
Abstract
Background:
Hamstring injuries have a high incidence of reinjury. However, the risk factors for reinjury remain unknown.
Purposes:
To investigate the incidence of hamstring injuries in male Japanese professional football (soccer) players and identify the risk factors for reinjury.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A total of 209 Japanese professional football players were included in this study. The authors investigated the overall number, incidence, affected muscles, and locations of both hamstring injuries and reinjuries. In addition, age, history of injury, affected muscle, type of injury, time of occurrence in the season, and intramuscular tendon injury were compared between players with and without reinjury (t test, Fisher exact test, and Bonferroni analysis).
Results:
Overall, there were 43 hamstring muscle injuries (HMIs) in 27 players. The mean incidence of injury was 0.60 (/1000 player-hours), including 2.30 (/1000 player-hours) in games and 0.35 (/1000 player-hours) during training. Among 40 legs that were treated nonoperatively, 12 developed reinjury. The reinjured muscles included the biceps femoris (BF; 9/27), semitendinosus (2/6), and semimembranosus (1/7). The locations of reinjury included the proximal third (3/13), middle third (4/17), and distal third (5/10). There was no significant difference between the reinjury and no-reinjury groups in terms of the evaluated items. However, in BF injuries, the type of injury was significantly associated with the incidence of reinjury. The rate of BF injury recurrence according to injury type was 0% (0/9) for type 1-M injuries, 67% (6/9) for type 1-T injuries, and 33% (3/9) for type 2 injuries (P = .0127).
Conclusion:
This study demonstrated that the overall incidence of HMI in male Japanese professional football players was 0.60 (/1000 player-hours), including 2.30 (/1000 player-hours) in games and 0.35 (/1000 player-hours) during training. The rate of recurrence was 30%. In the BF, the injury type classified on magnetic resource imaging was the only factor associated with recurrence. Bleeding around the intramuscular tendon without structural tendon injury was an important factor for predicting the recurrence of BF injuries. Type 1-T injuries should be managed differently from type 1-M injuries.
Hamstring muscle injury (HMI) frequently occurs in elite football (soccer) players and may result in a prolonged absence from play. 10 There has been several reports on prevention programs to reduce the incidence of HMI.1,4,8,23 However, in European professional football players, HMI has been reported to account for 12% to 24% of all injuries, representing the most common subtype of injury.9-11 The incidence of acute HMI has been reported to vary from 0.3 to 4.99 (/1000 player-hours [ph]).8,9,16,19 In addition, HMI is well known to be associated with a high risk of reinjury. The incidence of hamstring reinjury has been reported to range from 14% to 40%.8,11,18,20,23,24,27,32
The diagnosis and classification of muscular injuries are based on both clinical and magnetic resource imaging (MRI) findings, which are used to determine the prognosis and lay-off times.6,14,26,28 The severity and location of the tear are important factors to consider in the prognosis. Studies have reported that intramuscular tendon injuries require a longer period for a return to complete play (RTP) and carry a higher risk of recurrence in comparison with hamstring injuries without tendon involvement.2,3,5,20,23,24,27,31 However, it is important to note that these studies included participants from diverse age groups and sporting events. To our knowledge, there are no reports on the incidence and recurrence of HMI in professional football players in Japan. The risk factors for recurrence of HMI in professional football players remain unknown. The aim of this study was to investigate the incidence of HMI and identify the risk factors for reinjury in male Japanese professional football players. We hypothesized that the risk factor for reinjury depends on the classification according to the baseline MRI study.
Methods
Ethical Considerations
This study was approved by the Ethics Committee of our institution (No. 36-232). Informed consent was waived because of the retrospective nature of the study.
