
Abstract
Background:
The use of postoperative bracing after anterior cruciate ligament (ACL) reconstruction remains a topic of debate. Although braces are widely prescribed to enhance joint stability and provide psychological support, their actual impact on functional outcomes, muscle strength, pain, kinesiophobia, quality of life, and return-to-sport (RTS) rates is unclear—particularly in recreational athletes.
Purpose:
To evaluate the effects of postoperative knee brace use on knee function, muscle strength, pain, kinesiophobia, quality of life, and RTS rates over a 12-month period in recreational soccer players who underwent ACL reconstruction.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A total of 50 male recreational soccer players who underwent arthroscopic ACL reconstruction between 2020 and 2023 were included. Postoperative brace use depended on the clinical routines of 2 orthopaedic teams: one routinely prescribed a knee brace, while the other did not. Thus, patients were categorized into brace (n = 25) and no-brace (n = 25) groups accordingly. All patients followed the same standardized rehabilitation program. Assessments were performed preoperatively and at 15 days and 3, 6, and 12 months postoperatively. Outcome measures included the visual analog scale for pain, Tampa Kinesiophobia Scale, International Knee Documentation Committee score, Lysholm Knee Scoring Scale, isokinetic muscle strength testing at 60 deg/s and 180 deg/s, the 36-item Short Form Health Survey quality of life assessment, and RTS rates.
Results:
No statistically significant differences were found between the groups regarding pain, knee function, kinesiophobia, quality of life, or RTS rates at any time point (P > .05). However, baseline isokinetic extension torque at 180 deg/s was significantly higher in the brace group compared with the no-brace group (314.7 ± 66.1 Nm vs. 279.7 ± 59.6 Nm; P = .03). At the 12-month follow-up, this relationship was reversed, with the no-brace group demonstrating significantly greater extension torque at 180 deg/s than the brace group (340.8 ± 62.2 Nm vs. 301.2 ± 57.5 Nm; P = .02). Within-group improvements were observed over time in several parameters, but most did not reach statistical significance (P > .05). Brace use did not provide additional benefit in any of the evaluated outcomes.
Conclusion:
Postoperative bracing did not lead to improved clinical outcomes, including function, strength, pain, psychological readiness, or RTS success, in recreational soccer players following ACL reconstruction. These findings suggest that routine bracing may not be necessary in this population. Further prospective studies are needed to validate these retrospective observations.
Keywords
The role of bracing in the postoperative management of anterior cruciate ligament (ACL) reconstruction remains a subject of ongoing debate. While some studies suggest that bracing provides additional stability and reduces anterior tibial translation, others argue that it may lead to muscle atrophy and does not significantly contribute to functional recovery or return-to-sport (RTS) outcomes.25,32 Despite its widespread use, the value of postoperative bracing in ACL rehabilitation remains controversial, particularly among recreational soccer players, for whom clinical protocols may vary and psychological needs may differ from those of elite athletes.14,26,43
Soccer is one of the most widely played sports globally and is associated with a high risk of ACL injury due to frequent cutting, pivoting, and deceleration movements.8,20 While arthroscopic ACL reconstruction restores mechanical stability, successful postoperative rehabilitation is critical for functional recovery and RTS.13,24
Postoperative bracing has been traditionally recommended to protect the graft and control knee movements during early recovery.14,43 Some studies support the notion that braces enhance knee stability and prevent excessive tibial translation, thereby protecting the surgical graft.20,38 However, other research suggests that braces do not provide substantial benefit and may even contribute to quadriceps muscle atrophy due to mechanical unloading. 40 Furthermore, some findings indicate that braces do not significantly improve rehabilitation outcomes or enhance RTS success. 26 A survey conducted by the AOSSM reported that 63% of surgeons still recommend bracing for athletes returning to play, despite the lack of consensus regarding its effectiveness. 41
An important factor in ACL rehabilitation is kinesiophobia, the fear of movement, which is particularly relevant to athletes, including soccer players.6,29 Kinesiophobia, characterized by fear and anxiety regarding physical activity and the specter of reinjury, may hinder rehabilitation progress and delay RTS. While some studies suggest that bracing provides psychological reassurance by enhancing perceived stability, others argue that it may reinforce fear-avoidance behavior, thereby hindering the rehabilitation process. The effect of bracing on kinesiophobia remains largely unclear, further complicating clinical decision-making.11,16,23,24
Considering the ongoing controversy surrounding brace use in ACL rehabilitation, this study aimed to retrospectively evaluate its impact on knee function, muscle strength, and kinesiophobia in recreational soccer players following ACL reconstruction. By focusing on recreational soccer players who may face distinct psychological and logistical challenges during recovery, our study aims to clarify the practical value of bracing in a real-world athletic setting.
