
Abstract
Background:
An anatomic modified Broström reconstruction has replaced traditional nonanatomic procedures as the standard of care for chronic lateral ankle instability. This technique typically involves repair of both the anterior talofibular ligament and the calcaneofibular ligament. However, this reconstruction is often limited by damage to native tissue and prolonged healing time, which restricts early weightbearing.
Hypothesis:
The suture tape–augmented Broström procedure would allow for early weightbearing without increasing the risk of early reconstruction failure, while allowing a satisfactory return to sport.
Study Design:
Case series; Level of evidence, 4.
Methods:
A retrospective chart review was conducted on patients who underwent a suture tape–augmented Broström reconstruction between August 2020 and January 2023. All patients followed a standardized accelerated rehabilitation protocol that included immediate postoperative weightbearing as tolerated. Primary outcomes included the ability to perform a single-leg hop and heel rise at 6 weeks postoperatively. Secondary outcomes included visual analog scale (VAS) scores, postoperative complications (eg, deep vein thrombosis [DVT], infection, return to operative suite, or failure), patient satisfaction, and return to sport.
Results:
A total of 133 patients were screened for inclusion in this retrospective review. A total of 119 patients met the inclusion criteria, with a mean follow-up duration of 16.7 ± 8.2 months (range, 6-52 months). A total of 27 patients had cartilage injuries requiring marrow stimulation; 20 of these were located in zone 6 of the talar dome. At 6 weeks postoperatively, 90% of patients were able to perform a single-leg heel raise and 81% could complete a single-leg hop. The mean VAS score at final follow-up (mean, 16.7 ± 8.2 months postoperatively) was 1.0 ± 1.9 (range, 0-8). At 1-year postoperative follow-up, 99% of patients reported satisfaction and 95% had returned to sport. Male patients were significantly more likely to complete the single-leg hop test at 6 weeks (P = .04). No instances of reconstruction failure, revision surgery, DVT, or postoperative infection were reported.
Conclusion:
Suture tape–augmented modified Broström reconstruction enabled immediate postoperative weightbearing without evidence of reconstruction failure. Most patients achieved excellent functional outcomes by 6 weeks, with minimal complications, high satisfaction, and return to sport before 1 year.
Keywords
Chronic lateral ankle instability poses a significant challenge to orthopaedic surgeons, particularly in the athletic population, necessitating effective surgical interventions for optimal functional recovery and reduced recurrence rates. Ankle sprains are a common injury among athletes, and patients frequently respond well to nonoperative interventions. 3 However, approximately 20% to 32% of patients fail nonoperative treatment and experience persistent pain, instability, and dysfunction. 2 Chronic lateral ankle instability can yield a change in joint biomechanics and joint contact forces, which may lead to posttraumatic osteoarthritis. 10
An anatomic modified Broström reconstruction is the current standard of care for surgical intervention. While the reconstruction technique is currently still debated, biomechanical studies have shown that a nonaugmented sutured anchor Broström reconstruction has <50% strength compared with native lateral ligamentous tissue, immediately after the repair. 12 Consequently, it is commonplace to immobilize, limit weightbearing status, and limit progression of athletic activity because of the risk of compromising the repair. Kirk et al 4 has shown that early unprotected range of motion is associated with lengthening failure. Recent literature also suggests an up to 28% failure rate with nonaugmented reconstruction techniques.7,13
Given the concern for early elongation, limited strength of the repair—which requires prolonged protected weightbearing—and slow progression to full activity, a suture tape–augmented Broström procedure has been proposed. This may help maximize the benefits of early range of motion exercises and weightbearing while protecting the repair. 9 In an athletic population, early weightbearing allows for accelerated rehabilitation while preserving tone and proprioception. While previous studies have examined suture tape augmentation or early mobilization separately, few have evaluated outcomes from a standardized protocol that combines immediate weightbearing, accelerated rehabilitation, and suture tape augmentation in a large cohort. This study adds to the current literature by analyzing real-world outcomes from a consistent operative and rehabilitation approach in a high-demand population.
