
Abstract
Background:
Shoulder instability is one of the most common problems in judo. Some studies have examined outcomes of shoulder stabilization in judo athletes. While open procedures yield acceptable results, arthroscopic stabilization has yielded poor outcomes or involved small sample sizes. For >20 years, the authors have treated competitive judo athletes with soft tissue Bankart repair and soft tissue augmentation, such as rotator interval closure.
Purpose:
To present the results of a treatment algorithm for arthroscopic soft tissue stabilization with selective augmentation in competitive judo athletes, with special emphasis on the risk of recurrence, range of motion restrictions, and return-to-sport outcomes
Study Design:
Case series; Level of evidence, 4.
Methods:
Competitive judo athletes who underwent arthroscopic soft tissue shoulder stabilization for recurrent traumatic anterior shoulder instability between August 2004 and December 2015 were included. Patients with <2 years of follow-up were excluded. All procedures were performed according to the treatment algorithm. Outcomes assessed included recurrence, return to sport, range of motion, Rowe score, and Subjective Shoulder Value for sports (SSV-sports).
Results:
A total of 84 shoulders in 78 competitive judo athletes (58 male, 20 female; mean age at surgery, 19 years) were included. Among them, 6 athletes (4 male, 2 female) underwent bilateral surgery, resulting in 62 shoulders from male athletes and 22 shoulders from female athletes. The mean follow-up was 65 months (range, 24-166 months). All procedures were performed according to the treatment algorithm. The overall recurrence rate was 4.8% (4/84 shoulders), and all recurrences occurred in the tsurite group. The mean loss in abduction–external rotation was observed but did not affect return to sport. Among the 74 patients without recurrence, 69 (93%) returned to the same or higher preinjury competition level. The Rowe and SSV-sports scores were significantly improved postoperatively.
Conclusion:
The treatment algorithm for arthroscopic soft tissue shoulder stabilization in competitive judo athletes resulted in good clinical outcomes, with low recurrence rates and a high rate of return to preinjury levels in tsurite- as well as hikite-side shoulders.
Judo is a competitive martial art that has developed in Japan. Since the first contest in the 1964 Olympic Games in Tokyo, judo has achieved worldwide popularity. Judo includes various techniques, such as throwing and grappling. These techniques pose a potential risk of both upper and lower extremity injuries. Injuries in the upper extremity are the most common, accounting for 41% of all judo injuries, and more than half of the upper extremity injuries occur in the shoulder. 1 Uchiyama et al 26 reported that the prevalence of traumatic shoulder instability in top-level collegiate teams in Japan was 8.9%.
In judo, each arm requires different functional characteristics: tsurite and hikite (Figure 1). Normally, the dominant arm tends to be used as tsurite, and the nondominant arm as hikite. Tsurite, which means the hand for pulling up, usually grips the lapel of the opponent's uniform around the neck. Hikite, which means the hand for pulling, usually grips and pulls the opponent's sleeve. Tsurite is usually used with the shoulder abducted and requires shoulder external rotation when throwing the opponent, while hikite is used in the adducted position (Figure 2). 26

Grips of judo. (1) Tsurite grips the left lapel of the opponent. (2) Hikite grips the right sleeve of the opponent.

Throwing the opponent. The tsurite-side shoulder requires external rotation in the abducted position.