Methods
This retrospective cohort study was conducted on 50 male recreational soccer players who underwent arthroscopic ACL reconstruction at Duzce University Faculty of Medicine, Department of Orthopaedics and Traumatology, between 2020 and 2023. The study aimed to evaluate the effects of postoperative brace use on knee function, muscle strength, pain, and kinesiophobia during a 1-year follow-up period. The study was conducted in accordance with the Declaration of Helsinki and was approved by the Duzce University Clinical Research Ethics Committee. Informed consent was obtained from all participants, and data were anonymized before analysis.
Participant Selection
A total of 62 recreational soccer players who underwent ACL reconstruction between 2020 and 2023 were initially evaluated for this retrospective cohort study. However, 12 patients were excluded due to missing follow-up data (n = 7) or ACL graft rerupture requiring revision surgery (n = 5). As a result, 50 patients met the inclusion criteria and were included in the final analysis.
The inclusion criteria consisted of male recreational soccer players aged 18 to 32 years who had a primary, isolated ACL rupture requiring arthroscopic reconstruction. In this study, “isolated ACL rupture” was defined as an ACL injury without any concomitant ligamentous involvement, including medial collateral ligament, posterior cruciate ligament, or lateral collateral ligament sprains. Patients were excluded if they had any multiligamentous knee injury, congenital or acquired knee deformities, previous knee surgery, systemic diseases affecting the musculoskeletal system, or if they experienced ACL graft rerupture requiring revision.
Furthermore, patients with complex or degenerative meniscal tears (eg, root tears or bucket-handle tears) or chondral lesions classified as Outerbridge grade 2 or higher were excluded. However, small, stable meniscal tears treated during ACL reconstruction (eg, partial meniscectomy or repair of longitudinal tears) were not exclusionary. Additionally, patients with incomplete follow-up data were excluded from the final analysis.
Surgical and Follow-up Protocol
All surgeries were performed by 2 experienced orthopaedic surgeons (S.S., Z.O.K.), each following their standard clinical practice. One routinely prescribed postoperative bracing, while the other did not. All reconstructions were performed using ipsilateral semitendinosus ± gracilis tendons prepared as quadrupled hamstring autografts, with suspensory fixation techniques applied for both femoral and tibial sides. No bone–patellar tendon–bone, quadriceps tendon, or allograft reconstructions were used. In addition, no lateral extra-articular procedures (eg, anterolateral ligament reconstruction or lateral tenodesis) were performed in any patient.
After surgery, patients were categorized into 2 groups according to the postoperative protocol followed: those in the brace group (n = 25) wore a Donjoy Armor Knee Brace with Fourcepoint technology (DJO Global), which was locked in full extension for the first 2 weeks and then gradually unlocked to allow increasing flexion. They were advised to wear the brace for ≥6 weeks. Patients in the no-brace group (n = 25) did not use any postoperative bracing. All patients followed a standardized rehabilitation program under the supervision of a licensed physical therapist (V.U., I.S.). The first 8 weeks of rehabilitation were conducted in the clinic, where structured physical therapy sessions focused on early range of motion (ROM) exercises, neuromuscular training, and progressive strengthening protocols. After this period, some patients continued their rehabilitation at private clinics, in different cities, or within their own club facilities, depending on their individual circumstances.
Follow-up assessments were conducted at preoperative baseline and at 15 days, 3 months, 6 months, and 12 months postoperatively to evaluate knee function, muscle strength, pain, edema, kinesiophobia, and overall recovery.19,39 Furthermore, to determine leg dominance, each participant was asked, “Which leg do you naturally use to kick a ball?” The selected leg was recorded as the dominant side in accordance with standard clinical practice. RTS was defined as the patient's ability to resume full participation in recreational soccer training and match play without medical or functional restrictions, based on both self-report and physical therapist confirmation.
