
Abstract
Background:
Posterior cruciate ligament (PCL) tibial avulsion fractures are infrequently observed clinical entities, primarily due to the challenges in arthroscopic management of the posterior compartmental process. This condition frequently leads to either significant injury sequelae or suboptimal outcomes.
Purpose:
To evaluate the clinical outcomes for arthroscopic treatment for PCL avulsion fractures from anterior compartment loop-and-tack to the pulled-in posterior compartment with suspension fixation.
Study Design:
Case Series; Level of evidence, 4.
Methods:
The study period spanned from May 2017 to June 2020, with a mean postoperative follow-up time of 30 months (range, 24-50 months). The study inclusion criteria included arthroscopic PCL tibial avulsion fracture fixation using our loop-and-track technique only. A total of 27 patients with acute PCL avulsion fractures who met our criteria were recruited. The exclusion criteria included PCL tibial avulsion malunioned fractures, multiple ligament injuries, and patients lost to follow-up. This technique was performed using an anterior compartment loop-and-tack and pulling in from the posterior compartment with suspension fixation via a tibial tunnel. Anterior fixation was achieved using the Endobutton device with knotted fixation and knotless rivets to secure the wire tails. Bony healing was examined by radiograph. Clinical and functional outcomes were scored using the Lysholm knee score, the International Knee Documentation Committee (IKDC) 2000 knee subjective function score, and the IKDC examination. Paired t tests were used to compare the Lysholm and subjective IKDC scores before and after treatment. A nonparametric paired test was used to compare IKDC knee examination scores before and after surgery.
Results:
A total of 24 patients, 19 male and 5 female patients, were included in this study. The arthroscopic anterior compartment loop-and-tack technique had a short operative time (50 ± 23.73 minutes, 45-90 minutes), with good stability, bony healing, and satisfactory functional recovery of the knee in all patients. No popliteal fossa neurovascular complications, implant loosening, or slippage were observed. The mean Lysholm knee score improved from 17.25 ± 6.30 preoperatively to 97.35 ± 2.94 (P < .001) at the last follow-up. The mean IKDC 2000 subjective knee function score improved from 19.95 ± 1.43 to 97.05 ± 2.89 (P < .001) at the previous follow-up. There was also a significant improvement in the IKDC examination grade (11 grade C and 13 grade D to 22 grade A and 2 grade B after the surgery).
Conclusion:
Our loop-and-track technique for treating PCL tibial avulsion fractures improves clinical outcomes with minimal complications. This technique may be considered in the treatment options for patients with PCL tibial avulsion fractures.
Posterior cruciate ligament (PCL) tibial avulsion fractures are often caused by an impact on the anterior tibia in the flexed knee state. They are most often seen in crashes involving motorcycles and electric bicycles.1,10 In most patients with PCL tibial avulsion fractures, hemorrhagic crusts formed by skin contusions are seen around the tibial tuberosity. The diagnosis can be confirmed by the posterior drawer test, radiograph, and computed tomography (CT) examination. The reported incidence of general PCL injuries varies between 3% and 38% of acute knee injuries. 1 PCL tibial avulsion fracture represents a very rare subset of PCL injuries,10,12,18 and could lead to joint displacement, joint instability, or even dysfunction.2,21 Treatment options for these injuries include nonoperative treatment, open and arthroscopic reduction, and internal fixation. Acute PCL avulsion injuries (<1 week) with displacement of >6.7 mm should be considered for operative treatment. 21 PCL avulsion fractures of the tibia are a specific type of PCL injury that is difficult to manage. 16 General PCL surgery always requires adequate visualization and fixation of the posterior compartment, 17 and it needs more time to learn and perform the operation. It is straightforward for experienced orthopaedic surgeons to perform open reduction and internal fixation without the learning curve of arthroscopic surgery. However, open surgery is invasive and requires a period of recovery. 11 Arthroscopic reduction and fixation is a less invasive operation and can simultaneously treat intra-articular lesions. 5 The current commonly used method of fixation of PCL tibial avulsion fractures requires posterior wire binding or screws for fixation. However, this method has a relatively steep learning curve, and repeated posterior compartment operations may pose risks to neurovascular structures. Other disadvantages include unreliable fixation due to small bone fragments and the risk of slippage.4,18
We utilized anterior compartment loop-and-tack suspension fixation to overcome the challenges of arthroscopic posterior compartment operations and the limitations of small avulsion fracture fixation techniques. This study aimed to summarize the clinical and functional results of this technique in a retrospective case series. We hypothesized that this new technique would achieve satisfactory therapeutic effects and provide a novel surgical approach in the clinic.
Methods
This study conducted from May 2017 to June 2020, was approved by the Institutional Review Committee of the Shenzhen Nanshan People's Hospital (No. LW-2023-001). The acute tibial avulsion fracture of the PCL was diagnosed using radiographs, CT, and magnetic resonance imaging (MRI) before surgery (Figure 1). Arthroscopic surgery was then performed by the same surgeons (Weimin Guo et al). The inclusion criteria included that the displacement of the fracture was >6.7 mm, and only the anterior compartment loop-and-tack fixation technique was used for arthroscopic PCL tibial avulsion fracture fixation, as well as at least 2 years of clinical follow-up. Patients aged 18 to 70 years with acute injuries (<1 week) were included in our study. The exclusion criteria included patients with multiple ligament injuries, malunioned fractures (>3 W), and patients lost to follow-up.