Accordingly, a normal range of external rotation is vital for the tsurite-side shoulder, especially external rotation in shoulder abduction. Open surgeries often cause restrictions in shoulder external rotation,26,28 which may be responsible for the low complete return rate on the tsurite side. 26 The coracoid transfer procedure has been shown to be effective in managing anterior shoulder instability with labral injury and/or glenoid bone loss, particularly in high-risk collision athletes, offering superior stability and a low recurrence rate of dislocation. 2 However, as a nonanatomic technique, it has been associated with potential complications such as restricted external rotation, neurological injury, graft nonunion or osteolysis, and progressive glenohumeral osteoarthritis. 2 These concerns warrant caution when considering the procedure in athletes, such as judokas, for whom preservation of shoulder range of motion (ROM) is critical for performance. We have been performing arthroscopic Bankart repair (ABR) with or without rotator interval closure (RIC) in all collision/contact athletes, including judo athletes, except for in shoulders with critical glenoid bone loss (>25%), to minimize the risk of ROM loss. 12 Since 2012, we have been adding Hill-Sachs remplissage (HSR) as a selective augmentation for high-risk collision/contact athletes to reduce recurrences. 17 HSR is known as an effective arthroscopic procedure to reduce recurrence rates but may pose the risk of external rotation loss.5,8 We have been less frequently indicating HSR for tsurite-side shoulders to preserve external rotation while positively indicating it for the hikite side. However, differences in the outcomes between tsurite- and hikite-side shoulders have not been elucidated.
The aim of this study was to assess the outcomes of our algorithm for arthroscopic soft tissue stabilization in competitive judo athletes, with particular attention toward arm dominance (tsurite vs hikite), recurrence, and return to sport (RTS).
Methods
Patients
This study was a single-center, retrospective case series that was approved by our institute's review board (proposal IRB/ERC No. 2017014, obtained on June 22, 2017), and all participants provided written informed consent. Judo athletes who underwent arthroscopic shoulder stabilization at our institute between August 2004 and December 2015 were abstracted from the patient database. The inclusion criteria of this study were as follows: (1) competitive judo athletes, (2) recurrent traumatic anterior shoulder instability, and (3) arthroscopic soft tissue stabilization without bone grafting. The exclusion criteria were as follows: (1) retirement for reasons other than medical reasons and (2) <2 years of follow-up. All surgical procedures were performed by one of the senior surgeons (H.S., N.T., K.M., and M.T.) or a fellow under close supervision of the senior surgeons.
Data Collection
Medical records were reviewed to collect patient data, including demographics, ROMs, recurrence, complications, Rowe score, 20 and Subjective Shoulder Value for sports score (SSV-sports).3,10 Clinical evaluation was performed by one of the senior surgeons. ROM, including flexion, external rotation at the side, and external rotation at 90° of abduction, was measured using a goniometer. Internal rotation was evaluated as the spine level reachable by the thumb. Akoto et al 1 classified athletes into 5 levels: international elite (places 1-5 at the Olympic Games or world championships), international (national team), national (national championships medal), regional (first or second national league), or recreational sports. In this study, competitive athletes were defined as international elite, international, national, and regional athletes.
RTS was investigated using a questionnaire administered at the final follow-up by mail or telephone. The questionnaire included postoperative sports activity levels and the time to RTS. The postoperative sports activity levels were divided into 4 grades according to the classification of Gerometta et al 9 : (1) superior to the preoperative level, (2) identical, (3) inferior, and (4) change of sports.
Radiographic Evaluation
All shoulders were evaluated preoperatively using 3-dimensional (3D) reconstructed computed tomography (CT) (Alexion; Canon Medical Systems Corporation). The scanning parameters were as follows: image matrix, 512 × 512; pixel size, 0.5 × 0.5 mm; and slice pitch, 0.5 mm. The glenoid morphology and bone loss were assessed using the en face view of 3D-CT images and an image viewer (ShadeQuest/ViewC; FUJIFILM Medical Solutions Corporation).
