
Abstract
Background:
The meniscus-bone angle (MBA), defined as the angle formed by the lateral meniscus with respect to the lateral tibial slope, has recently been identified as an intrinsic factor associated with primary anterior cruciate ligament (ACL) injuries. However, no studies have investigated the influence of MBA and other intrinsic factors excluding the influence of extrinsic factors, especially the level of sports activity.
Purpose/Hypothesis:
The purpose was to evaluate the intrinsic factors of primary ACL injury while controlling for the effect of sports activity level. It was hypothesized that the MBA would be a significant factor associated with ACL deficiency, irrespective of the sports activity level.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A total of 143 knees in 139 patients with ACL injuries (group A) and matched controls (matched by age, sex, and Tegner Activity Scale score), 143 knees in 143 patients without ACL injuries (group N), were evaluated. Patient height, body weight, body mass index, lateral posterior tibial slope angle (LPTSA), medial posterior tibial slope angle (MPTSA), MBA of the lateral meniscus, and relative posterior inclination angle (RPIA; MBA – LPTSA) were evaluated between the 2 groups.
Results:
The MBA (group A: 22.3°± 4.5°; group N: 29.1°± 3.7°) and RPIA (group A: 15.0°± 6.1°; group N: 24.1°± 4.1°) were significantly (P < .001) smaller in group A, whereas LPTSA (group A: 7.3°± 3.4°; group N: 5.0°± 2.7°) and MPTSA (group A: 7.1°± 3.0°; group N: 5.6°± 2.4°) were significantly (P < .001) larger. Logistic regression analysis with ACL injury as the dependent variable showed significant differences in MBA (OR, 0.645; 95% CI, 0.579-0.718; P < .01) and LPTSA (OR, 1.3; 95% CI, 1.14-1.48; P < .001) between the 2 groups. The receiver operating characteristic curves for the MBA showed a sensitivity of 76.2% and a specificity of 83.9% with the cutoff value of 25.2° (area under the curve, 0.88).
Conclusion:
A low MBA with a cutoff value of 25.2° was the most significant independent factor associated with primary ACL injury when controlling for differences in sports activity level.
Keywords
Anterior cruciate ligament (ACL) injuries occur in 1.5% to 1.7% of healthy athletes. Many such injuries are caused by noncontact or minor contact mechanisms.11,12,38 The incidence of ACL injuries is increasing, and many extrinsic and intrinsic factors for ACL injury have been identified. Extrinsic factors are related to the athlete's environment, such as weather conditions, field conditions, shoe-surface interactions, type of sports, and level of sports. Intrinsic factors consist of the athlete's sex, body weight, hormone levels, knee anatomy, muscle strength, pivoting biomechanics, and neuromuscular control.2,30,31 Among intrinsic factors, the anatomic factors include the posterior tibial slope angle (PTSA), intercondylar notch morphology, femoral condyle morphology, and alignment.14,15,18,19,35 An increased PTSA is widely believed to be associated with a higher risk of ACL injury. Additionally, the lateral meniscus (LM) is a crucial contributor to knee stability, in both anterior tibial subluxation and rotatory stability.10,14,17,20,23,25,39,43 The contribution of the LM posterior root to controlling internal rotation in both ACL-intact and ACL-deficient knees was previously reported. 14 Some biomechanical studies have shown that LM tears increase the rotation and anterior laxity of the tibia, which could be reduced by repairing the torn LM.10,17,25 Furthermore, the importance of the LM compared with the medial meniscus as a secondary stabilizer was also demonstrated. 21
Recently, the meniscus-bone angle (MBA) in the sagittal plane alignment, defined as the angle formed by the meniscus with respect to the tibial slope, has been proposed as a new factor associated with ACL injury.1,16,29 Initially, an index of soft tissue rather than a bony index such as PTSA was suggested by Hudek et al. 16 The slope based on the height difference between the anterior and posterior segments of the meniscus was termed the meniscal slope, and there was an association between increased meniscal slope and noncontact ACL injuries. 16 Subsequently, the MBA was defined by Sturnick et al, 29 who reported an association between low MBA and the presence of ACL deficiency in males, followed by some similar studies.1,9,22 Large MBA is thought to be effective for deceleration of the femur in pivoting maneuvers, and the LM with large MBA may impede tibiofemoral subluxation and ACL injury.