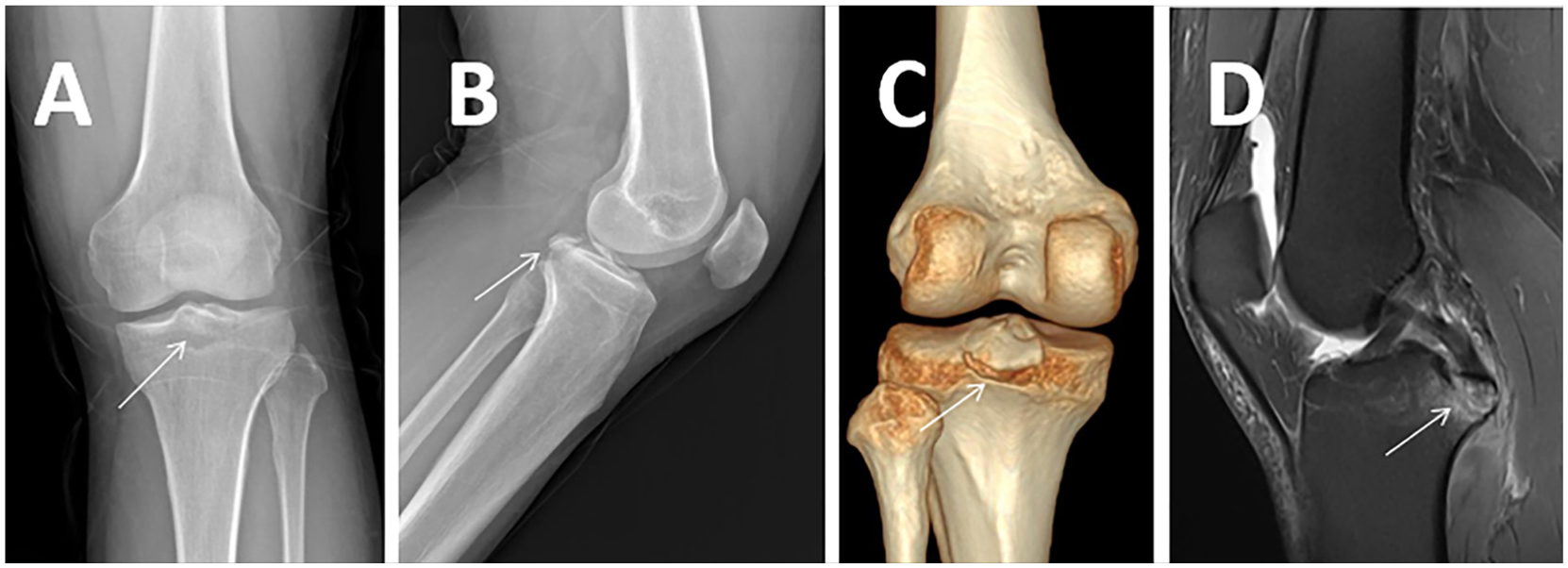
Case of a 32-year-old female patient with a PCL tibial avulsion fracture of the right knee. (A) Nonweightbearing anterior-posterior radiograph (arrows showing avulsion fracture). (B) Nonweightbearing lateral radiograph. (C) Weightbearing coronal CT imaging. (D) Sagittal T2 fat-suppressed MRI showing displacement of the fracture (arrow). MRI, magnetic resonance imaging; PCL, posterior cruciate ligament.
Evaluation Method
In both the pre- and postoperative phases, we assessed patients using the International Knee Documentation Committee (IKDC) subjective score and the IKDC examination grade. The IKDC Subjective Score is a patient-reported questionnaire evaluating knee function, symptoms, and daily activities, with scores ranging from 0 to 100, where higher scores indicate better knee function. The IKDC examination grade, a component of the IKDC system, involves a clinical evaluation by the physician, assessing knee stability, range of motion, swelling, and pain. Based on these assessments, the knee's condition is categorized into 4 grades: grade A (normal), indicating no significant abnormalities with normal function; grade B (nearly normal), indicating minor abnormalities with near-normal function; grade C (abnormal), indicating significant abnormalities with restricted function; and grade D (severely abnormal), indicating severe abnormalities with markedly limited function. Additionally, we conducted comprehensive evaluations of injuries and healing using radiographs, CT scans, and MRI scans from coronal and sagittal planes, both pre- and postoperatively.
Surgery Method
The surgery involves anterior loop fixation, posterior reduction, and stabilization of the PCL using high-strength sutures. It employs a single-bone tunnel technique, starting from the anterior aspect of the tibia and extending posteriorly, below the tibial attachment of the PCL. In the anterior bone tunnel, a combination of a suture button, a titanium plate, and non-locking rivets is used to secure the high-strength suture. This allows for suspended fixation of PCL avulsion fractures.
The patient was placed in the supine position, and combined spinal-epidural anesthesia was administered. After applying a tourniquet, the anatomic landmarks, including the patella, patellar ligament, femoral condyles, tibial plateau, and tibial tubercle, were identified and marked. Prophylactic antibiotics were given before the procedure. A 30° arthroscope was used to visualize the joint cavity. Depending on intraoperative requirements, we employed the high lateral parapatellar, high medial parapatellar, low intermediate, or posteromedial approach.
