
Abstract
Background:
Biomechanical studies support the use of suture tape reinforcement for limiting graft elongation and increasing strength in knee ligament reconstructions.
Purpose:
To compare posterior cruciate ligament (PCL) laxity, complication and reoperation rates, and patient-reported outcomes (PROs) after all-inside single-bundle PCL reconstruction (PCLR) with versus without independent suture tape reinforcement.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A retrospective cohort study of consecutive patients who underwent primary, all-inside allograft single-bundle PCLR with and without independent suture tape reinforcement at a single academic institution from 2012 to 2019. Medical records were reviewed for patient characteristics, additional injuries, and concomitant procedures. PRO scores (including the International Knee Documentation Committee [IKDC], Tegner activity scale, and Lysholm scores), bilateral comparison kneeling radiographs, and physical examination findings were collected at a minimum of 2 years postoperatively.
Results:
Included were 50 patients: 19 with suture tape reinforcement (mean age 30.6 ± 2.9 years) and 31 without suture tape reinforcement (control group; mean age 26.2 ± 1.6 years). One PCLR graft in the suture tape group failed. Posterior drawer examination revealed grade 1+ laxity in 4 of 19 (21%) of the suture tape cohort versus 6 of 31 (19%) of the control cohort (P > .999). Bilateral kneeling radiographs showed similar side-to-side differences in laxity between the groups (suture tape vs control: mean, 1.9 ± 0.4 vs 2.6 ± 0.6 mm; P = .361). There were no statistically significant differences between the groups in postoperative IKDC (suture tape vs control: 79.3 vs 79.6; P = .779), Lysholm (87.5 vs 84.3; P = .828), or Tegner activity (5.6 vs 5.7; P = .562) scores.
Conclusion:
All-inside single-bundle PCLR with and without independent suture tape reinforcement demonstrated low rates of graft failure, complications, and reoperations, with satisfactory PROs at a minimum 2-year follow-up. Radiographic posterior tibial translation was comparable between the 2 groups.
The posterior cruciate ligament (PCL) is composed of the anterolateral and posteromedial bundles, providing primary restraint to posterior tibial translation (PTT). Isolated PCL injuries are often treated nonoperatively because of the potential for ligament healing. 34 However, acute PCL disruption is commonly associated with injuries to the anterior cruciate ligament (ACL), medial collateral ligament (MCL), and posterolateral corner (PLC). 45
Previous studies have reported increased rates of subsequent meniscus tears in PCL-deficient knees. 5 Recent reports with long-term follow-up identified a 6-fold higher rate of symptomatic arthritis in patients lacking a PCL when compared to patients with intact PCLs. 32 PCL reconstruction (PCLR) is currently recommended for symptomatic knee instability after nonoperative treatment and in the setting of a multiple ligament knee injury.
A variety of PCLR techniques have been described using autograft versus allograft, 16,41 single versus double bundle, 31 and open inlay versus arthroscopic transtibial. 27 Although data directly comparing each of these techniques are sparse, reported clinical outcomes have demonstrated no significant differences. 1,35 Ligament repair or reconstruction with the addition of an internal brace has resulted in improved biomechanics, including decreased cyclic displacement and increased load to failure, in addition to encouraging clinical results. 11,37 A recent cadaveric study of all-inside PCLR with and without internal brace augmentation revealed that suture tape reinforcement improved initial stability by decreasing PTT to levels similar to the PCL-intact knee. 12 In another cadaveric biomechanical study, the addition of suture tape resulted in decreased total graft elongation and increased ultimate strength independent of suspensory versus interference fixation. 25
The purpose of our study was to compare (1) PCL laxity, (2) complication and reoperation rates, and (3) patient-reported outcomes (PROs) after all-inside single-bundle PCLR with and without independent suture tape reinforcement at a minimum 2-year follow-up. We hypothesized that PCLR with suture tape reinforcement would result in equivalent complications, reoperations, and PROs but improved posterior translation on kneeling stress radiographs.