PTSA is also reported to be involved in the tibiofemoral subluxation; the larger the PTSA, the greater the anterior tibial subluxation. 42 Therefore, both MBA and PTSA may be considered to contribute to the tibiofemoral subluxation, and the relative angle incorporating these parameters (described as relative posterior inclination angle [RPIA]) may be more important for understanding the tibiofemoral subluxation (Figure 1).
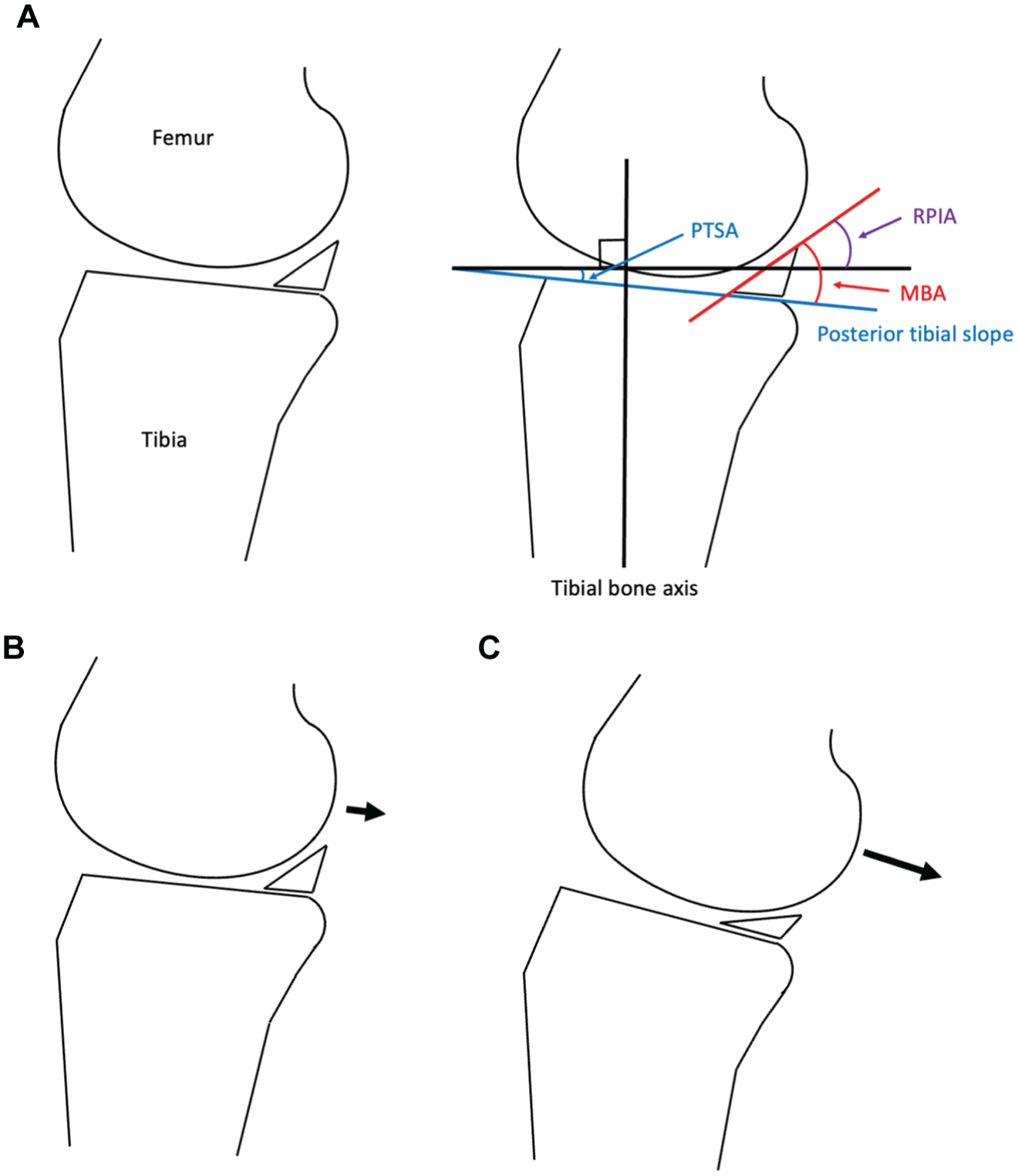
(A) Schema of meniscus-bone angle (MBA), posterior tibial slope angle (PTSA), and relative posterior inclination angle (RPIA). The knee with (B) large MBA and small PTSA and (C) small MBA and large PTSA. Large MBA and small PTSA may contribute to the deceleration of the femur moving posterior (B). In contrast, small MBA and large PTSA may accelerate the femur moving posteriorly, leading to the tibiofemoral subluxation and anterior cruciate ligament injury (C).