Evaluation Methods
Knee Stability Assessment. Knee stability was assessed using the pivot-shift test, a standard clinical method for evaluating rotational instability in ACL-deficient knees. The test was performed with the patient lying in a supine position, with the hip flexed to 30° and the knee in full extension. A valgus force was applied while internally rotating the tibia, and the knee was gradually flexed. The degree of tibial subluxation was classified into 4 categories: no shift (grade 0), a slight glide indicating mild instability (grade 1), a distinct clunk suggesting moderate instability (grade 2), and a severe subluxation reflecting significant instability (grade 3). This assessment was conducted preoperatively and at 15 days, 3 months, 6 months, and 12 months postoperatively to monitor changes in knee stability over time. 22
Pain Assessment. Pain levels were assessed using the 10-cm visual analog scale (VAS), where 0 indicated no pain and 10 represented the most severe pain. VAS measurements were recorded at 5 time points: during the preoperative surgical planning visit (typically 1-3 days before surgery), and postoperatively at 15 days, 3 months, 6 months, and 12 months. Given the variable time from injury to surgery among participants, preoperative VAS scores may not fully reflect the acute postinjury phase and are acknowledged as a limitation. 23
Range of Motion. Knee ROM was measured using a digital inclinometer (Baseline Bubble Inclinometer; Fabrication Enterprises Inc). Measurements were performed in a supine position. For knee flexion, the patient actively flexed the knee while the inclinometer was aligned with the midline of the femur and tibia. For knee extension, the measurement was taken with the heel resting on the examination table and the posterior aspect of the knee elevated using a support; full passive extension was encouraged, and 0° was defined as neutral alignment of the femur and tibia. Hyperextension values, if present, were recorded as negative.
All measurements were performed by the same physical therapist to reduce interrater variability. Side-to-side comparisons were not recorded. Intrarater reliability testing was not conducted, which is acknowledged as a limitation. 15
Muscle Strength Evaluation. Muscle strength was assessed using an isokinetic dynamometer (Cybex Norm; Cybex, division of Lumex Inc). All patients performed a standardized warm-up consisting of 5 minutes of low-resistance cycling and dynamic stretching exercises prior to testing. Quadriceps and hamstring strength were evaluated at angular velocities of 60 deg/s (5 repetitions) and 180 deg/s (15 repetitions) to assess peak torque and endurance, respectively.
The hamstring-to-quadriceps (H/Q) ratio was calculated at both velocities to evaluate muscle balance.
Isokinetic testing was performed at all scheduled follow-up time points; however, at 15 days postoperatively, testing was limited to low-intensity submaximal efforts for monitoring purposes only and was not used for maximal torque interpretation. In the brace group, the brace was removed during the 15-day evaluation to allow unrestricted movement. All tests were conducted by the same physical therapist using a standardized protocol. 34
Knee Circumference and Edema Evaluation. Knee circumference was measured to assess postoperative edema and potential quadriceps muscle atrophy. Two separate measurements were performed using a nonelastic, millimeter-marked tape measure at (A) the midpatellar level to evaluate joint swelling and (B) 15 cm above the superior border of the patella to assess thigh muscle bulk. All measurements were taken with the patient in a supine position and the quadriceps fully relaxed. The same trained physical therapist conducted all measurements to ensure consistency. Measurements were recorded preoperatively and at 15 days, 3 months, 6 months, and 12 months postoperatively. 21
Kinesiophobia Assessment. Kinesiophobia was evaluated using the Tampa Kinesiophobia Scale (TKS), a 17-item questionnaire assessing the fear of movement and reinjury. Each item was scored on a 4-point Likert scale (1 = strongly disagree, 4 = strongly agree), with higher scores indicating greater levels of kinesiophobia. The TKS was administered preoperatively and at all postoperative follow-up time points. 17
Knee Function Assessment. Knee function was assessed using the International Knee Documentation Committee (IKDC) 2000 Subjective Knee Form and the Lysholm Knee Scoring Scale. The IKDC consists of 18 questions evaluating knee symptoms, sports activity, and daily functional status, with scores ranging from 0 to 100, where higher scores indicate better function. The Lysholm Knee Scoring Scale evaluates knee stability, pain, and overall functional ability, also scored from 0 to 100, with higher scores representing better knee performance. Both scales were applied at each follow-up time point.28,35
Quality-of-Life Assessment
Quality of life was assessed using the 36-item Short Form Health Survey (SF-36), a validated questionnaire evaluating eight health domains: physical functioning, role limitations due to physical health, bodily pain, general health perception, vitality, social functioning, role limitations due to emotional problems, and mental health. Scores range from 0 to 100, with higher scores indicating better perceived health status. The SF-36 survey was administered at baseline and at 15 days, 3 months, 6 months, and 12 months postoperatively to monitor changes in patients' quality of life throughout the recovery process. 18
Statistical Analysis
Statistical analysis was performed using SPSS 22.0 (IBM). An a priori power analysis was conducted using G*Power (Version 3.1.9.7; Heinrich Heine University) to determine the required sample size for detecting significant differences in muscle strength, knee function, and kinesiophobia between the brace and no-brace groups. Based on an effect size (d) of 0.8, a power (1-β) of 0.80, and a significance level (α) of .05, the analysis determined that a minimum of 24 participants per group was required. Considering potential dropouts, 50 patients were included in the final analysis. 27
Descriptive statistics were calculated for all variables. The Shapiro-Wilk test was used to assess the normality of quantitative variables, and the Levene test was applied to examine the homogeneity of group variances. Independent samples t tests were used for intergroup comparisons of normally distributed continuous variables, while the Mann-Whitney U test was applied for nonnormally distributed data.