Methods
After receiving institutional review board approval, we identified consecutive patients who underwent a primary PCLR using the all-inside technique 9,27,30,40 from October 2012 to January 2019. Over the study period, all surgeries were performed by fellowship-trained orthopaedic surgeons (M.J.S. and B.A.L.). Inclusion criteria consisted of patients who (1) underwent all-inside allograft single-bundle PCLR with or without independent suture tape reinforcement and (2) were available for follow-up regarding confirmation of any complications, reoperations, and current PROs. Exclusion criteria consisted of (1) revision PCLR and (2) follow-up duration <2 years. Patients were divided into 2 groups: reconstruction with suture tape reinforcement (suture tape group) and reconstruction without suture tape reinforcement (control group). Between 2012 and 2017, the all-inside PCLR technique did not include internal brace augmentation; however, surgeries performed between 2017 and 2019 did incorporate internal brace into the reconstruction.
A total of 66 patients who underwent PCLR with the all-inside technique between October 2012 and January 2019 were identified. Of these patients, 16 were excluded: 4 underwent revision PCLR as the initial procedure at our institution, and 12 were lost to follow-up. As a result, 50 patients (81%) were eligible for final inclusion for analysis in the study, with 19 patients in the suture tape group and 31 patients in the control group (Figure 1).

Flowchart of study patients in the suture tape and control cohorts. (PCLR, posterior cruciate ligament reconstruction.)
Surgical Technique
The preferred technique of the surgeons was all-inside PCLR using a quadrupled peroneus longus or tibialis anterior tendon allograft with both tibial and femoral suspensory fixation. 40 A quadruple looped allograft with a final length of approximately 90 mm with a final diameter between 10 and 12 mm was used for all reconstructions. A 40-mm tibial socket was drilled using the anatomic PCL Tibial Guide (Arthrex) and the FlipCutter II (Arthrex). The femoral socket was typically prepared through an inside-out approach to protect the articular cartilage of the femur. A low-profile cannulated reamer was used to drill a 25-mm socket. The double suspensory mechanism utilized a TightRope RT (Arthrex) for the femoral socket and a TightRope ABS (Arthrex) for the tibial socket. For the suture tape reinforcement group, suture tape reinforcement was achieved by looping the suture tape through the femoral button. This allowed for independent tensioning and fixation through an anchor on the tibia (Figure 2).

Quadruple tibialis anterior allograft with independent suture tape reinforcement (ST). The suture tape is looped independently in the femoral suspensory button and approximated to the graft with a circumferential running absorbable suture.
Final tensioning was completed on the femoral and tibial loops at 90° of flexion with a slight anterior drawer and backup fixation of tibial sutures on the tibial cortex was achieved using a 5.5-mm SwiveLock anchor (Arthrex). For the suture tape reinforcement group, after final graft tensioning, any creep was removed from the suture tape before fixing it independently with an additional SwiveLock anchor with the knee at 90° of flexion (Figure 3).

(A) View of the left knee at 90° of flexion through the anteromedial viewing portal with a 30° arthroscope showing combined single-bundle PCL reconstruction/graft (PCL-G) with suture tape reinforcement (ST) and anterior cruciate ligament (ACL) reconstruction/graft (ACL-G). (B) View of the left knee at 90° of flexion through the anteromedial viewing portal with a 30° arthroscope showing isolated single-bundle PCL-G without suture tape reinforcement and ACL. F, femur.
The rehabilitation was standardized between the groups and has been described in detail. 9,24,40 Briefly, touch weightbearing during ambulation with crutches and a custom PCL brace locked in extension were allowed for the first 6 weeks. Gradual weightbearing was introduced with a goal of full range of motion and normal gait at 12 weeks; bracing was continued for up to 12 months postoperatively.
Outcome Evaluation
Patient charts were individually reviewed to obtain patient characteristics, preoperative physical examination findings, operative details, concomitant injuries, reoperations, complications, and PROs (Tegner activity scale, Lysholm score, visual analog scale for pain [VAS; 0-10], and International Knee Documentation Committee [IKDC] scores). 6,17 Clinical outcomes including range of motion, physical examination findings at final follow-up, and bilateral comparison kneeling stress radiographs were also reviewed. Patients with isolated PCL injuries were denoted as such, and those with multiligament injuries were assigned knee dislocation (KD) grades according to the Schenck classification system. 33 Surgical interval was categorized as acute (<3 weeks from injury), semiacute (3-6 weeks from injury), or delayed (>6 weeks from injury). 23 Patients were contacted for follow-up via telephone to obtain PROs when necessary. All patients were assessed by physical examination performed by the operating surgeon during clinical follow-up. PCLR failure was defined as graft rupture on magnetic resonance imaging (MRI), PCL laxity grade ≥2, side-to-side difference (SSD) in laxity ≥5 mm on radiograph, or need for revision PCLR.
