
Abstract
Background:
Remplissage with Bankart repair (RMBR) is an arthroscopic procedure performed on <25% of Bankart lesions with off-track Hill-Sachs lesions (HSLs) that alters the insertion of the infraspinatus muscle into the humeral head. However, the effects of RMBR surgery on humeral head displacement due to changes in biomechanics and kinematics have not been fully elucidated.
Purpose:
To evaluate how the biomechanical and kinematic effects of the post-RMBR glenohumeral joint influence humeral head displacement using the finite element analysis (FEA) method.
Study Design:
Controlled laboratory study.
Methods:
Biomechanical and kinematic experiments were performed on 24 established finite element (FE) models, which included 12 normal glenohumeral joint models and 12 post-RMBR glenohumeral joint models at the abduction and external rotation (ABER) position. FEA was used to compute the total displacement of the humeral head during passive anteroinferior loading and active contraction of the infraspinatus muscle.
Results:
Under passive anteroinferior loading, the humeral heads showed less total anterior displacement after RMBR than did normal glenohumeral joints in the ABER position (1.94 ± 0.48 vs 5.19 ± 1.91 mm; P = .003). When the infraspinatus muscle was stimulated to contract, the humeral heads of post-RMBR glenohumeral joints exhibited greater total posterior displacement in the ABER position than did the normal glenohumeral joints (4.22 ± 0.23 vs 2.44 ± 0.56 mm; P < .001).
Conclusion:
Displacement of the humeral head is influenced by changes in the insertion of the infraspinatus tendon after RMBR surgery, which consequently affects the lever arm and torque generated by the infraspinatus muscle on the humeral head.
Clinical Relevance:
The FEA results confirmed that a change in the insertion of the infraspinatus tendon alters the lever arm and torque produced by the infraspinatus muscle on the humeral head. This leads to changes in the displacement of the humeral head in the ABER position after the RMBR procedure. These findings deepen the understanding of RMBR surgery in clinical practice and can assist physicians in deciding whether to choose this surgical approach in patients with combined HSL.
Keywords
Recurrent anterior shoulder instability is frequently linked to trauma and concurrent bone defects, making recurrent anterior shoulder instability the most prevalent type of shoulder instability.1,47,49 Recurrent shoulder instability often involves Bankart lesions and Hill-Sachs lesions (HSLs), for which the previously reported prevalence of recurrent anterior shoulder instability ranges from 60% to 100%.18,51,62 Most Bankart lesions are avulsions of the capsulolabral structures off of the anteroinferior glenoid. Glenoid bone loss can then occur with repeated dislocations.3,39 HSLs are common injuries caused by compression of the anteroinferior rim of the glenoid, resulting in a bone defect over the posterosuperior humeral head. 48 The size of the HSLs are larger in recurrent anterior shoulder dislocation. 44 The injuries are significant risk factors for further instability.
Purchase et al 50 described remplissage in 2008 as arthroscopic filling of the posterior joint capsule and infraspinatus tendon into the HSL for the treatment of patients with traumatic shoulder dislocation having Bankart lesions combined with HSLs.The clinical outcomes of remplissage with Bankart repair (RMBR) have been satisfactory, with a reduction in the rate of postoperative recurrence, 38 an improvement in the rate of return to sports,12,23 and low postoperative complications.19,30,63 The mechanism for stability in the RMBR procedure involves filling the infraspinatus tendon into the bony defect, which converts intra-articular lesions into extra-articular lesions. This prevents contact between the humeral head’s superior labrum and the anterior edge of the glenoid. 6 The most recent findings from our team suggest that the checkrein effect and active muscle control resulting from the medial shift of the infraspinatus tendon insertion point after RMBR surgery also contribute to the stability of the RMBR procedure. 67 However, the surgical approach alters the original physiological anatomy of the infraspinatus tendon. The effects of these alterations on the displacement of the humeral head due to changes in biomechanics and kinematics have not been fully explained.