We hypothesized that a suture tape–augmented Broström procedure would allow immediate weightbearing while preventing early failure, thereby facilitating earlier return to return to function.
Methods
A retrospective chart review was performed of a single orthopaedic foot and ankle surgeon (K.D.M.) practicing at a large academic tertiary referral center with a high volume of collegiate athletes. The chart review was limited to patients who had undergone lateral ankle instability repair with a suture tape (Internal Brace; Arthrex)–augmented Broström reconstruction from August 2020 to January 2023. Our inclusion criteria consisted of magnetic resonance imaging confirmation of anterior talofibular ligament (ATFL) injury, a positive anterior drawer, failure of nonoperative management, and postoperative physical examination consisting of a single-leg hop test and/or single-leg heel raise at 6 weeks. Our exclusion criteria included patients with concomitant cartilage injuries requiring allograft repair, posterior arthroscopic debridement, peroneal tendon repair, syndesmosis repair, and calcaneal osteotomies as detailed in the CONSORT (Consolidated Standards of Reporting Trials) diagram (Figure 1). All patients participated in our accelerated rehabilitation protocol, which included immediate postoperative weightbearing as tolerated in a fracture boot for 2 weeks followed by weightbearing as tolerated in a lace-up ankle brace for ≥4 weeks. Physical therapy (PT) was initiated at 2 weeks postoperatively, as detailed below.

CONSORT (Consolidated Standards of Reporting Trials) diagram illustrating patient flow through the study. Of 133 patients assessed for eligibility, 14 were excluded due to concomitant procedures or graft-requiring cartilage injuries. None was lost to follow-up. VAS, visual analog scale.
Demographic data were obtained for each patient. Our primary outcome was the ability of patients to perform a single-leg hop test and/or a single-leg heel raise at 6 weeks as shown in Figure 1. Secondary outcomes were collected by phone interviews or direct patient interaction and included visual analog scale (VAS) scores, postoperative complications (deep vein thrombosis [DVT], failure, infection, return to operative suite, etc), patient satisfaction, and return to sport at 1 year. The VAS scale was 0 to 10 with 0 indicating no pain at all. Patient satisfaction was reported as yes or no at the 1-year follow-up. A functional physical examination test was performed by the senior author (K.D.M.) in clinic at the 6-week postoperative mark.
