
Abstract
Background:
Bankart repair eliminates acquired shoulder laxity in overhead throwing athletes and sometimes results in decreased maximum shoulder external rotation angle and rates of return to play at preinjury levels. The authors developed a novel surgical reconstruction of the anterior band of the inferior glenohumeral ligament (AIGHL) to maintain shoulder laxity for throwing while stabilizing the shoulder joint.
Hypothesis:
AIGHL reconstruction would stabilize the shoulder joint while not decreasing maximum external rotation, whereas Bankart repair would decrease maximum external rotation.
Study Design:
Controlled laboratory study.
Methods:
Eight fresh-frozen cadaveric shoulders were tested in a custom shoulder-testing system. Anterior glenohumeral translation, maximum shoulder external rotation, and humeral head location relative to the glenoid were compared among the following conditions: an intact shoulder, a thrower’s shoulder model created by stretching the AIGHL, a Bankart lesion, Bankart repair, and AIGHL reconstruction. In AIGHL reconstruction, a fascia lata graft was patched between the detached AIGHL laterally and glenoid medially at maximum shoulder external rotation to maintain the AIGHL’s original length.
Results:
In the thrower’s shoulder, external rotation and anterior translation were significantly increased (intact, 128° and 2.8 mm; thrower’s shoulder, 142° and 7.3 mm; P < .05). A Bankart lesion significantly increased anterior translation (8.3 mm) when compared with the intact condition (P < .01). Bankart repair restored anterior translation (3.0 mm) to intact levels. However, maximum shoulder external rotation significantly decreased after Bankart repair (135°) when compared with the thrower’s shoulder (P = .01). AIGHL reconstruction restored anterior translation (6.5 mm) to the level of the thrower’s shoulder without decreasing the maximum shoulder external rotation (144°). In the simulated late cocking position, the location of the humeral head relative to the glenoid was unchanged, even after Bankart repair or AIGHL reconstruction.
Conclusion:
Bankart repair restored anterior translation to intact levels (tighter than in the thrower’s shoulder), but AIGHL reconstruction restored it to the level of the thrower’s shoulder. Maximum shoulder external rotation was restored to the level of the thrower’s shoulder after AIGHL reconstruction, whereas Bankart repair significantly decreased external rotation when compared with the thrower’s shoulder.
Clinical Relevance:
AIGHL reconstruction may be useful for Bankart lesion in overhead throwing athletes to restore anterior stability while maintaining maximum shoulder external rotation.
To stabilize shoulder joints with anterior instability, the anterior band of the inferior glenohumeral ligament (AIGHL) is often plicated upon anteroinferior labral repair (Bankart repair)4,12,25 because shortening of the stretched AIGHL with reattachment of the anterior labrum decreases anterior glenohumeral translation and thus prevents shoulder redislocation. 2 Clinical studies have shown that Bankart repair prevents shoulder redislocation when the bony defect in the glenoid or humeral head, or both, is not severe.1,4,10,25-27 However, for overhead throwing athletes, low rates of return to play at preinjury levels after Bankart repair have been reported.3,8,9,13,16,28,31,32 In one study on elite and professional baseball pitchers, only 20% could return to play at their preinjury levels after Bankart repair. 28
One of the reasons why many overhead throwing athletes cannot return to their previous levels of play after Bankart repair is thought to be the decrease in shoulder external rotation postoperatively. 9 The reported decrease in external rotation after Bankart repair was 12.5° in a biomechanical study 2 and 7.8° in a clinical study. 9 A decreased shoulder external rotation angle after Bankart repair can reduce pitching performance 9 because failing to maintain or restore a thrower’s external rotation to preinjury levels can result in decreased throwing velocity and pitching performance. 33
Use of a suture repair technique shortens the AIGHL because the inclusion of sufficient tissue in the suture bites causes the AIGHL to become plicated. Biomechanically, shortening of the AIGHL decreases shoulder external rotation and anterior glenohumeral translation.2,19 Therefore, some surgeons try to cause minimal plication of the AIGHL to maintain the maximum shoulder external rotation angle after Bankart repair for throwing athletes. 9 However, shortening of the AIGHL cannot be completely avoided, even with the use of small suture bites or knotless suture anchors. To prevent this shortening that can occur during Bankart repair, we developed a technique of arthroscopic AIGHL reconstruction that uses a fascia lata graft (Figure 1). In this procedure, a fascia lata graft is attached between the torn AIGHL with labrum and the glenoid at the maximum shoulder external rotation at 90° of shoulder abduction to maintain the original length of the AIGHL after suturing. The objective of this study was to evaluate the effect of AIGHL reconstruction on shoulder external rotation and anterior stability in a thrower's shoulder model with a simulated Bankart lesion by comparing the outcomes with those of Bankart repair. We hypothesized that AIGHL reconstruction would stabilize the shoulder joint as compared with the Bankart lesion while not limiting shoulder external rotation, whereas Bankart repair would decrease shoulder external rotation when compared with the thrower’s model.