The finite element analysis (FEA) method enables the examination of the biomechanical and kinematic effects on bones, tendons, and ligaments.34,52,61 This method bypasses some of the limitations inherent in traditional cadaveric experiments and clinical research. It is increasingly advantageous in the field of shoulder joints and is widely used in related research.4,20,64,65 The shoulder joint is more susceptible to anterior dislocation when the shoulder is in the abduction and external rotation (ABER) position. 10 In the ABER position, the infraspinatus muscle serves to restrict the anterior movement of the humeral head.1,7,17 There has been no FEA investigation into the effect of the RMBR procedure on humeral head displacement in the ABER position due to changes in biomechanics and kinematics. The purpose of this study was to use established finite element (FE) models of the normal glenohumeral joint and the post-RMBR glenohumeral joint in the ABER position to calculate the total displacement of the humeral head under loading, analyze the effect on this displacement due to changes in the insertion of the infraspinatus tendon after surgery, and then determine how the biomechanical and kinematic effects of the post-RMBR glenohumeral joint influence humeral head displacement. We hypothesized the following: (1) Compared with those of normal glenohumeral joints, FE models of post-RMBR glenohumeral joints in the ABER position exhibit a reduction in total anterior displacement of the humeral head under passive anteroinferior loading. (2) The FE models of the post-RMBR glenohumeral joint in the ABER position demonstrate a significantly greater total posterior displacement of the humeral head than do the FE models of the normal glenohumeral joint under active contraction of the infraspinatus muscle. (3) The RMBR procedure, which involves filling the infraspinatus tendon into the HSL, changes the lever arm exerted by the infraspinatus muscle on the humeral head. Given that the muscle force of the infraspinatus remains constant, the resulting torque changes, which in turn affects the displacement of the humeral head.
Methods
Establishment of Normal Glenohumeral FE Models
The study received approval from the ethics review committee of Chinese People’s Liberation Army General Hospital, and all participants provided informed consent. We selected 6 participants who met the inclusion criteria. The selection of 6 volunteers is not based on any specific reason. During the model-building process, the surface of the model is smoothed, and certain special anatomic features are ignored. However, the overall anatomic structure remains unchanged, and the use of imaging data from participants with normal structures does not affect the results of the experiment as the number of participants is increased. The inclusion criteria for individuals were as follows: (1) <50 years of age, (2) no shoulder deformity, (3) no history of shoulder trauma, (4) no history of shoulder surgery, (5) no positive findings on physical examination or functional evaluation by an orthopaedic sports medicine physician, and (6) no evidence of musculoskeletal disease on computed tomography (CT) and magnetic resonance imaging (MRI) scans. Modeling was performed using CT imaging data from 6 male participants (age range, 23-40 years; height range, 170-176 cm; weight range, 62.5-80 kg) with an ABER position in the right shoulder joint. The DICOM-formatted CT imaging data of the 6 participants were individually imported into Mimics Research software (Version 21.0; Materialise) to construct simulation models of the glenohumeral joint complex, which consisted of the scapula and the humeral head.46,65 The initial skeletal models were imported into 3-matic research software (Version 13.0; Materialise). The models underwent smoothing, repair, interference removal, and interference checking processes. Subsequently, surface and volume meshing were executed, resulting in 6 FE models of the normal glenohumeral joint complex in 100° of abduction and 90° of external rotation (Figure 1).

Normal glenohumeral joint model and mesh splitting. (A) Model of a normal glenohumeral joint in the abduction and external rotation (ABER) position, including the humeral head, scapula, joint cartilage, and labrum. The infraspinatus and humeral head cortical bone are shown in a transparent state. This model represents one of the normal glenohumeral joints in group 1 and group 3. Other normal glenohumeral joint models are similar. (B) ABER-positioned normal glenohumeral joint model with divided surface and volume meshes. The mesh divisions of the other normal glenohumeral joint models are similar.
