
Abstract
Background:
Patellar dislocation is a common condition in adolescents, characterized by high rates of recurrent instability and an associated risk of osteochondral fracture (OCF). The risk of recurrent instability in this patient population, both with and without OCF, after a first-time dislocation remains unclear.
Purpose:
To determine and compare the incidence of recurrent patellar instability and the need for subsequent stabilization procedures between adolescents with and without OCF after first-time dislocation. A secondary objective was to report clinical outcomes of those patients.
Study Design:
Cohort study, Level of evidence, 3.
Methods:
This study was a retrospective analysis of adolescents who underwent their first-time patellar dislocation between 2016 and 2021 at a single orthopaedic hospital, with a minimum follow-up of 3 years. Patients were divided into 2 groups based on whether OCF was present: the OCF group and the non-OCF group. Baseline characteristics, radiographic measurements, and follow-up time were compared. Primary outcome measures included the incidence of recurrent patellar instability and the need for subsequent stabilization procedures. Secondary outcome variables included clinical outcome scores (such as Kujala score, Lysholm score, Tegner score, and International Knee Documentation Committee score), knee range of motion (ROM), as well as the ability to return to sport.
Results:
A total of 33 adolescents were included, with 15 in the OCF group and 18 in the non-OCF group. The only difference noted in baseline characteristics, radiographic measurements, and follow-up time was a higher tibial tuberosity-trochlear groove (TT-TG) in the OCF group (17.1 mm vs 14.5 mm; P = .048). Compared with the non-OCF group, the OCF group had a significantly higher incidence of recurrent patellar instability (66.7% vs 27.8%; P = .025) and a greater need for subsequent stabilization procedures (53.3% vs 16.7%; P = .026). No differences were noted in clinical outcome scores, ROM, and return to sport rate.
Conclusion:
Adolescents with first-time patellar dislocation combined with OCF face a significantly higher recurrence rate (66.7%) compared with those without OCF, leading to increased subsequent stabilization procedures (53.3%). High-risk anatomic factors, such as elevated TT-TG values, further exacerbate instability. Targeted interventions are recommended for this high-risk population to reduce the recurrence of this condition.
Patellar dislocation is one of the most common knee injuries among adolescents, with an incidence rate of 5.8 to 7 per 100,000 individuals in the general population, rising dramatically to 29 per 100,000 in teenagers aged 10 to 17 years.5,9,32 Moreover, osteochondral injuries are present in up to 76% of patients after first-time dislocations, with osteochondral fracture (OCF) occurring in 31% to 58% of acute cases.15,16,21 OCF is commonly considered an indication for surgical intervention in acute patellar dislocations.8,29
Furthermore, literatures suggest a high rate of recurrent instability after surgeries for patellar dislocation with OCF, especially when medial patellofemoral ligament (MPFL) reconstruction (MPFLR) is not performed.6,8,29 Pedowitz et al 23 reported that 61% of adolescents undergoing surgical treatment for acute patellar dislocation with OCF experienced recurrent instability during a mean follow-up of 4.1 years. However, the surgical interventions in this study included both isolated arthroscopic debridement of osteochondral fragments and MPFL repair, which may not accurately reflect the rate of recurrent instability after patellar dislocation with OCF, as there is no direct comparison to patients without OCF. In cases where fragments are located outside the main contact and weightbearing area of the knee or are too small for fixation, isolated arthroscopic debridement with OCF removed is commonly performed, preserving the native patellar supporting structures. Consequently, the observed instability outcomes in this group may closely reflect the natural history of a first-time patellar dislocation complicated by an OCF.13,15,25
To date, it remains unclear what the recurrence rate of instability and the need for subsequent stabilization procedures are for adolescents with first-time patellar dislocation accompanied by OCF who undergo isolated arthroscopic debridement with OCF removed, and how these rates compare to those of adolescents with first-time dislocation without OCF. If the recurrent instability rate and the need for subsequent stabilization procedures in the OCF group exceed those of the non-OCF group, this would support the early inclusion of MPFLR or bony procedures alongside initial loose body removal to prevent future dislocations and associated joint damage. The purpose of the present study was to determine the rate of recurrent instability and the need for subsequent stabilizing procedures in adolescents with first-time patellar dislocations accompanied by OCF who undergo isolated arthroscopic debridement with OCF removed. We sought to compare outcomes with those in a non-OCF group. The secondary objective was to evaluate the clinical outcomes in both groups.