Anterior band of the inferior glenohumeral ligament (AIGHL) reconstruction with a fascia lata graft.
Methods
Specimen Preparation
Eight fresh-frozen cadaveric shoulders were tested in a custom shoulder-testing system (mean age, 62.8 years; range, 49-72 years) (Figure 2). There were 4 male and 4 female donors. Human cadaveric shoulders were acquired from a body donation program (United Tissue Network). All specimens were thawed overnight before dissection and testing and had no evidence of rotator cuff tears, labral tears, capsular tears, or other gross disease under macroscopic inspection. All skin, soft tissues, and muscles were removed from the specimens, with the exception of the shoulder capsule and coracoacromial ligament.

Custom shoulder-testing system.
Shoulder-Testing System
The custom shoulder-testing system was used to create laxity in the human cadaveric shoulders and to measure glenohumeral translation and humeral rotation (Figure 2). The shoulder-testing system allowed 6 degrees of freedom in the glenohumeral joint. Two translation plates provided anterior-posterior and superior-inferior translation. Compression-distraction force was applied via a lever arm and bearing system attached to the top translation plate, where the scapula box was mounted. The humeral cylinder was fixed at the top of the arc of the shoulder-testing system. The angle of the arc of horizontal abduction or adduction could be adjusted to create various degrees of shoulder abduction. The shoulder-testing system allowed humeral external rotation and internal rotation, which were measured with a goniometer at the distal end of the humerus.
The long head of the biceps was cut at the proximal musculotendinous junction. The intra-articular portion of the biceps tendon was left intact. The scapula was potted with the glenoid oriented parallel to the top edge of the scapular box by using plaster of Paris. The humeral shaft was transected 2 cm distal to the deltoid tuberosity and fixed to the humeral cylinder. The shoulder was then mounted on the custom shoulder-testing system. All specimens were kept moist with 0.9% saline throughout the experiment.
Biomechanical Testing and Conditions
Biomechanical testing was performed at 60° of glenohumeral abduction (90° of shoulder abduction) to simulate an abduction position during throwing.5,7,11,17 Anterior glenohumeral translation, maximum shoulder external and internal rotation, and location of the humeral head relative to the glenoid were measured. Each specimen was subjected to 5 experimental stages: intact shoulder, simulation of a thrower’s shoulder by using a previously reported method to stretch the AIGHL,5,7,11,19,22,23 creation of a Bankart lesion, Bankart repair, and AIGHL reconstruction with a fascia lata graft (Figure 3).

Testing conditions: A, Intact shoulder. B, Thrower’s shoulder model created by stretching the anterior band of the inferior glenohumeral ligament (AIGHL). White arrows show the elongated AIGHL. C, Creation of the Bankart lesion. D, Bankart repair. E, Just before fixing the fascia lata graft to the AIGHL for AIGHL reconstruction. F, Completion of AIGHL reconstruction with the fascia lata graft. A, acromion; AI, anterior band of the inferior glenohumeral ligament; C, coracoid; F, fascia lata graft; G, glenoid; H, humeral head.
Anterior Glenohumeral Translation
Anterior glenohumeral translation was measured with a 3-dimensional digitizer (accuracy, 0.3 mm; Microscribe 3DLX [Immersion Corp]). For preconditioning, a 20-N force in the anterior and posterior directions was applied for 5 cycles. Then, anterior glenohumeral translation was recorded, with a 10- and 15-N anterior force applied for 2 trials each.19,22 During measurement of anterior glenohumeral translation, 22 N of compressive force was applied.