Player Characteristics
This was a retrospective study of HMI in a male Japanese professional football team that belonged to a Japanese professional football association (J.League). The study was conducted over 6 consecutive seasons from 2013 to 2018. The total number of players in this period was 209 player-seasons. These players were included in this study. Their mean age at the beginning of the season was 24.7 ± 1.3 years. The team belonged to division 1 for 4 years and division 2 for 2 years. Team practice usually started in the middle of January and ended at the beginning of December. The mean number of regular matches per year was 45.6 ± 3.4. The exposure time over 6 year-seasons of training was 62,594 hours (mean, 10,432 hours per year-season), while the exposure time in games was 9148 hours (mean, 1525 hours per year-season). Thus, the total exposure time was 71,742 hours (mean, 11,957 hours per year-season). The mean follow-up period for each HMI was 18.7 ± 16.6 months, and that of the entire cohort was 28.8 ± 22.8 months. HMI was defined as a positive tenderness corresponding with increased signal intensity on fluid-sensitive sequences of MRI performed within 48 hours after onset, which resulted in the player being absent from team training for ≥4 days. Hamstring contusion, which was defined as direct muscle injury, was not included in this study.
MRI Classification
All players with HMI were examined by MRI using a 3.0-T system (SIGNA Pioneer; GE HealthCare). The obtained sequences and detailed parameters are shown in Table 1.
Routine Sequences and Detailed MRI Parameters Used to Evaluate Hamstring Muscle Injuries a

FA, flip angle; FOV, field of view; IDEAL, iterative decomposition of water and fat with echo asymmetry and least-squares estimation; NEX, number of excitations; SLT, slice thickness; TE, echo time; TR, repetition time.
The club doctor diagnosed HMI on the same day and provided a classification of the injury. The type of HMI was defined based on coronal, sagittal, and axial MRI slices. We modified the Japan Institute of Sports Sciences (JISS) classification 21 as follows: type 1–muscle (type 1-M), myofascial injury in the peripheral aspect of the muscle and muscle belly; type 1–tendon (type 1-T), bleeding around the intramuscular tendon without structural tendon injury (Figure 1); type 2, injury at the muscle-tendon junction or involving the intramuscular tendon; and type 3, injury at the bone-tendon junction (Table 2). The anatomic site of the injury (proximal, middle, or distal third) was also recorded using sagittal and coronal MRI scans.

T2-weighted IDEAL (iterative decomposition of water and fat with echo asymmetry and least-squares estimation) MRI scans of a right hamstring muscle injury in a 26-year-old player. (a) Oblique coronal view. (b) Oblique sagittal view. (c) Oblique axial view. Bleeding was seen in the middle third of the biceps femoris. A high signal intensity area was observed in the intramuscular tendon even though the intramuscular tendon was intact (arrows), indicating a type 1-T injury.

JISS, Japan Institute of Sports Sciences.
The inter- and intraobserver agreements of the MRI classification were evaluated by calculating kappa coefficients for assessments in 20 randomly selected players. The interobserver agreement was evaluated by 3 examiners (T.O., H.F., and D.K.), and the intraobserver agreement was evaluated by a single examiner (H.F.) by performing image data assessment twice with 2 months between the 2 assessments. The inter- and intraobserver agreement measures (kappa coefficients) were 0.85 and 0.86, respectively. Both inter- and intraobserver reliability calculations demonstrated high levels of agreement (<0.00; poor, 0.00-0.20; slight, 0.21-0.40; fair, 0.41-0.60; moderate, 0.61-0.80; substantial, >0.80; almost perfect). 15
Rehabilitation Program
In all cases of HMI, the type of injury was diagnosed, and a rehabilitation program was planned according to the classification. The planned periods from injury to RTP were as follows: type 1 (1-M and 1-T), 2 weeks; type 2, 6-10 weeks; and type 3, 3 months (if surgery was performed, this was taken into consideration in determining the timing of the player's RTP). All injured athletes underwent the same rehabilitation regimen with the same team physical therapist during the 6-year study period. For type 2 and 3 injuries, running at >80% of the player's maximum speed was allowed after conformation of tendon thickening on follow-up MRI. The time for the maximum sprint of 50 m, measured in the off-season, was used as a reference for this rehabilitation. The criteria for RTP required players to have >90% muscle strength in knee bending relative to the opposite side, in both the fully extended and shortened positions during isometric and isokinetic contractions. Additionally, they had to be able to sprint at full speed without experiencing pain or soreness. Recurrence was defined as a subsequent injury that occurred at the same location as the previous injury, and which occurred before RTP or within 2 months after RTP.
