
Abstract
Background
Rotator cuff tears can result in pain which can be debilitating. The etiology of failed repair or retears is multifactorial. Multiple risks factors were proposed, with critical shoulder angle (CSA) being one of the factors of emerging interest. Other radiological parameters including glenoid inclination (GI), lateral acromial angle (LAA), and acromial index (AI) were also suggested for a possible correlation.
Methods
A retrospective review of 397 rotator cuff repairs on January 1, 2000 to December 31, 2023 recruited from two major hospitals was carried out. Primary outcome measure of radiographic shoulder angles (CSA, GI, LAA, and AI) was measured.
Results
There is no statistical difference in radiographic shoulder angles measured in the rotator cuff retear group and the no retear group. Retear patients were more likely to have Goutallier grade 3 and 4 (p = 0.01). Goutallier grade 4 was the potential predictor of retear regardless of sex (Odds ratio=5.25 (1.38, 20.02); p = 0.02).
Conclusion
There is no definite association of rotator cuff retear and radiographic parameters including CSA, GI, LAA, and AI in this study.
Introduction
Rotator cuff tears are present in a significant portion of population, resulting in pain and disability. It can result in a loss of range of movement, decreased strength, and increased function limiting pain, which can be debilitating especially to the active or younger group of patients. Many opt for surgery due to progressive symptoms not controlled with conservative means. It is estimated that 75,000 rotator cuff surgeries are performed annually in the United States, with the number on increasing trend. 1 Rotator cuff retears after repair is reported to be 11% to up to 94% in literature. 2 Compared with primary rotator cuff repair, revision is more difficult and less effective, rendering surgeons to opt for other operative means such as superior capsular reconstruction or arthroplasty in some cases.
The etiology of rotator cuff tendinopathy, failures of repair, or retears is multifactorial and not completely understood. Risks factors including sociodemographic, preoperative characteristics, radiological findings, and intraoperative findings were proposed and reviewed. 3 Some studies looking specifically at radiological parameters correlate a higher CSA to rotator cuff tears and retears after repair.2–8 CSA is one of the factors of emerging interest. It is measured between a line connecting superior and inferior margins of glenoid, and another line connecting inferior margin of glenoid with inferolateral aspect of the acromion in true anteroposterior view of shoulder. Biomechanical studies have shown that an increase in CSA is correlated to increased compression and shear forces of the shoulder and rotator cuff, potentially overloading the supraspinatus tendon.9,10 However, this correlation was also met with skepticism.11,12 Some studies explored the correlation of primary cuff tear or cuff disease and other radiological parameters including GI, 13 LAA, and AI. 14 However, convincing data is lacking.
Existing studies focus on various parameters being potential risk factors in different population demographics for primary rotator cuff tears or retears after repair. This study is a retrospective review aiming to perform analysis with more comprehensive radiographic parameters on a large-scale cohort of patients who have follow-up for 24 years from the southern region of China. This study attempts to identify whether CSA and other reported radiographic shoulder parameters including glenoid inclination (GI), lateral acromial angle (LAA), and acromial index (AI) are associated to a higher risk of retear after rotator cuff repair in a large sample size with patients of a similar background and demographic.
Method
A retrospective review was performed, reviewing rotator cuff repairs done on January 1, 2000 to December 31, 2023 at two major hospitals. Ethical approval had been received from local ethics committee (Ref. No.: 2025.169). Informed consent had been sorted from every patient. A total of 401 cases with rotator cuff repairs were generated through the Clinical Data Analysis and Reporting System (CDARDS) using the International Statistical Classification of Diseases and Related Health Problems (ICD-10) for rotator cuff repair on July 1, 2024. Three hundred and ninety seven cases were included in the study. Four cases were excluded from analysis, in which one patient was under 18 years old, two patients with surgeries aborted, and one patient with latissimus dorsi transfer done instead of rotator cuff repair.
