
Abstract
Background:
Anatomic lateral ankle ligament reconstruction has been proposed for patients with chronic ankle instability. A reliable approach is a reconstruction technique using an allograft and 2 fibular tunnels. A recently introduced approach that entails 1–fibular tunnel reconstruction might reduce the risk of intraoperative complications and ultimately improve patient outcome.
Hypothesis:
We hypothesized that both reconstruction techniques show similar ankle stability (joint laxity and stiffness) and are similar to the intact joint condition.
Study Design:
Controlled laboratory study.
Methods:
A total of 10 Thiel-conserved cadaveric ankles were divided into 2 groups and tested in 3 stages—intact, transected, and reconstructed lateral ankle ligaments—using either the 1– or the 2–fibular tunnel technique. To quantify stability in each stage, anterior drawer and talar tilt tests were performed in 0°, 10°, and 20° of plantarflexion (anterior drawer test) or dorsiflexion (talar tilt test). Bone displacements were measured using motion capture, from which laxity and stiffness were calculated together with applied forces. Finally, reconstructed ligaments were tested to failure in neutral position with a maximal applicable torque in inversion. A mixed linear model was used to describe and compare the outcomes.
Results:
When ankle stability of intact and reconstructed ligaments was compared, no significant difference was found between reconstruction techniques for any flexion angle. Also, no significant difference was found when the maximal applicable torque of the 1-tunnel technique (9.1 ± 4.4 N·m) was compared with the 2-tunnel technique (8.9 ± 4.8 N·m).
Conclusion:
Lateral ankle ligament reconstruction with an allograft using 1 fibular tunnel demonstrated similar biomechanical stability to the 2-tunnel approach.
Clinical Relevance:
Demonstrating similar stability in a cadaveric study and given the potential to reduce intraoperative complications, the 1–fibular tunnel approach should be considered a viable option for the surgical therapy of chronic ankle instability. Clinical randomized prospective trials are needed to determine the clinical outcome of the 1-tunnel approach.
Keywords
Ankle sprain is a common injury, 23,40 especially among the athletic population. 16,22,25,31 Despite nonoperative treatment for acute ankle sprains, 26 32% to 40% 18,28,43 of all patients develop chronic ankle instability (CAI), which is defined as recurrent sprains and residual local symptoms 3 to 6 months after the initial acute ankle sprain. 11 Operative procedures are recommended for patients with CAI and failure of nonoperative treatment. The direct ligament repair described by Broström 4 and modified by Gould et al 20 using the lateral inferior extensor retinaculum as an amplification is considered the gold standard. Good long-term clinical results 3,33 and improvement of abnormal ankle kinematics 39 have been reported for this technique. Reconstruction is recommended as a primary surgical approach if the quality of the remaining ligamentous tissue is insufficient for direct repair or if the patient has general joint laxity. 42 Different surgical procedures are available to reconstruct the lateral ankle ligaments, with similar clinical outcomes and biomechanical stability. 1,5,8,24,37,38
A commonly used reconstruction technique entails a gracilis graft and 2 bone tunnels through the fibula, 12,24 and good clinical outcomes with this method have been reported previously. 24 However, despite the lack of published data, personal experiences in our clinic have shown intraoperative complications while tensioning the graft; namely, the bone bridge between the 2 tunnels was vulnerable to breakage in some patients. To avoid this complication, a technically less demanding operation procedure using only 1 fibular bone tunnel was proposed. 13 However, no studies are available on the biomechanical characteristics of this new reconstruction technique to assess ankle stability. Normal ankle kinetics and kinematics are essential to achieve good clinical outcome and normal function of the ankle. 6,21
The aim of this study was to conduct a biomechanical comparison of reconstruction of lateral ankle ligaments using 2 fibular bone tunnels 12,24 versus 1 fibular tunnel 13 versus ankles with intact and transected lateral ligaments. We hypothesized that the changes in stiffness and laxity between the intact and the reconstructed ankles do not differ significantly between the two reconstruction techniques.
Methods
Specimens and Preparation
This study was granted approval from the local ethics committee. The study used 10 Thiel-conserved cadaveric ankle specimens with an average age of 81.5 years (range, 67-92 years) and 10 gracilis tendon grafts. The specimens were provided blinded from the Institute of Anatomy of the University of Zürich. All specimens had intact lateral and medial ligaments and tibiofibular syndesmosis. No specimen presented a criterion of exclusion, such as abnormal anatomic feature of the ankle (eg, malformation), signs of previous operation, or injury of the ligaments.