A repeated-measures analysis of variance (ANOVA) was conducted to analyze changes in continuous variables over time within each group. ANOVA is a statistical method used to compare mean differences across multiple time points while accounting for within-patient variability. In this study, 2-way repeated-measures ANOVA was performed to evaluate both the main effect of time (preoperative vs postoperative follow-ups) and the interaction effect between time and group (brace vs no brace). Post hoc Tukey and Sidak tests were applied to identify specific time points when significant differences occurred. Additionally, generalized estimating equations were used as a complementary method for analyzing longitudinal data and accounting for missing values.
For categorical variables, Pearson chi-square test and Fisher exact test were used to evaluate group differences. A P value of <.05 was considered statistically significant.
Results
As shown in Table 1, both groups were comparable in terms of age, height, weight, body mass index (BMI), time from injury to surgery, and affected knee side (P > .05). However, a significant difference was observed in dominant knee distribution (P = .024), with a higher percentage of right-leg dominance in the brace group (64%) compared with the no-brace group (32%).
Sociodemographic and Clinical Characteristics of the Patients a
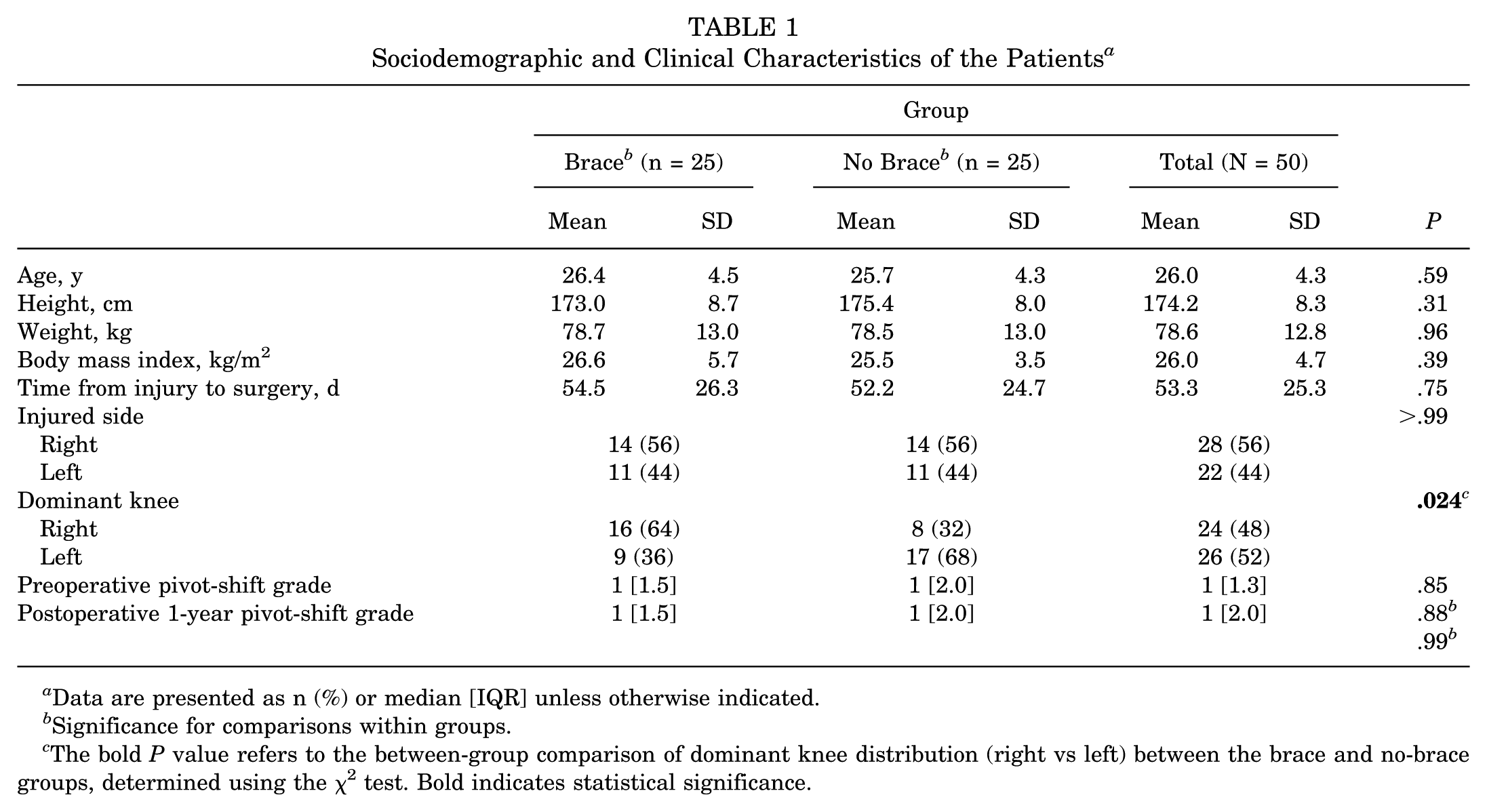
Data are presented as n (%) or median [IQR] unless otherwise indicated.
Significance for comparisons within groups.