Primary outcome measures of radiographic shoulder angles (CSA, GI, LAA, and AI) were determined. Secondary outcome measures including patient details, peri-operative injury characteristics, operative details, any retear, subsequent management, and follow-up findings were obtained through medical record reviewing. All measurements were performed by an orthopedic resident and an orthopedic sports specialist separately.
Sample size calculation
We carried out an in-house preliminary comparison of critical shoulder angle (CSA) between patients who suffered from retear and no retear (all were different from the existing patient cohort) before carrying out this study. Given the calculated effect size 0.25, α = 0.05 and power at 0.80, the total sample size was 120 (60 patients in each group).
Statistical analysis
Variables were compared between retear and no retear groups using Student's T-test for numeric variables and Chi square test for categorical variables. Goutallier classification in retear group and no retear group was compared using Chi-square test. Inter-rater reliability and Internal validity were assessed using intraclass correlation (ICC) with 95% confidence interval (CI) and Cronbach's α, respectively. Predictors of cuff retear, namely age, sex (ref: Male), body mass index (BMI)(Ref: Normal), diabetes (Ref: No), activity (Ref: Non-labour work), Goutallier grading (Ref: Grade 0), tear size, initial tear pattern (Ref: Complete), use of augmentation (Ref: No), and type of repair (Ref: Single row) were identified through stepwise multivariable logistic regression modelings, with controlling of confounders where applicable. All statistics were carried out using IBM IPSS 28 (Armonk, NY: IBM Corp). A two-sided p value of ≤0.05 was considered statistically significant.
Results
Basic demographics
Three hundred and ninety-seven patients (236 male and 161 female) with rotator cuff repair done were included in this study. There was no significant difference in retear and no retear group for mean age (58.95 ± 8.69 vs 57.20 ± 10.32, p = 0.21), hand dominance (p = 0.59), BMI (numeric (p = 0.69) and categorized (p = 0.89)), smoking status (p = 0.33), diabetes mellitus (p = 0.40), activity (p = 0.40), and side of injury (p = 0.88) (Table 1). There was a statistically significant difference in sex, with females more likely to have a rotator cuff retear after repair. The retear rate was 15.6% (n = 61; p = 0.02).
Basic demographics of patients in the two groups.
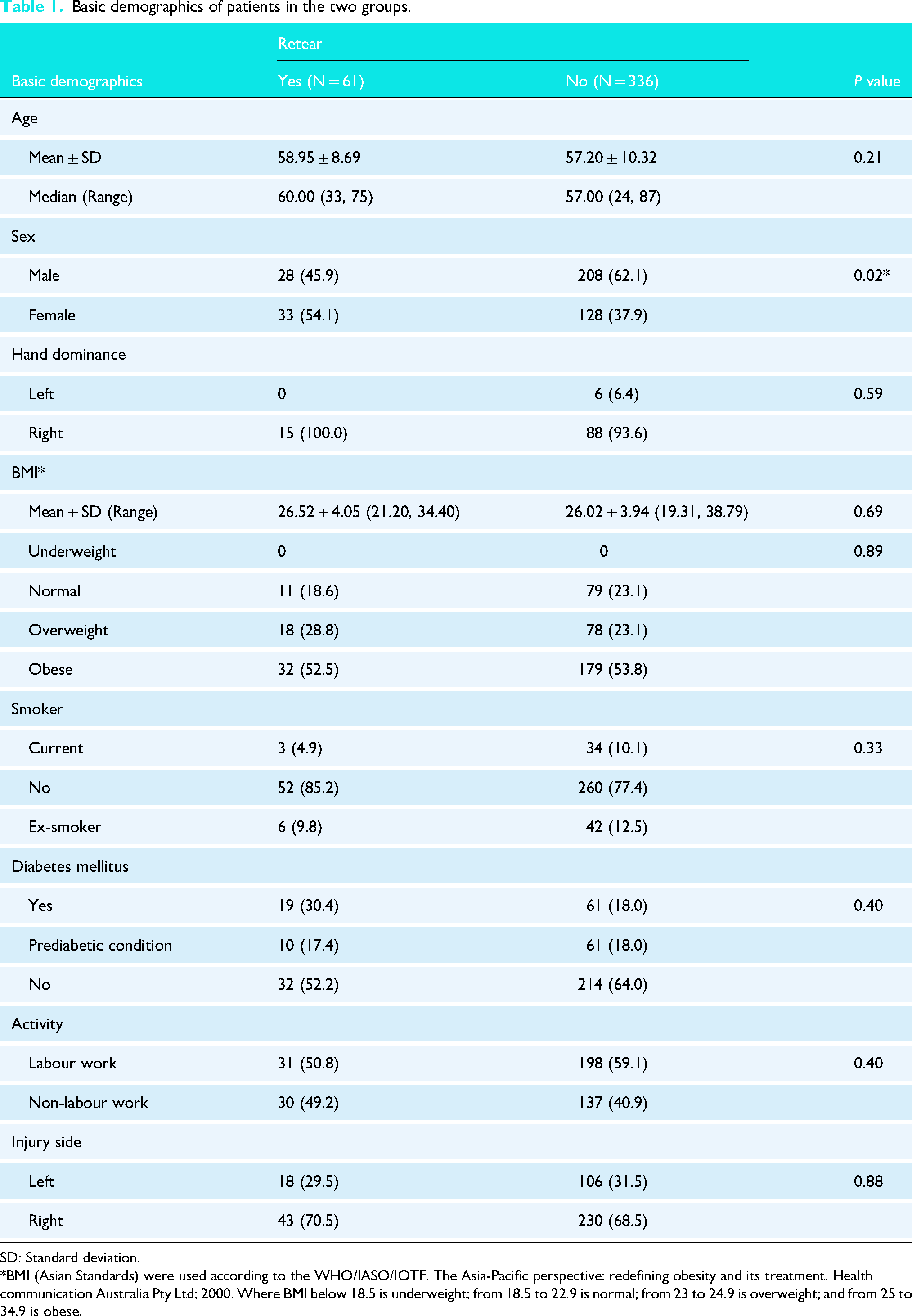
