
Abstract
Background:
Women are underrepresented in academic positions, authorship roles, and award recognition within orthopaedic sports surgery. We aimed to determine the extent of this disparity within clinical trial leadership.
Hypothesis:
it was hypothesized that women would be significantly underrepresented as principal investigators (PIs) of clinical trials, but that this disparity would decrease over time.
Study Design:
Cross-sectional study.
Methods:
The Clinicaltrials.gov database was queried using Medical Subject Headings terms to identify studies regarding orthopaedic sports surgery. A variety of trial characteristics were recorded, including PI gender, trial phase, study design, date of posting, location, and enrollment. Our primary outcome was the proportion of women PIs compared between 2005 and 2025. Secondarily, we analyzed geographic distribution across world regions, countries, states, and the United States (US) Census regions, as well as trial characteristics (phase and intervention). Frequencies and percentages were used to demonstrate women's representation within each of these variables, and chi-square tests evaluated associations between trial characteristics and gender. Logistic regression was performed to assess trends in representation over time. A representation quotient was calculated comparing the proportion of women PIs with the proportion of women sports surgeons in the US.
Results:
Overall, 64 of 377 (17%) trials within our sample were led by women. The number of women-led clinical trials increased at a mean annual rate of 0.83% from 2005 (0/2; 0%) to 2025 (3/5; 60%); nonetheless, this change was insignificant (R2 = 0.13; P = .11). PI gender was not significantly associated with US census region (P = .15) but was significantly associated with world region (P < .001). Representation was lowest in North America (23/216; 10.6%) and South America (0/6; 0%). Among countries, Australia (1/1; 100%), Portugal (2/2; 100%), and Pakistan (4/5; 80%) had the greatest representation. Gender was also not significantly associated with study phase or study status. For trials involving procedures, women had a greater proportion of leadership roles (21/77; 27.2%) than the overall sample. A representation quotient comparing the proportion of women PIs (0.11) with the proportion of women orthopaedic sports surgeons (0.06) in the US was 1.79.
Conclusion:
A small proportion of orthopaedic sports medicine clinical trials are led by women. However, women may be overrepresented in leadership roles in clinical trials compared with their representation in orthopaedic sports medicine.
Despite growing awareness and institutional efforts to promote gender equity, women continue to be markedly underrepresented in orthopaedic surgery. While women now make up nearly half of the United States (US) medical school graduates, they account for only 8% of practicing orthopaedic surgeons and 18% of residents in the specialty.1,12 This disparity is even more pronounced in leadership roles, where barriers such as implicit bias, inadequate mentorship, and funding inequities continue to limit career advancement for women.2,5,8 Leadership of clinical trials—particularly in the role of principal investigator (PI)—is one marker of academic success, influencing promotion, tenure, and national visibility. 6 Thus, examining who occupies these roles offers insight into structural inequities that persist in orthopaedic research.
Recent studies have begun to quantify gender disparities across orthopaedic subspecialties. For example, previous studies have highlighted gender-based differences in income, award recognition, and professional advancement in academic societies, reflecting persistent structural challenges across the orthopaedic pipeline.2,5,8 Furthermore, a national analysis of orthopaedic clinical trials found that only 18% of trials were led by women, with striking variation by subspecialty and geographic location. 6 Women also accounted for just 1% of PIs in hip and knee arthroplasty trials, but nearly 27% in pediatric orthopaedic research. 16 Finally, women are also significantly less likely to be represented as head team physicians among National Collegiate Athletic Association sports teams or serve in leadership positions in orthopaedic sports societies globally.7,32 Sports medicine—an influential subspecialty in both clinical and public-facing orthopaedics—has yet to be studied in this context.