Evaluation Items of Primary and Subsequent Hamstring Injury
A retrospective review of the players with HMI was conducted. The following items were analyzed: day of onset, age at injury, overall number of injuries, incidence of injury (/1000 ph), past history of HMI (injured on the same side >2 months prior), situation in which the injury occurred (during training or game), affected muscle (biceps femoris [BF], semitendinosus [ST], or semimembranosus [SM]), location, time of occurrence in the season, rehabilitation program, time to RTP, and MRI classification. The information on past history was obtained from “Health mate,” which is distributed by J.League and includes the medical records of each player.
A retrospective review of the players with recurrent HMI was also conducted. The following factors were analyzed: total number of recurrences, incidence of recurrence, time of onset of the recurrence, affected muscle, location, relationship between the affected muscle and the location, MRI classification, and incidence of recurrence according to injury type and muscle.
Statistical Analysis
The following factors were compared between players with and without reinjury: age, past history of HMI, affected muscle, time of occurrence in the season, and type of injury. In addition, for each muscle injury, statistical analysis was performed to compare the following factors between the 2 groups: age, past history of HMI, time of occurrence in the season, and type of injury.
All analyses were performed using EZR with R commander (Version 1.54). Descriptive statistics were used to describe the characteristics of muscles with reinjury. Univariate analysis of the patients with and without reinjury was conducted using the t test and Fisher exact test. When a statistically significant difference between the 2 groups was identified, Bonferroni analysis was used to determine whether it was a risk factor for recurrence. The mean and standard deviation were calculated for descriptive purposes. P values <.05 were considered to indicate statistical significance.
Results
HMI in 6 Seasons
In 6 seasons, there were 43 HMIs in 27 players. The mean age of the players at injury was 27.1 ± 4.5 years. There were 22 players who experienced an injury during training, and 21 who experienced an injury during a game. The total incidence of HMI was 0.60 ph, including 2.30 ph in games and 0.35 ph during training (Table 3).
Characteristics of Players and Hamstring Muscle Injuries Each Year a

Data are presented as mean ± SD or n (%) unless otherwise indicated. ph, /1000 player-hours.
The injured muscles included the BF (n = 29), ST (n = 6), and SM (n = 8). The locations of injury were as follows: the proximal third (16 legs; BF, n = 12; ST, n = 0; SM, n = 4), the middle third (17 legs; BF, n = 10; ST, n = 4; SM, n = 3), and the distal third (10 legs; BF, n = 7; ST, n = 2; SM, n = 1). According to our modified JISS classification, there were 15 legs with type 1-M HMI (BF, n = 9; ST, n = 3; SM, n = 3), 13 legs with type 1-T HMI (BF, n = 9; ST, n = 3; SM, n = 1), 9 legs with type 2 HMI (BF, n = 9; ST, n = 0; SM, n = 0), and 6 legs with type 3 HMI (BF, n = 2; ST, n = 0; SM, n = 4). Among the 13 legs with type 1-T injuries, there was 1 leg with a proximal third injury, 9 legs with middle third injuries, and 3 legs with distal third injuries (Table 4).