SD: Standard deviation. *BMI (Asian Standards) were used according to the WHO/IASO/IOTF. The Asia-Pacific perspective: redefining obesity and its treatment. Health communication Australia Pty Ltd; 2000. Where BMI below 18.5 is underweight; from 18.5 to 22.9 is normal; from 23 to 24.9 is overweight; and from 25 to 34.9 is obese.
Pre-operative characteristics
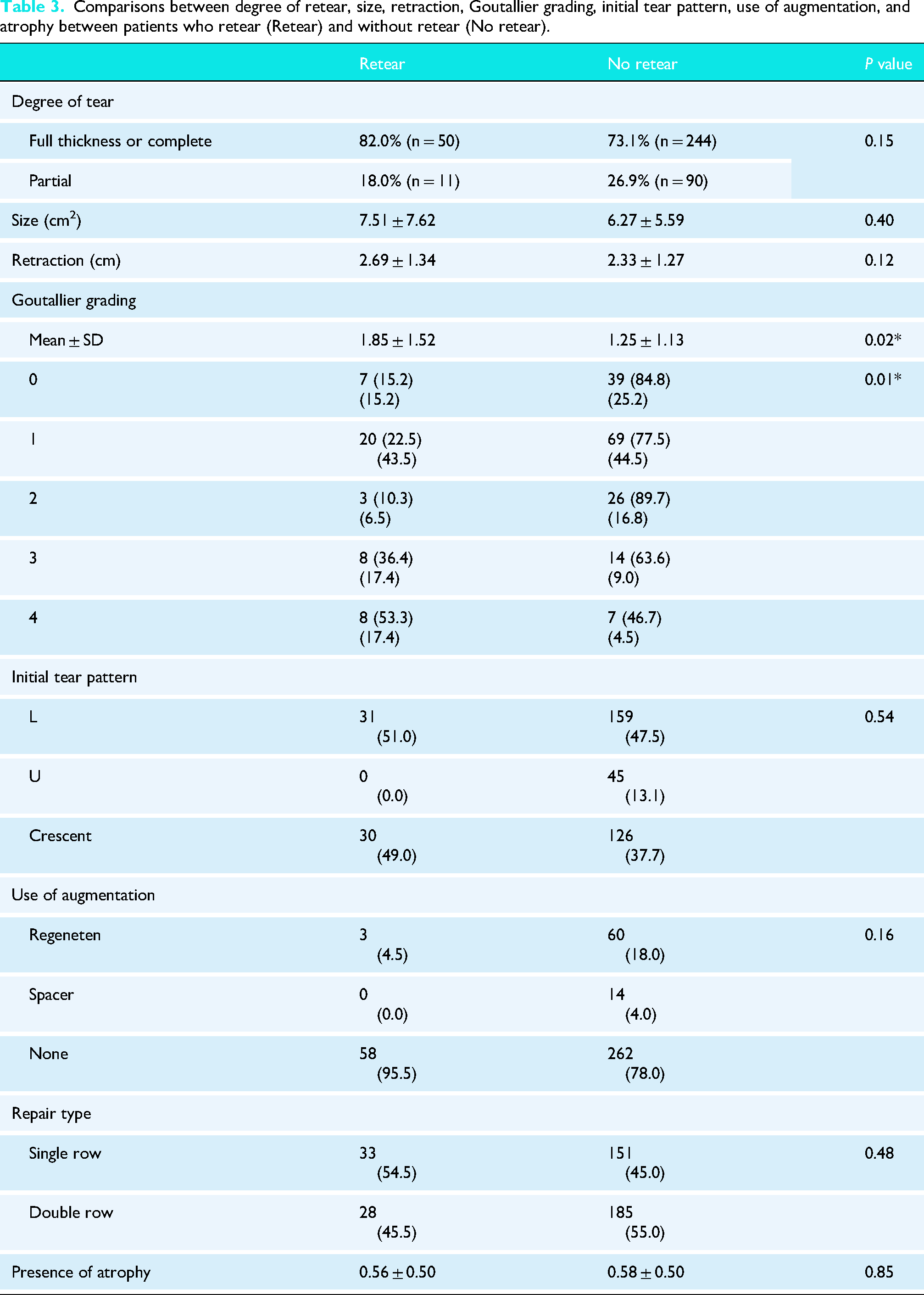
There was a total of 61 patients with rotator cuff retear. About 69.8% (n = 277) patients had a single tendon tear, 27.2% (n = 108) patients had two tendons involved, and 3.0% (n = 12) patients had more than three tendons involved. About 82% (n = 50) patients were documented to have complete or full thickness tears, while 18.0% (n = 11) with partial thickness tear, with no statistical difference in retear and no retear group. Further subgroup analysis for complete and full thickness tear also showed no statistical difference (p = 0.31).
CSA, GI, LAA, and AI showed no statistical difference in both groups (Table 2). There was no statistical significance in intraclass correlation (ICC) and Cronbach's α between measurements of orthopedic resident and orthopedic sports specialist in all radiographic measurement variables.
Comparisons between degree of retear, size, retraction, goutallier, and atrophy between patients who retear (retear) and without retear (no retear).