Therefore, this study aimed to evaluate gender representation among PIs of sports orthopaedic clinical trials. Specifically, we aimed to (1) assess the proportion of women serving as lead investigators over time, (2) analyze the geographic distribution of women PIs internationally and within the US, and (3) evaluate clinical trial characteristics associated with women's leadership. We hypothesized that women would be underrepresented in orthopaedic sports clinical trials but would show increasing representation over time, in line with trends observed in other orthopaedic subspecialties.6,16
Methods
Study Design
We conducted a cross-sectional survey of the ClinicalTrials.gov database on April 24, 2025, to identify clinical trials on sports-related orthopaedic surgery topics. We queried this database using the following Medical Subject Headings (MeSH) phrase: ("Orthopaedic Surgery" OR "Orthopaedic Procedures" OR "Orthopedic Surgery" OR "Orthopedic Procedures") AND ("Sports Injury" OR "Sports" OR "Sports Medicine"). Recorded information for each trial included PI name, study status, studied conditions, type of intervention, sponsor, collaborators, phases, enrollment, study design, date the trial was first posted, and associated locations. Clinical trial phases describe the steps in testing novel drugs or interventions, ranging from Phase 0, an exploratory study with limited human exposure, to Phase 4, trials involving long-term follow-up of large numbers of patients following US Food and Drug Administration (FDA) approval. 22
Inclusion and Exclusion Criteria
Our initial query of the Clinicaltrials.gov registry yielded 740 trials that met our MeSH search terms. Trials with a specific phase were included, along with those that listed not applicable, to ensure this analysis included trials studying devices, behavioral therapies, combination products, and procedures. Studies without a listed phase were excluded, and trials with no listed PI were excluded as well. Finally, we excluded trials with PI names that demonstrated an unsatisfactory gender prediction probability (Figure 1).
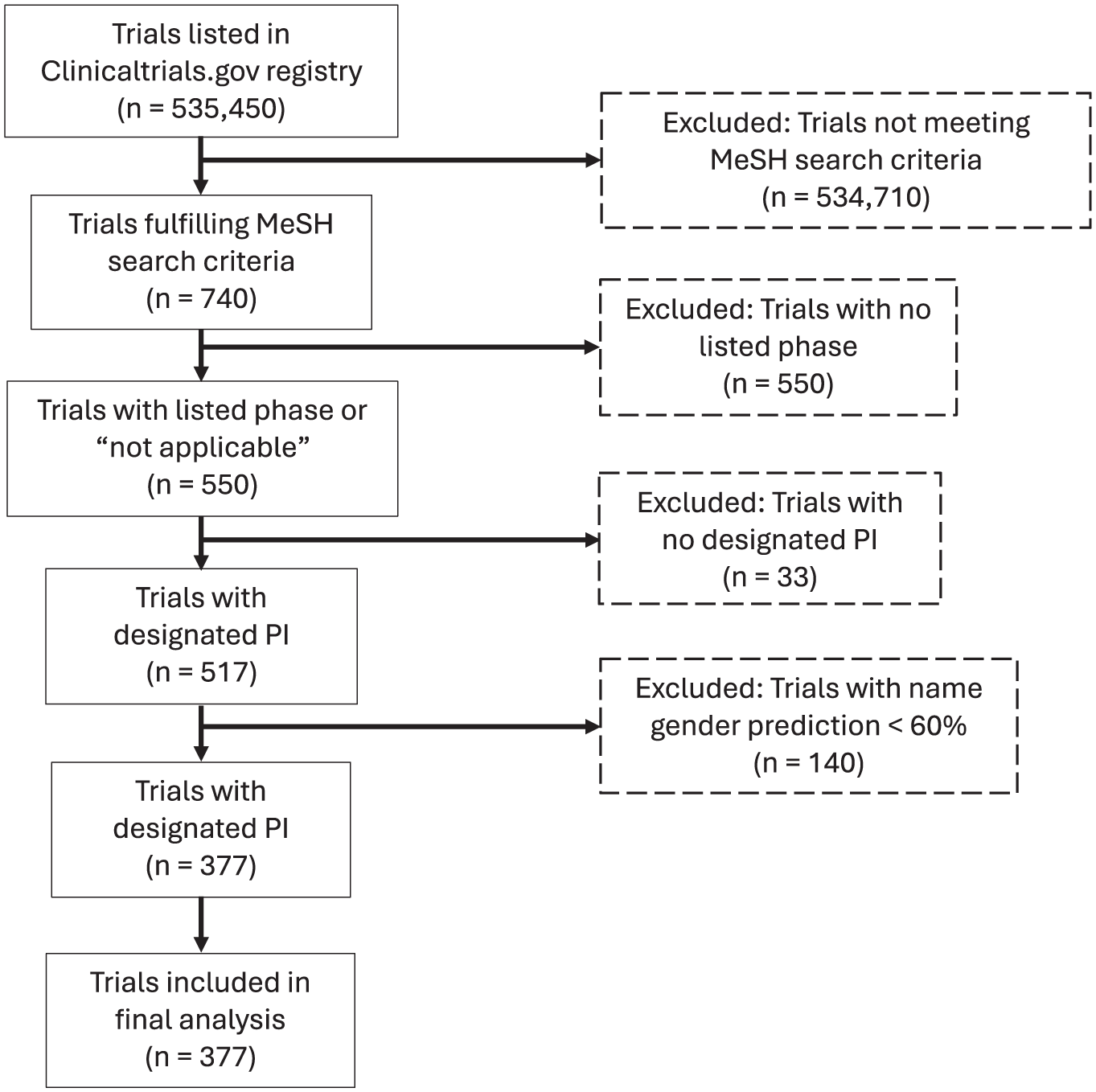
CONSORT flow diagram depicting trial selection process. CONSORT, Consolidated Standards of Reporting Trials; MeSH, Medical Subject Headings; PI, principal investigator.