The anterolateral approach was used to perform synovectomy between the anterior cruciate ligament (ACL) and PCL, allowing exposure of the posterior edge of the femoral attachment of the PCL. Synovial tissue between the PCL and the medial femoral condyle was partially resected. The arthroscope was inserted through the anterior compartment and advanced into the posteromedial compartment. Posteromedial portals were established percutaneously under direct arthroscopic visualization using a spinal needle. Synovectomy around the tibial avulsion fracture site and evacuation of the hematoma were performed using an arthroscopic shaver and suction.
Then, the posterior internal approach was observed, and the PCL locator (Figure 2A) was placed between the ACL and PCL. The pin of the locator was located at the distal fracture line. A 2-cm incision was made inside the tibial tubercle, and the 2.3-mm diameter Kirschner wire was drilled from anterior to posterior by the PCL drill guide (Smith & Nephew) (Figure 2, B and D). The sleeve was removed and the locator was kept in place to protect the nerve and blood vessels posterior to the knee joint, avoiding any stabbing. The bone tunnel was expanded with a 4.5-mm hollow drill and the polydioxanone suture (PDS) was passed through the bone tunnel from anterior to posterior. The PDS was grasped from the anterior inner approach (Figure 2C).

Drilling the bone tunnel under arthroscopy and placing the PDS suture inside. (A) Arthroscopic images show that the posterior internal approach was taken for observation, and the PCL tibial locator was used to position the PCL tibial stop. (B) Under the PCL tibial locator positioning and protection, a 2.3-mm diameter needle was passed through the tibia to reach the bone block line. (C) A 4.5-mm diameter hollow drill was passed through the tibia, and the PDS suture was passed through the hollow drill bit. The PDS suture was grasped with a grasper from the anterior middle approach. (D) Surgical diagram: A 2.3-mm Kirschner needle drilled from the tibial cortex toward the center of the bone fragment with the help of a posterior tibial cruciate ligament locator. PCL, posterior cruciate ligament; PDS, polydioxanone suture.
The anterolateral portal was visualized, and a suture hook (Cuff Stitch: STRAIGHT 20 UP; Smith & Nephew) was introduced through it, passing between the PCL and the medial femoral condyle to access the posterior compartment. Through the middle portal, wire grasping forceps were inserted between the ACL and PCL and advanced into the posterior compartment (Figure 3A). The PDS suture was then grasped using the suture hook (Figure 3B) and retrieved into the anterior articular cavity (Figure 3C). A PDS suture was subsequently used to shuttle 2 high-strength sutures into position (Figure 4A). From the middle portal, both ends of 1 suture were retrieved, and the knot was advanced while a probe was used simultaneously to hook the suture loop. This technique helps prevent PCL ischemia caused by excessive knot tension, which could migrate toward the PCL root. It reduces the risk of fragment loosening due to an inadequately tightened knot (Figure 4, B and D). The second high-strength suture was tied using the same technique. Through the middle portal, the PDS suture within the tibial bone tunnel and the 4 ends of the 2 high-strength sutures were simultaneously retrieved and guided into the anterior compartment from outside the joint (Figure 4C). Under arthroscopic visualization via the posteromedial portal, traction was applied to draw the sutures into the posterior compartment (Figure 5A) and then through the tibial tunnel to the anterior aspect of the tibia (Figure 5, B and D). The free ends of the 2 high-strength sutures were passed through the 2 central holes of a titanium button plate. With the knee maintained in 90° of flexion by an assistant (M.H.), the anterior drawer test was performed. The suture ends were tied securely, and a knotless anchor was used to fix the distal opening of the tibial tunnel. The fracture fragment was firmly secured with satisfactory alignment (Figure 5, C and D). Arthroscopic assessment through the anterolateral portal confirmed normal ACL tension, and the anterior drawer test was negative.

Placing the PDS suture in the anterior joint cavity under arthroscopic guidance. (A) Arthroscopic images showing the placement of a suture hook between the PCL and the medial femoral condyle in the anteromedial approach to the posterior interval, and a grasping forceps between the anterior and posterior cruciate ligaments in the medial approach to the posterior interval. (B) The PDS thread in the suture hook is grasped with the grasping forceps. (C) The PDS thread is placed in the anterior joint cavity. PCL, posterior cruciate ligament; PDS, polydioxanone suture.

Suture looping and ligation of the PCL. (A) Arthroscopic images showing 2 different colored high-strength wires brought in with PDS wires through the PCL. (B) Two fixation wires are tied separately to fix the PCL. (C) PDS traction wires are trapped at the end of 4 fixation wires in the tibial tunnel. (D) Surgical diagram: under anterior surveillance, the PCL is ligated around the wire. PCL, posterior cruciate ligament; PDS, polydioxanone suture.