PCL laxity was evaluated by physical examination and by measuring the SSD on postoperative bilateral kneeling stress radiography using the technique by Jackman et al. 18 In total, 33 patients had postoperative bilateral kneeling stress views obtained at a minimum of 1 year. All measurements were performed and verified by an independent fellowship-trained sports medicine orthopaedic surgeon (E.T.). All postoperative stress radiographs were read by musculoskeletal-trained radiologists who were blinded to the procedure performed.
Statistical Analysis
Data were analyzed using JMP Pro Version 14 (SAS Institute). Baseline patient characteristics were presented as means, medians, and percentages, with ranges or standard error of mean when appropriate. Data were analyzed for parametric/nonparametric assumptions, and continuous variables were analyzed using Student t tests or Wilcoxon rank-sum tests. Categorical variables were analyzed using chi-square analysis or Fisher exact tests when appropriate. Statistical significance was defined as P <.05.
Results
As described above, 50 patients were eligible for final study inclusion and analyses; 38% of the study population underwent reconstruction with suture tape (Figure 1). The average clinical follow-up time was 60 months (range, 24-96 months) in the control group versus 34.6 months (range, 24-51) in the suture tape group (P < .001). There were no other significant differences between the groups regarding patient characteristics. The characteristics of the cohorts are listed in Table 1, while pre-operative examination findings are shown in Table 3.
Characteristics of the Study Cohorts a

a Data are expressed as mean ± SEM (95% CI) or n (%). Boldface P value indicates a statistically significant difference between groups (P < .05). VAS, visual analog scale.
Injury characteristics and additional operative procedures performed at the time of PCLR are displayed in Table 2. Three patients in the control group had staged procedures, and 1 patient in the suture tape cohort had a staged procedure. There were no differences in injury characteristics or additional procedures.
Patient Injury Characteristics and Additional Procedures a

a Data are expressed as n (%). ACL, anterior cruciate ligament; LCL, lateral collateral ligament; MCL, medial collateral ligament; PLC, posterolateral corner; PMC, posteromedial corner.
Preoperative Physical Examination Findings and KD Grade a

a Data are expressed as n (%). KD, knee dislocation; PCL, posterior cruciate ligament.
b According to Schenck classification. 33
There were no differences in postoperative PROs between the cohorts, excluding postoperative VAS at rest, which was statistically decreased in the suture tape cohort (0 vs 0.4; P = .047) (Table 4). However, this 0.4-point difference between groups in resting VAS is unlikely to be clinically significant. The control group had more concomitant injuries, although this did not reach statistical significance. Univariate analysis of concomitant injuries showed no significant impact on 2-year clinical outcomes.
The results of the posterior drawer examination were comparable between the groups at the final follow-up, with grade 1 laxity in 4 patients in the suture tape group and 6 patients in the control group. No patient had a grade 2 or grade 3 posterior drawer on final follow-up. Bilateral kneeling stress radiographs were collected for 33 patients, including all 19 patients in the suture tape cohort and 14 patients in the control cohort (Table 4). The mean time to kneeling stress radiographs was 20.2 months in the suture tape group and 25.0 months in the control group. There was no difference in laxity measurements between cohorts, with a mean SSD difference of 1.9 mm in the suture tape group and 2.6 mm in the control group (P = .361) (Figure 4).
Patient Outcomes at Final Follow-up a

a Data are expressed as mean ± SEM (95% CI) or n (%) with ranges as indicated. Boldface P value indicates a statistically significant difference between groups (P < .05). IKDC, International Knee Documentation Committee; VAS, visual analog scale.
b Collected for 19 patients in the suture tape cohort and 14 patients in the control cohort.
