
Abstract
Background:
Increased posterior tibial slope (PTS) is a known risk factor for anterior cruciate ligament (ACL) injury and incidence of concomitant meniscal tears. However, the effect of PTS on the severity of concomitant meniscal injury has not been investigated.
Purposes:
To characterize the association between PTS and concomitant meniscal injury severity among patients with ACL injury and identify risk factors for high-severity meniscal tears.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
We retrospectively identified patients who underwent primary ACL reconstruction (ACLR) at a single institution from 2015 to 2021. Patients were excluded if they had a multiligament injury, underwent magnetic resonance imaging (MRI) >12 weeks before surgery, or had >1 year between the injury and surgery. We collected patient demographics, preoperative course, surgical details, and measured medial and lateral PTS. The primary outcome was the presence of a high-severity meniscal tear identified at the time of arthroscopy, defined as a medial or lateral complex, bucket-handle, root, or Zone 3 radial tear. We determined the association between PTS and high-severity meniscal tears using both univariate and logistic regression analyses.
Results:
We included 219 patients—47% women, aged 25.3 ± 10.3 years, with a body mass index (BMI) of 25.6 ± 4.5 kg/m2— in the analysis. A total of 41 patients (18.7%) underwent a medial meniscal procedure, 68 patients (31.1%) underwent a lateral meniscal procedure, 42 patients had both medial and lateral meniscal procedures (19.2%), and 68 patients had no meniscal tear (31.1%). The mean medial PTS was 4.3°± 2.8°, and the mean lateral PTS was 5°± 3.1°. The rate of any high-severity meniscal tear was 11.4% or 11% for a high-severity medial or lateral meniscal tear, respectively. BMI was positively associated with medial or lateral high-severity meniscal tears (odds ratio, 1.12 [95% CI, 1.04-1.21]; P = .003). Neither medial nor lateral PTS was associated with high-severity meniscal tears (all, P > .05).
Conclusion:
Our study shows that neither medial nor lateral PTS was associated with high-severity meniscal tears in patients undergoing ACLR within 1 year of injury, given the available numbers in this study. While BMI was an independent factor associated with meniscal tear severity, delays in surgery did not increase the odds of severe meniscal tear incidence when taking into account PTS. Our study does not support the use of PTS to alter the timing or indications for ACLR out of concern for an increase in the severity of encountered meniscal tears.
Anterior cruciate ligament (ACL) injury alters the stability and biomechanics of the knee. 34 The medial meniscus acts as a secondary restraint to anterior translation, while ACL deficiency places increased force on the menisci, as demonstrated by multiple biomechanical studies.1,26,32 Unsurprisingly, the prevalence of meniscal tears increases with the duration of ACL deficiency, and the rate of meniscal procedures decreases with the restoration of stability after ACL reconstruction (ACLR).11,19,22,28 Nearly two-thirds of patients undergoing ACLR have been reported to have a concomitant meniscal injury, with the vast majority undergoing treatment. 13
The timing of ACLR is crucial because medial meniscal tears are more common with delays and are believed to result from increased forces on the menisci.3,8,14,21,25,33 The severity of a meniscal tear can guide what treatment is needed; this is determined by multiple factors—including tear location, size, type, and stability—and can affect the rate of repair failure.6,10,13 Furthermore, concomitant meniscal injury has been linked to the development of arthritis, the need for meniscal treatment predicts worse articular cartilage damage, and more severe meniscal tears may increase the risk and speed of arthritis development.2,12,16,20 Understanding which patient-specific factors influence the severity of concomitant meniscal injury could help to limit additional injury.
Increased posterior tibial slope (PTS) is a known risk factor for ACL injury,29,35 and more recently, it has been associated with meniscal tears, both with and without an associated ACL tear.7,15,18 Specifically, both increased medial and lateral PTS and compartmental asymmetry are associated with more severe meniscal injury patterns and worse repair survivability.7,36 Biomechanical studies have demonstrated increased force on the medial meniscus and ACL with increased PTS, suggesting that PTS may be an independent contributor to meniscal injury and severity that can be amplified by ACL deficiency.24,30 However, the effect of PTS on the severity of meniscal injury has not previously been investigated, nor has its association with the development of severe meniscal pathology with delays to surgery for ACLR.
The purpose of our study was to characterize the association between PTS and concomitant meniscal injury severity in patients with ACL injuries and to identify risk factors for high-severity meniscal tears. Our hypothesis was that high-severity medial or lateral meniscal tears would be associated with higher medial or lateral PTS measured on magnetic resonance imaging (MRI) and that high-severity tears would be associated with delay to surgery.
