
Abstract
Background:
While the majority of retears of the rotator cuff occur in the early postoperative period, some tears occur several years after repair. The risk factors associated with late retears have not been studied.
Purposes:
To evaluate the frequency of retears in the late postoperative period after primary rotator cuff repair (RCR) compared with that in the early postoperative period and analyze various demographic and radiologic factors associated with late-period retears.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
Among 2463 patients who underwent RCR from 2011 to 2017, 485 patients were diagnosed with rotator cuff retears using magnetic resonance imaging at a single institution, and 345 patients sustained a retear at ≤6 months (group E) or >2 years after repair (group L). To reduce the selection bias, propensity score matching (PSM) was performed using age, sex, and initial mediolateral (ML) tear size. The association between demographic factors, including smoking (non/current/ex), diabetes mellitus (DM, noncontrolled/uncontrolled), and radiologic factors, including initial tear size and late-period retear, were analyzed.
Results:
Group E had 314 (91%) and group L had 31 (9%) patients. Multiple regression analysis using the Firth method after PSM identified that controlled DM (odds ratio [OR], 4.42; 95% CI, 1.06-18.39; P = .04) and uncontrolled DM (OR, 8.81; 95% CI, 1.82-42.55; P = .007) were associated with late-period retear. Using the receiver operating characteristic curve, the group was divided into groups A (≤ cutoff) and B (> cutoff) based on the cutoff value (2.75 cm) of the ML size. Multiple regression analysis was performed in each group, revealing that current smoking (OR, 8.68; 95% CI, 1.35-55.67; P = .02) and uncontrolled DM (OR, 13.60; 95% CI, 1.88-98.46; P = .01) were significantly associated with late-period retear in group A.
Conclusion:
Although the incidence was lower than that in the early period after RCR, retears also occurred >2 years after RCR. Compared with early-period retears, DM was significantly associated with late-period retears. In addition, the risk of late-period retear was high among patients who were current smokers and those with uncontrolled DM in the presence of a small-sized ML tear.
As the incidence of primary rotator cuff repair (RCR) continues to increase, the number of postoperative retears is also on the rise.2,7,13,18 Retears after RCR are most commonly reported to occur in the early postoperative period, between 6 weeks and approximately 6 months, but they have also been reported to occur in the late postoperative period.14,30 In a study analyzing the incidence of retears over time after RCR, findings revealed that retears occurred in approximately 36% of patients within 6 months and in approximately 16% of patients after 2 years. 30
Various factors affect retear rates.16,28,31,37 Previous studies have demonstrated that patient factors such as advanced age, smoking, osteoporosis, and diabetes mellitus (DM) are associated with a high risk of retear.6,8,9,31 In addition, radiologic factors such as mediolateral (ML) tear size and fatty infiltration of the supraspinatus and infraspinatus have been reported to be associated with postoperative cuff healing.15,28 However, most studies that have analyzed risk factors for retear have assessed cuff integrity in the early postoperative period or have not specifically defined a period. Therefore, risk factors associated with retears occurring in the late postoperative period have not been reported.
Although studies have reported that retears occur most frequently in the early postoperative period,12,29 few studies have evaluated the incidence of retears occurring in the late postoperative period. Additionally, retear rates have been reported to vary widely.2,12,27 Therefore, in this study, we evaluated the frequency of retears in the late postoperative period after primary RCR compared with that in the early postoperative period and analyzed various demographic and radiologic factors associated with late-period retears.
Methods
This retrospective case-control study examined the correlation between various risk factors and rotator cuff retear after arthroscopic RCR. Informed consent was obtained from all patients, and final approval was obtained from the institutional review board.
Patient Selection and Methods
Among 2463 patients who underwent RCR by a single senior surgeon (Y.-G.R.) at our institution between 2011 and 2017, patients diagnosed with retears using magnetic resonance imaging (MRI) were retrospectively reviewed. Patients were instructed to undergo MRI at 6 months and 2 years after surgery to assess post-RCR integrity. Retears were evaluated according to the classification by Sugaya et al. 38 Types 4 (minor discontinuity) and 5 (major discontinuity) were defined as retears. The inclusion criteria were as follows: (1) patients with retears confirmed by MRI ≤6 months after RCR and (2) patients with retears confirmed by MRI 2 years after RCR (no retears confirmed by MRI or ultrasonography >6 months and ≤ 2 years) (Appendix Figure A1), as well as (3) patients without trauma history after RCR. The exclusion criteria were as follows: (1) patients with MRI- or ultrasonography-confirmed retear >6 months after surgery and ≤2 years; (2) an initial partial repair that did not completely cover the footprint; (3) previous shoulder surgery on the ipsilateral side; and (4) no preoperative MRI. After applying the inclusion and exclusion criteria, 345 patients were enrolled in the analysis during the study period (Figure 1).