The bold P value refers to the between-group comparison of dominant knee distribution (right vs left) between the brace and no-brace groups, determined using the χ2 test. Bold indicates statistical significance.
Preoperative and postoperative pivot-shift grades did not differ significantly between the groups (P > .05), and no significant intragroup changes were observed over the 12-month follow-up period (P > .05). These findings indicate that brace use did not provide additional stabilization benefits postoperatively.
As demonstrated in Table 2, there were no statistically significant differences between the brace and no-brace groups in terms of pain levels (VAS), kinesiophobia (TKS), knee function (IKDC and Lysholm Knee Scoring Scale), or quality of life (SF-36) at any postoperative time point (P > .05).
Clinical Values Measured in Different Periods According to Group a
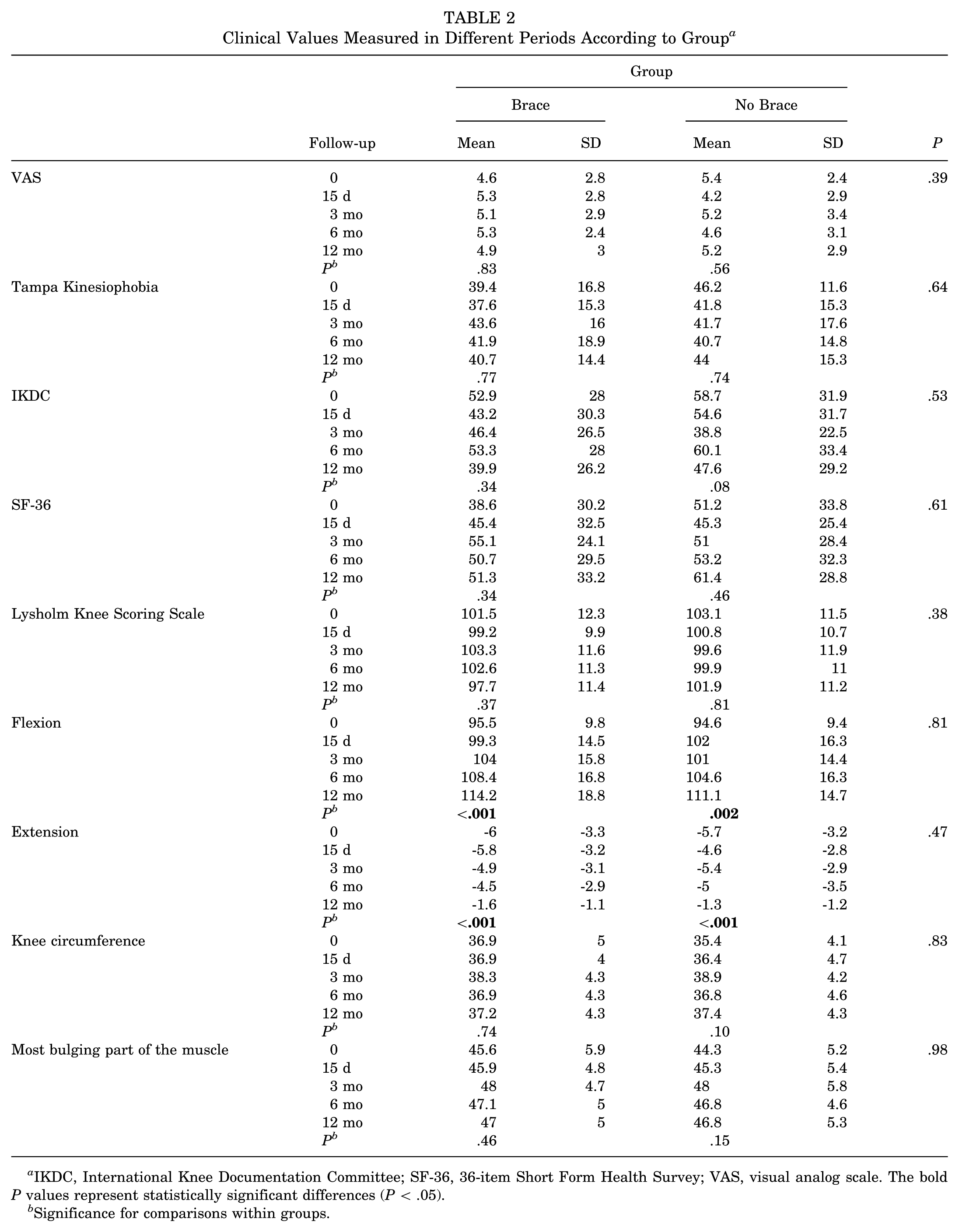
IKDC, International Knee Documentation Committee; SF-36, 36-item Short Form Health Survey; VAS, visual analog scale. The bold P values represent statistically significant differences (P < .05).
Significance for comparisons within groups.
There was no statistically significant change in pain levels (VAS) over time within either the brace group (P = .83) or the no-brace group (P = .56). Similarly, TKS scores did not show significant within-group changes during the follow-up period (brace, P = .77; no brace, P = .74). No statistically significant differences were observed between the groups at any time point for either parameter.