Methods
After institutional review board approval (No. U21-10-4593), we retrospectively identified patients at a single institution who underwent primary ACLR within 1 year of injury from 2015 to 2021. Patients were excluded for multiligament injury, lack of preoperative MRI within 1 year of surgery, or inadequate MRI by not showing enough proximal tibia for measuring PTS. We chose to exclude patients with injury and MRI obtained >1 year before surgery because of previous studies demonstrating changes in PTS with time after ACL injury in skeletally immature patients. 23 We reviewed the electronic medical record to collect patient characteristics (age, sex, body mass index [BMI]), preoperative course (timing of MRI and surgery), and surgical details (verification of primary ACLR and concomitant procedures). Our primary outcome was the presence of high-severity medial and/or lateral meniscal tears at the time of arthroscopy. High-severity meniscal tears were defined as complex, root, bucket-handle, or Zone 3 radial tears. Our high-severity definition was expanded from that of Driban et al 12 to include bucket-handle tears in their definition of destabilizing tears (Figure 1). Lawrence et al 21 similarly grouped bucket-handle tears into their definition of severe meniscal tears.

MRI of high-severity meniscal tears (arrowheads). (A) T1-weighted coronal view of a flipped bucket-handle medial meniscal tear. (B) T1-weighted sagittal view of a flipped bucket-handle medial meniscal tear with double-PCL sign. (C) T2 fat-suppressed coronal view of a lateral meniscus root tear. (D) T2 fat-sat coronal view of a lateral meniscal radial tear in Zone 3. (E) T2 fat-suppressed sagittal view of a complex lateral meniscus posterior horn tear. MRI, magnetic resonance imaging; PCL, posterior cruciate ligament.
Imaging Analysis
The timing of MRI related to injury/surgery was collected. If multiple MRIs were available, the first MRI after the time of injury was utilized. Two raters (S.F. and R.O.) measured medial and lateral PTS on sagittal MRI using the previously validated methods of Hudek et al 17 (Figure 2). A subset of patients was measured by both raters twice, separated by 6 weeks, for temporal blinding to perform reliability analyses. Raters were blinded to the presence of meniscal injury identified at the time of arthroscopy. The difference between medial and lateral PTS was also calculated for each patient.

(A) The longitudinal axis of the tibia was drawn on MRI in the method validated by Hudek et al 17 to quantify (B) medial and (C) lateral PTS. MRI, magnetic resonance imaging; PTS, posterior tibial slope.
Intraoperative Assessment
Meniscal pathology and procedures were determined from operative reports dictated by the treating surgeon, all of whom were fellowship-trained sports medicine orthopaedic surgeons. Meniscus pathology was classified by the location (anterior horn, body, posterior horn, or root), zone (1, 2, 3), and type of tear in accordance with the International Society of Arthroscopy, Knee Surgery, and Orthopaedic Sports Medicine Knee Committee classification of meniscal tears.4,31 Medial/lateral meniscal procedures were classified as repair, partial meniscectomy, or rasping. When zone information was undocumented, radial and root tears were assumed to be Zone 3 if meniscal repair was performed and thus grouped into high-severity tears.
Statistical Analysis
Patient, injury, and surgical characteristics were reported as means and standard deviations for continuous variables and as frequencies and percentages for categorical variables. Continuous variables were compared between meniscus severity groups using Student t tests, and categorical variables with chi-square tests. Binary logistic regression was performed to evaluate the strength of association between medial and lateral PTS and high-severity meniscal tears in the medial or lateral compartments, the medial compartment alone, and the lateral compartment alone. Regression analysis also accounted for age, sex, BMI, and time from injury to surgery. Intra- and interrater reliability for measuring medial and lateral PTS via MRI were assessed using intraclass correlation coefficients (ICC). For intrarater reliability, ICC3,2 were used because the same 2 raters performed measurements twice on a subset of patients. For interrater reliability, ICC3 models were used because the means of the individual raters’ 2 measurements on a subset of patients were compared. We classified ICC <0.5 as poor reliability, values between 0.5 and 0.75 as moderate reliability, values between 0.75 and 0.9 as good reliability, and values >0.90 as excellent reliability. Subgroup analysis was performed to compare patients undergoing surgery >12 weeks after injury with those undergoing surgery <12 weeks after injury. A priori statistical significance was set at P < .05.
Results
We identified 408 patients who underwent primary ACLR during the study timeframe. After applying the exclusion criteria (multiligament injury, n = 6; lack of preoperative MRI within 1 year of surgery, n = 164; inadequate MRI for measuring PTS, n = 19), 219 patients were included in the analysis. There were 103 women (47%), and the overall cohort had a mean age of 25.3 ± 10.3 years and a BMI of 25.6 ± 4.5 kg/m2.