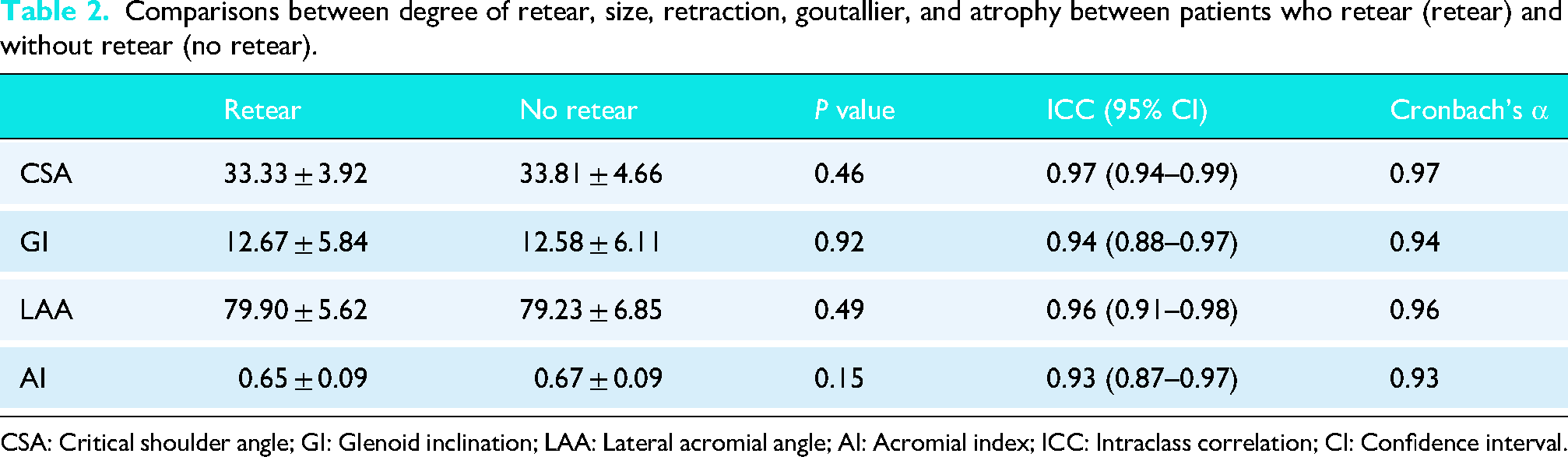
CSA: Critical shoulder angle; GI: Glenoid inclination; LAA: Lateral acromial angle; AI: Acromial index; ICC: Intraclass correlation; CI: Confidence interval.
Goutallier grading was found to be statistically different in the two groups, higher in retear group (1.85 ± 1.52 vs 1.25 ± 1.13, p = 0.02) (Table 3). Further classifications on Goutallier grading showed that grading was found to be significantly higher (Grade 3 and 4) in retear group (34.8% combined) than no retear group (13.5% combined) (p = 0.01). There was no statistical difference in size (p = 0.40), retraction (p = 0.12), initial tear pattern (p = 0.54), and atrophy (p = 0.85) in both groups.
Comparisons between degree of retear, size, retraction, Goutallier grading, initial tear pattern, use of augmentation, and atrophy between patients who retear (Retear) and without retear (No retear).
Independent predictors of retear
Results from crude regression models (Model 1 series) showed sex (Female) (Odds ratio = 1.95 (1.11, 3.35); p = 0.02) and Goutallier grade 3 (Odds ratio = 3.27 (1.07, 10.66); p = 0.04) and 4 (Odds ratio = 6.53 (1.79, 23.81); p < 0.01) were potential predictors causing retear (Table 4). After controlling for sex, Goutallier grade 4 was still found to have statistical significance (Odds ratio = 5.25 (1.38, 20.02); p = 0.02). Goutallier grade 3 was not statistically significant after controlling for sex.
Stepwise logistic regression analysis of retear on different prognostic factors dependent variable: retear yes.