Maximum Shoulder External and Internal Rotation Angles
For preconditioning, 1.5 N·m of torque in external and internal rotation was applied for 5 cycles just before measurement of the shoulder rotation angles. Maximum external and internal rotation angles were then measured with a 360° goniometer by applying 2.2 N·m of torque under 22 N of compressive force.
Location of the Humeral Head Relative to the Glenoid
To evaluate the soft tissue balance under each condition, the location of the humeral head apex was recorded with respect to the glenoid using the Microscribe 3DLX.7,11 The humeral head apex is the most prominent point on the humeral head articular surface relative to a plane defined by the articular margin. The location of the humeral head apex at maximum external rotation (simulated late cocking phase during throwing) and at maximum internal rotation (simulated deceleration phase during throwing) was calculated with respect to the geometric center of the glenoid in the anterior-posterior, superior-inferior, and medial-lateral directions.
Creation of the Thrower’s Shoulder Model
The required laxity of the AIGHL that is necessary for throwing performance was experimentally created to simulate the thrower’s shoulder; this model has been described.5,7,11,19,22,23 To stretch the AIGHL, the humerus was externally rotated to 20% beyond maximum external rotation at 60° of glenohumeral abduction, which represented 90° of shoulder abduction. The 20% increase in maximum humeral external rotation was achieved by gradually applying an external torque of 1.5 N·m for 1 minute, followed by relaxation for 30 seconds. The external torque was increased in 1-N·m increments until the targeted humeral external rotation was reached. The humerus was then secured with a locking clamp in this position for 30 minutes. After this excessive external rotation of the humerus, the AIGHL in all specimens was elongated macroscopically without any capsular tear. This finding was similar to those of previous studies.5,7,11,19,22,23
Creation of the Bankart Lesion
To simulate the Bankart lesion experimentally, a sharp surgical knife was used to detach the AIGHL with labrum from the glenoid from the 2- to 6-o’clock position in the right shoulder (6- to 10-o’clock position in the left shoulder). The mean tear length was 30.8 mm.
Bankart Repair
Three 2.8-mm suture anchors (FASTak; Arthrex) loaded with No. 2 braided polyester suture material were placed at the 2-, 4-, and 6-o’clock positions in the right shoulder (6-, 8-, and 10-o’clock positions in the left shoulder) at the anterior edge of the glenoid. One limb of the suture in each anchor was passed through the AIGHL 6 mm away from the detached labrum. Nonsliding knots (RC (Rotator Cuff) knot) 24 were then tied to complete the Bankart repair.
AIGHL Reconstruction
For AIGHL reconstruction, a fascia lata graft was prepared by harvesting fascia lata from fresh-frozen cadaveric lower extremity specimens (mean ± SD age, 55 ± 12 years; 3 male and 5 female). Two layers of fascia lata were overlapped to make a thickness similar to the native AIGHL. The mean thickness of the fascia lata graft was 2.8 ± 0.8 mm and that of the AIGHL was 2.1 ± 0.4 mm. The graft width was the same as the tear width of the AIGHL after creation of the Bankart lesion. The graft length in the medial-lateral direction was 35 mm.
After all measurements had been completed after Bankart repair, all sutures were cut and removed, and all 3 suture anchors were removed with the same driver that was used to insert them, to avoid destroying the anchor holes in the glenoid. Then, 3 new 2.8-mm suture anchors were inserted into the same anchor holes used in the Bankart repair. Also, 2 more 2.8-mm suture anchors were placed 1 cm medial to the glenoid articular surface at the 3- and 5-o’clock positions in the right shoulder (7- and 9-o’clock positions in the left shoulder).
First, the lateral part of the fascia lata graft was attached to the torn articular edge of the AIGHL with 2 mattress sutures with No. 2 braided polyester. The medial part of the fascia lata graft was fixed to the glenoid via a double-row technique: lateral fixation at the anterior edge of the glenoid with 3 suture anchors and medial fixation 10 mm medial to the glenoid rim with 2 suture anchors. This was done at the maximum shoulder external rotation position in the thrower’s shoulder model, with 60° of glenohumeral abduction (90° of shoulder abduction), to restore the length of the AIGHL to that just before creation of the Bankart lesion.