Of the overall cohort of 219 patients included in this analysis, 179 (81.7%) underwent ACLR in <12 weeks from injury, and 40 (18.3%) had their reconstruction from 12 weeks to 1 year after injury. All meniscal tears underwent some form of meniscal procedure, and the analysis of tears is presented in conjunction with the meniscal procedures. A total of 41 patients (18.7%) underwent a medial meniscal procedure, 68 patients (31.1%) underwent a lateral meniscal procedure, 42 patients had both medial and lateral meniscal procedures (19.2%), and 68 patients had no meniscal tear (31.1%). The mean medial PTS was 4.3°± 2.8°, and the mean lateral PTS was 5°± 3.1°. The mean difference between medial/lateral PTS in patients with a meniscal tear was 0.7°± 2.6°. Only 3 patients had a medial PTS >10°, and 12 patients had a lateral PTS >10°. Descriptive statistics for the meniscal tear type/location/zone are found in Table 1, along with their association with medial and lateral tibial slope. Specifically, lateral meniscus root tears had no association with medial or lateral PTS.
Descriptive Statistics for Meniscal Tears and Their Association With PTS a

Bold P values indicate statistical significance (P < .05). OR for meniscal tear zones 2 and 3 are compared with zone 1 tears. PTS, posterior tibial slope; OR, odds ratio.
The rates of any high-severity meniscal tear were 21% (n = 46), 11.4% (n = 25), or 11% (n = 24) for high-severity medial or lateral meniscal tears, respectively. On univariate analysis, BMI was the only significant factor associated with a high-severity tear. Between-group comparisons of those with and without high-severity meniscal tears are presented in Table 2. When looking individually at high-severity medial or lateral meniscal tears, respectively, BMI was significantly higher in those with severe medial meniscal tears (28.5 vs 25.2 kg/m2; P < .001), but not severe lateral meniscal tears (26.3 vs 25.5 kg/m2; P = .422). There was no association between BMI and medial posterior horn or root tears on logistic regression (odds ratio [OR], 1; P = .638; OR, 1; P = .966, respectively) or lateral posterior horn or root tears (OR, 1; P = .667; OR, 1.1; P = .345, respectively).
Descriptive Statistics for Patients With and Without High-Severity Medial or Lateral Meniscal Tears a

Data are presented as mean ± SD or %. The bold P value indicates statistical significance (P < .05). BMI, body mass index; PTS, posterior tibial slope.