The specific details of each structure are as follows: (1) Bone and cartilage: The thickness of the cortical bone of both the humeral head and the glenoid was set to 3.2 mm. 32 The mean thickness of the cartilage in the model was set at 1.3 mm, based on the mean cartilage thickness of approximately 1 to 1.5 mm measured from cadaveric and MRI scans.8,20,24,37 The population of our references is the general public, and the previous glenohumeral joint FEA was referenced for the cartilage thickness. During the FEA, the contact friction coefficient between the cartilage remains constant, and the cartilage thickness has a negligible effect on the experimental outcomes. (2) Glenoid labrum: The glenoid labrum was constructed using the same nodes as the cartilage union of the scapula and glenoid. 20 (3) Muscle: The infraspinatus muscle was modeled based on its normal anatomic origin and insertion points, as well as the footprint area at the humeral head.11,13,41,53 The material properties of each structure of the glenohumeral joint in the ABER position were determined based on previous studies (Table 1).9,20,26,28,53,65,66
Material Properties

Creation of Post-RMBR Glenohumeral FE Models
Using the 6 ABER normal glenohumeral joint models, we simulated the construction of models with Bankart lesions accompanied by HSLs. In the anteroinferior aspect of the glenoid (at 5-7 o’clock), we simulated a Bankart lesion model with glenoid bone loss of 15%. The areas of glenoid bone loss in the models showed no significant differences. Off-track HSL models were simulated in the posterosuperior region of the humeral head. The dimensions of the HSLs were as follows: length, 32 mm; width, 20 mm; and depth, 3 mm. The cortical bone at the simulated injury site was subtracted, the humeral head cartilage on the surface was removed, and the infraspinatus tendon was simulated to fill the HSL with 2 anchors. 20 Thus, post-RMBR glenohumeral joint models in the ABER position were constructed (Figure 2).
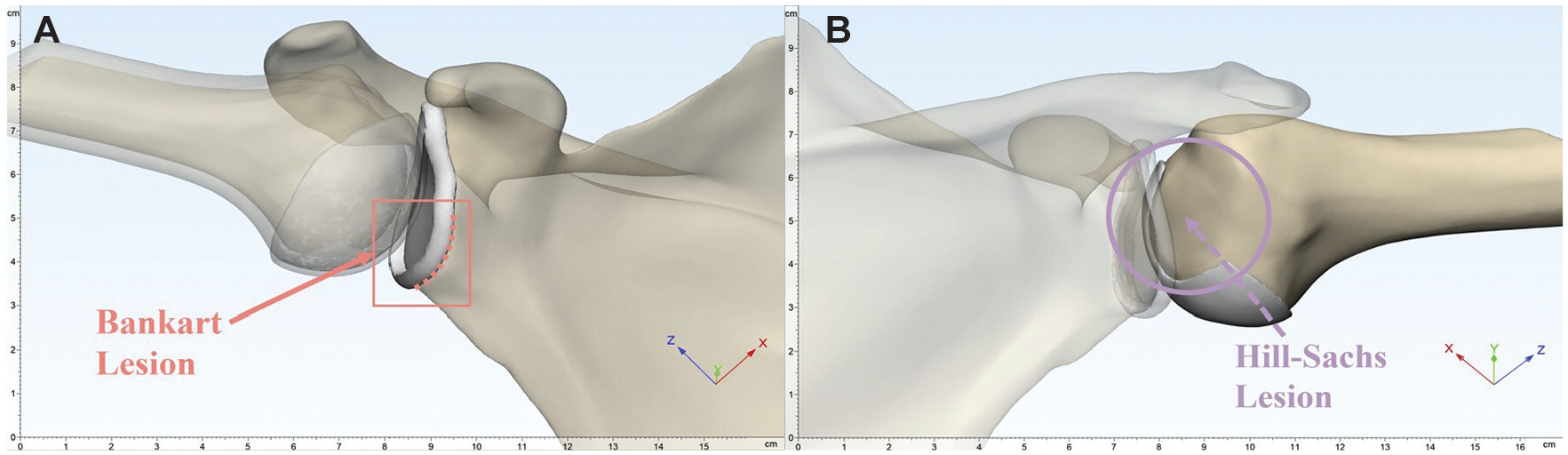
Glenohumeral joint model simulating a Bankart lesion and Hill-Sachs lesion (HSL). (A) Bankart lesion of the glenohumeral joint in the abduction and external rotation (ABER) position. The red dashed line indicates the site of avulsion of the anteroinferior glenoid labrum. (B) The HSL of the glenohumeral joint in the ABER position. The area indicated within the purple circle is the HSL region, located at the posterosuperior part of the humeral head (the scapula and the glenoid are transparent).
SolidWorks software (Version 2021; Dassault Systèmes) was used to simulate the construction of intraoperative anchors. Three 3.0 mm–long anchors (Gryphon BR; DePuy Mitek) were used for the Bankart injury (Figure 3A) and two 3.4-mm anchors (Healix Transtend; DePuy Mitek) were used for the Hill-Sachs injury (Figure 3A).15,20,27,29 The 12 constructed glenohumeral joint complex FE models were each duplicated, resulting in 24 models. These 24 models were divided into 4 groups: groups 1 and 3 each consisted of 6 normal ABER position glenohumeral joint models, while groups 2 and 4 each contained 6 post-RMBR glenohumeral joint models. There is no difference between the models of groups 1 and 3, but the loads for FEA are different. There is no difference between the models of groups 2 and 4, but the loads for FE are different.