Characteristics of Hamstring Muscle Injuries a
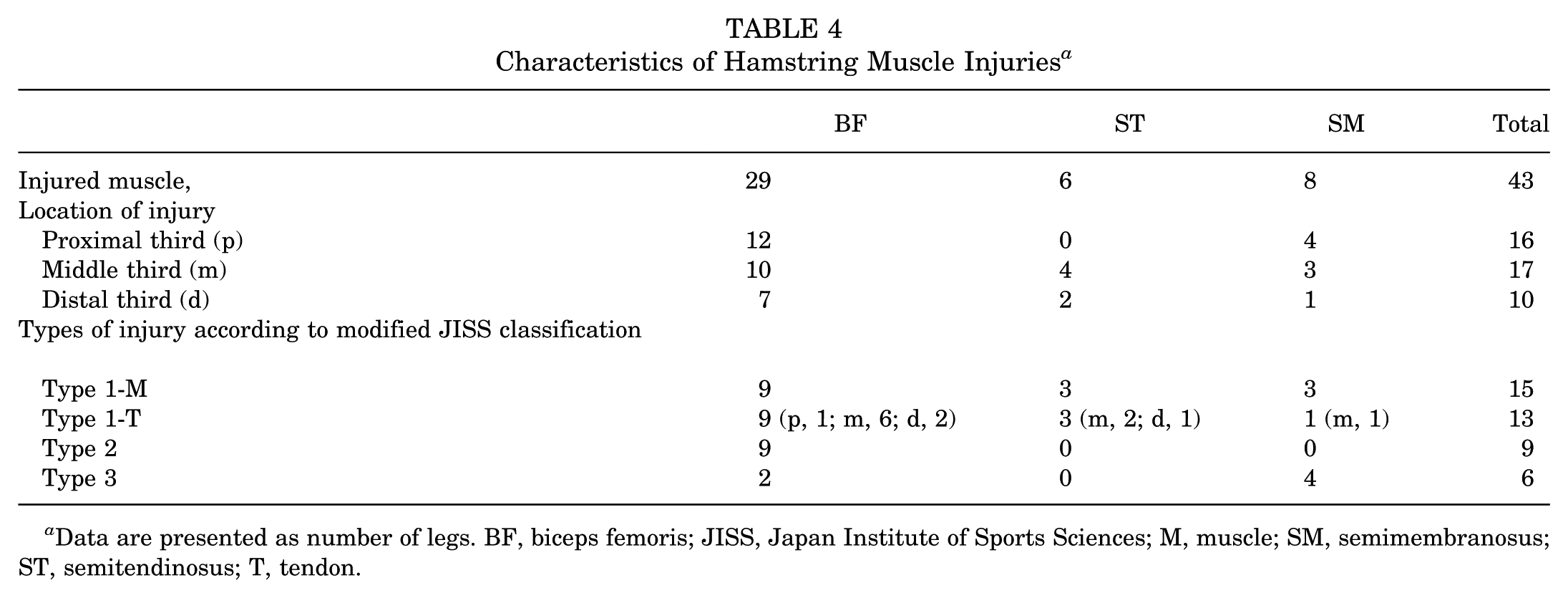
Data are presented as number of legs. BF, biceps femoris; JISS, Japan Institute of Sports Sciences; M, muscle; SM, semimembranosus; ST, semitendinosus; T, tendon.
The time of injury was as follows: January to February (n = 8), March to May (n = 11), June to August (n = 16), and August to December (n = 8). There were 18 players with a history of HMI on the same side.
Reinjury
Three of 6 legs with type 3 HMI (BF, n = 2; SM, n = 1) surgically treated. Thus, the remaining 40 legs were treated nonoperatively. Two legs (type 1-T [ST, n = 1] and type 2 [BF, n = 1]) developed reinjury before RTP. The remaining 38 cases returned to complete play after the rehabilitation program. A total of 12 legs developed reinjury. The timing of reinjury after RTP was as follows: within 1 week after RTP (n = 5), 1 to 4 weeks after RTP (n = 2), and 4 to 8 weeks after RTP (n = 3). The reinjury rate was 30% (12/40). The time of occurrence in the season was as follows: January to February (n = 2), March to May (n = 6), June to August (n = 3), and August to December (n = 1).