Flow diagram of patient enrollment. MRI, magnetic resonance imaging; RCR, rotator cuff repair.
In previous systematic reviews and meta-analyses that analyzed retear rates according to time points after RCR, the most frequent time for retears after RCR was 3 to 6 months after surgery, and retears have been reported even 24 months after surgery. 30 Based on this, patients with MRI-confirmed retears were divided into 2 groups according to the period: those whose retears occurred ≤6 months after surgery (group E, early postoperative period) and those whose retears occurred >2 years later (group L, late postoperative period).
Demographic Data
The following demographic variables assessed 1 day before surgery were compared between groups E and L: age, sex, side, body mass index, smoking status, alcohol consumption, work level, stiffness, DM, hyperlipidemia, and thyroid disease. Smoking status was categorized as a nonsmoker, current smoker, and former smoker. 21 The work level was classified as low (sedentary), medium (less physical activity), or high (heavy) according to the degree of manual labor. 22 Stiffness was assessed by passive range of motion and was defined as forward flexion 40°, external rotation at 20°, and internal rotation 5 spine level less than to the contralateral side. 20 DM was categorized on the basis of glycated hemoglobin (HbA1c) measured ≤1 month before surgery as controlled (HbA1c level <7.0%) or uncontrolled (HbA1c level ≥7.0%). 20
Radiologic and Intraoperative Data
All radiologic parameters compared between groups E and L were evaluated independently and in a blinded manner by 2 orthopaedic surgeons (M.S.K. and S.H.S.) including initial ML and anteroposterior (AP) tear size, fatty infiltration, 10 and occupation ratio 27 of each rotator cuff muscle; critical shoulder angle 33 ; and acromiohumeral interval. 34 Tear size was measured using T2-weighted MRI images, and fatty infiltration and occupation ratio were evaluated based on a Y-shaped view of T1-weighted oblique sagittal MRI images. The intraoperative data included arthroscopic/open repair, the technique (single row/suture bridge), biceps long head tendon procedure (intact/tenotomy/tenodesis/augmentation), and subscapularis repair.
Operative Techniques and Rehabilitation
All RCRs were performed by a single senior author (Y.G.R) as a standard procedure with the patient in the beach-chair position under general anesthesia and/or interscalene block. The torn rotator cuff was sufficiently mobilized to minimize the tension on the repair construct, and the original footprint of the greater tuberosity was prepared. Depending on the tear size, the number and location of anchors were determined to achieve maximal strength in the repaired rotator cuff. Conventional single-row RCR was performed through the antegrade passage; for the suture bridge RCR, a horizontal mattress suture was placed to form a medial row, and the suture limb was then bridged over the tendon and fixed laterally. For the open repair, deltoid splitting was performed using a superolateral approach.
Postoperative immobilization was performed using an abduction brace for 4 weeks. Single-plane exercises were conducted within the scapular plane, limited to a level tolerable for pain over the subsequent 2 weeks. Active-assisted motion exercises commenced 6 weeks postoperatively.
Statistical Analysis
The Mann-Whitney U test, Wilcoxon signed-rank test, and chi-square or Fisher exact tests were used to compare demographic variables and radiologic parameters. Any significant predictive values in the univariate analysis were included in the multiple logistic regression analysis to identify independent factors associated with late-period retear. To reduce the bias of the binary outcome analysis that may occur when the number of events is small (rare) or when the difference in sample numbers between groups is large, multiple regression with the Firth penalized likelihood method was used. In addition, receiver operating characteristic (ROC) curves were used to calculate the cutoff value of initial ML tear size, and based on this, the study population was divided into group A (≤cutoff value) and group B (>cutoff). Subgroup analysis was performed to analyze the effect of late-period retears according to the initial ML tear size. To reduce selection bias in groups E and L, propensity score matching (PSM) was performed using age, sex, and initial ML tear size. After PSM matching, an analysis was conducted to ascertain whether differences were present in independent factors associated with late-period retears compared with those before matching. Moreover, a subgroup analysis (groups A and B) was also performed. Significance was set at P = .05, with associated 95% CIs. The SPSS software package (Version 21.0; IBM Corp) was used for all statistical analyses. Post hoc power calculations were performed using R software (Version 4.0.3). The interobserver reliability of the radiologic parameters was determined using intraclass correlation coefficients (ICCs) with a 2-way random effects model and Cohen kappa statistic (К). An ICC of <0.01 was determined to be poor; 0.01 to 0.2, slight; >0.2 to 0.4, fair; >0.4 to 0.6, moderate; >0.6 to 0.8, good; and >0.8 to 1.0, excellent. 25 A К value of 1.0 was determined to be perfect agreement; >0.80 to 1.0, excellent agreement; >0.60 to 0.80, good; >0.40 to 0.60, moderate; >0.20 to 0.40, fair; and ≤0.2, poor. 25 A priori analysis performed using G*Power (Version 3.1.9.7; Heinrich-Heine-Universität Düsseldorf) indicated that the required sample size was 66 patients; thus, the sample size in this study was sufficient to achieve a power of >0.80.