Statistical Analysis
Demographic and functional outcomes were included in the statistical analysis for each patient. The single-leg hop test and heel-raise test were viewed as pass/fail. A 2-samples t test was used to compare outcome measures. Statistical significance was defined as P < .05.
Operative Procedure
An initial diagnostic arthroscopy was performed with debridement as needed. Osteochondral lesions measuring <10 mm were treated with limited marrow stimulation, while those >10 mm were treated with cartilage allograft and were excluded from this study. After arthroscopy, an oblique longitudinal incision was made from the distal fibula to the fourth metatarsal. A 1-cm periosteal cuff of tissue was elevated from the tip of the fibula to 2 cm proximal. Residual ATFL and calcaneofibular ligament were sharply released. The distal fibula was prepared with a rasp, and a bed of bleeding bone was established at the repair site. The proximal band of the ATFL was traced to its insertion on the lateral wall of the talus. Electrocautery was used to mark the site just off the articular cartilage margin at the natural bare area, which was then drilled and tapped. A 4.5-mm SwiveLock anchor (Arthrex), loaded with suture tape, was inserted (Figure 2). A free needle was used to pass the suture tape superficially relative to the ATFL (Figure 3). Two 2.3-mm all-suture knotless anchors (DX Knotless FiberTak; Arthrex) were then inserted, 1 at 6 mm proximal to the tip of the fibula for the calcaneofibular ligament and 1 at 18 mm for the ATFL. The ATFL and calcaneofibular ligament were reapproximated to the fibula. The suture tape was then laid superficially to the ATFL and inserted 12 mm proximal to the fibula tip with a 3.5-mm anchor (Figure 4). The periosteal flap was imbricated to the inferior extensor retinaculum with 2-0 Vicryl suture (Ethicon). At this point, the suture tape was covered by native tissue. The dermal layer was closed with 3-0 Vicryl and the skin with 3-0 nylon. Local anesthetic was injected. Xeroform, dry dressing, and ACE wrap (3M) were applied. A standard CAM boot (Aircast) was then placed. DVT prophylaxis consisted of aspirin 81 mg twice a day for 14 days. 9
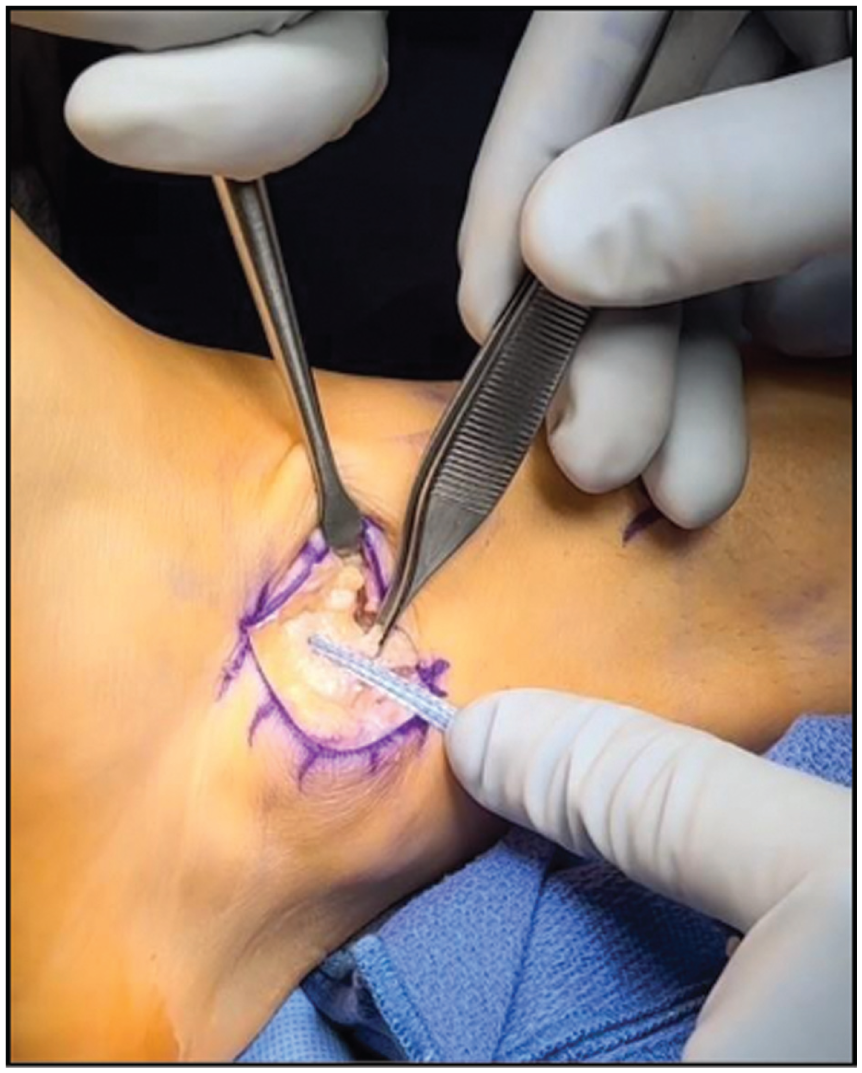
The forceps display the proximal band of the anterior talofibular ligament (ATFL). A 4.5-mm anchor is placed at the insertion of the ATFL about the lateral wall of the talus (bare area).

The suture tape is passed superficially to the anterior talofibular ligament.