Reinjury occurred to the BF in 9 of 27 legs (33%), ST in 2 of 6 legs (33%), and SM in 1 of 7 legs (14%). Reinjury occurred in the proximal third portion in 3 of 13 legs (23%), middle third portion in 4 of 17 legs (24%), and distal third portion in 5 of 10 legs (50%). In the BF, the incidence of reinjury was 33% (3/10) in the proximal third portion, 40% (4/10) in the middle third portion, and 29% (2/7) in the distal third portion. In the ST, the incidence of reinjury was 0% (0/4) in the middle third portion and 100% (2/2) in the distal third portion. In the SM, the incidence of reinjury was 0% (0/3) in both the proximal and middle third portions and 100% (1/1) in the distal third portion. All 7 legs in which reinjury occurred in the proximal and middle third portions had BF injuries. The 5 legs in which reinjury occurred in the distal third portion included 2 of 7 legs with BF injuries, 2 of 2 legs with ST injuries, and 1 of 1 leg with an SM reinjury. The classifications of recurrent injuries were as follows: type 1-M, 2 legs (of 15); type 1-T, 7 legs (of 13), and type 2, 3 legs (of 9).
The incidence of recurrence was determined according to injury type and muscle. Type 1-M, 1-T, and 2 injuries accounted for 0% (0/9), 67% (6/9), and 33% (3/9) of injuries in the BF. Type 1-M and type 1-T injuries accounted for 33% (1/3) and 33% (1/3) of the injuries in the ST. Type 1-M, 1-T, and 3 reinjuries accounted for 33% (1/3), 0% (0/1), and 0% (0/3) of the reinjuries in the SM (Table 5).
Characteristics of Hamstring Muscle Reinjury a
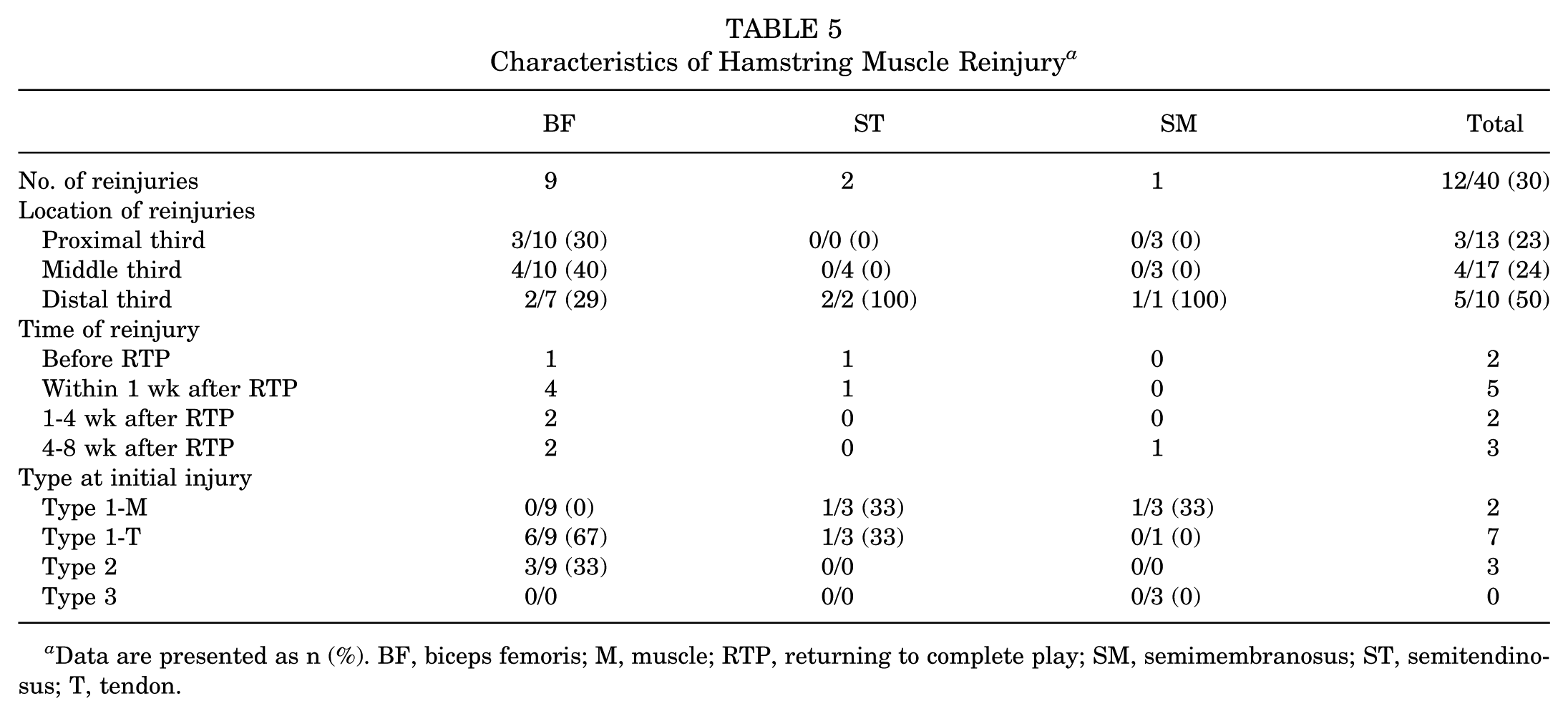
Data are presented as n (%). BF, biceps femoris; M, muscle; RTP, returning to complete play; SM, semimembranosus; ST, semitendinosus; T, tendon.
Statistical Analysis
There were no significant differences between the reinjury (n = 12) and no-reinjury (n = 28) groups with respect to age (P = .23), history of past injury (P = .73), injured muscle (P = .76), location of injury (P = .31), time of occurrence in the season (P = .16), and type of injury (P = .097) (Table 6).
Comparison of Parameters in the Reinjury and No-Reinjury Groups a

Data are presented as number unless otherwise indicated. BF, biceps femoris; HMI, hamstring muscle injury; M, muscle; SM, semimembranosus; ST, semitendinosus; T, tendon.