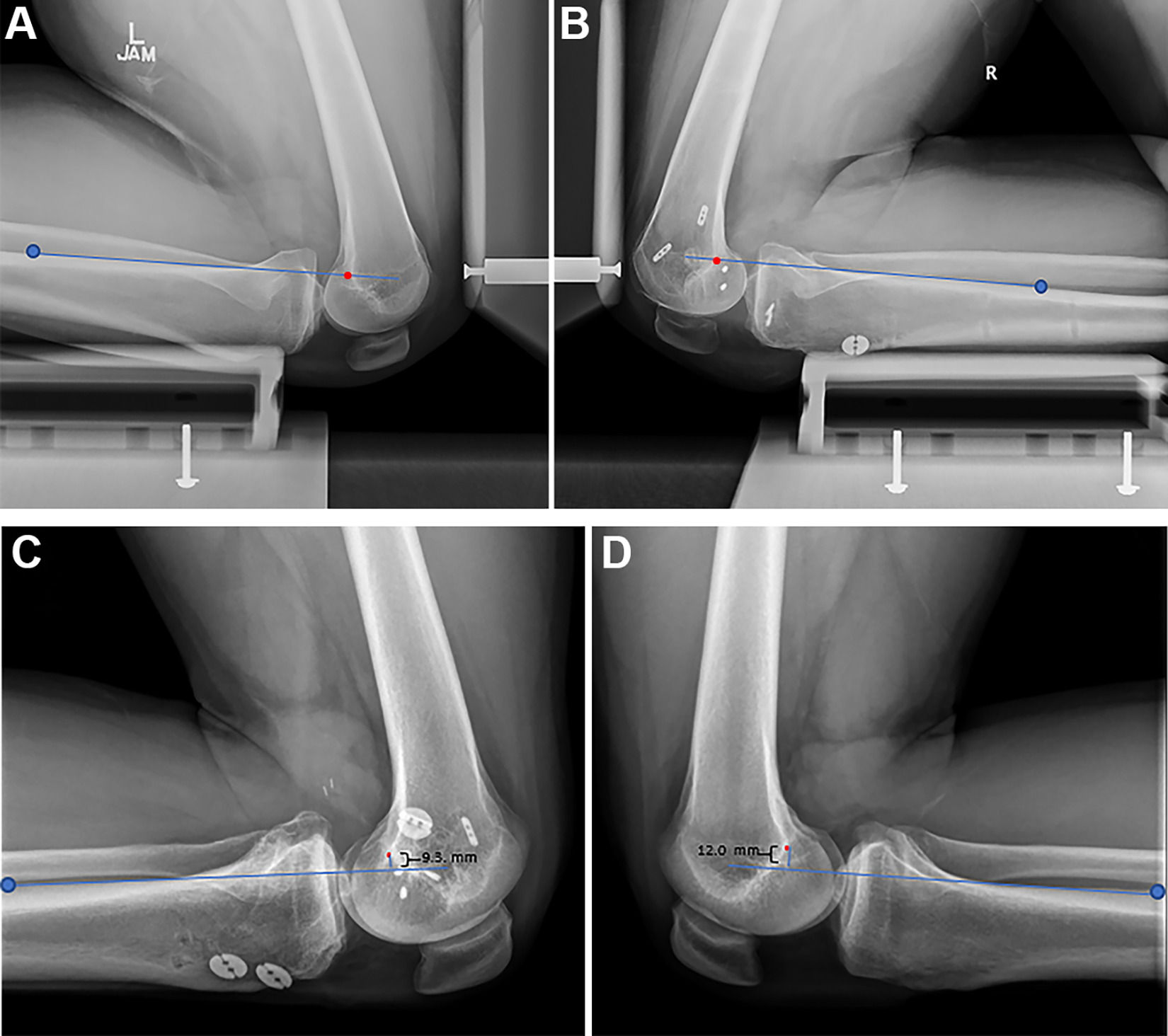
Bilateral postoperative kneeling stress radiographs of the (A) uninjured left knee and (B) operated right knee after combined posterolateral corner (PLC) and posterior cruciate ligament (PCL) reconstruction with PCL graft suture tape reinforcement. There was no side-to-side difference in posterior tibial translation. Bilateral postoperative kneeling stress radiographs of the (C) left knee after combined anterior cruciate ligament, PCL, and PLC reconstruction without PCL suture tape reinforcement and (D) uninjured right knee. There was a 2.7-mm increase in posterior tibial translation at 2 years after combined reconstruction. Posterior tibial translation was measured from a line along the posterior tibial cortex (blue line) starting 15 cm distal to the tibial plateau (blue dot) to the most posterior aspect of the Blumensaat line (red dot), as described by Jackman et al. 18