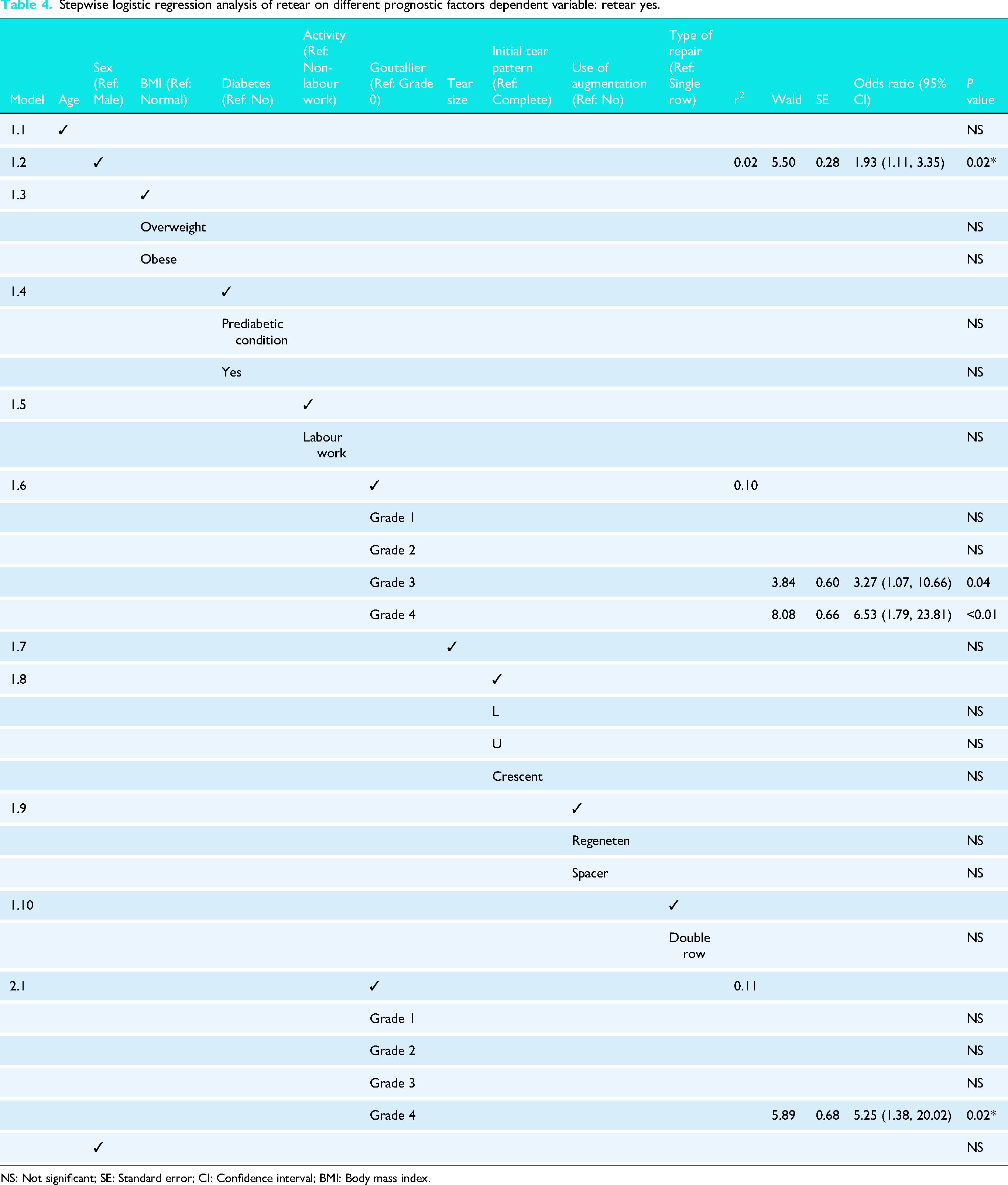
NS: Not significant; SE: Standard error; CI: Confidence interval; BMI: Body mass index.