For injuries of the BF, a statistically significant difference was observed regarding the type of injury. Reinjury occurred in 0 of 9 type 1-M injuries, 6 of 9 type 1-T injuries, and 3 of 9 type 2 injuries (P = .0127). Furthermore, there was a significant difference in the incidence of recurrence of type 1-M and type 1-T injuries (P = .027). Although the result did not reach statistical significance, BF reinjury tended to develop at the start of the season (P = .068), and ST reinjury tended to develop at the distal third portion (P = .066) (Table 7).
Comparison of Items Evaluated in Each Muscle in the Reinjury and No-Reinjury Groups a

Data are presented as number unless otherwise indicated. Boldface type indicates statistical significance. BF, biceps femoris; HMI, hamstring muscle injury; M, muscle; SM, semimembranosus; ST, semitendinosus; T, tendon.
Discussion
The major findings in this study demonstrated that the overall incidence of HMI in male Japanese professional football players was 0.60 ph, including 2.30 ph in games and 0.35 ph during training. The rate of recurrence was 30%. In the BF, the injury type classified on MRI was the only factor associated with recurrence. Reinjury occurred in 0 of 9 type 1-M injuries, 6 of 9 type 1-T, and 3 of 9 type 2 injuries (P = .0127). In the BF, type 1-T injuries had a significantly higher incidence of recurrence compared with type 1-M injuries, although all players with type 1 (both 1-M and 1-T) injuries were able to RTP within 2 weeks.
This is the first report, to our knowledge, on the incidence of injury and reinjury of the hamstring muscle in male Japanese professional football players undergoing the same rehabilitation program overseen by the same physical therapist and with the same criteria for RTP based on the classification according to the baseline MRI study.
Ekstrand et al9,11 reported that the incidence of HMI in the Union of European Football Association (UEFA) was 4.99/1000 ph in games and 0.52/1000 ph in training. In our study on the J.League, the incidence was 2.30/1000 ph in games and 0.35/1000 ph in training, which was lower than the incidence in UEFA, especially in games. The definition of HMI and the number of official matches may have contributed to these differences. Ekstrand et al 11 defined HMI as an injury that compels players to lay off for >1 day, while our study defined HMI as an injury that compels players to lay off for >4 days. Moreover, the number of official matches played in UEFA was roughly 1.3 times greater than that in J.League. The intensity of muscle exertion during gameplay should surpass that during training.