The glenoid morphology was classified into 3 types: normal, attritional, and bony Bankart.15,23,24 The size of the glenoid bone loss was calculated as a percentage loss of the diameter of the best-match circle on the inferior aspect of the glenoid.15,23,24
The Hill-Sachs lesions were assessed with the maximum depth on axial CT images. A small defect was defined as having a depth <3 mm, and a large defect as having a depth ≥3 mm. 16 The location of the Hill-Sachs lesions was evaluated using the glenoid track concept (on- or off-track lesion). 27
Surgical Strategy
We performed ABR in all judo athletes, except for in shoulders with >25% glenoid bone loss, where bone grafting is indicated. Bony Bankart lesions were repaired without resection, with the bony fragment incorporated into the Bankart repair.15,23 RIC incorporating the subscapularis tendon was performed as an augmentation in most shoulders. 12
Although the indications for HSR were comprehensively determined considering various factors, such as age, sex, joint laxity, and athletic levels, our general principle was as follows. For the hikite side, HSR was performed for shoulders with 13.5% to 25% glenoid bone loss regardless of the size of the Hill-Sachs lesions, as ≥13.5% glenoid bone loss was considered subcritical bone loss associated with poor clinical outcomes. 21 HSR was also performed for shoulders with <13.5% glenoid bone loss combined with a large Hill-Sachs lesion. For the tsurite side, HSR was only performed for shoulders with 13.5% to 25% glenoid bone loss combined with a large Hill-Sachs lesion to minimize the risk of external rotation loss.
All other lesions, such as superior labrum anterior and posterior (SLAP) lesions, capsular tears, humeral avulsion of the glenohumeral ligament lesions, and partial articular surface tendon avulsion, were also repaired arthroscopically.
Surgical Techniques
All surgeries were performed in the beach-chair position under general anesthesia,11,15 and joint laxity of both shoulders was preoperatively assessed. The standard posterior portal was used as the viewing portal, and the anterior and anterosuperior portals were used as the working portals. After investigation of the glenohumeral joint, separation and mobilization of the labroligamentous complex from the glenoid neck were performed from the 2- to the 7-o’clock position (right shoulder) using an elevator, rasps, scissors, shavers, and a radiofrequency instrument introduced through the anterior portal. A small amount of the articular cartilage was curetted from the anteroinferior edge of the glenoid to promote tissue healing. The freed labroligamentus complex was repaired using at least 4 suture anchors (Gryphon BR, DePuy Synthes; Osteoraptor OS, Smith & Nephew) inserted between the 2- and 6-o’clock positions. The labroligamentous complex was cranially pulled up with a grasper that was introduced through the anterosuperior portal to restore proper tension of the labroligamentous complex.
RIC was performed in most cases as an augmentation to Bankart repair. After confirming that there was no significant restriction in external rotation intraoperatively, a high-strength suture was passed through the superolateral edge of the subscapularis tendon with the arm in the neutral position. The arm was then externally rotated beyond 60°, and the same suture was passed through the anterior capsule just posterior to the long head of the biceps tendon. An additional suture was placed more medially using the same technique. Finally, the knot was tied blindly through the anterior portal with the arm maintained in >60° of external rotation. This technique was aimed at minimizing the risk of postoperative external rotation loss.
HSR was selectively performed for shoulders with large or off-track Hill-Sachs lesions, following modifications of the original technique described by Purchase et al. 17 Two or 3 suture anchors were inserted into the valley of the Hill-Sachs lesion. The sutures were placed in the infraspinatus muscle, teres minor muscle, and thick capsule between the 2 tendons using a suture grasper (DePuy Synthes). To ensure appropriate placement and minimize the risk of motion restriction, we directly visualized the attachment sites of the infraspinatus and teres minor muscles from the subacromial space and carefully confirmed the suture positions before passage. All sutures were tied under direct subacromial visualization. 12
SLAP lesions were classified intraoperatively according to the classification system of Snyder et al. 22 When instability of the superior labrum was confirmed, repair using suture anchors was performed. Anterior-only repair or combined anterior and posterior repair was selected based on lesion morphology and labral mobility.
Postoperative Protocol
After 3 weeks of immobilization using a brace, passive and assisted-active exercises were initiated. Three months after the surgery, patients started a strengthening program. Judo practice was allowed at 4 months after surgery, starting from uchikomi (the repeated practice of the throwing techniques) according to the functional recovery of each patient. Randori (free sparring) was usually allowed at 5 or 6 months postoperatively after achieving good shoulder function, followed by a return to competition.