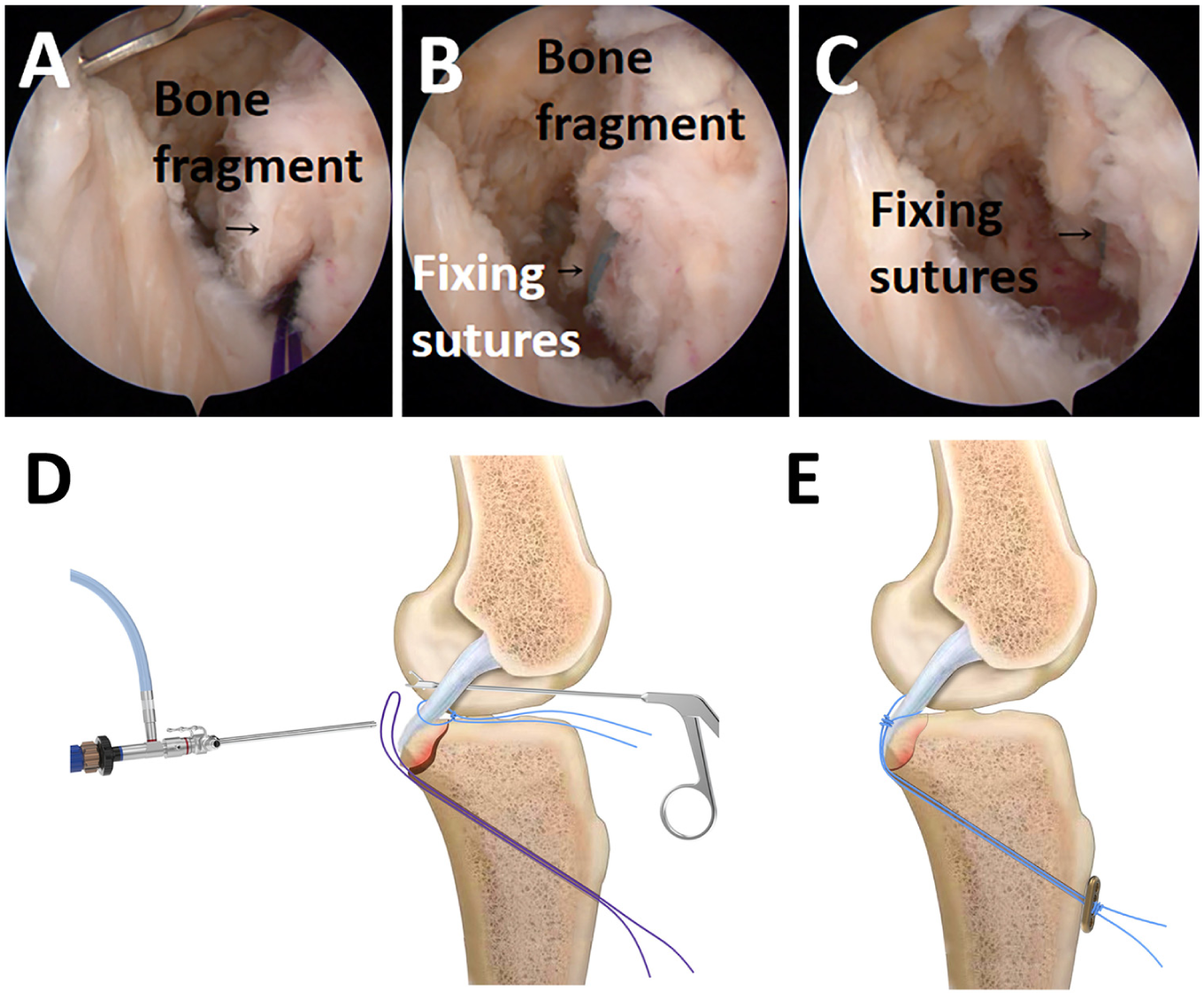
Fixating the PCL tibial avulsion fracture fragment under arthroscopy. (A) Arthroscopic images showing the PDS wire pulling the 4 suture tails of the 2 high-strength wires from anterior into posterior. (B) Pulling the high-strength wires anteriorly through the tibial tunnel. (C) The PCL tibial avulsion fracture block is firmly fixed and in a satisfactory position. (D) Surgical diagram: the traction wire introduces the high-strength wire posteriorly from the anterior and pulls it out through the tibial bone tunnel. (E) Surgical diagram: the end of the high-strength wire is passed through the button titanium plate, and the anterior drawer test is knotted for fixation. PCL, posterior cruciate ligament; PDS, polydioxanone suture.
Postoperative Management and Rehabilitation
Initial treatment consisted of local ice application, along with routine administration of analgesics or oral nonsteroidal anti-inflammatory drugs for a period of 2 to 3 days. Isometric quadriceps femoris muscle contractions and ankle joint exercises were initiated on the first postoperative day. At the same time, ambulation with the use of bilateral crutches was encouraged, with the injured limb remaining nonweightbearing for a duration of 1 month. After the operation, the knee was immobilized in an extended position using an adjustable knee brace with adjustable mobility for a duration of 4 weeks, supplemented by the placement of a folded towel as a rectangular cuboid posterior to the tibia for additional support.
An outpatient follow-up visit was scheduled 2 weeks after surgery for suture removal. During this visit, the surgeon assessed the active range of knee flexion and provided guidance on functional rehabilitation exercises to improve mobility. Knee flexion was minimized for the first 4 weeks after surgery. From 4 to 12 weeks after surgery, knee flexion was restricted to 90°, with a maximum of 120° permitted after 12 weeks. When active knee flexion exercises were started, the patient was instructed to gradually increase the range of motion, frequency, and intensity while avoiding excessive extension or pain. Outpatient follow-up visits were performed at 1, 2, 3, 6, and 12 months after surgery, including frontal and lateral knee radiographs or CT imaging to monitor progress and assess recovery.