Before testing, the ankles were carefully dissected to expose the lateral ankle ligaments. The soft tissue of the lower leg was dissected to leave the distal shaft of the tibia, 15 cm above the ankle joint, bare for mounting. Of the 10 ankle specimens, 8 were paired, whereas 2 were unpaired. Equal numbers of the paired specimens were assigned to one of the 2 reconstruction groups (using either 1 or 2 fibular tunnels). The unpaired specimens were randomly assigned to 1 of both groups. Both groups consisted of 5 specimens and had similar age distribution.
A biomechanical investigation of each specimen was performed in 3 stages (Figure 1): with intact, transected, and reconstructed lateral ankle ligaments (anterior talofibular ligament [ATFL] and calcaneofibular ligament [CFL]).

Consort flowchart. ADT, anterior drawer test; MAT, maximum applicable torque; TTT, talar tilt test.
Surgical Procedures
After testing of intact and transected states, ankle joints were reconstructed by either the 1-tunnel or 2-tunnel technique, which are explained below (see the Appendix, available as supplemental material, for more detailed explanation). Both reconstruction techniques used gracilis allografts and interference fit screws (Megafix B 6 × 19 mm, 2870619 B; Karl Storz GmbH & Co KG) to fix the grafts in the talar blind-ended tunnel and the calcaneal blind-ended tunnel.
1-Tunnel Technique
For the 1–fibular tunnel technique, 13 the following steps were executed sequentially:
A 5–mm thick gracilis allograft was prepared by reinforcing stitches on each end. An approximate graft length of 10 to 15 cm was needed. The graft was kept irrigated by Thiel solution to maintain its tissue properties.
A blind-ended tunnel with a diameter of 5 mm and a depth of 20 mm was drilled at the talar insertion of the ATFL, perpendicular to the talus, midway between the superior and inferior borders of the lateral talar wall.
The graft was inserted in the talar blind-ended tunnel using a guide wire.
The graft was fixed into the talus by an interference fit screw.
The fibular tunnel with a diameter of 5 mm was drilled from the origin site of the ATFL from anterior to posterior through the fibula, beginning 1 cm proximal from the distal tip and routing almost horizontally to posterior. The posterior end of the tunnel lies approximately 1 cm proximal and 1.5 cm posterior from the CFL insertion site.
The graft was passed from anterior to posterior through the fibular tunnel (Figure 2B).
The calcaneal tunnel was drilled 5 mm wide, from postero inferior to the peroneal tubercle and inferior to the peroneal tendons to the medial side of the calcaneus while sparing the sural nerve.
The graft was adapted in length and passed superficial to the peroneal tendons through the calcaneal tunnel from lateral to medial.
The graft was tensioned manually as in clinical routine with the foot held in neutral position and secured by an interference fit screw in the calcaneus.
2-Tunnel Technique
The reconstruction technique using 2 tunnels into the fibula 12,24 was performed as with the 1–fibular tunnel technique, differing only in steps 5 and 8:
5. The first tunnel drilled into the fibula was 5 mm in diameter and ran from the former insertion site of the ATFL directed posteriorly and proximally (about 30°). The graft was passed from anterior to posterior through the first tunnel. The second tunnel was drilled distally to the first one and ran almost parallel to it, so its exit point was directly at the CFL insertion site. A bridge of 5 mm with cortical bone separated the 2 tunnels, so the tunnels would not break while the graft was tensioned at the end. The graft was passed through the second tunnel from posterior to anterior (Figure 2A).
8. The graft was passed underneath the peroneal tendons into the calcaneal tunnel, running from lateral to medial.

Schematic images of the reconstruction techniques. (A) Reconstruction with 2 fibular tunnels. (B) New reconstruction method using 1 fibular tunnel. From Wirth SH, Renner N, Weigelt L. Wenn Stabi-Programme nichts mehr helfen. Sportphysio. 2016;4(3):112-118. ©2016 Georg Thieme Verlag KG. Reprinted with permission.
Biomechanical Testing Setup
A universal testing machine (Zwick 1456; Zwick GmbH & Co KG) was used. The ankle specimens were held in a specially designed testing setup (Figure 3). For each test, the distal shaft of the tibia was rigidly mounted on the testing machine by cylindrical clamping with screws pointing from all sides into the bone, leaving the fibula to articulate freely. The foot was fixed on a wooden footplate using 2 screws into the calcaneus and a tight strap running over the metatarsal heads. The height of the tibia attached to the testing machine was adjusted so that the ankle specimens were in an unloaded or loaded state for the stress tests, as defined by the protocol (described below).