Determination of Gender
After exporting a list of PI names from trials that fulfilled the described MeSH terms, first names for each PI were extracted. Similar to previous studies, we used Genderize.io. This previously used and validated application programming interface service predicts individuals’ genders based on a first name and provides a probability for each prediction.4,10,11,16,28 Similar to past studies, names with a gender prediction probability of <60% were excluded from this analysis, and gender was treated as binary (man or woman).
Data Collection
Our final list of trials was exported from Clinicaltrials.gov as an XML (extensible markup language) file and then converted to a Microsoft Excel Spreadsheet. These data were then imported into R (R Foundation for Statistical Computing) for statistical analysis. This query and data export were performed on April 23, 2025.
Primary and Secondary Outcomes
The primary outcome of interest for this study was how the proportion of women PIs has changed over time. Secondarily, we analyzed relative rates of representation based on continent, country, state, and US census region. We also aimed to determine whether PI gender was associated with the trial's study phase, status, or tested intervention. Finally, a representation quotient (RQ) was calculated to determine whether the proportion of women PIs was similar to that of women orthopaedic sports surgeons in the US.
To model how the proportion of studies with women PIs changed over time, we performed a logistic regression with the year each study was first posted to Clinicaltrials.gov as the independent variable and gender as a binary dependent variable. Descriptive analysis, including frequencies and percentages, was used to determine the proportion of women PIs leading studies in each continent, country, state, and US census region that met our search criteria. Color density heat maps were used to illustrate these proportions for countries (Figure 2) and states (Figure 3). Chi-square tests were used to determine whether gender was significantly associated with each trial's continent, US census region, study phase, status, and tested intervention. The RQ was calculated by comparing the proportion of women PIs with the proportion of women orthopaedic sports surgeons in the US. P values with P < .05 were considered significant. All statistical analyses and figure preparations were performed using R software Version 4.4.1 for macOS (R Foundation for Statistical Computing).
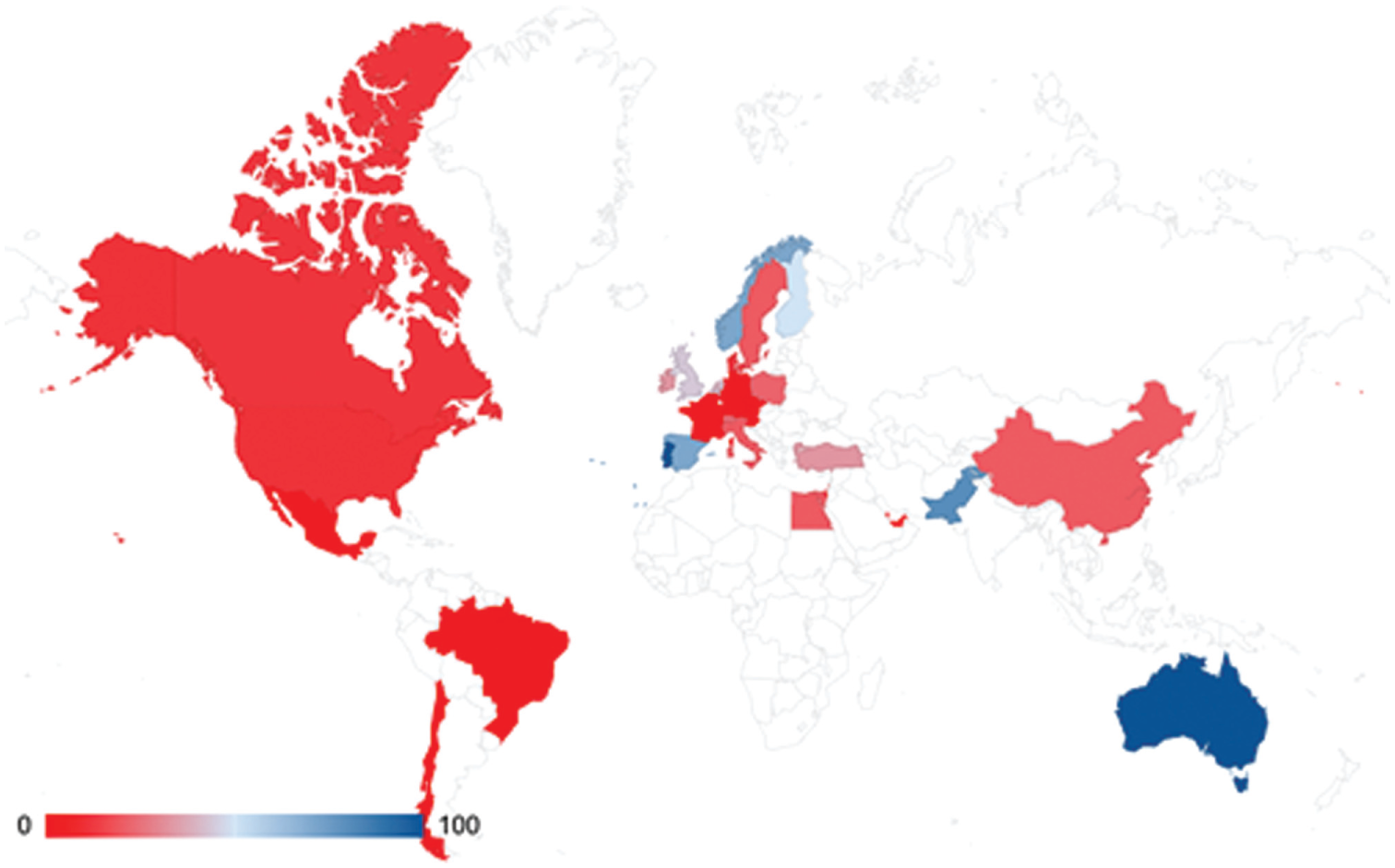
Heat map showing the relative representation of Women PIs by country. PI: principal investigator.

Heat map showing the relative representation of Women PIs by US state. PI: principal investigator.