Statistical Analysis
Pathology, RTS, and clinical outcomes were compared between tsurite- and hikite-side shoulders. The Mann-Whitney U test, chi-square test, and Fisher exact probability test were used to compare the 2 groups. The Wilcoxon signed-rank test was used to compare pre- and postoperative data. The level of significance was set at a P value <.05. All statistical analyses were conducted using R Version 4.0.5 (R Foundation for Statistical Computing).
Results
Patients
Between August 2004 and December 2015, 117 shoulders in 107 consecutive competitive judo athletes underwent shoulder stabilization at our institute. Of these, 5 shoulders were excluded owing to >25% glenoid bone loss requiring bone grafting (n = 2) or multidirectional instability (n = 3). Among the remaining 112 shoulders, 2 were excluded due to patient retirement unrelated to medical issues, and 26 were lost to follow-up (follow-up rate, 76%). Ultimately, 84 shoulders in 78 patients were included in the final analysis (Figure 3).

Flow diagram for patient selection.
Patient characteristics and group classifications (tsurite vs hikite) are summarized in Table 1. There were no significant differences in baseline characteristics between the groups.
Patient Characteristics

Pathology
Injuries of the shoulder are summarized in Table 2. There were no statistically significant differences in radiographic or intraoperative findings between tsurite- and hikite-side shoulders. All shoulders exhibited a Bankart lesion with or without bony fragments, and all concomitant lesions were repaired.
Pathological Findings by Side a
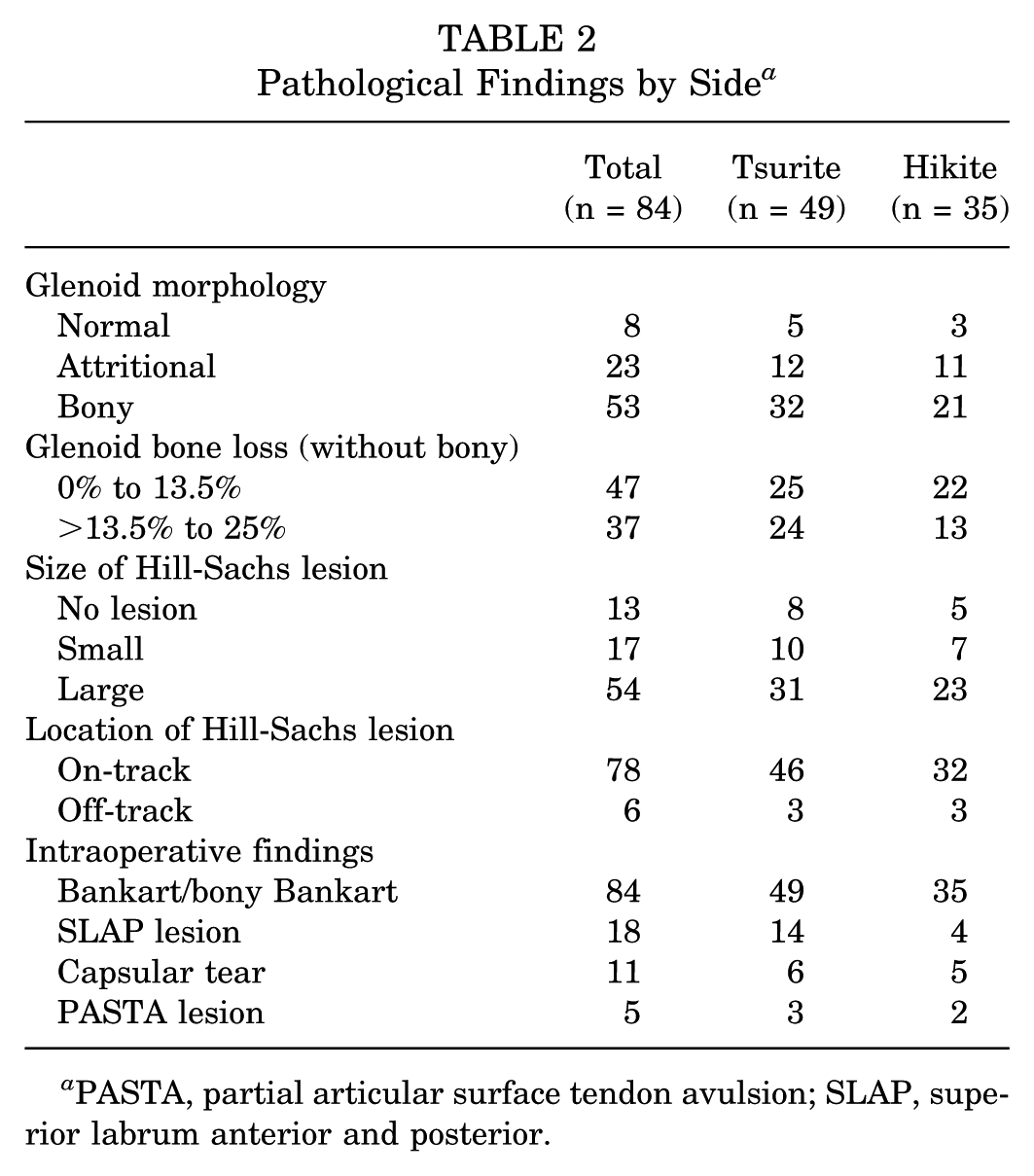
PASTA, partial articular surface tendon avulsion; SLAP, superior labrum anterior and posterior.
Surgical Procedures
ABR or arthroscopic bony Bankart repair (ABBR) was performed in all cases. RIC was performed in 48 (98%) tsurite-side and 29 (83%) hikite-side shoulders. HSR was performed in 6 (12%) tsurite-side and 13 (37%) hikite-side shoulders. Although HSR tended to be performed more frequently in hikite-side shoulders, no significant differences were noted (P = .08).