The post–remplissage with Bankart repair (RMBR) glenohumeral joint model and mesh splitting. (A) Model of a post-RMBR glenohumeral joint in the abduction and external rotation (ABER) position, including the humeral head, scapula, joint cartilage, labrum, and anchors. The scapula, infraspinatus, and humeral head are shown in a transparent state. This model includes the post-RMBR glenohumeral joints in group 2 and group 4. Other normal glenohumeral joint models are similar. (B) ABER-positioned post-RMBR glenohumeral joint model with divided surface and volume meshes. The mesh divisions of the other post-RMBR glenohumeral joint models are similar.
FEA of the Glenohumeral 3D Models
The tetrahedral grids of the FE models were imported into ANSYS Workbench software (Version 19.2; ANSYS). Material properties (Table 1) were assigned to each structure of the glenohumeral models for static analysis. 55 The scapular boundary conditions were fixed, and the infraspinatus muscle, glenoid labrum, and glenoid cartilage were bonded to the scapula. Then, the medullary bone and cartilage of the humeral head were bonded to the humeral head cortical bone, which was bound to the infraspinatus muscle. In previous in vitro biomechanical studies of the shoulder joint, a load of 10 to 15 N was applied to the joint.58 -60,67 In the present study, a 10-N load simulating the infraspinatus muscle was applied to the glenohumeral joint.
For groups 1 and 2 (Figure 4, A and B), a 10-N passive load was applied to the humeral head models in the anteroinferior direction, simulating the force environment when the glenohumeral joints dislocated anteriorly in the ABER position. After setting the boundary conditions, FEA was performed to calculate the total anterior displacement produced by the humeral head in both the normal glenohumeral joint models and the post-RMBR glenohumeral joint models. The total anterior displacements of the normal glenohumeral joints and the post-RMBR glenohumeral joints in the ABER position were subsequently compared to determine the difference in the total anterior displacement produced by the humeral head when the glenohumeral joints were dislocated anteriorly.
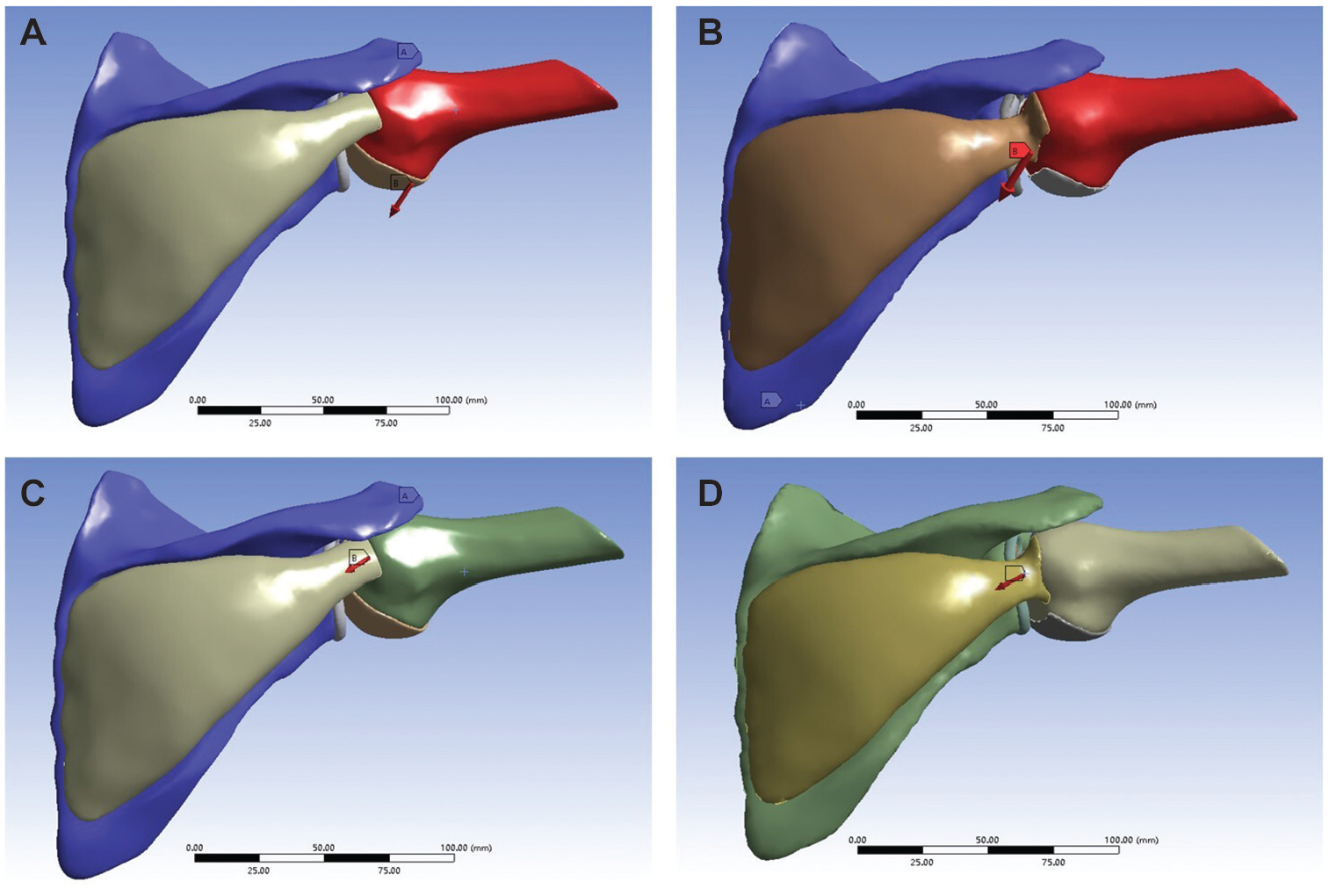