Results
Changes in Representation Over Time
After applying the exclusion criteria, our sample comprised 377 clinical trials (Figure 1). Of 377 trials included in our study, 64 (17%) listed women as their PIs and 313 (83%) listed men. Logistic regression determined that the proportion of PIs who were women increased between 2005 and 2025 (R2 = 0.13; P = .11), with an annual increase of 0.83%; nonetheless, this was not statistically significant (Figure 4). The years with the smallest proportion of women were 2005 (0/2; 0%), 2006 (0/6; 0%), and 2013 (0/16; 0%) (Table 1). The years with the greatest proportions were 2025 (3/5; 60%) and 2010 (3/7; 42.9%).

Trends in the proportion of women PIs over time. PI, principal investigator.
Number of Women-Led Trials by Year a

PIs, principal investigators.
Data from 2025 reflect trials reported through April 23.
Geographic Trends
The majority of trials within our sample came from North America (216/377; 57.9%). A considerable proportion were listed in Europe (109/377; 28.9%) and Asia (27/377; 7.2%), with Africa, Australia, and South America each representing <2% of trials. Studies with no listed location (14/377; 3.7%) were categorized as Unlisted. Those found within US census regions were primarily listed in the South (63/177; 35.6%), followed by the West (46/177; 26%), the Midwest (41/177; 23.2%), and the Northeast (27; 18.8%). Most trials listed Not applicable for the study phase (303/377; 80.4%).
Representation of women PIs was greatest in Australia (1/1; 100%). However, this region listed only 1 trial. Among world regions with multiple trials, representation was comparable among Africa (1/4; 25%), Europe (29/109; 26.6%), and Asia (8/27; 29.6%). North America (23/216; 10.6%) and South America (0/6; 0%) demonstrated the lowest proportions. Differences in representation among specific countries are shown in Figure 2.
There was a significant relationship between PI gender and world region (Table 2). Proportions compared with the overall sample were notably greater in Europe (29/377; 7.7%), North America (23/377; 6.1%), and Asia (8/377; 2.1%) than Africa (1/377; 0.3%), Australia (1/377; 0.3%), and South America (0/377; 0%).
Characteristics of Analyzed Clinical Trials

PI gender was not significantly associated with US census region (P = .15) (Table 2). Differences in representation among individual states are demonstrated in Figure 3. The RQ comparing the proportion of women PIs (0.11) with the proportion of women orthopaedic sports surgeons (0.06) in the US was 1.79. This reference value for the proportion of women surgeons was taken from a systematic review 21 of 13 studies analyzing demographic diversity in orthopaedic sports medicine between 2010 and 2023.