On the other hand, the 30% reinjury rate in our study was higher in comparison to the reports of van der Made et al 30 (19%), Malliaropoulos et al 18 (14%), Pollock et al 24 (18%), and Ekstrand et al 11 (16%), although it was less than the 40% reinjury rate reported by Verrall et al. 32 Several factors, including older age, prior hamstring injuries, intramuscular tendon involvement, a larger initial injury volume located at the BF, the presence of localized discomfort on posterior thigh palpation after RTP, and a history of anterior cruciate ligament or calf strain injuries, have been identified as potential risk factors for reinjury based on baseline MRI and clinical findings. ‡ In contrast, several studies have reported a mild to moderate correlation between reinjury and the findings on the baseline MRI study, including intramuscular tendon damage.18,20,26,30,31,33 In addition, Shamji et al 27 emphasized the significance of detecting injury that involves the distal muscle-tendon junction in the BF, due to the complex anatomy of this area, where the long and short heads have different sites of origin and separate innervation. The definition of HMI, sports events, category, sex, and age of participants varied in these studies.
Although the study only involved Japanese professional football players, there were no significant differences between the reinjury and no-reinjury groups with respect to age, past injury history, injured muscle, injury location, time of occurrence in the season, and type of injury. However, a statistical difference was observed regarding the type of injury in BF. In 9 of 13 type 1-T injuries (BF, ST, and SM), the injury was located in the middle third portion. In the case of type 1-T injuries involving the BF, a 2-week rehabilitation program was planned for all legs, which is the same as the protocol for type 1-M injuries. Six of these legs developed recurrent injuries, although the players were able to RTP within 2 weeks. Those findings suggest that the players with type 1-T injuries should be managed differently from those with type 1-M injuries. Delaying RTP or changing the rehabilitation program 3 might contribute to reducing the recurrence of type 1-T injuries. Although we used precise MRI sequences and parameters, it was not always easy to differentiate the intramuscular tendon from the myofascia. Evangelidis et al 12 reported that the length of the proximal aponeurosis was 16.7 ± 2.8 cm (range, 10.5-22 cm). Rehorn and Blemker 25 reported that the length of the proximal aponeurosis was 17.8 cm and that the thickness was approximately 3 mm. Further study is necessary to improve the precision of detecting intramuscular tendon injuries, particularly at the middle portion of the BF, which marks the end of aponeurosis on MRI.
Although no statistically significant difference was found in this study, there was a tendency for reinjury of the BF to occur at the start of the season, and a tendency for reinjury of the ST to occur in the distal third portion. Low temperatures at the start of the season, from January to February in Japan, may contribute to recurrence. In 2 of 6 legs with ST injuries that developed recurrent injuries, the injuries were located in the distal third portion. The reason for this was unclear because of the small sample size of this study.
This study had several limitations, including its retrospective design; a small sample size, which affects its statistical power; a narrow focus on male professional football players as participants; a lack of evaluation of other factors (eg, clinical findings and past injuries in other body parts); a lack of all 3 reviewers evaluating intraobserver agreement; and the definition of MRI classification, which was not clearly defined through qualitative evaluation.
Conclusion
Our study demonstrated that the overall incidence of HMI in Japanese male professional football players was 0.60 (/1000 ph): 2.30 (/1000 ph) in games and 0.35 (/1000 ph) in training. The rate of recurrence was 30%. In the BF, the injury type classified on MRI was the only factor associated with recurrence. Bleeding around the intramuscular tendon without structural tendon injury was an important factor for predicting the recurrence of BF injuries. Type 1-T injuries should be managed differently from type 1-M injuries.
Footnotes
Final revision submitted July 10, 2025; accepted September 8, 2025.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from The Jikei University School of Medicine (No. 36-232).