
Abstract
Background:
Aberrant anterior tibial artery (AATA) is an uncommon variation of the anterior tibial artery. It is an important vascular variation that increases the risk of vascular complications in some knee surgeries (high tibial osteotomy, posterior cruciate ligament reconstruction, etc).
Hypothesis:
The anatomic and morphometric features of AATA remain unclear. The authors hypothesize that the posterior femoral morphology and popliteus muscle-related features may be associated with the presence of AATA.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Between December 2022 and December 2024, knee magnetic resonance imaging (MRIs) were analyzed to detect AATA. Images in which image analysis was not optimal due to artifacts, images of patients with previous surgery around the knee, and patients with vascular malformations in the lower extremity were excluded. A control group was formed through computer-assisted randomization, comprising an equal number of men and women with AATA as patients. The condylar twist angle, posterior condylar angle (PCA), posterior tibiofemoral angle, popliteus sulcus depth (PSD), and PSD/lateral condylar width (LCW) parameters were measured on the MRIs of all patients and recorded for each patient. Patients with AATA variation were scanned for the presence of MRI of the opposite knee outside the time interval determined for the study, and it was analyzed whether patients with opposite knee MRIs had bilateral AATA.
Results:
After applying the inclusion and exclusion criteria, 4075 knee MRIs were analyzed. A total of 78 AATA variations were detected, with a prevalence of 1.91%. The prevalence of AATA was 2.04% in women and 1.78% in men. The PCA was statistically higher in patients with AATA compared with the control group (P < .005). PSD and PSD/LCW were found to be lower in patients with AATA compared with the control group (P = .012, P = .05). The prevalence of bilateral AATA in patients with AATA variation was 48.5%.
Conclusion:
The prevalence of AATA was found to be 1.91%. High PCA, low PSD, and PSD/LCW are radiologic parameters associated with AATA variation. Both the popliteus musculature and posterior femoral morphometry are related to the occurrence of AATA variation.
The popliteal artery passes lateral to the adductor magnus muscle on its way to the distal extremity, passes through the adductor canal, and then obliquely to the distal edge of the popliteus muscle. 5 Anatomic variations of the terminal branching of the popliteal artery are relatively common, occurring in approximately 10% of extremities 11 and limb loss.3,12 Studies in the literature have shown that the popliteal artery may have different variations, such as a high origin of the anterior tibial artery, separation of the vessels above the knee joint, or above the popliteus muscle. 9 One of the variations of the popliteal artery is the so-called aberrant anterior tibial artery (AATA), which is found in 1.9% to 4% of the population according to the cases studied.7,8,10 In this variant, the AATA runs between the popliteus muscle and the posterior tibial cortex. Surgeons performing sports surgery may encounter complications related to AATA variation, especially when performing high tibial osteotomy (HTO) and posterior cruciate ligament (PCL) reconstruction. The risk of popliteal artery injury in HTO ranges from 0.03% to 0.05%, whereas the rate in PCL reconstruction is between6,10 0.5% and 1%. This variant can be detected by autopsy, angiography, ultrasound, and computed tomography angiography studies.9,18 However, apart from these methods, magnetic resonance imaging (MRI) can also be used to identify this variant, although it is not widely reported. 10 MRI appears as an excellent modality because it allows for the complete analysis of the articular, vascular, and soft tissue knee structures, and is included in the majority of presurgical knee evaluations. 13
There are few studies in the literature on the anatomic features, prevalence, and clinical effect of AATA. This study aimed to reveal the anatomic morphological features of patients with AATA variation by comparing them with those of patients with a popliteal artery structure without variation. The authors believe that identifying associated anatomic morphometric parameters will provide a benefit that will increase both the clinical importance and the recognition of ATA.
Methods
This was a retrospective case-control study. Within the scope of the study, the sample size was calculated by power analysis. To determine the required sample size, an a priori power analysis was conducted using G*Power (Version 3.1.9.6). The study was based on the following parameters: a reliability (confidence) level of 95% (α = .05), an expected effect size (Cohen’s d) of 0.75, and a desired power of 90% (1−β = 0.90). Based on these inputs, the minimum total sample size required was calculated to be 78 participants. Additionally, a separate power analysis (Principal Component Analysis) was conducted for the PCA. The effect size (Cohen’s d) was calculated as 0.786, and the resulting statistical power was 0.998.