Complications and reoperations are shown in Table 5. One patient in the suture tape reinforcement cohort experienced graft failure. A total of 26% of the suture tape patients (5/19) and 10% of the control patients (3/31) had a reoperation (P = .232). Reoperations in the suture tape cohort included 2 multiligament knee reconstruction revision surgeries (1 patient with ACL/PCL/PLC reinjury at 2 years postoperatively after a noncontact pivoting injury and 1 patient with ACL/MCL revision at 1 year postoperatively due to a noncontact pivoting injury after previous ACL/PCL/MCL/PLC reconstruction), 2 superficial wound infections, 1 meniscal surgery with chondroplasty, and 1 arthroscopic lysis of adhesions for arthrofibrosis. In the control cohort, 2 patients developed arthrofibrosis that required arthroscopic lysis of adhesions, and 1 patient had a superficial wound infection requiring incision and drainage.
Complications and Reoperations a
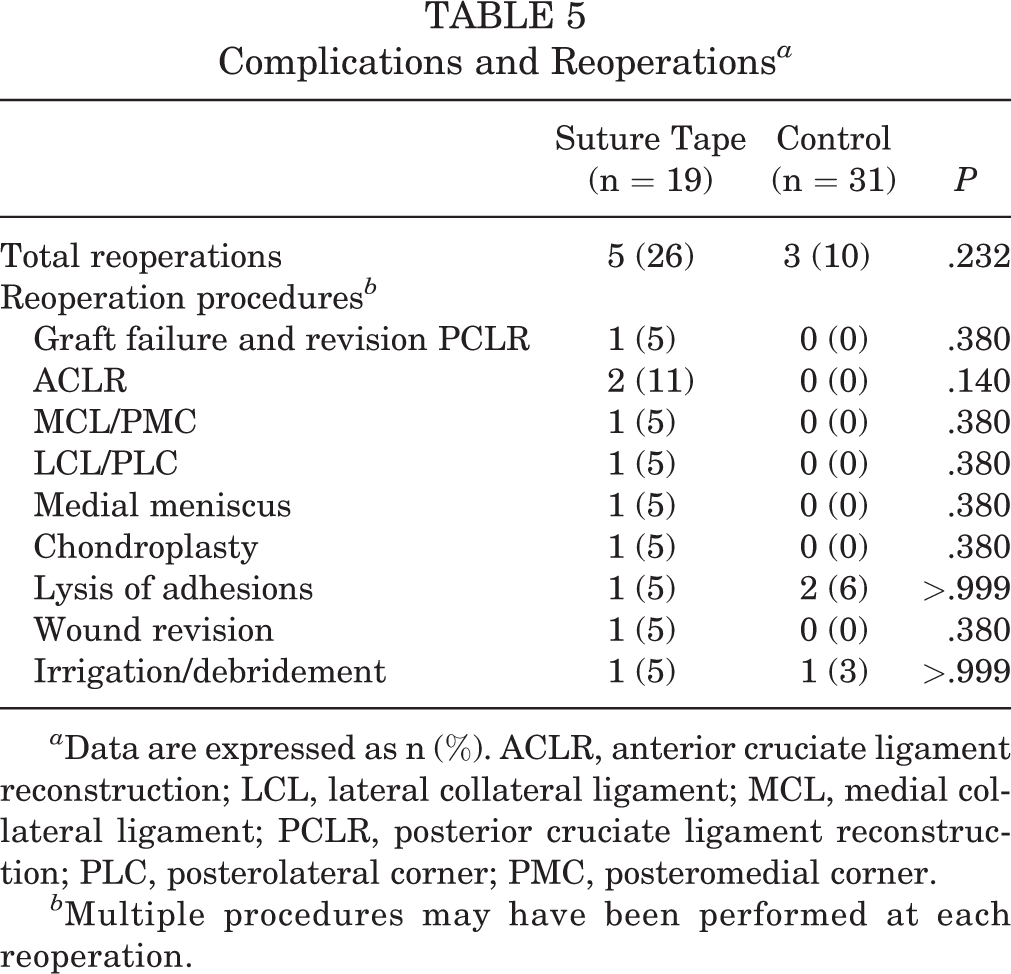
a Data are expressed as n (%). ACLR, anterior cruciate ligament reconstruction; LCL, lateral collateral ligament; MCL, medial collateral ligament; PCLR, posterior cruciate ligament reconstruction; PLC, posterolateral corner; PMC, posteromedial corner.