Two 1.8-mm all-suture knotless anchors are inserted. One at 6 mm and another 18 mm, from the tip of the fibula. A third hole is made 12 mm from the fibula tip to accommodate a 3.5-mm anchor for suture tape insertion.
Postoperative Protocol
A fracture boot was worn for 22 to 23 hours per day (including during sleep) to provide comfort and support all weightbearing until the first postoperative check (10-14 days) (Table 1). The patient was allowed to weightbear as tolerated immediately postoperative. All patients were transitioned to a lace-up ankle brace at the first postoperative visit, when formal PT was initiated as well. If patients felt they could not progress out of the boot at the initial postoperative visit, they were encouraged to discontinue it as soon as tolerated. Stationary and recumbent biking, as well as blood flow restriction therapy, were encouraged. Stationary and recumbent biking were performed out of the brace using supportive footwear. Range of motion exercises were also conducted out of the brace and progressed as tolerated under the guidance of the therapist. A standardized lower extremity blood flow restriction therapy protocol was used, incorporating both isolated calf exercises and compound upper and lower extremity movements under PT supervision. Patients began single-leg proprioception training and heel raises. We encouraged increasing ambulation speed and distance. Anti-inflammatories, ice, elevation, and compression were paramount to minimize swelling as activity increased. At week 6, patients were weaned from the lace-up ankle brace. Elite-level athletes continued to practice in the brace or tape for an additional 4 weeks. Patients were to continue using their brace during a walk-to-run program and sport workouts/therapy. During weeks 8 to 12, noncontact sports were initiated and sport-specific therapy increased. Full return to sport and all activities were allowed at 12 weeks postoperative. Elite athletes were cleared to return to sport after 6 weeks if they had achieved ≥85% of their baseline (preoperative) agility functional scores, as measured by preoperative Global Positioning System tracking data from our institution's athletic training programs.
Postoperative Protocol Timeline Including Milestones and Interventions in Standardized Accelerated Rehabilitation Protocol a

Postop, postoperative; WBAT, weightbearing as tolerated.
Results
A total of 133 patients were screened for inclusion in this retrospective review. The final cohort included 119 patients after applying the study's inclusion and exclusion criteria, as shown in Figure 1. Our patients included 34 male and 85 female patients with a mean age of 37 ± 12.3 (range, 18-68) years. The mean body mass index (BMI) was 30 ± 8 kg/m2. Of the 119 patients included, 40 were active in organized sports at the time of surgery. Our mean follow-up was 16.7 ± 8.2 (range, 6-52) months (Table 2). At 6 weeks postoperatively, 90% of patients performed a single-leg heel raise successfully while 81% of patients performed a single-leg hop test (Table 3). The mean VAS at final follow-up was 1.0 ± 1.9 (95% CI, 0.7-1.3; range, 0-8). Of the 119 patients included, no failures were observed nor revision surgery required. Postoperative complications included neuritis (n = 9), all of which were transient and resolved with nonoperative management. Persistent pain was reported in 4 patients (Table 4). There was no statistical difference in primary and secondary outcomes in patients who underwent concomitant marrow stimulation at the time of the lateral ligament repair cartilage injuries. Male patients were more likely to be able complete a single-leg hop test at 6 weeks postoperative compared with female patients (88% vs 77%; P = .04; 95% CI for difference, 1.1%-20.4%). No other demographic factors, including age, BMI, or tobacco use, were significantly associated with early hop or heel-raise performance.