Finite element analysis of the loading conditions imposed. (A) In group 1, a 10-N load was applied to the humeral head in the anteroinferior direction in the normal glenohumeral joint model. (B) In group 2, a 10-N load was applied to the humeral head in the anteroinferior direction in the post–remplissage with Bankart repair (RMBR) glenohumeral joint model. (C) In group 3, a 10-N load was applied to the humeral head of the normal glenohumeral joint model to simulate contraction of the infraspinatus muscle. (D) In group 4, a 10-N load was applied to the humeral head of the post-RMBR glenohumeral joint model to simulate contraction of the infraspinatus muscle.
For groups 3 and 4 (Figure 4, A and B), a 10-N load was applied in the direction of infraspinatus muscle contraction, simulating the active contraction of the infraspinatus muscle in the ABER position of the glenohumeral joint. After setting the boundary conditions, FEA was performed to calculate the posterior total displacement produced by the humeral head in both the normal glenohumeral joint models and the post-RMBR glenohumeral joint models. The posterior total displacements of the humeral head in the normal glenohumeral joints and the post-RMBR glenohumeral joints in the ABER position were subsequently compared to determine the difference in posterior total displacement produced by the humeral head during active contraction of the infraspinatus muscle. The established FE models and FEA results were validated by comparing the direction and distance of humeral head displacement with those of previous related studies. Other muscles and tissues were not included in the FEA process, resulting in a greater displacement of the humeral head than that in previous in vivo studies.20,67
Statistical Analysis
All the results were analyzed using SPSS software (Version 25.0; IBM Corp), and a P value <.05 was considered to indicate statistical significance. Descriptive statistics, including the minimum, maximum, mean, and standard deviation, were calculated. The difference in total displacement between group 1 and group 2, as well as the difference between group 3 and group 4, was calculated. These differences conformed to a normal distribution, allowing for a paired test. Paired t tests and rank-sum tests were used to compare the total displacement of the humeral head in the normal glenohumeral joint with that in the post-RMBR glenohumeral joint under 2 loading scenarios. The Shapiro-Wilk test was used to test for a normal distribution, and P values were 2-tailed.