SLAP lesions were observed in 18 shoulders (14 tsurite side, 4 hikite side); 15 were classified as type 5, 2 as type 4, and 1 as type 3. Nine shoulders underwent anterior-only repair, and 9 underwent both anterior and posterior repair.
Recurrence/Complications
Four (4.8%) shoulders experienced recurrence, all of which were tsurite-side shoulders of teenage or young adult athletes who did not undergo HSR. No complications were observed other than the postoperative infection associated with recurrence in case 3.
Case 1
A 15-year-old female regional-level athlete, who had undergone ABR with RIC and capsular repair at the initial surgery, returned to judo despite incomplete recovery of external rotation and experienced recurrence 11 months postoperatively. At the time of recurrence, her external rotation at the side was limited (30° vs 60° on the contralateral side). She was managed nonoperatively and subsequently transitioned to a different sport.
Case 2
A 17-year-old male regional-level athlete, who had undergone ABBR with RIC and anterior-only repair for the SLAP lesion at the initial surgery, discontinued postoperative rehabilitation and returned to judo without medical clearance. He experienced recurrence 8 months postoperatively. Despite full ROM at the time of recurrence, his noncompliance with rehabilitation was considered a contributing factor. He was managed nonoperatively and subsequently transitioned to a different sport.
Case 3
A 19-year-old male national-level athlete, who had undergone ABBR with RIC at the initial surgery, developed a postoperative infection requiring arthroscopic debridement. He experienced recurrence at 24 months postoperatively. At the time of recurrence, internal rotation was moderately reduced (L2 vs T11 on the contralateral side). He was managed nonoperatively and returned to competition at a lower level.
Case 4
A 19-year-old male elite-level athlete, who had undergone ABR with RIC at the initial surgery, experienced recurrence 60 months postoperatively after winning a gold medal at the world championships. He subsequently underwent revision ABR with RIC and successfully returned to the same competitive level, earning a bronze medal at the next world championship.