b Multiple procedures may have been performed at each reoperation.
Discussion
The main findings of this study are that all-inside PCLR with or without suture tape reinforcement demonstrated low rates of complication, reoperation, and graft failure. Postoperative PCL laxity assessed by bilateral stress radiography at a minimum of 12 months was similar in both groups. Single-bundle PCLR with suture tape reinforcement did not result in significantly different clinical outcomes at a minimum 2-year follow-up compared with PCLR without suture tape reinforcement.
Persistent posterior laxity after PCLR is not uncommon, especially in the setting of a multi-ligamentous knee injury, in which other ligamentous structures may be at risk. Tunnel malposition, missed associated ligament injuries, decreased tibial slope, overly aggressive physical therapy, and patient nonadherence in the early postoperative period have all been associated with graft elongation. 19 Recent biomechanical studies on PCLR with the addition of suture tape reinforcement have demonstrated decreased graft elongation and increased ultimate load to failure. 11,37 Suture tape reinforcement may have the advantage of decreasing graft stress elongation during the proliferation, maturation, and ligamentization phases for soft tissue PCL grafts. 2,38
Artificial ligaments have the potential advantages of early return to function and limited need for biologic integration. 36 However, these constructs have been associated with increased complication rates due to synovitis, postoperative arthrofibrosis, and lower functional outcomes in the ACL reconstruction population. 3,44 Newer synthetic ligament augmentation devices have shown encouraging results in short- and mid-term outcomes for ankle ligament, 47 thumb ulnar collateral ligament, 10 elbow ulnar collateral ligament, 8 knee MCL injuries 26 and ACL 29 reconstruction, as well as ACL and PCL repair. 14,15,42 The use of suture tape has also been studied for rotator cuff repairs with no associated increases in rates of complication. 4
In the current study, there was no statistical difference in reoperation rates between groups. However, the suture tape reinforcement cohort did have more reoperations, including 2 multiligament knee reconstruction revision surgeries after traumatic injury (1 involved the PCL) and 2 superficial wound infections treated with surgical wound debridement, closure, and oral antibiotics. Interestingly, 2 patients had a reoperation for lysis of adhesion in the control group and 1 in the suture tape reinforcement group.
The use of suture tape in various ligament reconstruction techniques employs suspensory fixation with independent tensioning of the graft and the tape. Historically, ACL augmentation devices have been associated with high failure rates, and the concept of graft reinforcement and load sharing with suture tape has recently been suggested. A biomechanical study by Bachmaier et al 2 examined suture tape reinforcement compared with augmentation in ACL reconstruction using suspensory fixation. The soft tissue graft reinforcement leads to higher ultimate load to failure and reduced elongation, without stress shielding the soft tissue graft. This biomechanical study of ACL grafts might be transferable to PCL grafts using double suspensory fixation as described in the current study.
A recent biomechanical study demonstrated that adding a 2-mm suture tape to an all-inside quadrupled PCLR led to reduced total graft elongation while increasing ultimate strength to failure. 25 These results were obtained using either a tibial and femoral suspensory device or a suspensory device on the femur and an interference screw on the tibia. 25
Another biomechanical study of 11 knees comparing PTT in all-inside versus transtibial single-bundle PCLR with or without suture tape reinforcement was performed. 12 Single-bundle all-inside PCLR without reinforcement restored normal PTT except at 90° of knee flexion. Suture tape reinforcement to the all-inside reconstruction construct resulted in statistically comparable PTT with the intact knees at all flexion angles. When using a transtibial technique without augmentation, PTT was increased compared to intact knees at 60°, 90°, and 120° of flexion. Suture tape augmentation to this construct showed PTT comparable to the intact knee at flexion angles of 30°, 60°, and 120°. However, the all-inside PCLR with suture tape augmentation provided the best posterior stability and was the only construct with normal posterior translation at 90° compared with intact knees. These data support the theoretical biomechanical advantage of suture tape augmentation in PCLR.