Methods
The study protocol received approval from the Ethics Review Committee of our university-affiliated hospital. Written informed consent was obtained from all participating patients. A retrospective review of the medical records was conducted, encompassing 433 consecutive patients diagnosed with patellar dislocation from January 2016 to December 2021 (Figure 1). Diagnosis was based on the patient’s history, physical examination, and imaging results (Figure 2A), while case records were reviewed to ensure the inclusion of only first-time patellar dislocations. Among these, 116 adolescent patients were diagnosed with first-time patellar dislocations. Patients were eligible for inclusion if they met the following criteria: (1) age ≤18 years; (2) confirmed diagnosis of acute first-time patellar dislocation (ICD-10 code S83.0); (3) surgical removal of osteochondral fragments (the largest diameter ≤8 mm, comminuted or located outside the main contact and weightbearing area of the knee) in the OCF group; and (4) a minimum follow-up of 3 years. Patients were excluded if they had a history of previous patellar instability on the injured knee or underwent patellar-related surgeries (eg, MPFLR or repair, open reduction, and internal fixation of osteochondral fragments) during the index procedure. The definition for OCF was an intra-articular loose-body containing components of both cartilage and bone, which were verified using magnetic resonance imaging (MRI) or computed tomography. Patients were categorized into 2 groups based on the presence of OCF: the OCF group included patients with OCF after an acute first-time patellar dislocation, while the control group included patients with an acute first-time patellar dislocation without OCF (Figure 2B).
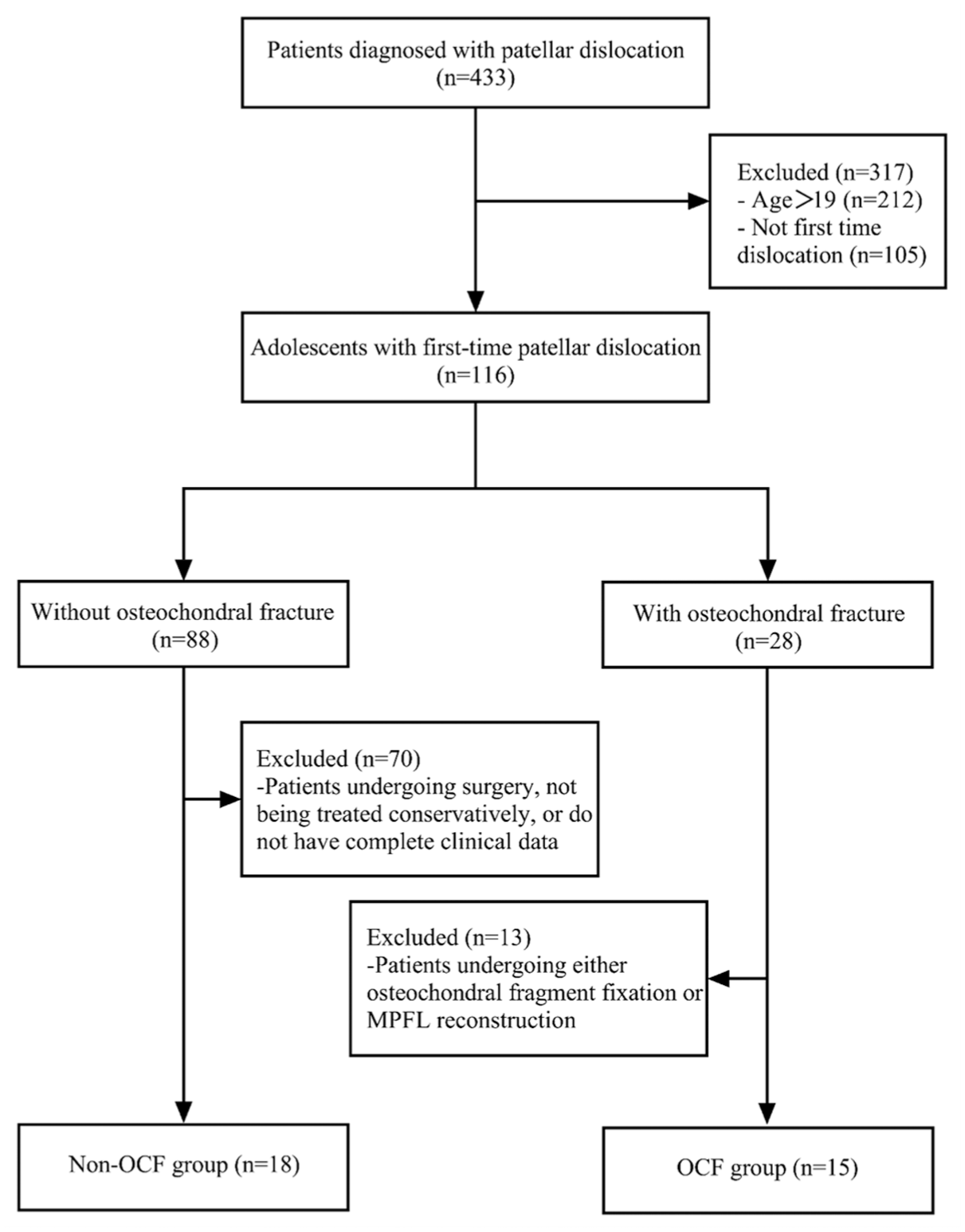
Flow chart of patient selection. OCF, osteochondral fractures; MPFL, medial patellofemoral ligament.

(A) An axial magnetic resonance image showing a focal osteochondral defect with an intra-articular loose body (arrow) in a patient from the OCF group. (B) An axial T2-weighted MRI and 3D CT of a patient from the non-OCF group at initial presentation. (C) An arthroscopic view demonstrating the removal of a loose osteochondral fragment in a patient from the OCF group. (D) A patient with first-time patellar dislocation without OCF receiving nonsurgical treatment with knee immobilization in full extension using a brace. CT, computed tomography; MRI, magnetic resonance imaging; OCF, osteochondral fractures; 3D, 3-dimensional.