(A) Biomechanical testing setup consisting of different translation and rotation elements. The ankle specimens were mounted on the testing setup to the footplate with a strap running over the metatarsal heads and 2 screws fixed the calcaneus (not visible) and mounted by cylindrical clamping of the tibia to the z-rotatory element, which was connected to the testing machine. Flexion occurred around the frontal y-axis, internal and external rotation around the longitudinal z-axis, and inversion and eversion around the sagittal x-axis. Anterior translation occurred along the sagittal x-axis, medial-lateral translation around the frontal y-axis, and craniocaudal translation along the longitudinal z-axis. (B) The cadaveric foot was mounted on a customized testing setup with markers on the bone segments and cameras assembled around the setup (1 camera visible, arrow).
The footplate was mounted on top of the testing setup. The setup allowed motion of the ankle in all directions except for plantarflexion and dorsiflexion, which were constrained and could not be changed during test runs, as in the study protocols of Bahr et al. 1,2 The anatomic axes of the ankle joint were determined as defined by the recommendations of the International Society of Biomechanics. 41 Neutral position was defined as the position where the tibia was mounted vertically relative to the horizontally lying footplate. The relative position of the bone segments was defined to be 0 in this neutral position. Before each test repetition, the foot was placed in neutral position under visual control. To minimize errors resulting from minimally varying neutral positions, 3 test repetitions were performed. Repetitive testing of the ankles without damaging the ligamentous tissue was possible by using rather small external loads compared with the reported loads to failure of the ATFL. 8,38
3-Dimensional Optical Assessment Method
During the application of external loads and moments on ankle specimens, the relative movements of the tibia, fibula, talus, and calcaneus were measured by a 3-dimensional optical tracking system (Optitrack; Natural Point Inc). Spherical retroreflective markers with a diameter of 6 mm were fixed to each bone with conventional wood screws. We used 5 cameras mounted around the testing setup to track marker displacements using infrared light. Motion capture data were gathered and labeled in Motive (NaturalPoint Inc) and exported to Visual3D (C-Motion Inc). All markers were assigned to their respective bone segments, which were then visualized using anatomic bone models. Relative 6 degrees of freedom displacement of the segments was calculated. These data were exported to Matlab (MathWorks Inc) and were further analyzed using a custom-made script that identified the data peaks captured at the different applied forces and moments.
Testing Sequence and Data Recording Analysis
To assess the biomechanical characteristics of the ankle joint with intact, transected, and reconstructed lateral ligaments, we used different stress tests, namely the anterior drawer test (ADT), the talar tilt test (TTT), and the maximum applicable torque (MAT) in inversion. The testing sequence was adapted from the protocol in the Bahr et al 1,2 studies of biomechanics of the anterior drawer and talar tilt test 1 and of ankle ligament reconstruction, 2 using the same forces and moments, but repeating the tests in different flexion angles as described below.
The ADT and TTT were performed in an unloaded state, simulating clinical examination of the ankle and minimizing stability arising from articulate surface contact 36 through axial loading, therefore providing more information about ankle stability arising from lateral ligaments.
For the ADT, a precision spring scale (Macroline 0-10 kg; Pesola AG) was attached to the footplate and used to manually apply anterior translation forces of 10, 20, 30, 40, and 50 N sequentially. 1,2 The tests were performed in 0°, 10°, and 20° of plantarflexion, because the ATFL is the primary restraint in plantarflexion of the ankle, 10 and were repeated 3 times. The displacement of the talus and calcaneus in relation to the tibia along the sagittal axis (posterior-anterior movement) was calculated, as well as the internal rotation of the talus and calcaneus around the longitudinal axis of the tibia.
For the TTT, a torque wrench with included torque meter (Tohnichi Mfg Co Ltd) was attached to the footplate and served to apply inversion torques of 1.1, 2.3, and 3.4 N·m sequentially. 1,2 The calibrated torque meter was equipped with a memory needle, which retains the highest torque reading applied. The tests were performed in 0°, 10°, and 20° of dorsiflexion, because strain in CFL increases in dorsiflexion, 10 and were repeated 3 times. The displacement of the talus and calcaneus in relation to the tibia along the longitudinal axis was analyzed. The talar tilt angle (ie, the angle in the frontal plane between the ankle mortise of the tibia and the talar dome) was calculated, as was the calcaneal tilt angle.
Talotibial and calcaneotibial laxity and stiffness are used to describe ankle stability in this study. Laxity was defined as the displacement occurring below the minimum threshold of measurable force and torque detection (<1 N and <0.2 N·m, respectively). The forces or moments were noted as a linear function of their corresponding displacement data, and a linear regression was used to describe this function. Laxity was defined as the x-intercept, whereas stiffness was defined as the slope of this linear function. Laxity in this study is relative to the neutral position at the beginning of each test repetition, which was assessed visually.