Recently, Parkes et al 29 investigated clinical outcomes in a young patient population after ACL reconstruction using hamstring autograft with or without suture tape reinforcement. They reported no adverse outcomes with the use of suture tape reinforcement and showed similar IKDC and Lysholm scores, but reported a 0.7-point difference in Tegner scores, favoring the suture tape group. In the current study, PCLR with and without suture tape reinforcement resulted in excellent functional outcome scores at a minimum 2-year follow-up. Moreover, there were no increased rates of complication or failure reported in the suture tape group.
Although many different surgical techniques have been described for PCLR, no single technique has been shown to achieve superior functional and clinical outcomes. 7,22,48 Biomechanical studies support the double-bundle reconstruction technique to better restore native knee biomechanics and control PTT than the anatomic single-bundle reconstruction technique; however, reported functional outcome scores are similar. 13,21,28,46
The results of our study indicated an SSD in laxity after single-bundle PCLR of 1.9 ± 0.4 mm (95% CI, 1.0-2.8) with suture tape and 2.6 ± 0.6 mm (95% CI, 1.3-3.9) without suture tape (P = .361). The control group had slightly increased posterior translation postoperatively compared with the suture tape group, although this difference did not reach statistical significance. These results support the effectiveness of our reported technique to restrain posterior translation of the tibia and reestablish knee biomechanics with or without suture tape reinforcement. The reported SSDs for posterior tibial laxity measurements and functional outcome scores are also comparable with previously reported data. 20,22,39,43
This is the first clinical study to our knowledge that investigates PCLR suture tape reinforcement. Given the rarity of PCLRs, this is a relatively large cohort study with comparable characteristics between the 2 groups. Bilateral kneeling stress radiographs allowed for objective side-to-side posterior tibial laxity measurements and did not demonstrate any significant difference between the suture tape reinforcement group and the control group.
Limitations
This study is not without limitations. Given the low incidence of isolated PCL injuries, we included patients with combined and multiligament knee injuries. This led to an inherent heterogeneous patient population. This is further exemplified by the variety of KD grades between the cohorts. Additionally, all procedures were completed by fellowship-trained surgeons practicing in a high-volume academic center, which could limit the generalizability of the findings, particularly related to functional outcomes and postoperative laxity. Because of the retrospective nature of the study, it was not initially powered to determine if there was a clinical difference from the use of suture tape reinforcement after all-inside PCLR. Clinical results were not correlated with postoperative MRI assessment to document graft integration. Finally, bilateral comparison kneeling stress radiography was available only in a subset of patients.
Conclusion
All-inside single-bundle PCLR with and without independent suture tape reinforcement demonstrated low rates of graft failure, complications, and reoperations with satisfactory PROs at a minimum 2-year follow-up. Radiographic PTT was comparable between the 2 groups.
Footnotes
Final revision submitted July 11, 2022; accepted August 23, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: Support was received from the Foderaro-Quattrone Musculoskeletal-Orthopaedic Surgery Research Innovation Fund. This study was partially funded by the National Institute of Arthritis and Musculoskeletal and Skin Diseases for the Musculoskeletal Research Training Program (grant T32AR56950). A.P. has received hospitality payments from Medical Device Business Services. A.J.K. has received grant support from DJO; consulting fees from Arthrex, JRF Ortho, and Responsive Arthroscopy; speaking fees from Arthrex; royalties from Arthrex and Responsive Arthroscopy; and honoraria from Vericel and JRF Ortho. A.P. is a board member for the Musculoskeletal Transplant Foundation. M.J.S. has received education payments from Elite Orthopedics. B.A.L. has received education payments from Linvatec, consulting fees from Arthrex, speaking fees from Arthrex and Smith & Nephew, and royalties from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Mayo Clinic (reference No. 15-000601).