The mean follow-up period was 30 months (24-50 months). At the last follow-up, knee function was assessed using Lysholm scores and subjective IKDC scores, and radiographs and physical examination determined the objective IKDC grade. The final follow-up assessment, including CT examination, revealed the invisibility of the fracture line, and physical examination confirmed knee stability. Five patients, who requested removal of the internal fixation, were evaluated through a second arthroscopic examination postoperatively.
Statistical Analysis
Data analysis was performed using SPSS 25.0 (IBM Corp). Paired t tests were used to compare the Lysholm and subjective IKDC scores before and after treatment. A nonparametric paired test was used to compare IKDC knee examination scores before and after surgery. P < .05 was considered statistically significant.
Results
During the study period, a total of 27 patients with acute (<1 week) PCL avulsion fractures underwent arthroscopic suspension internal fixation (Figure 6). Two patients (12%) with multiligament knee injuries were excluded, and 1 patient (6%) was lost to follow-up. 1 patient had both a PCL fracture and an ACL tibial avulsion fracture, and another patient had a combined tibial fracture. In all cases, 7 patients had meniscal injury, of whom 5 patients underwent meniscal repair.

Flowchart of the patient selection process for PCL tibial avulsion fractures. PCL, posterior cruciate ligament.
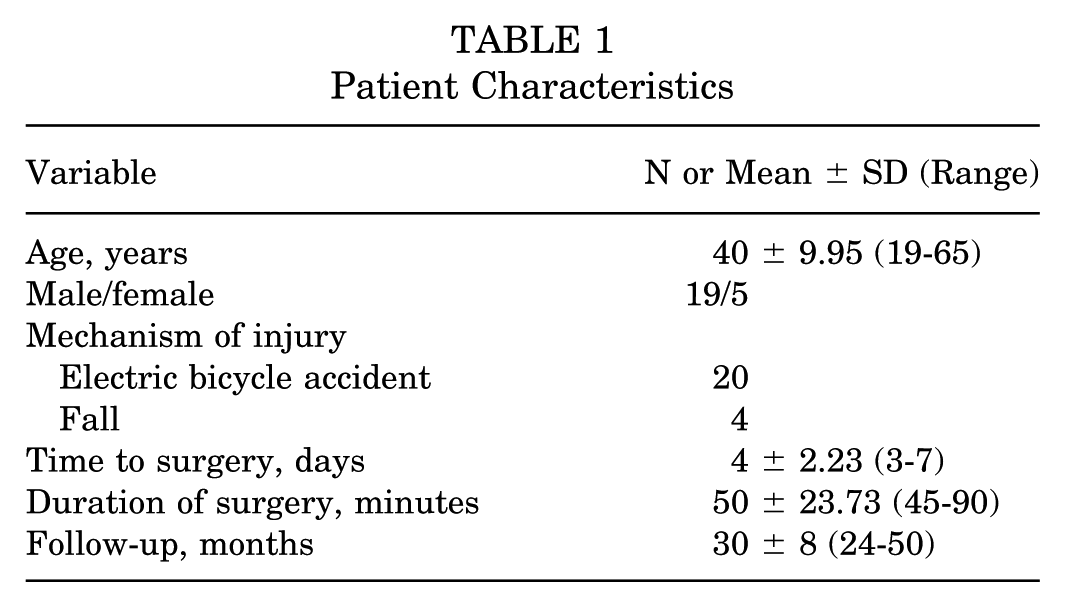
A total of 24 patients (19 men and 5 women) met the inclusion criteria and had a minimum of 2 years of follow-up. The mean age was 40 ± 9.95 years (range, 19–65 years). Fourteen patients had right knee injuries and 10 had left knee injuries; 20 injuries resulted from car accidents and 4 from falls. The time from injury to surgery was <1 week in all cases. The mean surgical time was approximately 50 ± 23.73 minutes (range, 45-90 minutes) (Table 1). All fractures healed well (Figure 7). The tension in the anterior and PCLs was satisfactory, and the use of high-strength wires did not cause any complications (eg, cutting).