An inversion stress test with a maximum applicable torque to failure was performed on the reconstructed ankles with an axial load of 375 N, simulating a lateral ankle sprain with partial load bearing during early recovery after reconstruction. This test also simulated the typical mechanism of injury of lateral ankle sprains as an inversion trauma. 17 An inversion stress was applied on the ankles in 0° of flexion by the torque wrench with a manually, continuously increasing amount of torque. The MAT was recorded on the torque meter when either the ligament reconstruction failed or a maximal torque of 12 N·m was reached without failure. The value of this maximal applicable torque, the location and type of failure, and the talar tilt angle were recorded.
Statistical Analysis
This multilevel experiment was analyzed using mixed linear models based on diagonal covariance for repeated measures using a restricted maximum likelihood method. 35 In a first model, validity of the data was checked, confirming the functional anatomic characteristics of the upper ankle joint. 9 The effect of the different angles of plantarflexion and dorsiflexion and the effect of ligament dissection and subsequent reconstruction were assessed in this first model containing these 2 factors (no interaction term) as fixed effects, and test repetition was modeled as a random effect. For outcomes with a significant response to ligament condition (intact, transected, or reconstructed), Bonferroni-corrected post hoc tests were used to compare the outcome at intact versus transected state, transected versus reconstructed state, and intact versus reconstructed state. This allowed a direct comparison of 2 different ligament conditions. For subsequent analyses, the 3 test repetitions per factor level were summarized by extracting respective median values.
A second mixed linear model compared the 2 reconstruction techniques to the intact state while controlling for the effect of flexion angle. This second model enabled a direct comparison of the outcomes of the 1- and 2-tunnel techniques. The effects of reconstruction were reported with estimated marginal means and associated standard error. The talar and calcaneal tilt angle and failure torque at MAT were compared between the 2 reconstruction techniques through use of the Mann-Whitney U test.
Where not otherwise specified, mean and standard deviation are reported. Statistical analysis was conducted with SPSS (IBM SPSS Statistics for Windows, Version 25.0). The level of statistical significance was set to α = .05.