Results
After RCR, 9% (n = 31) of the included retears occurred in the late period and 91% (n = 314) occurred in the early period. The mean time from surgery to the diagnosis of the retear was 29.4 ± 6.0 months in group L and 4.1 ± 1.7 months in group E (P < .001). In univariate analysis, group E was significantly older (P = .01) and had larger tear sizes (ML and AP; all, P < .001) than group L. Group L had a higher proportion of current smokers and DM than group E (P = .044 and P < .001, respectively). The demographic and radiological data of groups L and E are presented in Table 1.
Demographic, Radiologic, and Intraoperative Data for Groups E and L a

Data are presented as mean ± SD or n (%) Values with a P value less than 0.05 are displayed in bold. AHI, acromiohumeral interval; BMI, body mass index; CSA, critical shoulder angle; DM, diabetes mellitus.
The interobserver ICCs for the radiologic data ranged from good to excellent as follows: 0.86 for the initial ML tear size, 0.81 for the initial AP tear size, 0.76 for critical shoulder angle, and 0.88 for acromiohumeral interval. The rotator cuff muscle occupation ratios were also rated as good to excellent: 0.93 for the subscapularis, 0.94 for supraspinatus, 0.71 for infraspinatus, and 0.72 for teres minor. The K values for fatty infiltration between the independent observers were also rated good to excellent: 0.93 for subscapularis, 0.83 for supraspinatus, 0.85 for the infraspinatus, and 0.77 for teres minor muscles, respectively.
Factors Associated With Late-Period Retears
PSM matching is described in Table 2.
PSM Matching (1:4) With Age, Sex, and Initial ML Tear Size a

ML, mediolateral; PSM, propensity score matching; SMD, standardized mean difference.
The difference between the propensity scores of two units.
In multiple logistic regression analysis using the Firth method, current smokers (odds ratio [OR], 4.47; 95% CI, 1.31-15.27; P = .02), uncontrolled DM (OR, 11.92; 95% CI: 3.02-47.02; P < .001), and initial ML tear size (OR, 0.91; 95% CI, 0.83-0.99; P = .03) were significantly associated with late-period retear. After PSM matching using age, sex, and initial ML tear size to reduce selection bias, only controlled (OR, 4.42; 95% CI, 1.06-18.39; P = .04) and uncontrolled DM (OR, 8.81; 95% CI, 1.82-42.55; P < .007) were significantly associated with late-period retear (Table 3).