No statistically significant changes over time were observed in VAS, TKS, IKDC, Lysholm, or SF-36 scores within either group (all P > .05). However, both groups showed statistically significant improvements in knee flexion and extension ROM during the follow-up period (P < .001 for both). Intergroup comparisons revealed no significant differences between the brace and no-brace groups at any time point for any of the assessed parameters.
According to Table 3, no consistent significant differences were observed between groups for isokinetic flexion and extension torques at 60 deg/s and 180 deg/s, as well as the H/Q ratio throughout the follow-up period (P > .05).
Isokinetic Flexion, Extension Torque, H/Q Ratio, Isometric Flexion, and Extension Values Measured at Different Periods and Speeds According to Groups a

H/Q ratio, hamstring-to-quadriceps ratio. The bold p values represent statistically significant differences (P < .05).
Significance for comparison within groups.
Post hoc tests are nonsignificant even if the test is significant.
However, a statistically significant baseline difference in isokinetic extension torque at 180 deg/s was noted between groups (P = .03), with higher values in the brace group. Despite this initial advantage, at 12 months, isokinetic extension torque at 180 deg/s was significantly lower in the brace group compared with the no-brace group (P = .02).
Moreover, in the no-brace group, extension torque at 180 deg/s significantly increased at 12 months compared with baseline (P = .005), whereas no such improvement was observed in the brace group.