Data Analysis
Statistical analyses were performed with STATISTICA software (StatSoft Inc). All measurements were performed twice, and the mean value was used for data analyses. To compare the anterior glenohumeral translation, the maximum shoulder external and internal rotation, and the location of the humeral head relative to the glenoid among the 5 conditions, repeated measures analysis of variance was performed. When a significant main effect was found, Fisher post hoc analysis was performed to identify differences among the conditions. All data are shown as mean and standard deviation with significance at P < .05.
Results
Thrower’s Shoulder Model
After the anterior capsule was stretched by application of excessive external rotation torque, the maximum glenohumeral external rotation angle was significantly increased as compared with the intact shoulder, by 14°, without any tear of the shoulder capsule (P < .0001). Anterior glenohumeral translation under 10 N (P = .01) and 15 N (P = .03) was significantly increased, but the location of the humeral head relative to the glenoid did not change in the thrower’s shoulder model as compared with the intact shoulder (late cocking, P = .74; deceleration, P = .64) (Tables 1-3).
Anterior Glenohumeral Translation a

AIGHL, anterior band of the inferior glenohumeral ligament.
Significantly higher vs intact shoulder (P < .05).
Significantly lower vs thrower’s shoulder (P < .05).
Significantly lower vs Bankart lesion (P < .05).
Maximum Shoulder Rotation Angle a

AIGHL, anterior band of the inferior glenohumeral ligament.
Significantly higher vs intact shoulder (P < .05).
Significantly higher vs thrower’s shoulder (P < .05).
Significantly lower vs thrower’s shoulder (P < .05).
Significantly lower vs Bankart lesion (P < .05).
Significantly higher vs Bankart repair (P < .05).
Humeral Head Position Relative to Center of the Glenoid a
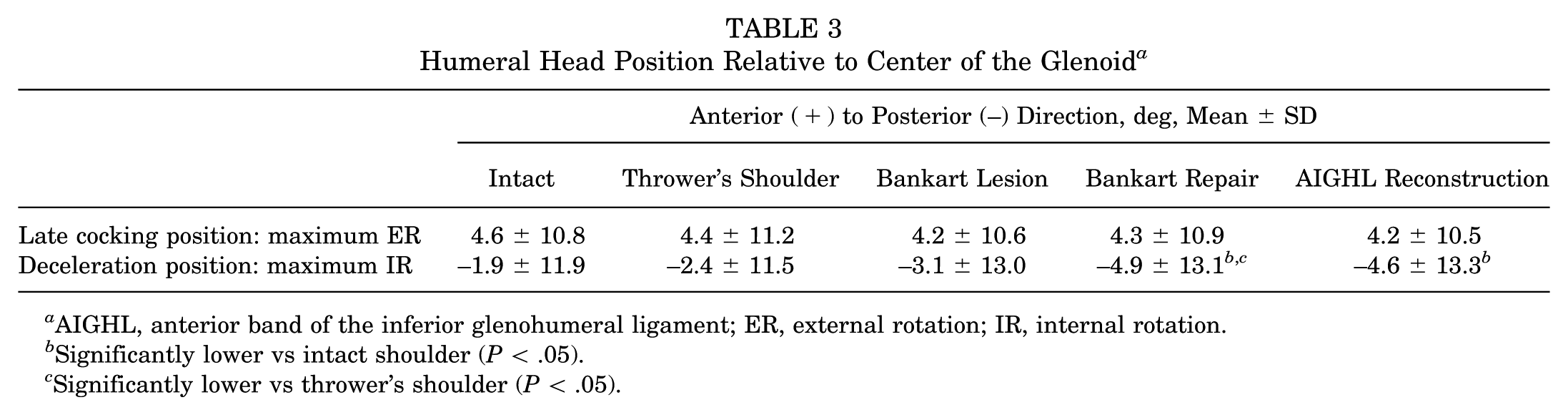
AIGHL, anterior band of the inferior glenohumeral ligament; ER, external rotation; IR, internal rotation.
Significantly lower vs intact shoulder (P < .05).
Significantly lower vs thrower’s shoulder (P < .05).