Multiple Logistic Regression Analysis With Firth Method a
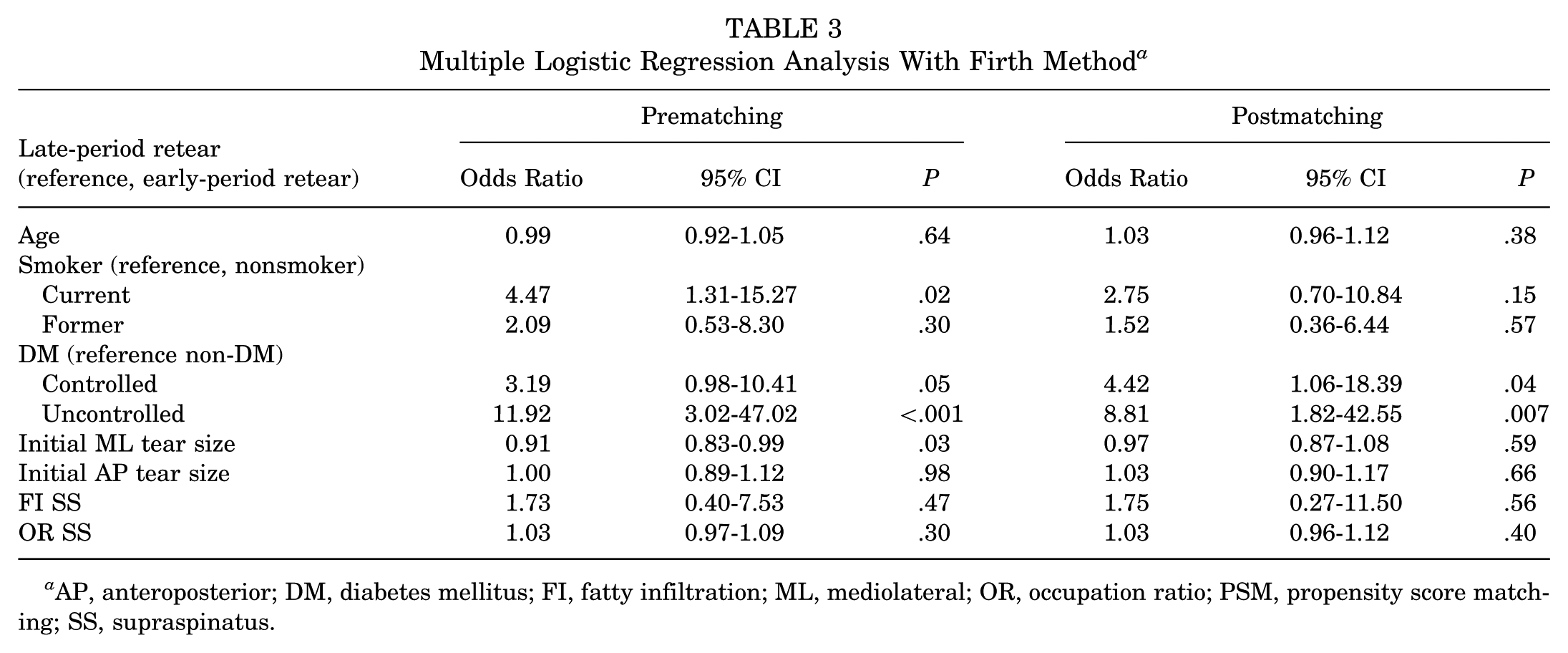
AP, anteroposterior; DM, diabetes mellitus; FI, fatty infiltration; ML, mediolateral; OR, occupation ratio; PSM, propensity score matching; SS, supraspinatus.
Post hoc power analysis was conducted using the proportion of patients with uncontrolled DM, which demonstrated a significant difference. The power of this study was 0.962 with an alpha error of .05.
Furthermore, to evaluate whether differences exist in the risk factors affecting late-period retears according to ML tear size, the cutoff value of ML tear size was calculated using the ROC curve. The area under the curve was 0.779, and the cutoff value with the highest sensitivity (77.4%) and specificity (69.1%) was 2.75 cm. Based on this, multiple logistic regression analysis using the Firth method was performed using the same factors for each subgroup in groups A (≤2.75; n = 90) and B (>2.75; n = 38) in the post-PSM matching data. In group A, current smoking (OR, 8.68; 95% CI, 1.35-55.67; P = .02) and uncontrolled DM (OR: 13.60; 95% CI, 1.88-98.46; P = .01) were significantly associated with late-period retears. For group B, only current smoking status was significantly associated with retear (P = .04) (Table 4).
Subgroup Multiple Logistic Regression Analysis With Firth Method of Late Retear Based on Cutoff Value for ML Tear Size a

Group A, ≤2.75 cm; Group B, >2.75 cm.
AP, anteroposterior; DM, diabetes mellitus; Inf, infinity value; FI, fatty infiltration; ML, mediolateral; OR, occupancy ratio; SS, supraspinatus.
Discussion
In the patients with rotator cuff retear included in this study, approximately 90% of the retears were diagnosed ≤6 months after repair and approximately 10% were diagnosed >2 years after surgery. In the post-PSM matching analysis, controlled and uncontrolled DM were associated with late-period retears, and patients with uncontrolled DM were approximately 9 times more likely to develop late-period retears than those without DM. In addition, subgroup analysis based on the cutoff value of the initial ML tear size (2.75 cm) demonstrated that not only uncontrolled DM but also current smoking, which was not significant in the overall data, had an effect on late-period retears. especially in group A (ML tear size ≤2.75 cm).