As seen in Table 4, within-group percentages were calculated based on the total number of patients in each respective subgroup (brace/no-brace and low/high TKS categories). No significant differences were observed in RTS rates between the brace and no-brace groups throughout the follow-up period (P > .05). Preoperatively, 88.9% of patients with low kinesiophobia (TKS <37) successfully returned to sports, whereas this rate was 93.8% in those with high kinesiophobia (TKS ≥37). However, this difference was not statistically significant (P = .61). Similarly, at 15 days, 3 months, 6 months, and 12 months postoperatively, there were no significant differences in RTS rates between patients with high and low kinesiophobia scores or between the brace and no-brace groups (P > .05).
Distribution of Patients With High and Low Kinesiophobia Scores in Different Periods According to Group and Return to Sports a

preop, preoperatively; TKS, Tampa Kinesiophobia Scale.
P value for comparison within the Brace group.
P value for comparison within the No-Brace group.
P value for the overall comparison including all patients.
Correlation analyses revealed no significant associations between age or BMI and clinical outcome measures, including pain (VAS), kinesiophobia (TKS), functional scores (IKDC, Lysholm), and isokinetic muscle strength, in either group (P > .05). Moreover, kinesiophobia and isokinetic strength scores showed no statistically significant differences between the brace and no-brace groups across the follow-up period.
Discussion
This study evaluated the effects of postoperative brace use on knee function, muscle strength, pain, and kinesiophobia over a 1-year follow-up in recreational soccer players who underwent ACL reconstruction. The findings indicate that brace use does not significantly influence key rehabilitation outcomes, challenging the necessity of routine brace implementation in postoperative protocols.
One of the most notable findings was that brace use did not lead to a significant improvement in knee ROM over time. In fact, the no-brace group demonstrated a more pronounced gain in flexion, suggesting that brace use may slightly limit early mobility gains. This finding is in contrast to some studies that report no negative impact of bracing on knee ROM1,9 and highlights the need for further investigation into patient-specific responses to postoperative immobilization. While our findings did not demonstrate a significant advantage of brace use in terms of functional outcomes or ROM, it is important to note that these results do not directly address the theoretical benefit of bracing in limiting anterior tibial translation to protect the graft—a biomechanical parameter not assessed in this study. 13 Although some studies suggest that brace use enhances knee stability, 14 our results indicate that there were no significant differences in pivot-shift test results between the brace and no-brace groups throughout the follow-up period.
A critical issue in ACL rehabilitation is whether external support is beneficial for maintaining stability while allowing progressive strengthening. Recent evidence suggests that early mobilization, rather than restriction through braces, leads to better functional outcomes by promoting neuromuscular adaptation and proprioceptive recovery.16,33 The role of psychological factors, particularly kinesiophobia, in ACL rehabilitation has been increasingly recognized. Our study demonstrated that brace use did not significantly reduce kinesiophobia levels at any time point.
Kinesiophobia, or fear of movement, is a crucial determinant of RTS outcomes, with some studies suggesting that braces may provide a psychological sense of security, thereby reducing movement fear. 30 However, other research indicates that prolonged external support may inadvertently increase kinesiophobia by reinforcing dependency and limiting active engagement in rehabilitation.42,44 Our findings align more closely with the latter perspective, suggesting that brace use does not provide a psychological advantage in reducing fear of reinjury. Instead, targeted psychological interventions, such as exposure-based therapy and confidence-building exercises, may be more effective in mitigating kinesiophobia and facilitating a return to preinjury activity levels. Further research is needed to explore whether psychological interventions combined with bracing strategies yield superior results.13,14,26
Muscle strength, particularly of the quadriceps and hamstrings, is a primary determinant of functional recovery following ACL reconstruction. Our isokinetic testing results showed no significant differences in flexion and extension torque between the brace and no-brace groups, supporting the notion that brace use does not enhance muscle strength recovery.36,45 Although slight improvements in strength were observed over the 12-month follow-up in both groups, these changes were minimal and did not reach statistical significance. This may reflect a plateau in neuromuscular recovery or suboptimal engagement in strength training during the rehabilitation period and warrants further investigation.
The concern that prolonged brace use may contribute to muscle atrophy due to reduced neuromuscular activation has been discussed in prior literature. 3 Some studies have reported a decline in quadriceps strength associated with postoperative bracing, possibly due to mechanical unloading and subsequent disuse atrophy.3,12 However, our study found no evidence of strength deterioration in the brace group compared with the no-brace group. These findings suggest that brace use does not significantly impair muscle recovery when combined with an appropriate rehabilitation protocol.