Creation of Bankart Lesion
After detachment of the anterior-inferior labrum, anterior glenohumeral translation was significantly increased as compared with the intact condition (10 N, P = .003; 15 N, P = .005). Maximum glenohumeral external rotation was significantly larger than in the intact condition (P < .0001) and thrower’s shoulder model (P = .01). The location of the humeral head relative to the glenoid did not change significantly after detachment of the anterior-inferior labrum (late cocking, P = .47; deceleration, P = .29) (Tables 1-3).
Bankart Repair
Bankart repair significantly decreased the anterior glenohumeral translation (10 N, P = .004; 15 N, P = .0003) and maximum shoulder external rotation angle (P < .0001) as compared with the Bankart lesion. The anterior glenohumeral translation (10 N, P = .01; 15 N, P = .002) and maximum shoulder external rotation angle (P = .001) after Bankart repair were significantly smaller than in the thrower’s shoulder model, just before creation of the Bankart lesion. At the late cocking position of throwing, the location of the humeral head relative to the glenoid did not change significantly after Bankart repair as compared with any other condition (P = .64-.90). However, in maximum internal rotation representing the deceleration phase, the humeral head shifted significantly posteriorly when compared with the intact condition (P = .01) and the thrower’s shoulder model (P = .03) (Tables 1-3).
AIGHL Reconstruction
AIGHL reconstruction significantly decreased anterior glenohumeral translation (10 N, P = .04; 15 N, P = .03) as compared with the Bankart lesion. There was no significant difference in anterior glenohumeral translation (10 N, P = .60; 15 N, P = .98) and maximum shoulder external rotation (P = .20) between AIGHL reconstruction and the thrower’s shoulder model. After AIGHL reconstruction, the location of the humeral head relative to the glenoid did not change significantly in the late cocking position as compared with any other condition (P = .48-.99). However, in the deceleration phase, the humeral head significantly shifted posteriorly when compared with the intact condition (P = .02) (Tables 1-3).
Discussion
Bankart repair is the gold standard for the treatment of traumatic anterior shoulder instability without severe bone loss.4,12,25 Here, we created increased anterior glenohumeral translation by AIGHL elongation and further anterior translation by detachment of the anterior-inferior labrum. Bankart repair restored glenohumeral anterior translation to the intact level, meaning that it has the effect of labral reattachment and AIGHL plication if one takes sufficient suture bites with a simple interrupted or mattress technique. Therefore, as Bankart repair can address AIGHL elongation and detachment from the anterior-inferior labrum—the primary pathology of anterior shoulder instability—it can lead to good stabilization in most patients with traumatic anterior shoulder instability without severe bone loss.
However, for overhead throwing athletes, especially baseball pitchers, return to play at preinjury levels is not easy, even after Bankart repair.3,8,9,13,16,28,31,32 Here, the shoulder laxity required for superior throwing performance14,16,22,29,30 was created by stretching the AIGHL in the thrower’s shoulder model.5,7,11,19,22,23 Afterward, a Bankart lesion was created to simulate traumatic anterior-inferior labral detachment 1 in the thrower’s shoulder. Then, Bankart repair restored anterior glenohumeral translation to the intact level, but anterior glenohumeral translation and maximum shoulder external rotation were significantly lower than in the thrower’s shoulder model. The decreased maximum shoulder external rotation may prevent the recovery of throwing form and performance in overhead throwing athletes 9 because ball velocity in baseball players is affected by the maximum shoulder external rotation angle at 90° of shoulder abduction. 33 Furthermore, the decreased maximum shoulder external rotation angle after Bankart repair may be one of the main reasons behind the low rate of return to play at preinjury levels after this repair in overhead throwing athletes. 9
We recently developed AIGHL reconstruction for the treatment of traumatic anterior shoulder instability in overhead throwing athletes. In AIGHL reconstruction, the fascia lata is attached to the glenoid medially and to the edge of the AIGHL laterally to restore the original length of the AIGHL. AIGHL reconstruction can therefore restore the native length of the ligament using a fascia lata autograft and can eliminate the unintended shortening that may occur during AIGHL plication when large suture bites are required for adequate fixation. The length of the AIGHL is significantly correlated with anterior glenohumeral translation and shoulder external rotation biomechanically. 19 Here, AIGHL reconstruction significantly decreased anterior glenohumeral translation and maximum shoulder external rotation when compared with the Bankart lesion. Furthermore, the maximum shoulder external rotation angle was normalized to that in the thrower’s shoulder model. Our results suggest that AIGHL reconstruction can restore anterior glenohumeral translation while maintaining the shoulder external rotation required for optimal throwing, whereas Bankart repair decreases external rotation. Therefore, AIGHL reconstruction can be a useful surgical option for traumatic anterior shoulder instability in overhead throwing athletes wishing to return to play at preinjury levels. The return to preinjury play needs to be tested in a future study.