Charts were reviewed for relevant demographic and historical information, including patient age, sex, weight, body mass index (BMI), injury laterality, and whether the patient had open physes. Operative notes were used to identify the loose osteochondral fragments procedure (removal vs fixation); whether the MPFLR or repair and lateral patellar support structures release were conducted; and any other concomitant procedures (eg, microfracture, chondroplasty). In the OCF group, all patients underwent standardized arthroscopic procedures using anteromedial and anterolateral portals. The joint cavity was irrigated to clear hemarthrosis, and loose osteochondral fragments were removed (Figure 2C). Microfracture techniques were applied to address femoral-sided weightbearing osteochondral defects, while defects covered by fibrin clots were left untreated. Patients requiring OCF fixation were excluded due to disruption of the patellar support structures. Patients in the control group received nonsurgical treatment, which included knee immobilization in full extension using braces or casts for 2 to 3 weeks (Figure 2D), combined with anti-inflammatory and analgesic medications. Physical therapy was initiated after immobilization to restore functionality, progressing gradually to full weightbearing. Rehabilitation protocols were adjusted based on treatment type. In the OCF group, patients were allowed immediate full weightbearing and low-intensity activity, with physical therapy beginning 1 week postoperatively to restore range of motion (ROM). Contact sports were avoided during the first 6 weeks, while running and high-intensity activities were reintroduced gradually after 2 months. In the control group, physical therapy began after the removal of immobilization devices, with activity restrictions consistent with those of the OCF group.
Primary outcomes included the incidence of recurrent patellar instability and the need for subsequent stabilization procedures, defined as any of the following: (1) the patient had further subluxation or dislocation episodes or (2) the patient underwent subsequent MPFLR or other patellar stabilization procedures. Secondary outcomes were assessed using the Lysholm score, Kujala score, Tegner score, International Knee Documentation Committee (IKDC) score, the knee ROM, and return to sport rate.