Results
Anterior translation of the talus or calcaneus relative to the tibia ranged from 4.10 to 12.10 mm over all ligament conditions when 50 N was applied during the ADT. When 3.4 N·m of torque was applied during the TTT, talotibial and calcaneotibial tilt angle ranged from 0.46° to 12.20° (Appendix Table A1). In contrast, internal rotation of the talus and the calcaneus during the ADT with 50 N ranged from –2.07° to 1.74°. Longitudinal displacements ranged from –3.80 to 0.5 mm during the TTT with 3.4 N·m. No further statistical analysis was conducted to assess internal rotation during the ADT and longitudinal displacement during the TTT.
Sagittal Laxity and Stiffness
Different ligament conditions had a significant effect on sagittal ankle stability. Sagittal laxity increased and sagittal stiffness decreased significantly when lateral ankle ligaments were transected, independent of the angle of plantarflexion (Figure 4, Table 1, and Appendix Table A3). Neither reconstruction technique restored tibiotalar sagittal laxity to the intact state, but both techniques restored calcaneotibial stability to the intact state.
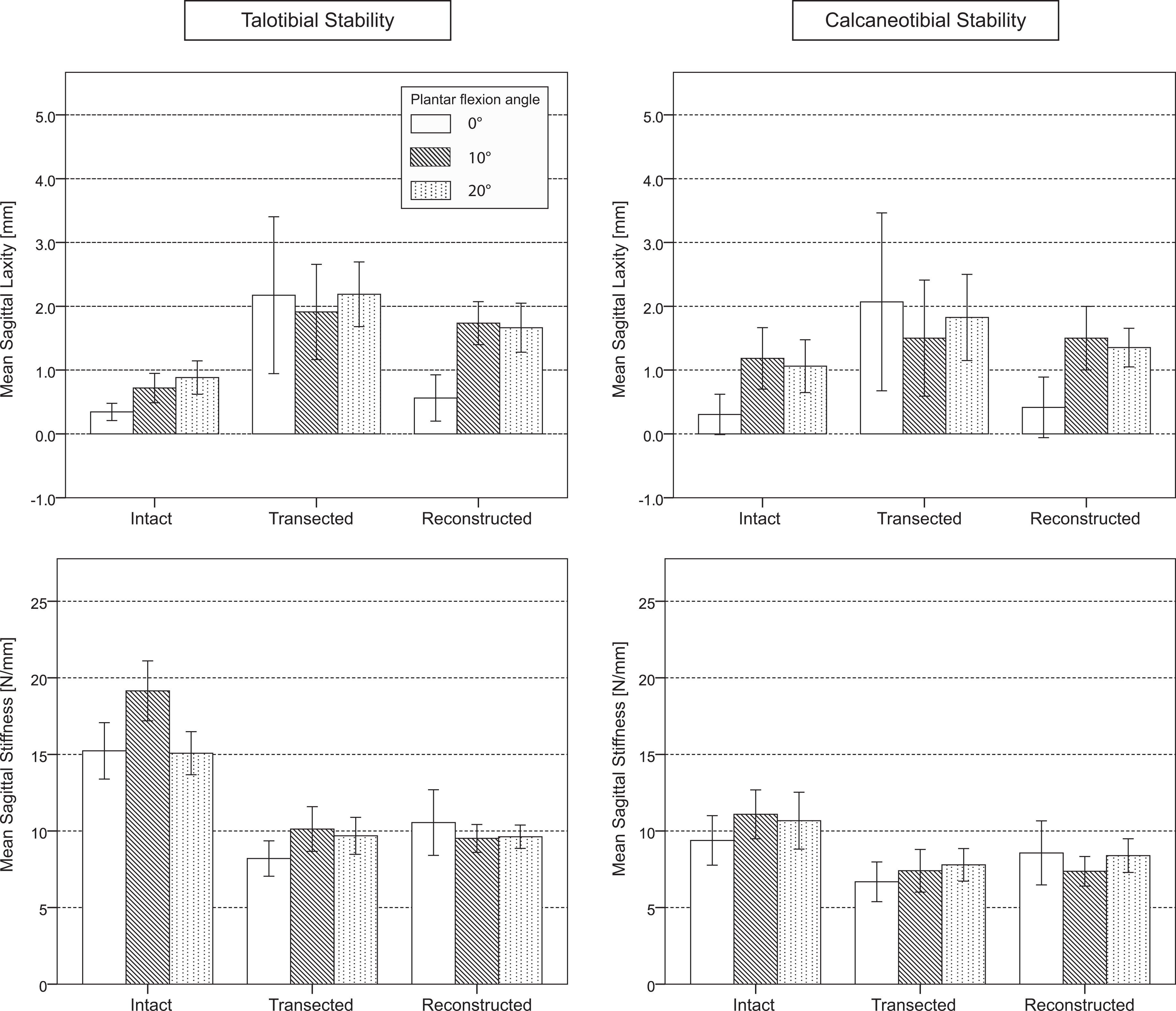
Mean talotibial and calcaneotibial sagittal laxity and stiffness and corresponding SE for different angles of plantarflexion and for different ligament conditions.
Mixed Linear Model for Comparison of the Factor Ligament Condition for 2 Levels Only a

aP < .05 indicates a significant effect of different ligament conditions on ankle stability. Only outcomes with significant effect over all 3 ligament conditions (Appendix Table A3, available as supplemental material) were further analyzed with a Bonferroni-corrected post hoc test.
With increasing plantarflexion angle, increasing sagittal laxity was described (Figure 4 and Appendix Table A3). When comparing talotibial versus calcaneotibial sagittal stability, we observed similar trends.
Tilt Angle Laxity and Stiffness
We found neither a significant difference in tilt angle laxity between the reconstructed and intact states nor a statistically significant difference in tilt angle laxity between the transected and reconstructed states (Figure 5 and Appendix Table A3). The different ligament conditions significantly changed talotibial tilt angle stiffness (Figure 5, Table 1, and Appendix Table A3), with a significant decrease after lateral ligaments dissection. Talotibial tilt angle stiffness of the reconstructed ligaments showed no significant difference when compared with the intact ligaments.