Interestingly, our results showed that isokinetic extension torque at 180 deg/s was significantly higher at 12 months in the no-brace group compared with the brace group (P = .02). Although a significant difference in extension torque at 180 deg/s was observed at the 12-month follow-up in favor of the no-brace group, no such differences were present at earlier time points. Therefore, it remains uncertain whether brace use truly limits long-term strength development, and further studies with larger samples and more frequent testing intervals are needed to clarify this finding. 5
Functional scores, including the IKDC and Lysholm Knee Scoring Scale, showed no significant differences between groups, reinforcing the argument that brace use does not enhance functional recovery. Both groups demonstrated progressive improvements over time, but the rate of recovery was comparable. Similarly, SF-36 scores indicated that brace use did not significantly influence overall quality of life during rehabilitation. These findings are in agreement with prior studies suggesting that postoperative rehabilitation protocols emphasizing progressive strengthening and early mobilization yield comparable functional outcomes with or without bracing.2,37
Evaluating the broader functional recovery outcomes, including return to physical activity and knee performance, our findings revealed no significant difference between braced and unbraced patients. Likewise, high or low levels of kinesiophobia did not appear to alter these recovery patterns (Table 4). These results support the hypothesis that brace use does not expedite the return to preinjury activity levels and that psychological readiness, rather than mechanical support, plays a more prominent role in this process.10,31
Postoperative pain management remains a crucial aspect of ACL rehabilitation. VAS scores showed significant pain reduction over time in both groups, but brace use did not provide additional pain relief. This finding challenges earlier studies that suggested bracing could reduce postoperative pain by providing joint support and restricting excessive motion. Instead, our results align with more recent studies indicating that well-structured rehabilitation protocols focusing on progressive loading and neuromuscular retraining are more effective in managing pain than external bracing alone.4,7
Given the lack of significant pain reduction with brace use, it may be unnecessary to incorporate braces solely for analgesic purposes in rehabilitation protocols. Future studies should explore whether specific brace designs, such as those incorporating dynamic unloading mechanisms, offer superior pain relief compared with traditional bracing approaches.
Limitations
Several limitations should be acknowledged when interpreting these findings. The sample size was relatively small, which may have limited the statistical power to detect subtle differences in secondary outcomes. Additionally, the follow-up period was restricted to 12 months, precluding the assessment of long-term effects beyond 1 year. Future studies should consider larger cohorts and extended follow-up periods to determine whether the effects of brace use evolve over time.
Another limitation was the potential variability in postoperative rehabilitation settings. While all participants underwent the same initial 8-week rehabilitation program in our clinic, some continued rehabilitation in different facilities, including private clinics and team-based rehabilitation settings. This heterogeneity may have influenced secondary outcomes, such as strength recovery and RTS rates. Standardizing rehabilitation protocols across study participants would provide a clearer assessment of brace efficacy.
Due to the retrospective nature of the study, group allocation was based on routine practice differences between surgical teams rather than random assignment. This may introduce selection bias and limit causal inference.
Furthermore, although all pivot-shift assessments were performed by an experienced clinician, no inter- or intrarater reliability analyses were conducted, and the subjectivity of this test should be considered when interpreting stability outcomes.
Additionally, isokinetic strength testing was performed as early as 15 days postoperatively, which may not reflect true muscular strength and could be affected by pain, bracing, or incomplete recovery.
Moreover, this study did not include any objective functional performance tests (eg, single-leg hop, agility drills), which may have limited the assessment of true functional capacity and RTS readiness. The exclusive reliance on self-reported questionnaires may not fully capture physical performance in active individuals.
Last, the study sample consisted only of male recreational soccer players, limiting the generalizability of findings to female athletes or individuals with different physical activity levels. Future research should aim for more diverse and inclusive cohorts.
Conclusion
This study showed that postoperative brace use does not significantly influence muscle strength, as well as self-reported pain, knee function, and kinesiophobia in recreational soccer players following ACL reconstruction. As all primary and secondary outcomes in this study were based on self-reported measures, these findings should be interpreted with caution. Our results raise questions about the value of routine postoperative knee bracing in ACL rehabilitation and suggest that brace prescriptions should be based on individualized patient needs and clinical judgment.
Footnotes
Acknowledgements
The authors thank all the patients and clinical staff who contributed to this study.
Final revision submitted September 8, 2025; accepted September 24, 2025.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Duzce University Clinical Research Ethics Committee (August 29, 2023; decision No. 2023/122).