Return to Sport
All patients returned to judo competitions. Among 74 patients without recurrence, 69 (93%) patients returned to the same or superior level compared with the preinjury level (Table 3). No significant difference was observed in the return levels between the tsurite- and hikite-side shoulders. The mean time to return was 7 months (range, 3-12 months), without a significant difference in arm dominance (tsurite or hikite).
Return to Sport and Clinical Outcomes a

SSV-sports, Subjective Shoulder Value for sports.
Excluded recurrence cases and included bilateral cases.
Clinical Outcomes
Among tsurite-side shoulders without recurrence, the mean Rowe score significantly improved after surgery from 24 (range, 5-50) to 96 (range, 75-100) (P < .001) (Table 3). The Rowe score also improved significantly from 27 (range, 5-75) to 95 (range, 85-100) in hikite-side shoulders (P < .001). No significant differences were observed in both pre- and postoperative scores between tsurite- and hikite-side shoulders.
Postoperative Range of Motion a

Values are given as mean (range) unless otherwise indicated. ER-abd, external rotation at 90° of abduction; ER-side, external rotation at side; IR, internal rotation.
The mean SSV-sports score significantly improved after surgery from 26 (range, 0-65) to 92 (range, 70-100) in tsurite-side shoulders (P < .001) and from 30 (range, 0-65) to 92 (range, 80-100) in hikite-side shoulders (P < .001) (Table 3). No significant differences were found in both pre- and postoperative scores between the sides.
ROM data >7 months postoperatively were available in 52 patients (28 tsurite-side and 24 hikite-side shoulders) (Table 4). The follow-up periods were as follows: tsurite side, 28 months (range, 7-120 months) and hikite side, 24 months (range, 7-78 months).
Discussion
ABR with selective augmentations for judo athletes yielded good clinical outcomes with 100% RTS. No significant differences were observed in the Rowe score, SSV-sports score, and ROM, except for in external rotation at the side, between the tsurite- and hikite-side shoulders. The recurrence rate was 4.8%, and all recurrences occurred in tsurite-side shoulders of teenage patients.
Several articles have reported outcomes of open surgery for traumatic anterior shoulder instability in judo athletes. Yoneda et al 28 and Rhee et al 19 have reported a 100% RTS rate without recurrence after open Bankart repairs. However, both studies only included a small number of participants and did not report the RTS levels. Uchiyama et al 26 assessed 50 judo athletes who underwent the open inferior capsular shift procedure and reported that 96% of the athletes returned to judo with a recurrence rate of 5.8%. They also reported that the rate of return to the preinjury activity level was only 62%. This study showed a similar RTS, slightly better recurrence rates, and a superior complete return rate (93%) to the study by Uchiyama et al.
In the study by Uchiyama et al, 26 it was concluded that restriction of external rotation after surgery should be minimal in tsurite-side shoulders for return to the preinjury activity level. We have treated the different indications of augmentations for each shoulder to preserve external rotation in tsurite-side shoulders. Our approach of tailoring augmentations to preserve external rotation in tsurite-side shoulders may have contributed to the better complete return rate in these shoulders.
The recurrence rate after ABR for judo athletes has been reported to be 17% to 33%.13,18,19 The recurrence rate in this study was far better than those rates. Our ABR procedures, including inferior glenohumeral ligament retensioning with extensive labral release, fixation of the labroligamentus complex with at least 4 suture anchors, and bony Bankart repair incorporating the bony fragment, might have contributed to the better recurrence rate.4,15,24
The augmentations, RIC and HSR, may also have an important role in reducing recurrences. 12 Shaha et al 21 reported that a subcritical bone loss ≥13.5% led to poor outcomes after isolated arthroscopic labral repairs. We have been positively performing the augmentations for shoulders with ≥13.5% glenoid bone loss with large Hill-Sachs lesions, even in tsurite-side shoulders.