Factors associated with high-severity tears, as determined by logistic regression, are shown in Table 3. Those factors associated with meniscal procedures are shown in Table 4. Neither medial nor lateral PTS was associated with high-severity meniscal tears or meniscal procedures (all, P > .05). Reliability analysis is reported in Table 5.
Associations With High-Severity Meniscal Tears on Binary Logistic Regression Analysis a
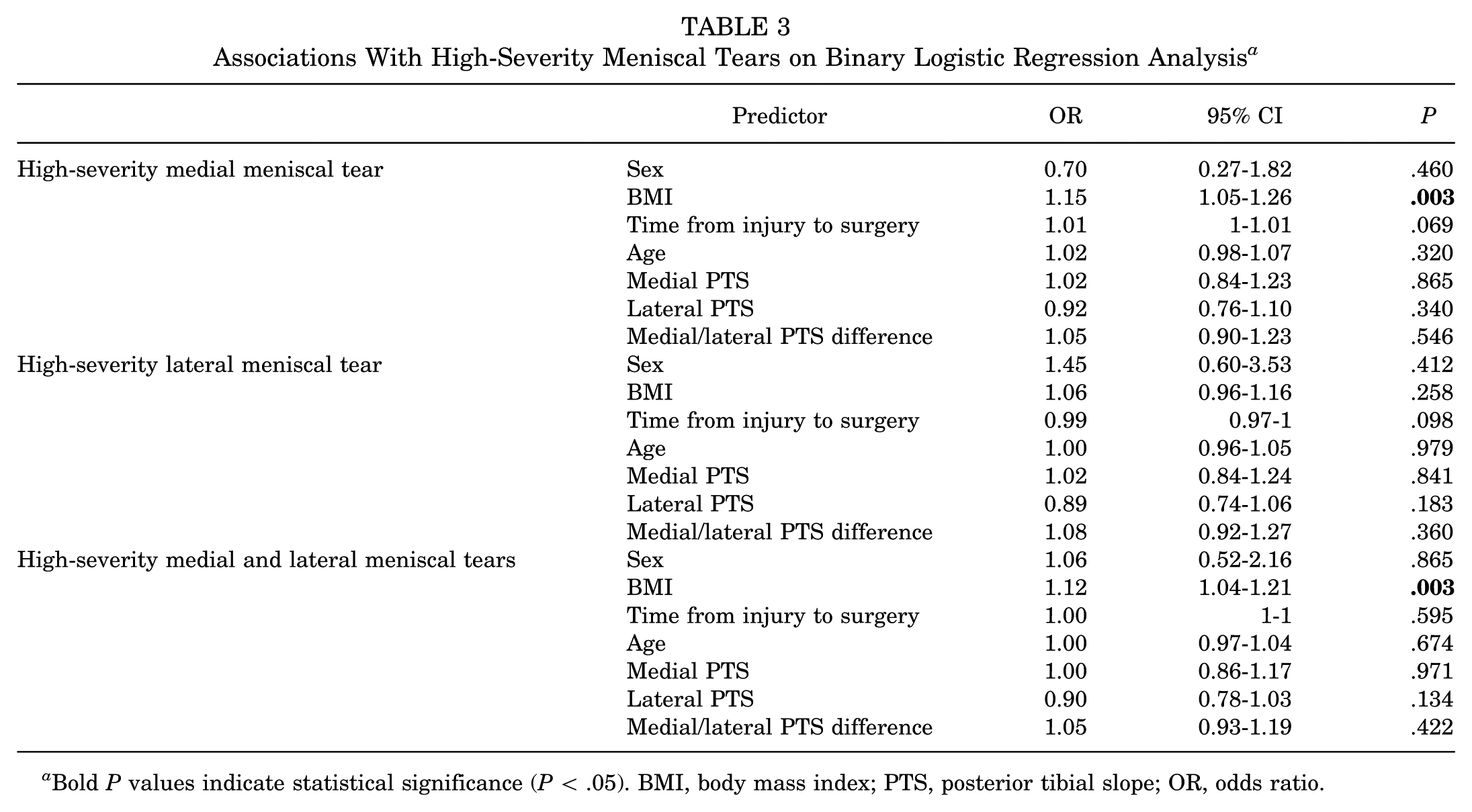
Bold P values indicate statistical significance (P < .05). BMI, body mass index; PTS, posterior tibial slope; OR, odds ratio.
Associations with Meniscal Procedures on Binary Logistic Regression Analysis a

Bold P values indicate statistical significance (P <.05). BMI, body mass index; PTS, posterior tibial slope; OR, odds ratio.
Reliability Analysis a

ICC, intraclass correlation coefficient; PTS, posterior tibial slope.
Discussion
The principal finding of this study was that in patients undergoing ACLR, neither medial nor lateral PTS was associated with high-severity meniscal tears (all P > .05). High-severity meniscal tears were more commonly medial than lateral and were associated with higher BMI (OR, 1.15 [95% CI 1.05-1.26]; P = .003). Additionally, delays in surgical intervention for ACL injury were associated with an increased rate of medial meniscal procedures in keeping with previous studies (OR, 1.01 [95% CI 1-1.01]; P = .013), but not for the severity of the tear (OR, 1.01 [95% CI, 1-1.01]; P = .069).
While grouping severe types of meniscal tears for comparison with controls has not been evaluated before for PTS, several studies have found an association between increased PTS and meniscal tears in general, for certain types of meniscal tears, or outcomes after meniscal repair. 36 In a systematic review, Jiang et al 18 found that in patients with concomitant ACL and meniscal injuries, lateral PTS was associated with any lateral meniscal and lateral meniscus root tears, which would have been considered severe tears by our definition. Bernholt et al 7 evaluated 206 patients in a matched cohort analysis of ACLR with and without lateral meniscus posterior root tears, and also found that steeper lateral PTS, medial PTS, and greater asymmetry between medial and lateral PTS were all statistically associated with lateral meniscus posterior root tears. Our findings differed in that we found no significant association between PTS and meniscal tear severity, nor for lateral meniscus or lateral meniscal root tears, specifically. This remained true in the present study for medial PTS, lateral PTS, and PTS differences.