There are few studies that have investigated the relationship between MBA and ACL injuries, and no study has investigated the relative angle combining the MBA and PTSA. Furthermore, these studies were conducted without any consideration of extrinsic factors such as sports activity level. Among extrinsic factors, sports activity itself is considered to be a significant confounding factor of ACL injuries, so matching the level of sports activity is important while investigating the intrinsic factors of ACL injuries.
Therefore, the aim of the present study was to retrospectively investigate the influence of intrinsic factors, including MBA and RPIA, on primary ACL injury, excluding the effect of extrinsic factors such as sports activity level by matching with the Tegner Activity Scale (TAS) score. We hypothesized that intrinsic factors, especially MBA and RPIA, would be significantly associated with ACL deficiency even after matching TAS score between the groups of ACL-injured and noninjured knees.
Methods
This study was approved by the Institutional Review Board of the Clinical Research Support Center of our hospital. All the study procedures were conducted in accordance with the relevant guidelines and principles of the Declaration of Helsinki. All participants provided informed consent for study participation, including consent for publication, and were free to withdraw from the study at any time.
The medical records of 2044 patients (2083 knees) who visited our hospital with knee joint symptoms and underwent knee magnetic resonance imaging (MRI) between January 2018 and December 2023 were retrospectively evaluated. Of these, 237 patients (241 knees) with ACL injuries were treated surgically at our hospital. Exclusion criteria included patients with LM injuries accompanied by acquired morphological changes caused by the injury or congenital morphological changes such as discoid meniscus, patients with a history of ipsilateral ACL injury who had undergone ACL reconstruction, and those with osteoarthritic changes. According to these criteria, 163 patients (167 knees) with ACL injuries were finally included in the analysis. Application of propensity score matching at a 1:1 ratio yielded 143 knees in the ACL injury group (group A) and 143 knees in the control group (group N). Matching was performed using a logit scale with a caliper width of 0.2. The matched variables included age, sex, and TAS score before injury (Figure 2). Basic patient data including age, sex, height, body weight, body mass index (BMI), TAS score, and the concomitance of medial meniscus injury accompanied by morphological changes caused by the injury or medial collateral ligament (MCL) injury were assessed. The lateral PTSA (LPTSA), medial PTSA (MPTSA), MBA of the LM, and RPIA (MBA – LPTSA) were evaluated.

Flowchart of the study population. From an initial cohort of 2044 patients who underwent knee magnetic resonance imaging (MRI), 163 patients with anterior cruciate ligament (ACL) injury met the inclusion criteria. After propensity score matching at a 1:1 ratio by age, sex, and Tegner Activity Scale (TAS) score, the study included 139 patients (143 knees) with ACL injury (group A) and 143 patients (143 knees) without ACL injury (group N). LM, lateral meniscus.
LPTSA, MPTSA, and MBA were measured from MRI scans as described previously. 22 Specifically, on a sagittal plane slice through the center of the tibia, 2 circles were drawn touching the articular surface and the anterior and posterior cortices, and the line passing through the center of each circle was set as the tibial bone axis. This line was copied and drawn on the central lateral and medial slice (copied tibial axis). The angles formed between the line perpendicular to the copied tibial axis and the tibial plateau surface (subchondral bone) line were defined as the LPTSA and MPTSA, respectively. The angle formed between the lateral tibial plateau surface line and the LM superior surface line on the same slice was defined as the MBA of the LM. RPIA was calculated by subtraction of these 2 angles (MBA – LPTSA) (Figure 3).