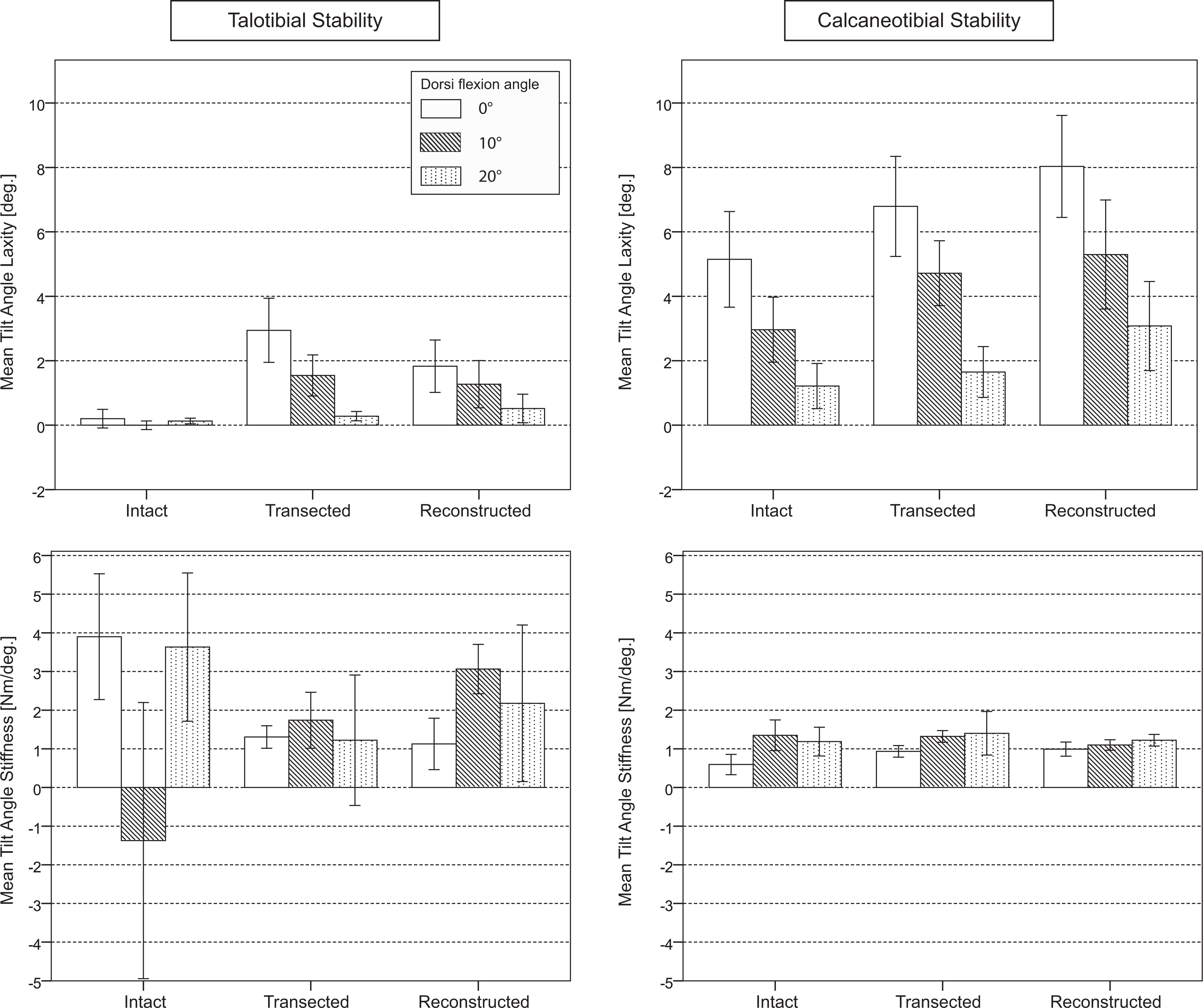
Mean talotibial and calcaneotibial tilt angle laxity and stiffness and corresponding SE for different angles of dorsiflexion and different ligament conditions. The negative value of mean talotibial tilt angle stiffness in 10° of dorsiflexion was interpreted as an outlier due to a measurement error from noise.
Dorsiflexion angle had a significant effect on calcaneotibial tilt angle stability and talotibial tilt angle stiffness (Figure 5 and Appendix Table A3). A decrease in stability was observed when the ankle was held in greater angles of dorsiflexion.
Comparison of Reconstruction Techniques
When comparing the difference in ankle stability from reconstructed to intact ligaments, we found that the 2 reconstruction techniques did not differ significantly in sagittal stability or talotibial tilt angle stiffness (Table 2 and Appendix Figures A3 and A4).
Second Mixed Linear Model for Comparison of 1-Tunnel Versus 2-Tunnel Reconstruction While Controlling for the Effect of Flexion Angle a

a The table shows the estimated marginal means and SEs of the difference of the outcomes from reconstructed to intact ligaments (rounded up to 2 decimals) and corresponding P value for comparison between the 2 reconstruction techniques.
Maximal Applicable Torque
Because of technical issues, 2 specimens of the 2-tunnel group could not be tested for MAT. Namely, when 375 N of axial load was applied, the ankles tilted in eversion and the bony congruence of the joint fixed them in this position even when torque was applied in inversion. Therefore, these 2 ankles were excluded from the MAT analysis.
When we compared reconstruction techniques using 1 versus 2 fibular tunnels, we found no significant differences in failure torque (median, 12.0 N·m [range, 2.0 to 12.0 N·m] vs 11.4 N·m [3.4 to 12.0 N·m], respectively; P = .690) or talotibial failure tilt angle (median, 5.2° [range, –1.9° to 12.7°] vs –0.8° [–1.1° to –0.1°], respectively; P = .250) during the MAT test. The reconstruction failure mode was always a loosening of the reconstruction, which occurred because of loosening from its bony attachments and tunnels, and from an increase in length of the allograft tendon. No rupture of allograft tendons was observed.