The majority of retears after RCR occur 3 to 6 months after surgery.14,32 In a multicenter prospective study, Iannotti et al 14 reported that retears occurred predominantly between 6 and 26 weeks after RCR. Miller et al 32 reported that retears occurred most frequently in the early postoperative period within 3 months after RCR in patients with large-to-massive rotator cuff tears. However, retears manifesting in the late period are considered to be rare. 11 In a previous systematic review and meta-analysis, retears after RCR occurred in 16% of patients at 24 months after RCR. 30 However, only a few studies have reported the frequency of retears in the late period. Furthermore, the studies included in the systematic review and meta-analysis that reported retears 24 months after surgery only performed MRIs at a single point in time, making it unclear whether the retear occurred after 24 months or whether the MRI performed 24 months after surgery detected an earlier retear.3,23 In this study, patients who had retears detected via MRI or ultrasonography between 6 and 24 months were excluded; approximately 90% of retears occurred in the early period and 10% occurred in the late period after primary RCR.
Previous studies have reported several risk factors for retears. However, most studies utilized MRI performed ≤1 year after RCR to confirm cuff integrity,4,5,15,29,35 which can be evaluated as a risk factor for retears occurring in the early period. Cho et al 5 evaluated the integrity of RCR after the primary procedure using MRI within 6 months of surgery and reported that hyperglycemia at the time of surgery was a risk factor for retears. In addition, factors such as smoking status, degree of retraction of the torn tendon, occupation ratio of the rotator cuff muscle, and fatty infiltration have been reported as risk factors for early-period retears.15,19,40 However, no studies have evaluated the risk factors associated with late-period retears. Uzun et al 39 analyzed risk factors for retears using MRI performed between 3 to 24 months after RCR but did not stratify retears into early versus late periods. In the present study, the factors affecting late-period retear were evaluated and compared with those affecting early-period retear by dividing the patients into groups with retear ≤6 months (group E) and >2 years (group L). After PSM matching to reduce bias, the risk of late-period retears was identified to be high in patients with controlled and uncontrolled DM.
Previous studies have reported that a hyperglycemic environment increases proinflammatory cytokine levels, causing persistent inflammation in tendons.12,24 In addition, it has been reported that impaired angiogenesis, one of the long-term complications of DM, leads to a decrease in vascular supply to tendons,1,17 which may affect retear that occurs in the late period after RCR. However, because there is no study analyzing the mechanism by which DM affects late-period retear, preclinical and clinical studies are needed to investigate this in the future.
Previous studies have demonstrated that the risk of retear increases with increasing ML tear size.26,31,36 In this study, the ML tear size of patients with early-period retear was significantly larger than that of patients with late-period retear. However, according to the subgroup analysis based on the cutoff value of the ML tear size, current smoking had an effect on late-period retears along with uncontrolled DM, especially in patients with a small tear size (group A). In particular, the effect of smoking on late-period retears according to ML tear size was significantly higher in group A than that in group B. Based on the results of this study, it can be inferred that even in patients with a small ML tear size, the risk of late-period retear may increase due to current smoking and uncontrolled DM. In the case of uncontrolled DM, no significant interaction was observed between groups A and B, which is considered to be because of the small number of patients in group B; this should be investigated in further studies.
Limitations
This study had several limitations. First, because this study was designed retrospectively, serial MRI evaluations could not be performed to confirm whether retear occurred after 2 years. Therefore, it may be difficult to determine whether retear occurred in the late period or before the 2-year period and symptoms only developed later. A prospective study evaluating retear through MRI at multiple time points is needed in the future. Second, patient demographic data (diabetes control, smoking status, etc) that may have changed during the follow-up period were not reflected in the analysis. Third, although the sample size was small, the number of patients with late-period retears was lower than that with early-period retears; and the number of patients in group B was insufficient, which may result in a type II error. Further studies should be conducted with a large number of patients in the group with a large ML tear size (group B). Fourth, as no previously reported cutoff value for ML tear size was present, we used the ROC curve to establish the cutoff value. As this cutoff value was determined based on the data of the current study, it may differ from the value used in the clinical field. Fifth, as this study compared retears that occurred in the early period within 6 months and the late period (after 2 years), only relevant patients were selected and analyzed. The results of patients with retears between 6 months and 2 years need to be further investigated.
Conclusion
Although the incidence was lower than that in the early period after RCR, retears also occurred >2 years after RCR. Compared with early-period retears, DM was significantly associated with late-period retears. In addition, in the presence of a small-sized ML tear, the risk of late-period retear was high among patients who were current smokers and those with uncontrolled DM.
Footnotes
Appendix
Final revision submitted July 17, 2025; accepted August 1, 2025.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Kyung Hee University Hospital at Gangdong (KHNMC 2024-02-025).