Data collection for the study commenced after obtaining ethics committee approval from our hospital (No. 2-24-753). The data for the study were collected between December 2022 and December 2024. To enhance external validity, we did not restrict any indications of MRI in the selection of patients. However, for all MRIs examined, we evaluated patient clinical characteristics through the hospital data system. While examining the MRI, evaluations were made in axial, sagittal, and coronal planes. Patients for whom image analysis was not possible due to motion artifacts, those with previous surgery around the knee, and those with a history of vascular surgery in the lower extremity were excluded. A control group, consisting of an equal number of male and female patients as the study group, was formed. MRIs of the patients in the control group were tested similarly to those of the study group, and AATA was not detected. Patients in this study group were randomized using computer-assisted randomization based on the scanned MRIs. MRI images of the normal anterior tibial artery and AATA are shown in Figure 1.

(A) Sagittal PDFS MRI of the normal knee anatomy shows the popliteal artery located posterior to the popliteal muscle. (B) Axial PDFS MRI of the normal knee anatomy shows the popliteal artery located posterior to the popliteal muscle. (C) Sagittal PDFS MRI of the knee shows the AATA between the tibial cortex and the popliteal muscle. (D) Axial PDFS MRI of the knee shows the AATA between the tibial cortex and the popliteal muscle. AATA, aberrant anterior tibial artery; PDFS MRI, proton density fat–saturated magnetic resonance imaging.
To test whether patients with AATA exhibited the same variation in both lower extremities bilaterally, the presence of contralateral knee MRIs was checked in both our hospital's records and the national health record system. The presence of bilateral knee MRIs and whether the variations were also bilateral were recorded separately. Only 1 knee MRI of patients with bilateral AATA variation was used for radiologic measurement.
In patients with bilateral AATA variation, only 1 knee MRI—typically the right side—was used for radiological measurements to avoid duplication and ensure that each patient contributed only 1 data point to the analysis.
The images were acquired on a GE Signa Pioneer 3T scanner with a slice thickness of 2 to 4 mm, a pixel size of 0.57 × 0.57 mm, an echo time of 12.4 msec, and a repetition time of 688 msec. The MRI protocol included acquisitions of proton density fat–saturated weighted images in coronal (TR/TE = 3100/35; echo train length, 8; 3 mm thickness; space between slices 0.5 mm), sagittal (TR/TE = 3300/35; echo train length, 8; 2 mm thickness; space between slices 0.5 mm), axial (TR/TE= 3300/35; echo train length, 8; 3.2 mm thickness; space between slices 0.5 mm), coronal T1-weighted image (TR/TE= 600/12; echo train length, 2; 3 mm thickness; space between slices 0.5 mm), and sagittal T2-weighted images (TR/TE= 4360/90; echo train length, 20; 2 mm thickness; space between slices 0.5 mm). All MRI examinations were reevaluated using the picture archiving and communication system (Extreme PACS) by 2 experienced orthopaedic surgeons (S.A., M.H.O.).
The measurements performed to define the morphometric parameters on MRI are described below. All measurements are shown in Figure 2. The measurements were based on the previous study by Aumann et al 2 on popliteal muscle tendinitis.
Condylar twist angle 2 : The condylar twist angle (CTA) between the anatomic transepicondylar axis and the posterior condylar axis of the femur.
Posterior condylar angle 1 : The posterior condylar angle (PCA) is the angle between the surgical epicondylar axis and the posterior condylar axis of the femur.
Posterior tibiofemoral angle 17 : The posterior tibiofemoral angle (PTFA) between the posterior condylar axis of the femur and the posterior base of the tibia.
Popliteus sulcus depth 2 : The popliteus sulcus depth (PSD) is calculated as the distance from the deepest point detected on coronal sections to the edges of the popliteal sulcus.
Popliteal sulcus depth/lateral condyle width (PSD/LCW) 2 : The width of the lateral condyle is measured at its widest diameter on the T1 coronal section. The measured popliteal sulcus depth/lateral condyle width (PSD/LCW) ratio is found mathematically by proportioning these two values to each other.