Radiographic Analysis
Imaging assessments included (1) skeletal maturity, determined from growth plate closure on anteroposterior radiographs of the knee (open physis classified as immature, closed physis as mature) 14 ; (2) patellar height, calculated using the Insall-Salvati index on sagittal MRI images (≥1.2 defined as patella alta, a commonly used threshold indicating at least mild patellar elevation) 10 ; (3) trochlear development, measured using the trochlear depth index (TDI) by the Pfirrmann method. 24 Based on the results of Stepanovich et al, 33 a TDI of <2 was classified as high-grade dysplasia, while TDI between 2 and 4 was classified as low-grade dysplasia; (4) tibial tuberosity-trochlear groove (TT-TG) distance 31 ; and (5) patellar tilt angle (PTA), with PTA >20° considered abnormal.1,2 Two experienced radiologists independently conducted all imaging evaluations.
Statistical Methods
Intraclass correlation coefficients were used to assess the consistency of imaging measurements. Continuous variables (eg, age, BMI, imaging indicator evaluations, clinical outcome scores, and ROM) between groups were compared using paired t tests or Wilcoxon signed-rank tests, depending on data normality. In contrast, categorical variables (eg, sex, skeletal maturity, and functional outcomes) were assessed with Pearson chi-square tests or Fisher exact tests. Statistical significance was defined as P < .05. All analyses were performed using IBM SPSS Statistics for Windows, Version 26.0 (IBM Corp).
Results
A total of 433 patients with patellar dislocation were identified, including 116 adolescents with their first episode of patellar dislocation. A total of 28 adolescents with their first patellar dislocation associated with OCF were identified. Of these, 13 patients who received concurrent osteochondral fragment fixation or MPFLR were excluded, resulting in a final cohort of 15 patients in the OCF group. The non-OCF group included 18 patients with first-time patellar dislocation without OCF, all of whom received nonoperative treatment (Figure 2). No significant differences were observed in the baseline demographic characteristics between the 2 groups (Table 1).
Patient and Radiographic Data a

Data are expressed as mean ± SD, unless otherwise indicated. The bold value indicates significance at P < .05. BMI, body mass index; OCF, osteochondral fractures; PTA, patellar tilt angle; TDI, trochlear depth index; TT-TG, tibial tubercle-trochlear groove distance.
The mean follow-up period for the OCF group was 76.9 ± 19.4 months (range, 46-99 months), with a mean age of 15.1 ± 2.2 years (range, 10-18 years). The group consisted of 9 female (60%) and 6 male patients (40%), and 6 patients (40%) were classified as skeletally immature based on the presence of open growth plates. The non-OCF group had a mean follow-up period of 72.8 ± 19.6 months (range, 47-104 months) and a mean age of 15.2 ± 1.8 years (range, 12-18 years), with 11 female (61.1%) and 7 male patients (38.9%). Eight patients (44.4%) in this group were determined to be skeletally immature.
In assessing the risk factors associated with patellar instability, it was observed that among the OCF group, 11 patients (73.3%) had patella alta, and 12 patients (80%) had a PTA >20°. Trochlear dysplasia was diagnosed in 13 patients (86.7%). The mean TT-TG distance was 17.1 ± 4.1 mm (range, 9.5-25.1 mm), with 3 patients (20%) exceeding 20 mm. The mean PTA was 21.7°± 5.6° (range: 10.7°-30.8°), while the mean Insall-Salvati index was 1.27 ± 0.21 (range, 0.88-1.65), and the TDI averaged 3.2 ± 1.2 mm (range, 1.2-6.1 mm). In contrast, in the non-OCF group, 8 patients (44.4%) had patella alta, 9 patients (50%) had a PTA of >20°, and 13 patients (72.2%) were diagnosed with trochlear dysplasia. The mean TT-TG distance was 14.5 ± 4.5 mm (range, 9.3-22.4 mm), with 2 patients (11.1%) exceeding 20 mm. The mean PTA was 20.6°± 4.5° (range, 13.6°-28.6°), while the Insall-Salvati index averaged 1.19 ± 0.15 (range, 0.89-1.46), and the TDI was 3.4 ± 1.1 mm (range, 1.4-5 mm). There were essentially no significant differences between the 2 groups except for the TT-TG distance. Detailed imaging measurements are summarized in Table 1.