Patient Demographics and Clinical Characteristics, Including Sex, Tobacco Usage, Age, and Mean Follow-up a
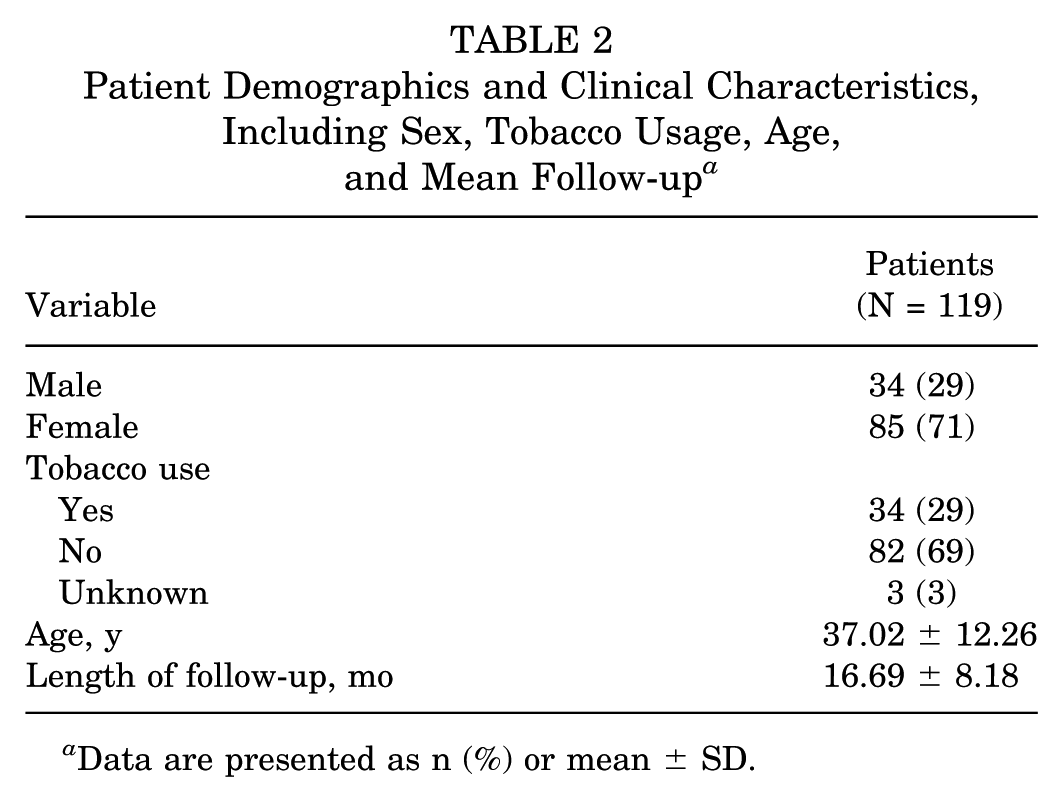
Data are presented as n (%) or mean ± SD.
Patient-Reported Outcomes After Suture Tape– Augmented Modified Broström Reconstruction

The total number of patients assessed (n) varies by outcome based on data availability at the time of follow-up or applicability of the test. For example, not all patients completed functional testing or 1-year follow-up assessments (e.g., satisfaction, return to sport).
Postoperative Complications in Patients Undergoing Suture Tape–Augmented Modified Broström Reconstruction (N = 119) a

Data are presented as n (%).
Discussion
There is no clear consensus regarding optimal functional rehabilitation protocol after a lateral ligament reconstruction procedure. Patient factors, reconstruction techniques, and surgeon experience can all contribute to a variety of protocols among providers. There is limited literature on early functional rehabilitation and weightbearing after a lateral ligament reconstruction. In the few studies that evaluate an immediate weightbearing protocol, a small sample size has been observed.1,5,6 Additionally, there is conflicting evidence for the support of early versus delayed mobilization, with some authors suggesting that a delayed mobilization protocol is superior. 11 However, the majority of the literature investigating this topic discusses techniques without suture tape augmentation.