Trial Characteristics
For those with a described phase, Phase 4 was the most common (26/377; 6.9%). The most prevalent trial status and intervention were Completed (163/377; 43.2%) and Device (94/377, 25%), respectively.
PI gender was not significantly associated with study phase (P = .11); however, women were represented only in Phase 2 (1/11; 9.1%), Phase 4 (2/26; 7.7%), and Not Applicable studies (61/303; 20.1%). There was also no significant association between PI gender and study status. PI gender was significantly associated with intervention type (P < .001). The most prevalent form of intervention was Procedure (21/77; 27.3%); and Biological, Combination Product, Diagnostic Test, and Dietary Supplement interventions had no women PIs.
Discussion
Women physicians in academic medicine have historically been underrepresented in leadership positions, promotions, and several specialties.16,26,27,31 This phenomenon is particularly evident in orthopaedic surgery, as women comprise only 8% of orthopaedic surgeons and 18% of trainees.1,12 Similarly, only 12.1% of orthopaedic sports fellows are women. 9 Because clinical trial leadership serves as a metric for professional progression and development, our study aimed to use women's representation among PIs to measure equity within orthopaedic sports medicine. We found that the proportion of women PIs between 2005 and 2025 did not increase significantly, despite a slight upward trend. Gender was significantly associated with world region but not with the US Census region. It was also significantly associated with the studied intervention but not the study phase or study status. However, the RQ determined that women may be overrepresented as PIs in relation to their overall representation as sports orthopaedic surgeons. Although representation increased over the course of the study period, our results indicate a significant need for improved women’s representation internationally and in multiple classifications of clinical trials.
Changes in Representation Over Time
Our results showed that the number of women leading clinical trials increased slightly over time, but this increase was not statistically significant. This proportion began at 0% in 2005 and peaked at 60% in 2025. While these figures are encouraging, our results are limited by year-to-year variability and the relatively small sample size of trials within the subspecialty compared with orthopaedics as a whole. For example, Burkhart et al 6 found that the proportion of women leading clinical trials in orthopaedics overall increased significantly from 13% (16/121) in 2007 to 22% (53/242) in 2022. However, a similar study of participation in trials concerning hip and knee arthroplasty also found that women were statistically underrepresented. 30
Other areas of academic sports medicine also reflect persistent disparities. Potter et al 24 found that women’s representation among moderators and course instructors at the AOSSM annual meeting increased marginally from 6.3% in 2015 to 7.7% in 2019. Kim et al 17 demonstrated that, while disparities have decreased since 1972, women still average fewer publications and are significantly less likely to be assigned lead authorship, despite being associated with higher levels of evidence. Women orthopaedic surgeons surpassed men in median funding per grant in 2015, and this relationship became statistically significant 11 in 2020. However, men received the majority of grants during the study period. 11 This also demonstrates that, while representation has improved over time, greater emphasis on promoting women's representation in clinical research is still necessary.
The annual increase in representation among other specialties is also greater than in our own sample. Jou et al 15 demonstrated that women's representation as a PI increased by 3% annually between 2010 and 2020 in a sample of 200 clinical trials. Lattanza et al 19 found that this figure increased by 1.2% annually in oncology clinical trials, and this increase was significant. Finally, the proportion of women PIs has doubled from 7.6% to 15.7% between the intervals 1998-2013 and 2014-2023 in vascular surgery. These findings reinforce particularly glaring disparities among trials studying orthopaedic surgery and its subfields.
Thus, there is a clear need for initiatives that support women's participation and advancement in orthopaedic sports surgery. One key barrier for women is exposure, especially during medical school and training.3,13,14 Organizations specifically geared toward the inclusion of women, such as the Ruth Jackson Orthopaedic Society and the Perry Initiative, offer outreach programs for medical students to provide exposure and mentorship.20,29 In addition to improving the pipeline for women into sports surgery, better support for women within the field is necessary. Improved promotion within academic leadership positions and greater award recognition are 2 possible ways to support women in academia. Greater direct investment in trials and studies led by women would also likely decrease these disparities. 11
Geographic Disparities
The proportion of women PIs was comparable among world regions. However, North and South America demonstrated lower rates than Africa, Asia, and Europe. This is generally inconsistent with previous studies on the geographic distribution of women PIs. For example, Burkhart et al 6 found that women trial leaders were most prevalent in Asia and South America. Jou et al 15 found that women were 1.78 times more likely to be represented in obstetric or gynecological trials conducted outside Asia; however, this disparity was not observed in our own sample. Among oncology clinical trials, Waldhorn et al 33 reported the greatest representation of women PIs in North America, with Denmark, France, and Sweden also exhibiting high rates. 33 This lack of consistency among specialties and even within orthopaedic subspecialties suggests that there is a need for improvement in representation, which is an international concern.