Results
Comparison of Total Humeral Head Displacement Under Anteroinferior Loading
In group 1 (Figure 5, A1-E1) and group 2 (Figure 5, A2-E2), a load of 10 N was applied to the humeral head anteroinferiorly to simulate the biomechanical environment during anterior dislocation of the glenohumeral joint. The total anterior displacements produced by the post-RMBR glenohumeral joints in group 2 were significantly less than those produced by the normal glenohumeral joints in group 1 in the ABER position (Figure 6A). The total displacement in group 1 ranged from 4.43 mm to 7.16 mm, with a mean of 5.19 ± 1.91 mm. In comparison, in group 2, the total displacement ranged from 1.06 mm to 2.46 mm, with a mean of 1.94 ± 0.48 mm. The difference in total displacement between the 2 groups was statistically significant (P = .003). The findings indicate that the total displacement of the humeral head in the post-RMBR glenohumeral joint is less than that observed in the normal glenohumeral joint when subjected to the same anteroinferior force loading (Table 2). This indicates that dislocation of the post-RMBR glenohumeral joint is less likely to occur. The observed variability is from general variability in shoulder anatomy among the original participants.

Total displacement generated by each humeral head model under loading. (A1-F1) Total anterior displacement of the humeral head exhibited by the normal glenohumeral joint models from group 1 in the abduction and external rotation (ABER) position when subjected to an anteroinferior load. (A2-F2) Total anterior displacement of the humeral head exhibited by the post–remplissage with Bankart repair (RMBR) glenohumeral joint models from group 2 in the ABER position when subjected to an anteroinferior load. (A3-F3) Total posterior displacement of the humeral head exhibited by the normal glenohumeral joint models from group 3 in the ABER position when the infraspinatus contracts. (A4-F4) Total posterior displacement of the humeral head exhibited by the post-RMBR glenohumeral joint models from group 4 when the infraspinatus muscle contracts.

Comparison of the total displacement across the models. (A) Comparison of the total anterior displacement between the normal glenohumeral joint models in group 1 and the post–remplissage with Bankart repair (RMBR) glenohumeral joint models in group 2 in the abduction and external rotation (ABER) position. (B) Comparison of the posterior total displacement between the normal glenohumeral joint models in group 3 and the post-RMBR glenohumeral joint models in group 4 in the ABER position.
Total Displacement of the Humeral Head in the ABER Position a
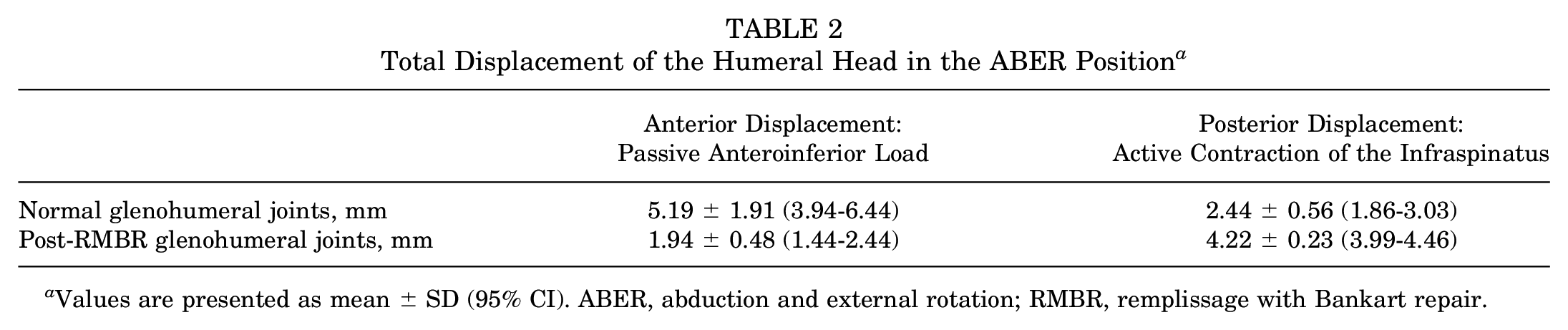
Values are presented as mean ± SD (95% CI). ABER, abduction and external rotation; RMBR, remplissage with Bankart repair.
