • MEPS: 92.4 • DASH: 27.5 • OES: 39.1 |
130 | 17/17 | — | 17/17 (52 wk) | NR | Heterotopic ossification (1) |
| Jones et al 16 (2012) | • MEPS: 87.5 • Nestor grading system: excellent (4/8), good (4/8) |
Full ROM | 6/8 | Occasional instability (2/8) | NR | 8/8 | None |
| Jung et al 17 (2019) | • MEPS: 85 • QuickDASH: 11.4 • NRS: 2 |
130 | 19/21 | Mild instability (2/21) | NR | NR | Stitch abscess (1) |
| Kastenskov et al 18 (2017) | • MEPS: 89 • VAS pain: 0 during rest, 3 during activity • OES: 45 |
136.4 | 18/18 | Mild pain during activity (6/18) | 18/18 | 16/18 | Posttraumatic osteoarthritis (5) |
| Kim et al 19 (2016) | • MEPS: 92 • Nestor grading system: excellent (11), good (2) |
141 | 13/13 | — | NR | NR | Pin site irritation (1); delayed union (1); mild widening of the radiocapitellar joint space (1) |
| Lee et al 20 (2003) | Nestor grading system: excellent 3/10, good 5/10, fair 2/10 | 128.5 | 10/10 | Stiffness (2/10) | NR | 10/10 (100) | Postoperative hematoma (1) |
| Lin et al 21 (2012) | • MEPS: 93.2 • Nestor grading system: excellent (10/14), good (3/14), fair (1/14) |
122.1 | 13/14 | Persistent instability (1/14) | NR | 13/14 (93) | MCL tear (1) |
| O’Brien and Savoie 23 (2014) | MEPS: 100 | 128.1 | 13/13 | — | 13/13 (7.7 wk) | 13/13 | Heterotopic ossification (1) |
| Olsen et al 26 (1996) | • MEPS: 92 • Modified Constant score: 89 |
136 | 18/18 | Moderate pain (5); loss of extension (2); loss of flexion (1) | 15/18 | 15/18 | Ulnar nerve paralysis (1); deficient triceps tendon graft (1) |
| Rodriguez et al 29 (2018) | • MEPS: excellent (9/23), good (10/23), fair (3/23), poor (1/23)* • VAS pain: 1.34 |
121 | 23/23 | — | 19/23 (19.5 wk) | 19/23 | Wound infection (1); cubital tunnel syndrome (3); contracture (1) |
| Sanchez-Sotelo et al 30 (2005) | Nestor grading system: excellent (18/37), good (10/37), fair (9/37) | 134.8 | 31/37 | Pain and recurrence of instability (6/37) | NR | 38/44 (86) | Wound infection (2); heterotopic ossification (1); ulnar nerve compression (2); deep vein thrombosis (1) |
| Savoie et al 31 (2008) | Andrews-Carson score: excellent (53/60), good (3/60), fair (3/60), poor (1/60) | NR | NR | NR | 58/60 (24 wk) | 51/60 (85) | Arthrofibrosis (1); ulnar nerve injury (6); wound infection (2); flexor pronator tear (2) |
| Schneider et al 32 (2022) | • MEPS: 78.6 • SEV: 78.9 • PRTEE: 21.5 • DASH: 20.4 |
NA | 72/72 | — | 72/72 (18.9 wk) | 67/72 | Heterotopic ossification (1); insufficient triceps tendon graft (5); suture granuloma (1) |
| Schoch et al 33 (2022) | • MEPS: 91.3 • VAS pain: 1.8 • OES: 46.5 |
131.3 | 178/178 | — | NR | NR | Ligament rerupture (2) |
| Vernet et al 34 (2015) | • VAS pain: 2.6 • MEPS: excellent (11/18), good (6/18), fair (1/19) b |
126.7 | 18/18 | — | 18/18 (14 wk) | 18/18 | None |
DASH, Disabilities of the Arm, Shoulder and Hand; MEPS, Mayo Elbow Performance Index; NR, not reported; NRS, Numeric Rating Scale; OES, Oxford Elbow Score; PREE, Patient-Rated Elbow Evaluation; preop, preoperative; ROM, range of motion; SEV, Subjective Elbow Value; VAS, visual analog scale.
MEPS scores were categorized as poor (<60), fair (60-74), good (75-89), or excellent (90-100).
Final revision submitted March 30, 2024; accepted April 12, 2024.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.