Patient Characteristics
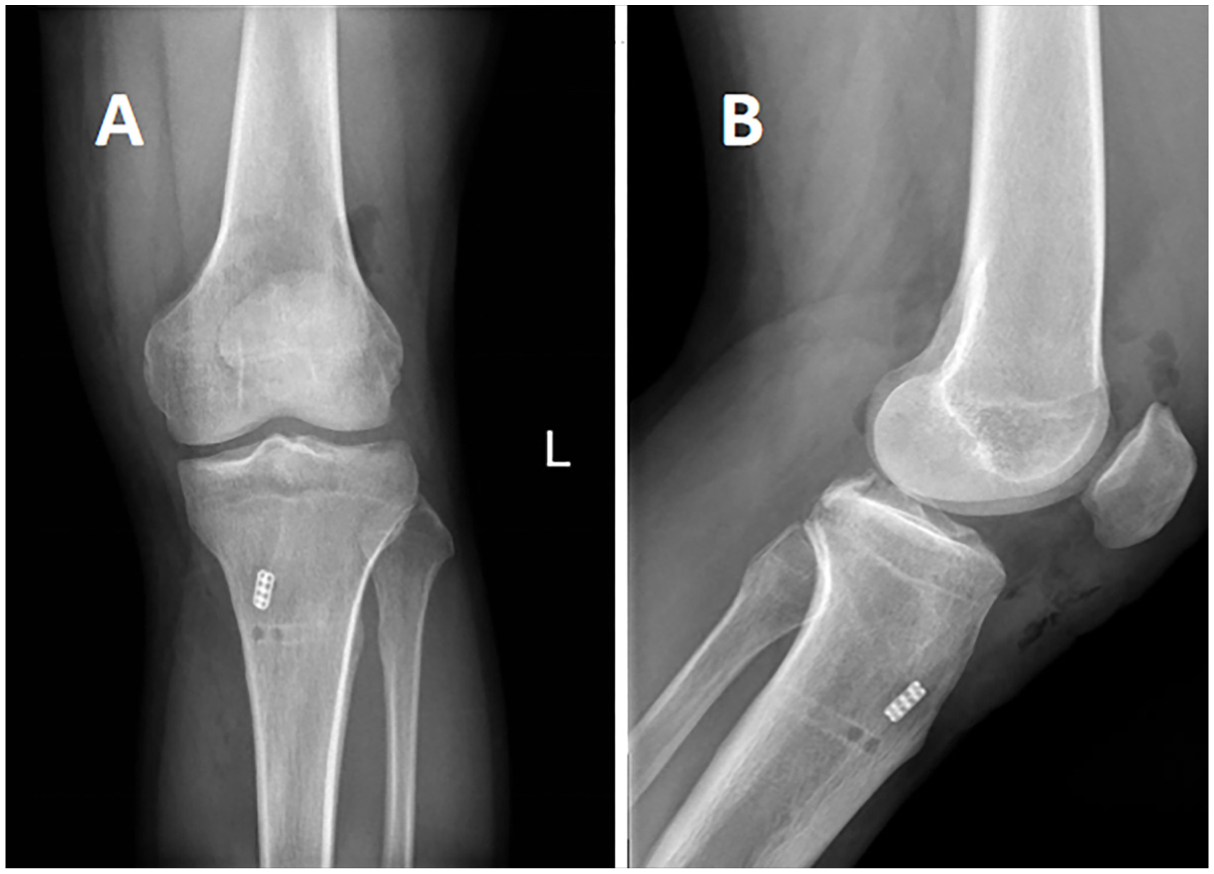
Postoperative follow-up radiograph examination. (A) Anteroposterior and (B) lateral radiographs on the second postoperative day showing the fixation of the avulsion fracture with the internal fixation in good position.
The mean Lysholm score improved significantly from 17.25 ± 6.30 preoperatively to 97.35 ± 2.94 at the last follow-up (Table 2). The statistical analysis revealed a t value of 41.179 with a P < .001, indicating a significant improvement. Similarly, the mean postoperative IKDC subjective score increased substantially from 19.95 ± 1.43 preoperatively to 97.05 ± 2.89 postoperatively, with a t value of 134 and a P < .001, further confirming the significance of this improvement. Additionally, there was a notable enhancement in the IKDC examination grades. Before surgery, 11 patients were classified with grade C, and 13 patients with grade D. Postoperatively, 22 patients were reclassified to grade A (normal), and 2 patients to grade B (near normal). Fracture healing was demonstrated by CT 2 to 3 months postoperatively (Figure 8), with negative anterior and posterior drawer test examinations. No complications, such as neurovascular injury, thrombosis, infection, or loosening of the bone block, were observed in any of the cases. In 5 patients, the ACL and PCL demonstrated satisfactory tension during the second postoperative arthroscopic exploration.
Comparison of Statistical Data Between Pre- and Postoperative Evaluation a
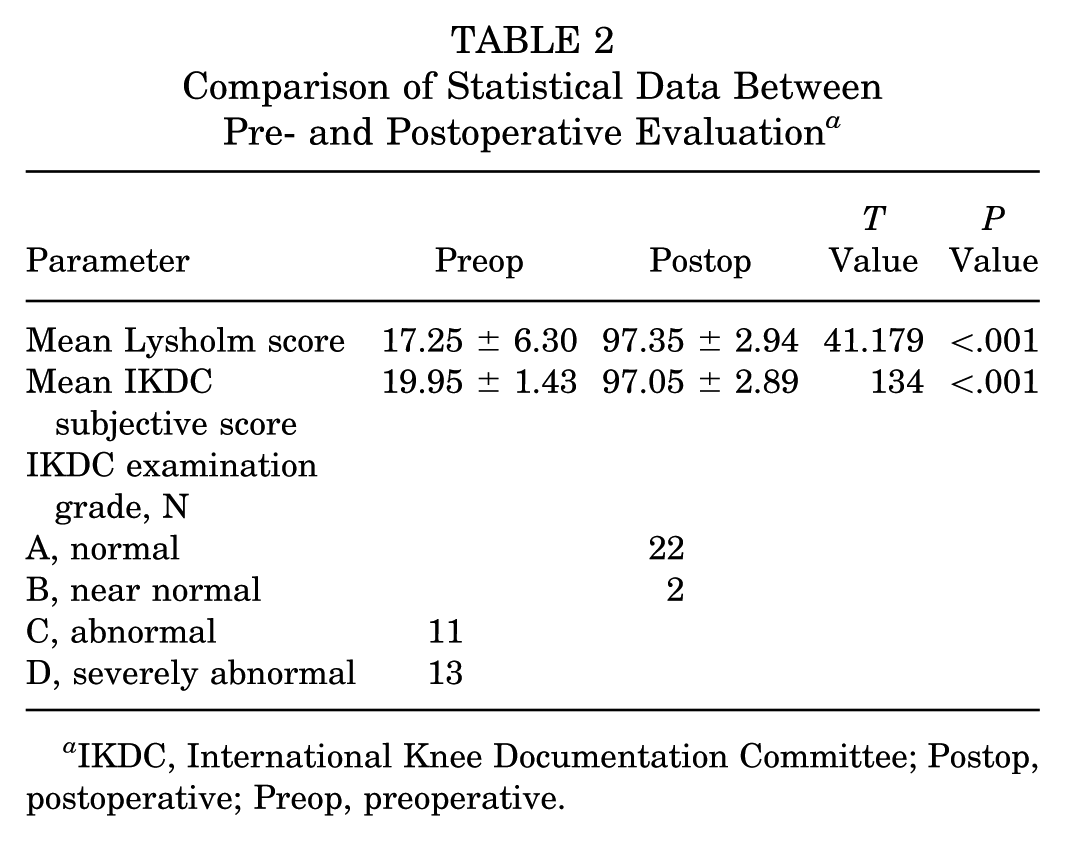
IKDC, International Knee Documentation Committee; Postop, postoperative; Preop, preoperative.