Comparison of Total Humeral Head Displacement Subjected to Infraspinatus Contraction
In group 3 (Figure 5, A3-E3) and group 4 (Figure 5, A4-E4), a 10-N load was applied in the direction of infraspinatus contraction to simulate the biomechanical environment during glenohumeral joint abduction. The total posterior displacement produced by the post-RMBR glenohumeral joints in the ABER position in group 4 was significantly greater than that produced by the normal glenohumeral joints in group 3 (Figure 6B). The results showed that group 3 had a minimum total displacement of 1.90 mm and a maximum total displacement of 3.30 mm, with a mean of 2.44 ± 0.56 mm. In contrast, group 4 had a minimum total displacement of 3.82 mm and a maximum total displacement of 4.46 mm, with a mean of 4.22 ± 0.23 mm. The difference in total displacement between the 2 groups was statistically significant (P < .001). The observed variability is from general variability in shoulder anatomy among the original participants.
Discussion
The most significant finding of this study was the validation through FEA that the change in the insertion of the infraspinatus tendon affects the torque generated on the humeral head by the infraspinatus muscle, thereby affecting the displacement of the humeral head. In normal glenohumeral joints, the lever arm abducts from the center of the humeral head to the point of insertion of the infraspinatus muscle. In the post-RMBR glenohumeral joints, this lever arm extends from the center of the humeral head to the point at which filling occurs in the HSL. Consequently, torque is also altered in a constant force state (Figure 7). The humeral heads show less total anterior displacement in the glenohumeral joint after RMBR surgery than in the normal glenohumeral joint in the ABER position under a passive anteroinferior load. Simultaneously, the humeral heads exhibit more total posterior displacement in the glenohumeral joint after RMBR surgery than in the normal glenohumeral joint in the ABER position under a load that simulates active infraspinatus muscle contraction. This also explains how the changes in biomechanics and kinematics of the glenohumeral joint caused by the RMBR procedure affect the displacement of the humeral head.

Changes in the force arm and torque in the glenohumeral joint after the remplissage with Bankart repair (RMBR) procedure. The purple circle represents the center of the humeral head, the purple quadrilateral represents the insertion of the infraspinatus muscle into the normal glenohumeral joint, and the purple pentagon represents the insertion of the infraspinatus muscle into the glenohumeral joint after the RMBR procedure. The blue arrow shows the force arm of the normal glenohumeral joint, the green arrow shows the force arm of the glenohumeral joint after RMBR surgery, and the red dashed line shows the trajectory of the change in torque.
In cases of recurrent traumatic shoulder instability, an increase in displacement of the glenohumeral joint can be more easily observed when the joint is at functionally important degrees of abduction, and the glenohumeral joint is more susceptible to anterior dislocation when the shoulder is in the ABER position.33,43,56,60 Therefore, we used CT imaging data from participants in the ABER position for FEA in our experiment. HSLs are common in traumatic recurrent shoulder dislocations, and we typically perform RMBR for <25% of Bankart lesions combined with off-track HSLs. 14 This approach is used to prevent reengagement of the HSL site with the anteroinferior portion of the glenoid. 5 The RMBR procedure effectively restores stability to the glenohumeral joint and reduces the postoperative recurrence rate of anterior glenohumeral dislocation. Moreover, this approach does not significantly affect the function of the postoperative glenohumeral joint but yields satisfactory clinical outcomes, causing it to be widely used in clinical practice.21,35,42,68
In the normal glenohumeral joint, the infraspinatus tendon, which is part of the posterior component of the rotator cuff, exerts compressive, abductive, and externally rotating forces on the joint.17,54 The RMBR procedure modifies the physiological and anatomic structure of the infraspinatus muscle by filling the infraspinatus tendon in the HSL system, which repositions its insertion on the humeral head. This alteration to the lever arm and torque (Figure 7) of the infraspinatus muscle contraction results in significant changes in the biomechanical and kinematic effects produced during abduction of the shoulder joint. The procedure has a firm checkrein effect on the humeral head, effectively limiting its anterior displacement. 6
The FEA results confirmed that the modifications made to the insertion of the infraspinatus tendon after RMBR surgery alter the lever arm and torque on the infraspinatus muscle contraction. These changes affect the biomechanical and kinematic environment of the glenohumeral joint, resulting in a decrease in the anterior displacement of the humeral head. Consequently, there are enhanced limitations on anterior displacement of the humeral head.
This study focused on the influence of changes in the lever arm and torque generated by the infraspinatus muscle on humeral head displacement, thereby explaining the alterations in humeral head displacement after RMBR surgery.