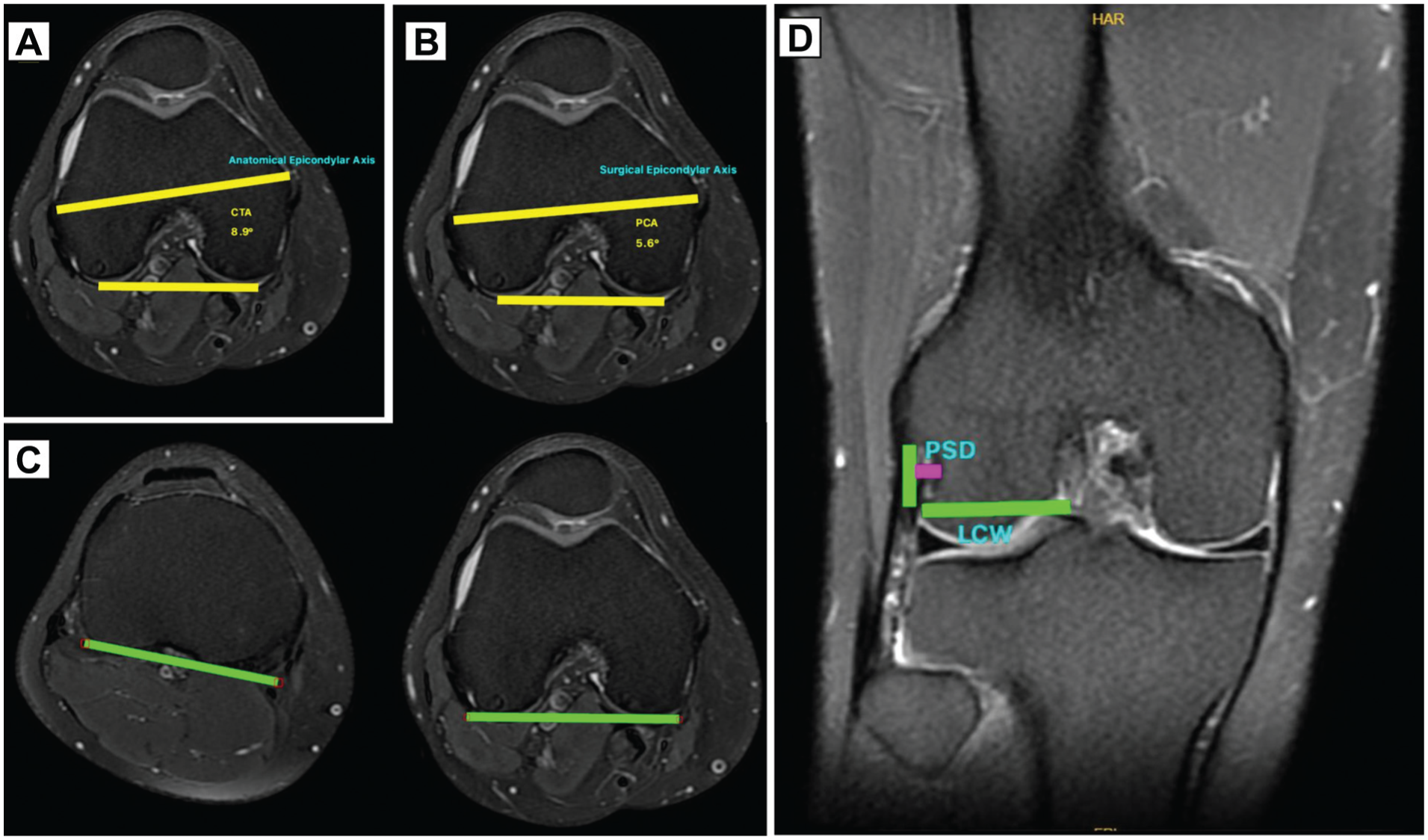
(A) CTA is the angle between the anatomic transepicondylar axis and the posterior condylar axis of the femur. (B) PCA is the angle between the surgical epicondylar axis and the posterior condylar axis of the femur. (C) PTFA is the angle between the posterior condylar axis of the femur and the posterior base of the tibia. (D) PSD is calculated as the distance from the deepest point detected on coronal sections to the edges of the popliteal sulcus. CTA, condylar twist angle; PCA, posterior condylar angle; PSD, popliteus sulcus depth; PTFA, posterior tibiofemoral angle.
All of the measurements mentioned above were performed by 2 different orthopaedic surgeons (A.K., C.C.) who did not have access to the demographic data of the patients. For statistical analysis, the mean values of both measurements were calculated.
Statistical Analysis
Statistical analyses of the study were performed using SPSS Version 26.0 (IBM Inc). The Kolmogorov-Smirnov test was used to determine whether the data exhibited a normal distribution across groups. For continuous variables, mean/median values were calculated. An independent samples t test was used when the normality conditions were met, and a Mann-Whitney U test was applied when normality conditions were not met. Categorical variables were expressed as percentages and frequencies and compared using the chi-square or Fisher exact tests. In all analyses, P < .05 was considered statistically significant.