In the OCF group, all 15 patients underwent arthroscopic debridement of loose osteochondral fragments. None of the patients received additional procedures such as MPFLR or repair, lateral retinacular release, or any bony procedures. Osteochondral fragments were predominantly located on the patellar medial facet in 12 patients, with 9 patients (60%) having OCF on the medial side, and 3 patients (20%) at the patellar ridge. Two patients (13.3%) had OCF on the femoral side, and 1 patient (6.7%) had OCF on both the patellar and femoral sides. Microfracture was performed in the 2 patients with femoral-sided OCF. No surgical complications were reported.
At the final follow-up, recurrent dislocation or subluxation occurred in 10 patients (66.7%) in the OCF group, which was significantly higher than the 27.8% (5 patients) observed in the non-OCF group (P = .025). Subsequent stabilization surgery (MPFLR or bony stabilization) was performed in 8 patients (53.3%) in the OCF group, compared with 3 patients (16.7%) in the non-OCF group, a statistically significant difference (P = .026) (Table 2).
Functional Outcomes of the Patient Cohort a

Data are presented as n (%). Bold values indicate significance at P < .05. OCF, osteochondral fractures.
Clinical outcomes, assessed by ROM (flexion degrees) and the Lysholm, Kujala, Tegner, and IKDC scores, revealed no significant differences between the groups (Lysholm: 84.5 in the OCF group vs 85.1 in the non-OCF group, nonsignificant [NS]; Kujala: 88.4 vs 89.1, NS; Tegner: 4 vs 4.1, NS; IKDC: 91.7 vs 91.1, NS; ROM: 132.6° vs. 132.1°, NS) (Table 3). Regarding the return to sports, 7 patients (46.7%) in the OCF group successfully resumed their activities, which was lower than the 13 patients (72.2%) in the non-OCF group; however, there was no statistically significant difference (Table 2).
Clinical Outcome Scores of the Patient Cohort a

Data are expressed as mean ± SD. OCF, osteochondral fractures; IKDC, international knee documentation committee; ROM, range of motion.
Discussion
This study provides a focused analysis of adolescent patients experiencing their first episode of patellar dislocation, comparing outcomes based on the presence of OCF and its specific management with isolated arthroscopic debridement (fragment removal). It highlights a recurrence rate of 66.7% in the OCF group after such treatment. Compared with adolescents with first-time patellar dislocation without OCF who received nonoperative treatment, the OCF group exhibited a significantly higher rate of recurrent instability and required more subsequent stabilization procedures. Additionally, the return to sport rate was substantially lower in the OCF group. Because the surgical approach in this study did not address the structural integrity of the medial or lateral stabilizing structures of the patella, the clinical outcomes in both groups likely reflect the natural progression of first-time patellar dislocation with or without OCF in adolescents.
The literature on recurrent instability after first-time patellar dislocation in adolescents shows substantial variability in recurrence rates,7,11,4,26,30 with limited stratification based on the presence of OCF. Pedowitz et al 23 reported a recurrence rate of 61% among adolescents treated surgically after acute patellar dislocation, including those with cartilage or osteochondral fragments. However, their study involved a heterogeneous cohort undergoing various surgical interventions, including MPFL suturing, microfracture, and chondroplasty, with 39% requiring secondary MPFLR. In contrast, our study exclusively included patients who underwent isolated arthroscopic debridement, excluding those who received MPFL suturing, reconstruction, or lateral retinacular release. These strict inclusion criteria reduce confounding factors and provide a clearer understanding of the natural progression of patellar dislocation with OCF. By differentiating patients with and without OCF, this study offers unique insights into the natural history of these distinct cohorts and improves the interpretability of the findings. Notably, the recurrence rate observed in our cohort aligns with findings of Pedowitz et al, 23 underscoring the high recurrence risk associated with OCF. The marked difference in recurrence rates likely stems from 2 key factors. First, the presence of an OCF may be a surrogate marker for a more severe initial injury, implying a higher-energy dislocation event that results in more substantial disruption of the MPFL and other medial stabilizers. Second, the OCF group demonstrated significantly higher TT-TG values, an established anatomic risk factor that contributes to inherent patellar instability. The combination of more severe soft-tissue injury and greater underlying anatomic risk likely explains the high rate of recurrent instability observed in the OCF group after an isolated debridement procedure that fails to address these fundamental pathologies.