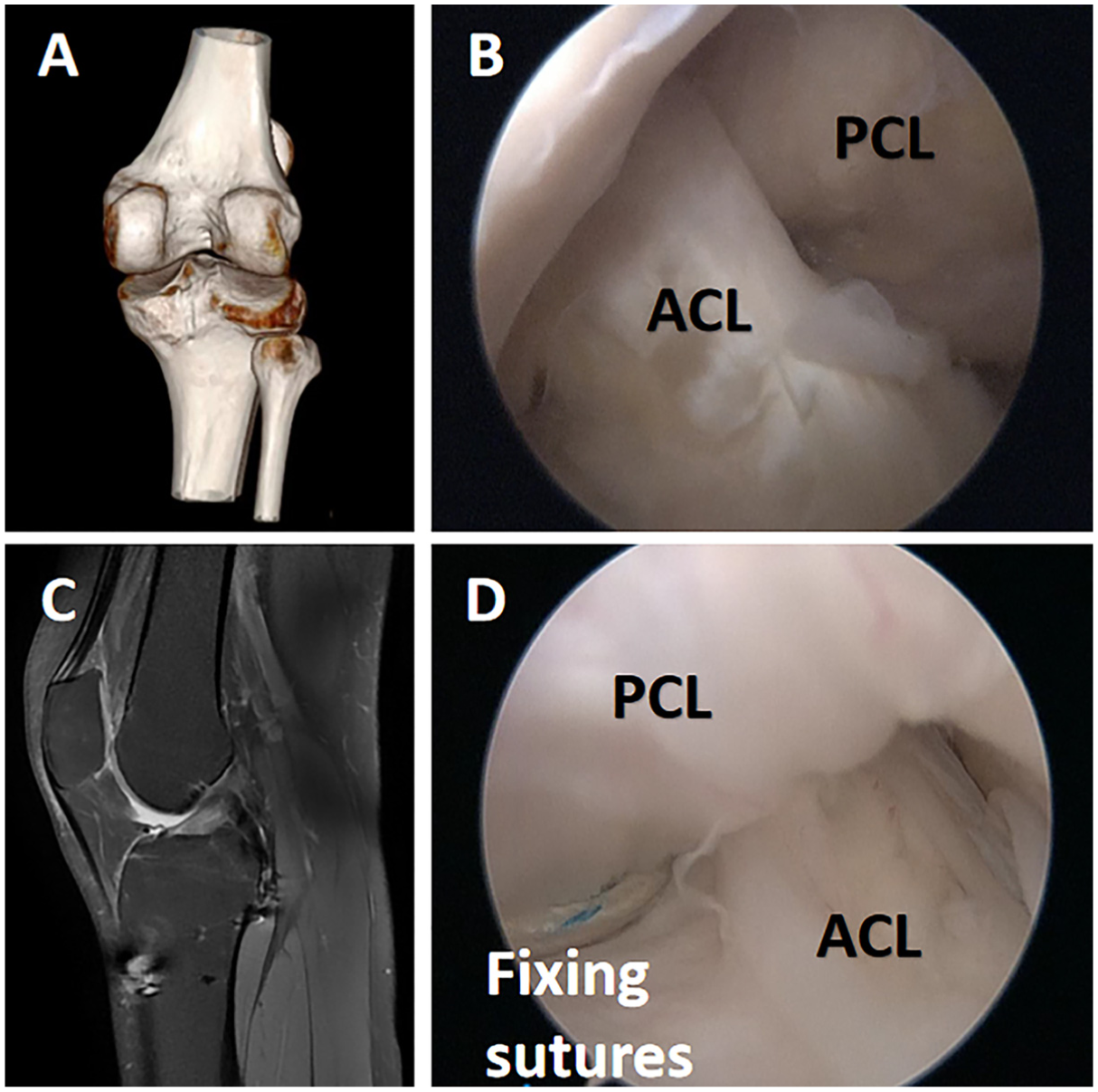
Postoperative imaging and examination. (A) Postoperative 3D CT scan showing the alignment of the fixation. (B) Second arthroscopic examination of the left knee in a 32-year-old patient, demonstrating satisfactory tension in both the ACL and the PCL. (C) Postoperative MRI of the knee, illustrating the position of the fixation. (D) No evidence of loosening or breakage of the fixation wires. ACL, anterior cruciate ligament; CT, computed tomography; MRI, magnetic resonance imaging; PCL, posterior cruciate ligament; 3D, 3-dimensional.