Operative details
About 99.2% (n = 394) patients underwent arthroscopic, 0.3% (n = 1) mini-open, and 0.5% (n = 2) open rotator cuff repairs. About 46.3% (n = 184) patients underwent single row repair, and 53.7% (n = 213) patients underwent double row repair. About 85.4% (n = 339) patients had subacromial decompressions done. About 19.4% (n = 77) patients had augmentation with Regeneten or spacer. About 18.1% (n = 72) patients had additional procedure done in the same session, including biceps tenotomy and labral repair. There were 1.3% (n = 5) reported cases of complications, including stiffness (0.8%, n = 3), septic arthritis (0.3%, n = 1), and implant pull out (0.3%, n = 1). Whereby the latter two cases required operative intervention.
There was no statistical difference in use of augmentation (p = 0.16) and repair type (p = 0.48) in both groups (Table 3).
Retear
About 15.6% (n = 62) patients were diagnosed with cuff retear. About 19.4% (n = 12) of patients with rotator cuff retear went for revision arthroscopic repair and 6.5% (n = 4) patients opted for reverse shoulder arthroplasty. The remaining patients decided for conservative management.
Of the retear group, 30.6% (n = 19) patients progressed to rotator cuff arthropathy on imaging, whereas in no retear group, 3.2% (n = 11) progressed to cuff arthropathy (p < 0.01).
Follow-up
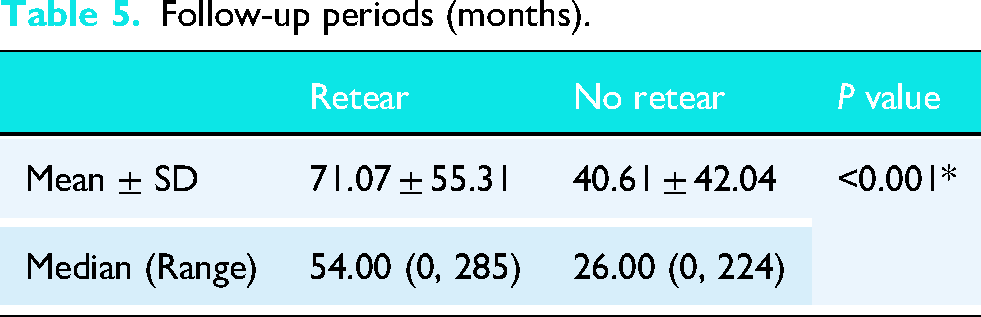
The median follow-up in this cohort was 28 months, with longest follow-up over 23 years (Table 5). Patients with cuff retear had a longer follow-up period than patients without cuff retear.
Follow-up periods (months).
Discussion
It is proposed in literature that an increased critical shoulder angle (CSA) increases shear joint reaction force of the shoulder in biomechanical studies, leading to an increased requirement and mechanical overload on the rotator cuff to stabilize the humeral head.9,10 Risk factors of primary rotator cuff tears were studied in literature, but there was still a lack of consensus on the risk factors of retears of repair after primary rotator cuff repair.
Systematic reviews found significant correlation between higher CSA and retears after rotator cuff repair, all reviews including four studies.3,6–8 Acromial morphology3,15 and glenoid morphology6,8 were reported to have statistically significant correlation with retear rates. On the other hand, there were also reports of insignificant association between rotator cuff repair and bony morphology in shoulder. Retrospective reviews reported no significant correlation in retear and patient reported outcome of repaired rotator cuffs with higher CSA,12,16 acromial morphology,3,5,6,8,17 and glenoid morphology.3,15,17 With the existing literature and conflicting evidence, there is no consensus on the cut off in each variable for an increased risk for retear clinically.
Multiple variables were proposed to be possible risk factors of retear after repair of rotator cuff, including sociodemographic factors (age, BMI, diabetes), radiographic parameters (fatty infiltration), and anatomical factors (tear size).2,3,18 However, other studies were unable to find definite correlation between the above factors,6,15 gender,3,6 and level of activities. 3
In our retrospective cohort study, there is no statistical difference and association of rotator cuff repair with shoulder morphology (CSA, GI, LAA, and AI). Retear patients are found to be more likely to have Goutallier grade 3 and 4. Through logistic regression modeling, Goutallier grade 4 is the potential predictor of retear regardless of sex. It is reported in a systematic review that retear rates are higher after surgical repair of rotator cuff in proportion to pre-operative Goutallier staging. 18
Hollman et al. previously reported comparable clinical improvement with conservative treatment, partial repair and isolated biceps tenotomy or tenodesis as an alternative for rotator cuff tears with Goutallier fatty infiltration grade 2 to 3 due to higher reported retear rates. 19 These alternative surgical options can be further studied for cuff tears with higher retear risk identified in this study, such as Goutallier grade 4, as well as a possible treatment for irreparable massive cuff tears.