Discussion
Reconstruction with 1 fibular tunnel did not significantly differ from the 2-tunnel method regarding differences in sagittal ankle stability and talotibial tilt angle stiffness in intact ankle ligaments. The maximal applicable torque in inversion and corresponding talar tilt angle also did not significantly differ between the reconstruction techniques. In the 2-tunnel group, 2 specimens had to be excluded from MAT analysis because the ankles tilted in eversion when axial load was applied. This probably originated from a slightly, laterally deviated sagittal axis of the ankle while the foot was mounted to the footplate, shifting the pivot point too laterally and therefore causing an eversion tilt with axial load.
Numerical comparison with other biomechanical studies is limited, because other studies used different testing protocols, flexion angles, and axial loads than those used here. 8,38 Still, the comparison among the 2 techniques of interest in this study remains valid. This study is the first biomechanical evaluation of a 1–fibular tunnel reconstruction technique using allografts compared with the intact ligament state and compared with a standard reconstruction procedure with 2 fibular tunnels and allograft. We demonstrated that the 1-tunnel technique restored ankle stability to a level noninferior to the 2-tunnel technique. Although using only 1 fibular tunnel, this technique is technically less demanding in our experience and has a lower risk of bone tunnel failure during graft tensioning.
Another important result was that talotibial sagittal stability was not restored completely to the level of intact ligaments by either reconstruction technique. For example, talotibial sagittal laxity increased significantly (Appendix Figure A4 and Table A3) from approximately 0.3 mm with intact ligaments to 2 mm with dissected ligaments in the neutral position. Talotibial sagittal laxity decreased again to approximately 0.6 mm after ligament reconstruction with either reconstruction method (Figure 4). A 0.3-mm difference in laxity in the intact state for the 2-tunnel method compared with a 1-mm difference in laxity in the intact state for the 1-tunnel method (Table 2), in relation to the absolute values of 0.3 mm with intact and 2 mm with dissected ligaments, is remarkable but still not significant. This could partly arise from the nonanatomic reconstruction of the CFL in the 1-tunnel technique. But given that the 2-tunnel technique did not restore talotibial sagittal stability either, other reasons must exist. A lack of tension of the graft owing to breaking out of the posterior fibular bone bridge could partly account for the increase in laxity, as observed while applying MAT in inversion. Further studies are needed to investigate this question. Still, a significant difference in the laxity of transected ligaments was shown after reconstruction, which means that the ankle stability of reconstructed ligaments lies somewhere in the range between the stability of intact and transected ligaments.
The motion capture data of anterior translation of the talus to the tibia during the ADT with 50 N and of tilt angle during the TTT with 3.4 N·m (Appendix Table A1) showed similar results as reported in previous studies. 1,24,27,30 In the current study, talotibial displacement of reconstructed ankles during the ADT with 50 N was 6.58 mm in neutral position. Jung et al 24 showed a displacement of 4.5 mm in a clinical evaluation of the 2-tunnel reconstruction using stress radiographs during the ADT. Bahr et al 1 used the peroneus brevis tendon as an autograft for the 2–fibular tunnel technique and reported 6 mm of talotibial displacement during the ADT with 50 N in a cadaveric biomechanical study. Because laxity in the current study was defined as the displacement occurring below the minimum threshold of measurable force or torque detection (<1 N or <0.2 N·m, respectively) and not as a force between 50 and 150 N or as a specified range of torque, 1,27,30 laxity values of intact and transected ligaments in this study were notably smaller only by definition.
In contrast, internal rotation during the ADT and longitudinal displacement during the TTT were not further analyzed, because their magnitude was too small and not in a range of previous reports. 2 Marker placement on the talus was rather close, because anatomically the talus is fitted tightly in the ankle joint and only a few bony parts are accessible for marker placements. This affected the motion capture in internal rotation and longitudinal displacement, resulting in small values that were additionally exceeded by noise from the motion capture. Stability of the 1-tunnel technique concerning internal rotation during the ADT and longitudinal displacement during the TTT therefore could not be investigated.