Discussion
In this retrospective study, we introduce a novel surgical approach for treating avulsion fractures of the PCL using arthroscopic anterior compartment loop-and-tack fixation. Based on our collected data, the mean duration of surgery was 50 ± 23.73 minutes, and the mean postoperative follow-up period was 30 ± 8 months. During the follow-up, significant improvements were observed in patients’ knee joint function, with substantial increases in key evaluation metrics, including the IKDC subjective score and IKDC examination grade. Furthermore, no severe postoperative complications, such as neurovascular injury, thrombosis, or bone block loosening, were observed in any cases. These findings further support the use of arthroscopic anterior compartment loop-and-tack as an effective and safe surgical technique for treating PCL avulsion fractures.
Some authors advocate nonoperative treatment with plaster fixation; however, the fracture did not heal after nonoperative treatment, so surgical treatment was recommended. 6 There is no consensus “gold standard” surgical approach. Some authors suggest that the fracture should be accessed through an inverted “L” incision in the posterior popliteal fossa of the knee in the prone position, along the medial head of the gastrocnemius muscle and the semimembranosus muscle, or through a small incision in the posterior knee to expose the fracture and fix it with hollow cancellous screws and spacers for fixation.6-9,13 However, most PCL tibial avulsion fractures are in multiple fragments. They are difficult to fix with hollow cancellous bone screws; thus, some authors have suggested drilling a bone channel from the anterior to the posterior fracture of the knee under arthroscopic surveillance, lancing the avulsion fracture and PCL with sutures, and fixing them with EndoButton suspension.1,19,20,22-24 In contrast to other authors11,15,22 who used arthroscopic suspension fixation of PCL tibial avulsion fractures with 2 or 3 bone channels 14 drilled in the tibia, this study utilized only 1 bone channel. The authors believe that after suture ligation of PCL tibial avulsion fracture, 2 tibial bone tracts do not promote the adjustment of the fracture, and drilling 2 bone tracts will significantly increase the operation time for additional checks, markings, and adjustments to ensure correct positioning and alignment. The observation of the posterior knee arthroscopic view is limited because of potential localized bleeding from the drilling procedure, as well as interference from bone debris or other postoperative changes that could obscure the arthroscope's field of view. Therefore, the authors believe that drilling 2 tibial tracts is not necessary. Some authors have placed suspension fixation at the PCL tibial avulsion fractures to compress the fracture block; however, the PCL tibial avulsion fracture block can be fixed with a hollow nail only when it is >20 mm. 18 The avulsion fracture is too small to accurately prepare a 4.5-mm diameter bone channel through the suture in its center by the cruciate ligament locator or EndoButton fixation. 3 Therefore, it is recommended to ligate the PCL tibial avulsion fracture with a high-strength wire. 14
Is complete anatomic reduction necessary for PCL tibial avulsion fractures? The authors contend that due to the loss of PCL function, posterior tibial sag, and ACL laxity associated with PCL tibial avulsion fractures, soft tissue entrapment between fracture ends can lead to nonunion. Therefore, meticulous debridement of fracture ends and achieving precise anatomic reduction are deemed essential.
In this study, patients underwent surgery a mean of 4 days after injury, with the procedure lasting approximately 1 hour. This technique enables efficient fracture reduction within a short timeframe. Compared with open surgery and techniques involving 2 bone tunnels, this method is less invasive, resulting in a reduced risk of neurovascular damage, improved wound healing, and a faster recovery of knee function. For surgeons, the loop-and-track technique offers a simpler and more convenient operation, is easier to learn and replicate, and helps reduce operating room time, leading to more efficient surgeries and improved treatment outcomes.
Limitations
There are limitations to our study. First, the sample included in this study exhibits a sex imbalance, which may introduce sex bias. Second, due to limitations in equipment availability, we did not utilize quantitative statistical indicators measured by the KT-1000 or KT-2000 arthrometer (MEDmeta) to assess knee stability. Additionally, we did not perform postoperative arthroscopy in each case. Third, the number of patients was insufficient, and further summary studies are needed. Fourth, our study only selected patients in the acute setting and may not be appropriate for more subacute or chronic fractures. Finally, there are no studies related to the biomechanical characteristics of sleeve fixation for PCL tibial avulsion fractures. This study was limited to assessing the feasibility of treatment by evaluating clinical outcomes.
Conclusion
Our loop-and-track technique treatment of PCL tibial avulsion fractures improves clinical outcomes with minimal complications. This technique may be considered in the treatment options for patients with PCL tibial avulsion fractures.
Footnotes
Final revision submitted May 29, 2025; accepted July 8, 2025.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Shenzhen Nanshan People's Hospital (no. LW-2023-001).