Limitations of this study
As this is a retrospective review, the limitation in our study includes bias, incomplete data, quality of radiographs, and lack of standardized follow-up protocols, mostly in the early years included in this study. However, formal documentation has progressively become more detailed and sophisticated in latter half of the study period. The quality of radiograph including X-ray, computed tomography, and magnetic resonance imaging also varied and refined throughout the years, more consistent in the latter study period. Moreover, 79 X-rays (19.9%) were excluded as they were found not on Grashey view to limit measurement errors. Two hundred and one MRIs were retrieved for analysis. There were patients who lost to follow up, and there was no routine imaging done to asymptomatic patients for rotator cuff retear or healing status in asymptomatic patients with those who came back for reassessments, of which, the rates of asymptomatic retear, rotator cuff arthropathy could be under reported. Despite the presence of surveillance bias in the study, the large study cohort may still add to the existing body of literature on rotator cuff prognostication.
With the limitations identified in our study, follow-up protocols, clinical reassessments, and imaging, changes have been implemented in the current practice. While prolonged timespan can lead to heterogeneity, a longer follow-up and a larger database incur strength of prognostication. With changes and standardization happening over the years, we hope our future studies will be able to identify and provide more answers to the current existing evidence. Future studies can include a prospective study with a longer follow-up on various radiological parameters. Standardized rehabilitation protocol, standardized radiographic assessment arm position, routine postoperative clinical reassessments, and shoulder function scores can be implemented to better understand the effect of repaired rotator cuff retear. Other potential aspects of risk factors can also be explored.
Conclusion
Rotator cuff retear after repair is a multifactorial disease including sociodemographic factors, intrinsic biology, anatomical factors, and intraoperative factors. Retear patients are found to be more likely to have Goutallier grade 3 and 4, and Goutallier grade 4 is found to be a potential predictor of retear regardless of sex. Female sex is also found to be associated to higher retear rates. According to our findings, there is no definite association or predictive value for radiographic parameters including critical shoulder angle, glenoid inclination, lateral acromial angle, and acromial index in cases of rotator cuff retear after repair.
Footnotes
List of Abbreviations
Acknowledgments
None.
ORCID iDs
Ethics approval and consent to participate
Ethical approval was obtained from the ethics review board of the Joint Chinese University of Hong Kong—New Territories East Cluster Clinical Research Ethics Committee (Research Ethics Committee Approval Number: 2025.169).
Consent for publication
Written informed consent was obtained from every participant.
Informed Consent
The study was performed in accordance with the Declaration of Helsinki and ICH-GCP. Written informed consent was obtained from all participants.
Authors’ contributions
FOSP (first author): conception, design of the work, acquisition, interpretation of data, drafted the work, and substantively revised. TCHL: acquisition, interpretation of data, drafted the work, and substantively revised. WWC: analysis, interpretation of data, drafted the work, and substantively revised. RWFM: substantively revised. CKW: substantively revised. JPN (corresponding author): conception, design of the work, drafted the work, and substantively revised. MTYO: substantively revised. PSHY: substantively revised. All authors have been given a copy of the manuscript, all have approved the submitted version (and any substantially modified version that involves the author's contribution to the study), and all have agreed both to be personally accountable for the author's own contributions and to ensure that questions related to the accuracy or integrity of any part of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and material
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Clinical trial number
Not applicable.