To evaluate the agreement between the measurements of the 2 groups, the Cohen kappa test was used for categorical variables, and the intraclass correlation coefficient (ICC) score was used for continuous variables. 15
Results
A total of 4075 MRIs were analyzed, including 2020 for male and 2055 for female patients. We detected 78 AATAs. A total of 156 patients were included in the study, including 78 patients in the study group and 78 patients in the control group. In both groups, there were 36 (46.1%) male and 42 (53.9%) female patients. Accordingly, the prevalence of AATA was 1.91%. While the prevalence of AATA in women was 2.04%, this rate was 1.78% in men. There was no statistically significant difference between male and female patients in terms of AATA prevalence (P = .245).
We found that 35 of 78 patients with AATA variation underwent bilateral knee MRI. Of these 35 patients, 18 (51.42%) did not have an AATA variation in the opposite knee.
The mean age was 41.31 ± 11.79 years in the study group and 42.31 ± 13.74 years in the control group. There was no significant difference between the 2 groups in terms of age variables that could affect the results (P = .629).
Data on radiologic measurements obtained from MRIs of patients in the 2 groups are presented in Table 1.
Radiologic Measurement Data of the 2 Groups a

Data are presented as mean ± SD. Bold P values indicate statistical significance. CTA, condylar twist angle; LCW, lateral condyle width; PCA, posterior condylar angle; PSD, popliteus sulcus depth; PTFA, posterior tibiofemoral angle.
The presence of an aberrant artery was examined by 214 2 orthopaedic surgeons using the single-blinded method, and near-perfect agreement was found between the results (Cohen's kappa = 0.935). The ICC score was used for continuous variables, and all values were ≥0.9. The mean ICC score was 0.911, indicating excellent agreement between the results. ICC scores for all radiologic measurements are shown in Table 2.
ICC Scores of Radiologic Measurements in the 2 Groups a
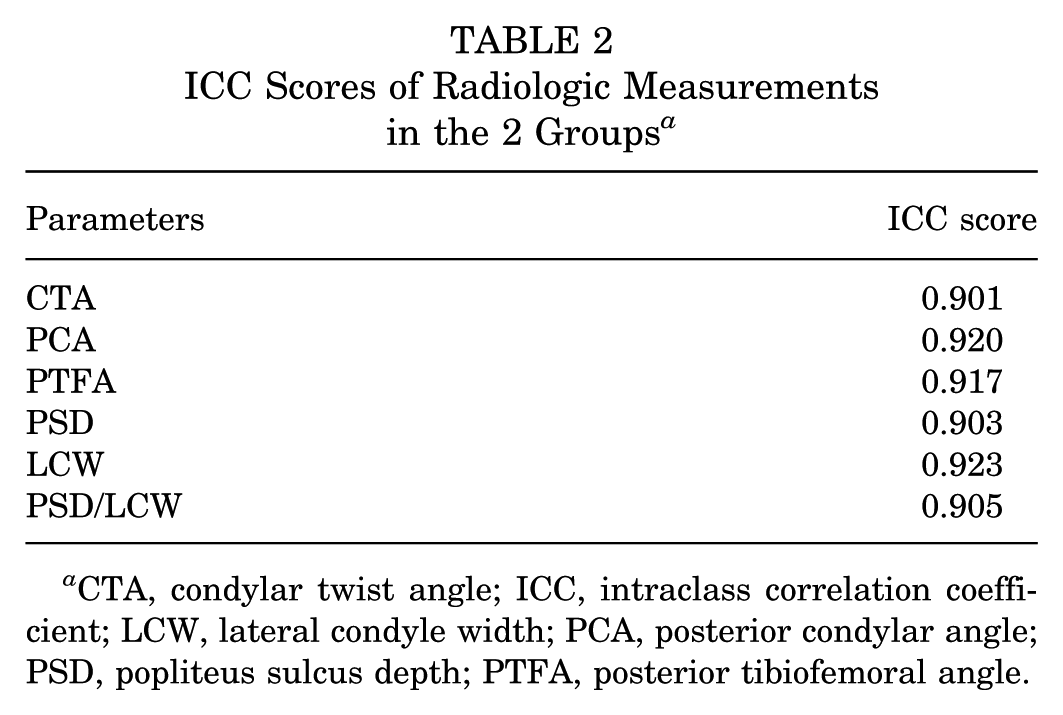
CTA, condylar twist angle; ICC, intraclass correlation coefficient; LCW, lateral condyle width; PCA, posterior condylar angle; PSD, popliteus sulcus depth; PTFA, posterior tibiofemoral angle.
In our study, morphometric measurements of patients with bilateral and unilateral AATA variation were compared. No statistically significant differences were found between the 2 groups in terms of morphometric measurements (P > .05 for all parameters).