In a cadaveric study, it was found that after RMBR surgery, the humeral head shifted more posteriorly and inferiorly at a shoulder joint abducted at 60°. 2 In a previous in vivo study using 3-dimensional MRI, compared with those of patients with normal shoulder joints, the humeral heads of patients who underwent the RMBR procedure were more posteroinferior in the ABER position during muscle relaxation. Additionally, the humeral head’s position moved farther posteriorly when the muscle contracted. 67 Notwithstanding the fact that the model incorporated solely the infraspinatus muscle, the findings of the FEA yielded outcomes that were comparable to those of previous in vivo experiments. These findings are consistent with the results of our current FEA study, which demonstrated the viability of constructing solely the infraspinatus muscle for the present experiment in the ABER position for a comparison between the normal glenohumeral joint and the glenohumeral joint after RMBR.
There was no significant difference in the force of the infraspinatus muscle between the postoperative glenohumeral joint (at least 24 months) and the normal glenohumeral joint.40,47 MRI also reveals good healing of the infraspinatus tendon filling in the HSL. 68 This suggests that the strength of the infraspinatus muscle can be restored to normal levels after RMBR. It is therefore feasible to use the same magnitude of force in performing the FEA.
The RMBR procedure increases the stiffness of the glenohumeral joint, which aids in maintaining joint stability. However, the increased stiffness and the motion restrictions resulting from the capsulodesis effect should be noted.16,57 The RMBR procedure alters the kinematics of the glenohumeral joint, and similarly, other nonanatomic surgical techniques aimed at enhancing shoulder joint mobility have demonstrated comparable outcomes, ultimately leading to the development of osteoarthritis.2,36 Previous studies have highlighted a significant association between glenohumeral instability repair and the subsequent development of glenohumeral arthritis.25,45,57 Specifically, the Putti-Platt procedure, similar to the RMBR procedure, restricts anterior displacement of the humeral head and is associated with a notable increase in both the incidence and severity of postoperative osteoarthritis. Therefore, attention should be paid to the potential long-term risk of osteoarthritis after RMBR surgery.31,57 Additionally, static posterior subluxation of the humeral head is commonly linked with glenohumeral arthritis. 22 Given that the RMBR procedure increases posterior displacement, this may contribute to the subsequent development of osteoarthritis.
Limitations
This research has certain limitations. The sample was limited to male participants and excluded factors such as age, sex, and individual variations in skeletal and soft tissue anatomy. To improve future studies, imaging data from a more diverse population would be beneficial. The post-RMBR model was developed based on a healthy glenohumeral joint model. Acquiring imaging data from a healthy shoulder in patients after RMBR is challenging. Future research could consider using imaging data from both the preoperative healthy state and postoperative state of the same patient for FEA. Previous research has not consistently used uniform material properties for FEA. Future investigations may use material properties that are more representative of human physiological structures and are consistently assigned. Modeling short-term variations in the infraspinatus muscle between a normal glenohumeral joint and post-RMBR is challenging. Therefore, we can only exclude the influence of muscle changes based on longer-term follow-ups postoperatively, as shown in previous studies. Certain structures, including other rotator cuff tissues, muscles, glenohumeral ligaments, and the long head of the biceps tendon, were not included in the shoulder joint models. The model of the shoulder joint complex did not incorporate other structures, resulting in greater total displacement of the humeral head in the FEA results than in reality. These experimental results were compared with those of previous FEA and in vivo experiments. The present results are consistent with previous results, and this increase in value does not affect our experimental conclusions.20,67 The increase does not affect the comparison of humeral head displacement between the normal glenohumeral joint and the post-RMBR glenohumeral joint after RMBR surgery. Future research will require more detailed models that are closer to the anatomic structures.
Conclusion
Displacement of the humeral head is influenced by changes in the insertion point of the infraspinatus tendon, which consequently affects the torque generated by the infraspinatus muscle on the humeral head. In normal glenohumeral joints, the lever arm extends from the center of the humeral head to the insertion point of the infraspinatus muscle during abduction. However, in post-RMBR glenohumeral joints, the lever arm extends from the center of the humeral head to the point of the HSL where filling has occurred. Therefore, under a state of constant force, the torque undergoes a corresponding change.
Footnotes
Final revision submitted August 22, 2024; accepted September 5, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study is supported by Capital’s Funds for Health Improvement and Research (2022-2-5051) and Chinese People’s Liberation Army General Hospital Transformation Project (ZH19008). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Chinese People’s Liberation Army General Hospital (reference No. S2023-026-01).