We performed RIC on most shoulders. RIC is considered to accelerate proprioception of the glenohumeral joint by reducing joint volume.6,7,14 However, it is generally believed that adding RIC to Bankart repair may increase the risk of postoperative loss of external rotation. Notably, in our cohort, external rotation was not significantly restricted in tsurite-side shoulders, most of which underwent Bankart repair with RIC alone. These findings suggest that, when carefully performed, RIC can be safely applied to tsurite-side shoulders of judo athletes without causing substantial restriction in external rotation.
HSR is known as a strong soft tissue augmentation. 8 Approximately one-third of hikite-side shoulders received HSR, and no shoulders experienced recurrence. However, the risk of motion loss is also a concern. 5 In our cohort, hikite-side shoulders showed no significant loss of external rotation at 90° of abduction, although a small but statistically significant loss was observed at the side. These findings suggest that HSR may also be appropriate for tsurite-side shoulders, especially in cases in which maintaining external rotation in the abducted position is more critical than at the side.
Four patients experienced recurrence after surgery. All the shoulders were on the tsurite side of teenage patients at the time of surgery, and no shoulders received HSR. Torrance et al 25 reported that ABR for contact athletes aged <16 years had a 2.2-fold risk of recurrence. HSR was not performed in the 4 shoulders to avoid a loss of external rotation because of tsurite-side involvement. HSR should be considered even for tsurite-side shoulders of teenagers regardless of the size of Hill-Sachs lesions and glenoid bone loss.
As mentioned previously, the Latarjet procedure has demonstrated excellent outcomes in managing anterior shoulder instability, especially in high-risk contact athletes. Baverel et al 2 reported that competitive athletes had significantly better outcomes and fewer recurrences than recreational athletes when treated with the open Latarjet procedure. However, as a nonanatomic bone-block technique, it carries potential complications, including restriction of external rotation, neurological injury, graft nonunion or osteolysis, and progressive glenohumeral osteoarthritis. 2 For judo athletes, particularly those with demands on the tsurite-side shoulder, where overhead external rotation is essential, these risks warrant special consideration. In this study, we avoided the use of the Latarjet procedure and instead applied arthroscopic soft tissue stabilization tailored to the functional demands of each shoulder. Despite excluding the Latarjet procedure, our algorithm achieved a low recurrence rate and a high rate of complete RTS, supporting the effectiveness of our algorithm in this population.
Limitations
This study had some limitations. It was a retrospective case series with a medium-term follow-up period, and the outcomes might differ with longer follow-up. A minimum follow-up of 5 years may have been more appropriate, particularly for this high-demand athlete population. Furthermore, although the Bankart procedure is known to produce excellent short-term outcomes, recurrence rates may increase over time. Therefore, the relatively low recurrence rate observed in this study should be interpreted with caution in the context of the medium-term follow-up period. Although postoperative ROM data were available for 62% of patients, assessments were conducted by the operating surgeon, which could have potentially introduced some measurement bias. While the follow-up rate for ROM evaluation is not ideal, the overall follow-up rate for the cohort was 76%, and recurrence and RTS outcomes were assessed in all included shoulders. Therefore, despite this limitation, the clinical findings, particularly the low recurrence rate and high RTS rate, remain robust and support the validity of the study's conclusions.
Conclusion
Arthroscopic soft tissue shoulder stabilization with selective augmentation for traumatic anterior shoulder instability in competitive judo athletes yielded favorable outcomes in both tsurite- and hikite-side shoulders, with a low recurrence rate and a high rate of RTS. Selective augmentations, including RIC and HSR, may be considered to reduce the risk of recurrence, even in tsurite-side shoulders, particularly in younger athletes.
Footnotes
Acknowledgements
The authors gratefully acknowledge the assistance of Daisuke Kajiwara, MD, for providing guidance with the judo grip photographs.
Final revision submitted August 11, 2025; accepted September 8, 2025.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Funabashi Orthopaedic Hospital (proposal IRB/ERC No. 2017014).