Discussion
The most significant finding of this study is that PCA was found to be statistically higher, and PSD and PSD/LCW were found to be lower in patients with AATA variation compared with the control group. In addition, in this study, AATA was detected in the largest number of patients reported in the literature. The prevalence of AATA was found to be 1.91%, and it was observed that the prevalence was higher in women than in men; however, this result was not statistically significant.
Klecker et al 10 retrospectively analyzed 1116 MRIs and found the prevalence of AATA to be 2.1%. Concha et al 13 examined 280 MRIs of 253 patients and found the prevalence of AATA to be 3.2%. Schuster et al 16 also retrospectively reviewed 1589 knee MRIs and found the prevalence of AATA to be 2.1%. In the present study, we examined a significantly higher number of MRIs than those in the existing literature to evaluate the prevalence of AATA. In this study, in which we retrospectively reviewed a total of 4075 MRIs, we found the prevalence of AATA to be 1.91%. Both this study and other studies in the literature show that the prevalence of AATA may differ between populations. In addition to the general prevalence of AATA, our study also evaluated the prevalence of AATA in both the female and male populations—the prevalence was 2.04% in women and 1.78% in men. The prevalence of AATA in women was higher than in men; nonetheless, no statistically significant difference was found (P = .245). We found that 35 of the patients with AATA variation also had MRIs of the contralateral knee, and we evaluated the contralateral knees for the presence of AATA. We could not detect this variation in the contralateral knee of (51.42%) of the patients. This information indicates that AATA is not always visible bilaterally, and we should evaluate each knee separately for AATA, particularly in the preoperative period.
The anatomic and morphometric properties of the AATA have not been clearly demonstrated.7,13 A clearer demonstration of the anatomic and morphometric properties of the AATA will contribute to knee surgeries such as HTO and PCL reconstruction, where the risk of injury to this vascular structure is higher than in other knee surgeries. Schuster et al 16 used both MRI and long-leg radiographs in their study, in which they evaluated whether patients with AATA variation were dependent on patient morphotype. In this study in which they performed a large number of measurements, they could not detect any significant relationship between the parameters and the presence of AATA. In our study, we found that high PCA, low PSD, and PSD/LCW ratio may be associated with the presence of AATA. These parameters were previously associated with popliteus muscle tendinitis in dancers by Aumann et al. 2 This suggests that the presence of AATA may be related to structural variations in the popliteus muscle. Studies indicate that PCA is not constant in all patients and may vary depending on the individual and the pathology of the knee joint. 4 The correlation between PCA and AATA in our study suggests that posterior femoral anatomy and morphometry may also be effective in the occurrence of AATA variation.
Although some surgeons perform the HTO in flexion to prevent vascular injury, this position will not affect the risk of injury to the AATA. A similar injury may occur during the opening of the tibial tunnel in PCL reconstruction.13,14 In total knee arthroplasty, which is one of the most common surgical procedures in orthopaedic practice, AATA injury may occur during placement of the posterior retractor. It is also possible to injure this artery variation depending on the approach used in some types of tibial plateau fractures. 16 Although MRI is routinely used for the detection of PCL injuries, MRI is not routinely used in HTO, total knee arthroplasty and tibial plateau fractures. Therefore, the presence or detection of AATA may be overlooked, and a risk of vascular injury may be encountered. Although the PCA parameter, which we found to be associated with the presence of AATA in our study, could not be detected on direct radiographs, the PSD and PSD/LCW parameters can be evaluated on direct radiographs. In light of the data obtained in our study, a more careful approach can be applied in terms of the presence of AATA by carefully evaluating these parameters in patients undergoing these surgical procedures.
First, the retrospective nature of the study is a limitation. Second, it is a study conducted in a single population and ethnic group. Third, the fact that the measurements are not performed in a 2-dimensional plane and are computer or artificial intelligence-assisted can be considered a limitation. The study's strength lies in its comprehensive review of the largest number of MRIs and analysis of the most extensive dataset of AATA cases among studies evaluating the prevalence of AATA in the literature. Another limitation of the study is its limited ability to assess the effects of demographic variables such as sex and age. Because the use of contrast-enhanced MRI provides a better option for evaluating vascular structures, the use of noncontrast MRIs also poses a limitation.
Conclusion
The prevalence of AATA was found to be 1.91%. High PCA, low PSD, and PSD/LCW are radiologic parameters associated with the presence of AATA. Both the structure of the popliteus muscle and the posterior condyles of the femur are effective in the formation of AATA variation. However, further studies are needed to determine the anatomic and morphometric features of AATA.
Footnotes
Final revision submitted June 12, 2025; accepted July 8, 2025.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Ankara Bilkent City Hospital Medical Research Scientific and Ethical Evaluation Board (2-24-753).