We also found that increased BMI was associated with higher rates of severe medial meniscal tears. This may be unsurprising, as the medial meniscus plays an important role as a secondary stabilizer to anterior translation and as a primary stabilizer in an ACL-deficient knee. However, the effect of BMI on adding stress to the posterior root and horn may be as evident as purported, as there was no association between BMI and medial or lateral posterior horn or root tears in the present study. Despite this, in a systematic review of studies analyzing BMI in ACL injury, it was identified that patients with an elevated BMI had 1.6 times greater odds of undergoing meniscectomy. 5 In the present study, we identified 1.09 times greater odds of undergoing a lateral meniscal procedure or concomitant medial and lateral procedures. BMI was the only significant factor associated with high-severity tears on univariate analysis, which persisted for high-severity medial meniscal tears at a slightly higher odds of 1.15. These findings suggest that overweight individuals transfer increased forces through the knee, particularly through the meniscus, during and after an ACL injury. However, our findings indicate that this may not occur preferentially in the posterior horn and root. Knowledge of this and other factors associated with high-severity meniscal tears may help in counseling this subset of patients on weight loss as well as considering surgery earlier, if indicated, to avoid additional meniscal injury.
Finally, we identified a small but positive association between the number of days from injury to surgery and the rate of medial meniscal procedures. Previous evidence on the time to surgery and the severity of meniscal tears is limited. In the present study, regarding meniscal tear severity, the time to surgery trended toward statistical significance, but with a clinically irrelevant change in odds when accounting for PTS and other factors. Lawrence et al 21 evaluated the timing of surgery for adolescent ACLR and its association with meniscal injury and severity. They categorized meniscal tear severity based on the repairability and presence of a bucket-handle tear. They found a relatively higher rate of irreparable and larger tears in those treated after 12 weeks. They did not, however, take into account BMI or PTS.
In a systematic review and meta-analysis on ACLR timing, Prodromidis et al27,28 found that ACLR timing significantly affected the risk of meniscal tear and chondral injury. At more than 3 months after injury, there was a higher rate of medial meniscal tears, but not lateral meniscal tears. 28 Similar delays in timing beyond 3 months were associated with a higher rate of chondral injury, and the rate and severity of these injuries worsened with time out to beyond 1 year. Similar findings have been reported in other large cohorts, with higher patient-reported outcomes associated with both the rate and severity of medial chondral injury. 9 Together, these studies support that delays in surgery beyond 3 months increase the rate of medial meniscal tears and associated chondral injury. Although our findings suggest that the effect of delay on surgery on the severity of the meniscal tear is limited, they do corroborate previous findings on the association between delay in surgery and increased rates of medial meniscal procedures.
Limitations
This study is not without limitations. First, our study may not have been powered to demonstrate a difference in PTS between those with and without high-severity meniscal tears, as only 46 patients had a high-severity meniscal tear. Additionally, the small number of patients with a PTS >10° may have contributed to the lack of difference, considering that a PTS of 12° is often considered clinically significant in ACL injuries. The reliability of imaging-based measurements to determine ACL injury risk associated with PTS has been questioned previously. In a systematic review of case-control studies comparing ACL-injured and ACL-intact patients, PTS was identified by the included studies as a reliable measurement. However, the PTS means reported for controls varied considerably between included studies. 37 Our study further demonstrated the reliability of PTS measurements and may help to delineate normative values in future meta-analyses. Therefore, further investigation is needed before PTS can be utilized in a clinically meaningful manner for meniscal injury.
Another limitation of this study was related to its retrospective design. Associations identified, therefore, do not imply causality. Meniscal tear characteristics and procedures were described and coded by multiple treating surgeons at our institution, and there may be variability in their classifications that could have impacted our numbers of high-severity tears. We also did not collect clinical outcomes associated with high-severity tears to determine a difference after this injury pattern. Therefore, our results are limited to the characterization of the factors related to the prevalence of high-severity tears. We chose to exclude patients with an MRI obtained >1 year before surgery because previous studies have demonstrated changes in PTS over time after ACL injury. 23 This limited our ability to conclude the effect of PTS on high-severity tears in patients undergoing operative intervention beyond 1 year from the time of injury. Additionally, we cannot rule out the possibility that patients had asymptomatic meniscal tears before their MRI or ACL tear, which could have influenced the study's findings. Certain insurers may have been more readily able to obtain MRIs at our institution, allowing for retrospective review, which could have introduced a selection bias. Finally, our findings may not be externally valid for high-severity meniscal tears in the absence of ACL injury.
Conclusion
Our study shows that neither medial nor lateral PTS was associated with high-severity meniscal tears in patients undergoing ACLR within 1 year of injury, given the numbers available in this study. While BMI was an independent factor associated with meniscal tear severity, delays in surgery did not increase the odds of severe meniscal tear incidence when taking into account PTS. Our study does not support the use of PTS to alter the timing or indications for ACR out of concern for an increase in the severity of encountered meniscus tears.
Footnotes
Final revision submitted July 9, 2025; accepted August 15, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.M.F. has received support for education from Supreme Orthopedic Systems LLC. E.S.C. is a consultant for Avanos Medical Inc and has received support for education and research from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from WCG (No. U21-10-4593).