Rates of women PIs were comparable in the South and Northeast but were considerably lower in the West and Midwest. This is surprising given that Kocjan et al 18 also found that the annual percentage of orthopaedic sports surgeons was lowest in the South (7.2%) compared with the West (10.4%), Midwest (14.2%), and Northeast (14.7%). 18 Regardless, our results demonstrate that disparities between men and women within trial leadership are universal, and broader initiatives are necessary to improve representation internationally. While certain countries may exhibit relatively higher rates of representation, these trends are not consistent across world regions or states, suggesting that improvements are needed internationally and nationwide.
Our RQ determined that women PIs in the US may be overrepresented in the leadership of clinical trials in comparison to the overall proportion of women orthopaedic sports surgeons. This may indicate that, despite the general underrepresentation of women surgeons in the US, disparities in clinical trial leadership are in fact less severe. However, this relationship may be obscured because our sample is significantly smaller than the systematic review that provided our reference for the proportion of women among sports surgeons overall. Moreover, limited data are available on international representation; thus, our RQ focuses only on the US.
Strategies for Improvement
Several strategies have been implemented to decrease the disparities described in our results. While few have described methods to improve the representation of women in clinical trials, multiple studies offer strategies that support inclusion in academic positions and societies. Ramos et al 25 note the importance of representation in leadership positions within orthopaedic societies, demonstrating a positive correlation between the number of female members and the number of women on the Board of Directors at the regional and state levels. Pipeline initiatives, such as the Perry initiative, often support these. Mason et al 23 found that women who completed Nth dimension's Orthopaedics Summer Internship had increased odds of applying to an orthopaedics residency. Thus, in addition to increased representation at the faculty level, grassroots initiatives also help reduce these disparities.
Limitations
This study has several limitations that should be considered when interpreting our findings. First, Clinicaltrials.gov does not require registration for trials conducted exclusively outside the US, trials without US enrollment, or studies that do not involve FDA-regulated interventions. Thus, our analysis may underrepresent trials conducted internationally or those initiated through investigator-driven efforts, limiting the generalizability of our findings. The MeSH terms and the exclusion criteria used to identify the trials in this study also yielded a relatively small sample. In particular, excluding studies with incomplete information on Clinicaltrials.gov, including PI name and location, significantly reduced the size of our sample. Future studies may aim to utilize a wider array of terms or more lenient exclusion criteria to offer a broader analysis.
Gender prediction algorithms like Genderize.io may also misclassify individuals, particularly those with uncommon, unisex, or culturally diverse names. To mitigate misclassification, we excluded names with a probability prediction below 60%. This approach did not allow us to capture PIs who identify as nonbinary, transgender, or otherwise outside of the traditional gender binary. While some degree of misclassification is likely, previous studies of women’s representation that used Genderize.io have shown that it is unlikely to have a significant effect on our results.4,10,11,16,28 Because of the observational nature of this analysis, we can only describe associations and cannot infer causality. Finally, years with the largest and smallest percentage of women PIs often had the lowest numbers of total studies. Thus, these extremes may be attributable to statistical variance. Future studies may aim to determine whether these disparities extend to participants found in these trials, comparing the proportion of men and women subjects in studies of men and women PIs.
Conclusion
This study highlights the ongoing underrepresentation of women as PIs of sports orthopaedic clinical trials. Although we observed modest improvement, women are still underrepresented as PIs relative to their overall representation as orthopaedic sports surgeons, and they continue to hold a small minority of PI roles in clinical trials. It is critical to foster early exposure of women to orthopaedic sports medicine through medical school outreach programs, research opportunities, and mentorship initiatives within residency. Additionally, increasing access to research funding explicitly targeted to women PIs and promoting unbiased selection processes for leadership roles are essential steps. Institutional efforts to recognize and address implicit biases and to celebrate the contributions of women in orthopaedic research will also be vital for achieving sustained progress.
Footnotes
Final revision submitted September 14, 2025; accepted September 18, 2025.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought because the study was considered exempt from institutional review board review, as it used publicly available data.