The optimal surgical management for adolescents with first-time patellar dislocation combined with OCF remains controversial. 27 While nonoperative treatment is widely accepted for first-time patellar dislocation, surgical intervention to address a loose body is often necessary in cases involving OCF. Surgeons frequently limit their focus to the removal of loose fragments without surgically addressing the universally present MPFL injury. Although this approach may expedite recovery and yield better cosmetic outcomes, 12 its long-term efficacy remains uncertain. An alternative strategy is to perform MPFLR or repair during the initial surgery, aiming to address both instability and osteochondral damage. However, several randomized controlled trials have reported no significant differences in short- to mid-term outcomes between MPFL repair and nonoperative treatment for acute patellar dislocation.19,20,22,25 Some evidence supports the use of MPFLR during the initial surgery for patients with OCF. Gurusamy et al 8 found that MPFLR reduced the risk of recurrent instability by 5-fold compared with alternative approaches, while also decreasing the need for secondary surgeries and improving return to sport rates. 8 These findings align with our observation that adolescents with OCF face a significantly higher risk of recurrent instability and a greater need for subsequent stabilization procedures, which exacerbate joint damage and predispose patients to patellofemoral arthritis.28,12,23 Based on these results, MPFLR or bony stabilization may provide additional stability and reduce the long-term complications associated with recurrent dislocation in adolescents with OCF.
Our findings also suggest a role for anatomic risk factors in the higher recurrence rate observed in the OCF group. Specifically, TT-TG values were significantly higher in the OCF group. Although the mean value of 17.1 mm is borderline pathological, this finding does suggest a greater tendency for patellar lateralization in these patients. Previous studies have demonstrated that structural abnormalities, such as trochlear dysplasia, patella alta, and increased patellar tilt, predispose patients to recurrent dislocation and instability.3,36 Uimonen et al 34 reported similar findings, showing increased patellar lateralization in patients with OCF compared with those without. This lateralization likely increases contact stress between the patella and the lateral trochlear facet, contributing to osteochondral damage.17,18,35 While the Insall-Salvati index, PTA, and TDI were also higher in the OCF group, these differences did not reach statistical significance. Nonetheless, the mean values exceeded thresholds associated with an increased risk of recurrent instability. These findings suggest that for patients with OCF, particularly those with concurrent anatomic risk factors, such as an elevated TT-TG value, isolated arthroscopic debridement may be insufficient to prevent recurrent instability. This high recurrence rate raises an important clinical question regarding the optimal management for this high-risk group. While our study design does not permit a direct recommendation, our data support the rationale for future prospective studies to investigate whether the inclusion of a concurrent stabilization procedure, such as MPFLR, could improve outcomes and reduce the need for secondary surgeries.
Limitations
This study has several important limitations. The most significant limitation is the small sample size and the substantial number of exclusions, particularly in the non-OCF group. Of the 88 adolescents initially identified as not having an OCF, 70 were excluded, primarily because they were not treated nonoperatively or had incomplete data. This high exclusion rate raises the possibility of selection bias, as the final non-OCF cohort of 18 patients may not be fully representative of all adolescents with a first-time dislocation without OCF. This potential bias could affect the observed recurrence rate in the control group and, consequently, the comparison with the OCF group. Second, the retrospective nature of the study introduces inherent limitations. Finally, the observed difference in TT-TG values between groups, while a key finding, also acts as a confounding variable that complicates the interpretation of recurrence rates. Future multicenter prospective studies with larger, more representative cohorts are necessary to validate these findings.
Conclusion
Adolescents with first-time patellar dislocation combined with OCF face a significantly higher recurrence rate (66.7%) compared with those without OCF, leading to increased subsequent stabilization procedures (53.3%). These findings suggest that for patients with OCF, particularly those with concurrent anatomic risk factors, such as an elevated TT-TG value, isolated arthroscopic debridement may be insufficient to prevent recurrent instability.
Footnotes
Acknowledgements
The authors gratefully acknowledge the academic guidance provided by the Department of Sports Medicine, West China Hospital, Sichuan University.
Final revision submitted July 20, 2025; accepted September 8, 2025.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Zhengzhou Orthopaedic Hospital.