The nonanatomic course of the CFL reconstruction, originating on the posterior fibular side, is a drawback of the 1-tunnel technique. In the past, nonanatomic techniques were used to reconstruct the lateral ankle ligaments by redirecting 1,14 or splitting the peroneus brevis tendon. 7 Because these techniques resulted in altered ankle kinematics 1,32 (eg, restricting hindfoot motion), their use was abandoned. But even with this nonanatomic course, stability similar to that of the anatomic reconstruction with 2 fibular tunnels was demonstrated. The allograft is routed superficial to the peroneal tendons in the 1-tunnel technique while running deep to the tendons in the 2-tunnel method. This could result in mechanical irritation of the peroneal tendon sheath in the 1-tunnel technique. Further clinical investigations regarding possible peroneal tendinopathies from different allograft routing are necessary.
In this study, an experienced foot and ankle orthopaedist operated on the ankle specimens and tensioned the grafts of the reconstructions manually, as done in his clinical routine. A high degree of initial graft tensioning of the CFL reconstruction has been reported to cause abnormal ankle kinematics and laxity. 34 Graft tensioning was not controlled objectively in this study, which replicates the clinical routine of surgical ankle ligament reconstruction but could risk abnormal ankle kinematic values and laxity.
This study describes a detailed approach for measuring bone displacements with a 3-dimensional optical motion capture system and thus enables broad application of this system in biomechanical studies. For example, Goetz et al 19 assessed ankle syndesmotic stability during stress tests on ankles using a similar motion capture system.
As expected from an in vitro experiment, the contribution of muscle strength and proprioception to ankle stability, as well as the effect of tissue remodeling and healing, could not be evaluated in this study. Nevertheless, this study provides important biomechanical information about both reconstruction techniques and about the kinetics of the ankle with intact and transected lateral ligaments. However, the clinical outcome of both reconstruction techniques has not yet been described and should be of future interest.
Limitations
The ankles and gracilis grafts used in this study were embalmed in Thiel solution due to limited availability of fresh-frozen specimens in Switzerland. Reports have stated that Thiel-embalmed tendons present lower failure stress compared with fresh-frozen tendons. 15,29 Despite this, we can make conclusions about the relative stability of both reconstruction techniques compared with intact ankles, because both reconstruction techniques were tested on specimens with the same properties of embalmed tissue; additionally, no failure of allograft tendon was observed in this study.
An a priori sample size calculation was not performed because of a lack of available estimates on clinically relevant effect sizes in the primary outcomes. The limited availability of specimens restricted our sample size to 10. Therefore, it is possible that no significant difference between the reconstruction methods was detected because of the small sample size, leading to an increased possibility of type II error.
The mean age of the ankle specimens used for this study was higher than the mean age of patients typically undergoing ankle ligament repair or reconstruction (81.5 years vs 21.5 years 33 to 36.5 years 24 ). This age difference could result in a higher stability of ligament reconstruction among younger patients with expectedly higher bone density and better tissue healing, so this study possibly underestimates ankle stability after reconstruction. Still, the comparison across reconstruction methods in this study holds, because both groups had a similar age distribution and all specimens showed normal anatomic characteristics of the lateral ankle ligaments.
Conclusion
Both reconstruction techniques improved sagittal laxity and stiffness, as well as tilt angle stiffness from the transected state, but neither technique restored ligament stability to the intact state. No significant difference in ankle stability was seen between the 1–fibular tunnel method and the standard 2–fibular tunnel reconstruction method in a Thiel-conserved cadaveric biomechanical model. Further clinical studies investigating the clinical outcomes of the 1-tunnel reconstruction technique are needed.
Supplemental Material
Supplemental Material, DS_10.1177_2325967120959284 - Biomechanics of Ankle Ligament Reconstruction: A Cadaveric Study to Compare Stability of Reconstruction Techniques Using 1 or 2 Fibular Tunnels
Supplemental Material, DS_10.1177_2325967120959284 for Biomechanics of Ankle Ligament Reconstruction: A Cadaveric Study to Compare Stability of Reconstruction Techniques Using 1 or 2 Fibular Tunnels by Martina Gautschi, Elias Bachmann, Camila Shirota, Tobias Götschi, Niklas Renner and Stephan H. Wirth in Orthopaedic Journal of Sports Medicine
Footnotes
Acknowledgment
The authors acknowledge PD DrMed Norman Espinosa for performing the surgery using 1 fibular tunnel with his clinical expertise as an experienced foot surgeon, Beda Rutishauser for his mechanical expertise in developing the test setup, Prof. Dr Jess Snedeker for his expertise in orthopaedic biomechanics and continuous support from the very beginning of this study, and Prof. em. Christian Gerber and Prof. DrMed. Mazda Farshad for their orthopaedic expertise and leadership throughout the study.
Final revision submitted April 15, 2020; accepted April 29, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: The bioabsorbable interference screws used in this study were donated from Karl Storz SE & Co KG. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the regional ethics commission of Canton Zürich (ref No. 2016-01289).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.