In this biomechanical study, AIGHL reconstruction was performed at the maximum shoulder external rotation position in a thrower’s shoulder model, with 60° of glenohumeral abduction (equivalent to 90° of shoulder abduction), to restore the original AIGHL length. For clinical application in patients, we recommend fixing the fascia lata graft at the maximum external rotation angle with 90° of shoulder abduction, as measured intraoperatively under general anesthesia.
We recorded the location of the humeral head relative to the glenoid to evaluate soft tissue balance, which affects shoulder biomechanics during throwing motion in the 2 main critical phases of throwing: the late cocking phase and the deceleration phase. 6 If a pathologic humeral shift can be seen after surgery, then surgery may cause a secondary throwing injury, even if anterior glenohumeral translation was completely restored. In the simulated late cocking position, the location between the humeral head and the glenoid did not change even after Bankart repair or AIGHL reconstruction. In the late cocking position, humeral head shift is thought to be one of the risk factors for throwing injuries,7,17,18,20,21 including shoulder internal impingement or subacromial impingement. Therefore, in terms of humeral head location, either Bankart repair or AIGHL reconstruction can be a relatively safe surgical treatment for throwing athletes. In the simulated deceleration position, the humeral head shifted posteriorly after Bankart repair or AIGHL reconstruction. During the acceleration-to-deceleration phase of throwing motion, excessive anterior force is one of the risk factors for shoulder injuries, 6 such as labral tear or rotator cuff injury. Therefore, the posterior shift of the humeral head after Bankart repair or AIGHL reconstruction may decrease the risk of shoulder injuries by preventing excessive anterior glenohumeral translation during throwing.
The strengths of our study include its direct measurement of anterior glenohumeral translation, maximum shoulder external and internal rotation, and humeral head location relative to the glenoid in cadaveric shoulders. These measurements cannot be done precisely in clinical studies. Also, several conditions were tested in each specimen. These parameters and repetitive measurements cannot be applied to living subjects. In addition, the same size and location of the labral tears could be created in each cadaveric shoulder.
Nevertheless, our study had a few limitations. First, we used a static testing model. However, compression force was applied to the glenohumeral joint to simulate muscle balance during throwing and thus create reasonable results. The second limitation was that the ages of the cadaveric specimens were greater than those of throwing athletes. Yet, Lee et al 15 reported that specimens from older persons are still appropriate for nondestructive biomechanical studies because the degree of stiffness in the functional range of the shoulder capsule ligament is similar between younger and older people. Third, bone loss was not created at the glenoid or on the humeral head in our specimens. Still, most throwers do not have severe bone loss, even after shoulder dislocation. Therefore, the Bankart lesion that we created in the thrower’s shoulder model should be similar to that in the clinical situation. Fourth, this was a time-zero study, and there might be stretching, remodeling, or scarring of tissues that may limit external rotation afterward in the living participant. Therefore, significant findings in this study need to be investigated in the clinical studies. Fifth, the thrower’s shoulder model had only a 20% increase in maximum external rotation, and some throwers may have more or less. Finally, the Bankart repair model took a 6-mm bite into the AIGHL and labrum, and it is possible to take a smaller bite and still maintain adequate repair of the labrum to the glenoid.
Conclusion
Although Bankart repair restored anterior translation to the intact level (tighter than in the thrower’s shoulder), AIGHL reconstruction restored it to the thrower’s level. Furthermore, the maximum shoulder external rotation angle was restored to the level in the thrower’s shoulder after AIGHL reconstruction, whereas Bankart repair decreased external rotation significantly when compared with the thrower’s shoulder. Therefore, AIGHL reconstruction can be a useful surgical option in Bankart lesions in overhead throwing athletes to restore anterior stability while maintaining the maximum shoulder external rotation angle after surgery.
Footnotes
Final revision submitted April 21, 2025; accepted May 15, 2025.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.