Immediate weightbearing can help prevent loss of proprioception and muscle atrophy that may be experienced with postoperative immobilization. Direct repair of lateral ligaments or suture anchor fixation in a Broström reconstruction may not be amenable to immediate postoperative weightbearing because of the risk of compromising the repair.4,5 These surgical techniques have also been shown to experience failure rates of up to 28% and high rates of decreased athletic activity.7,8,13
Coetzee et al 1 performed a retrospective review of patients who underwent a modified Broström procedure with suture tape augmentation and an immediate postoperative weightbearing protocol in a cast. They found that 86.4% of patients returned to normal or near normal functional level and found an accelerated time to return to play for athletes, with some participating as early as 8 weeks postoperative. Kulwin et al 5 performed a prospective study comparing a nonsuture tape– versus suture tape–augmented reconstruction with an identical postoperative protocol to Coetzee et al and found that patients undergoing a suture tape–augmented reconstruction reached their return to preinjury activity level 4.2 weeks quicker than those without the suture tape–augmented reconstruction.1,5 In both of these studies, no instances of reconstruction failure or recurrent instability were observed in patients who received a suture tape–augmented reconstruction. Similarly, augmented repairs using an accelerated rehabilitation protocol in a military population demonstrated early return to duty with only 1 reported failure. 9
Our study of 119 patients demonstrates that patients experience excellent functional outcomes in the acute and short-term postoperative setting with an immediate weightbearing and accelerated rehabilitation protocol. These outcomes are especially promising in the context of sports medicine, where rapid return to activity is often prioritized. Minimal complications were experienced in our study population, with neuritis being the most common. While male patients were significantly more likely to complete the single-leg hop test at 6 weeks, no other demographic factors were found to significantly predict early functional success. Further prospective studies may help clarify whether sex-based or other demographic influences affect early rehabilitation outcomes. Importantly, no failures, episodes of recurrent instability, or revision surgery were experienced at 1-year postoperative. This supports our hypothesis that a suture tape–augmented Broström reconstruction for lateral ankle instability allows for early weightbearing while preventing early failure.
While the use of suture tape and additional anchors may increase the immediate cost of the operative procedure, these expenses must be weighed against the potential economic benefits of an accelerated recovery. Earlier return to work and sport may reduce time lost from employment, PT sessions, and long-term health care utilization related to delayed rehabilitation or complications. For high-demand individuals, particularly those in physically intensive professions or competitive athletics, the ability to return to function within 6 weeks may offer meaningful financial and quality-of-life advantages that justify the upfront implant cost. Future cost-effectiveness analyses would be valuable to quantify these trade-offs more precisely.
This study was conducted at a large academic tertiary referral center with a high volume of athletic patients, including collegiate athletes. While this population may be more motivated and physically conditioned for rapid recovery, the standardized surgical technique and rehabilitation protocol may still offer value in broader clinical settings. Although only one-third of our patients were involved in organized sports, the majority still benefited from a rapid return to functional activities, which may facilitate earlier return to work and daily responsibilities in nonathletic or lower-demand populations. Future studies should evaluate the safety and efficacy of immediate weightbearing in more diverse patient populations, including older adults and those with lower baseline physical function.
Strengths and Limitations
Strengths of our study include the use of a single surgeon, single implant, and standardized postoperative protocol for our patients. Our initial arthroscopic evaluation before performing our augmented modified Broström allowed us to stratify patients with and without cartilage injury. There are also significant limitations to our study. We lack long-term follow-up and interval follow-up between 6 weeks postoperative and 1 year. In addition, we did not collect subjective functional outcome scores or return to preinjury level of activity outcome data. The study also did not track the recurrence of ankle sprains beyond 1 year. Finally, while the cohort included many physically active individuals, only one-third of patients were involved in organized sports, which may limit the applicability of findings to high-performance athletic populations.
Conclusion
Our study, with a large sample size, demonstrates that suture tape–augmented lateral ligament reconstruction for chronic lateral ankle instability allows for immediate weightbearing while preventing failure. Augmented repairs with immediate weightbearing and a protected accelerated rehabilitation program have allowed for early return to function (work) and in-season sports.
Footnotes
Final revision submitted August 4, 2025; accepted September 1, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: K.M. is a paid consultant for Arthrex, iWalk, Trition Inc, ConMed, and the United States Army. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from The Ohio State University (study No. 2022H0316).