Magnetic resonance imaging measurements of the lateral posterior tibial slope angle (LPTSA), medial posterior tibial slope angle (MPTSA), meniscus-bone angle (MBA), and relative posterior inclination angle (RPIA). (A) On a sagittal plane slicing through the center of the tibia, 2 circles were drawn touching the articular surface and the anterior and posterior cortices. The lines passing through the center of each circle were defined as the tibial bone axis. This line was copied and drawn on the central lateral and medial slice (copied tibial axis). The angles formed between the perpendicular line to this copied tibial axis and the tibial plateau surface (subchondral bone) line were defined as the (B) LPTSA and (C) MPTSA. (D and F) The angle formed between the lateral tibial plateau surface line and the lateral meniscus (LM) superior surface line on the same slice was defined as the MBA. (E and G) The angle formed by the subtraction of MBA and LPTSA was described as RPIA.
To determine the intra- and interobserver reliabilities of LPTSA, MPTSA, and MBA measurement on MRI, these parameters were measured on 30 randomly selected MRI scans by 2 orthopaedic surgeons (S.K. and S.N.) for interobserver reliability testing. The first observer (S.K.) repeated the measurement of these parameters at a 6-week time interval. The intra- and interobserver reliabilities were evaluated using the intraclass correlation coefficient (ICC). For the intraobserver reliabilities, the ICCs of LPTSA, MPTSA, and MBA were 0.94, 0.92, and 0.96, respectively. For the interobserver reliabilities, the ICCs of LPTSA, MPTSA, and MBA were 0.87, 0.83, and 0.88, respectively. Thus, based on this calculation, the measurement of LPTSA, MPTSA, and MBA on MRI was found to have good to excellent intra- and interobserver reliabilities.
Statistical Analysis
Continuous variables, including age, height, body weight, BMI, TAS score, LPTSA, MPTSA, and MBA, showed normal distributions; therefore, they were analyzed using the t test and are summarized as means. The categorical variables, including sex, the presence of medial meniscus injury accompanied by morphological abnormalities, and MCL injury, were analyzed using the chi-square test. Multivariate logistic regression analysis was used to identify independent factors associated with ACL deficiency. Receiver operating characteristic (ROC) curves were used to detect the optimum cutoff values and identify variables with strong discriminative ability. The Youden index was computed to determine the cutoff value with the highest sensitivity and specificity. The area under the curve (AUC) was used to compare the discriminative capacities of the predictive variables. Statistical analyses were performed using statistical software packages in R language (Version 4.2.1; R Development Core Team). The level of significance was set at a P value <.05.
Results
The detailed characteristics of patients in groups A and N are shown in Table 1. As age, sex, and TAS scores were matched, there were no significant differences between groups for any demographic or surgical variables assessed (all P > .05).
General Characteristics of the Patients in the 2 Groups a

Data are presented as mean ± SD unless otherwise indicated. Continuous and categorical variables were compared using the t test and chi-square test, respectively. Group A consists of patients with ACL injuries, and group N consists of patients without ACL injuries. BMI, body mass index; MCL, medial collateral ligament; MM, medial meniscus; TAS, Tegner Activity Scale.
The MPTSA, LPTSA, MBA, and RPIA measured from the MRI scans are shown in Table 2. MBA (22.3°± 4.5° vs 29.1°± 3.7°; P < .001) and RPIA (15.0°± 6.1° vs 24.1°± 4.1°; P < .001) were significantly smaller, whereas MPTSA (7.1°± 3.0° vs 5.6°± 2.4°; P < .001) and LPTSA (7.3°± 3.4° vs 5.0°± 2.7°; P < .001) were significantly larger in group A than in group N.
MPTSA, LPTSA, MBA, and RPIA Measured From MRI Scans a
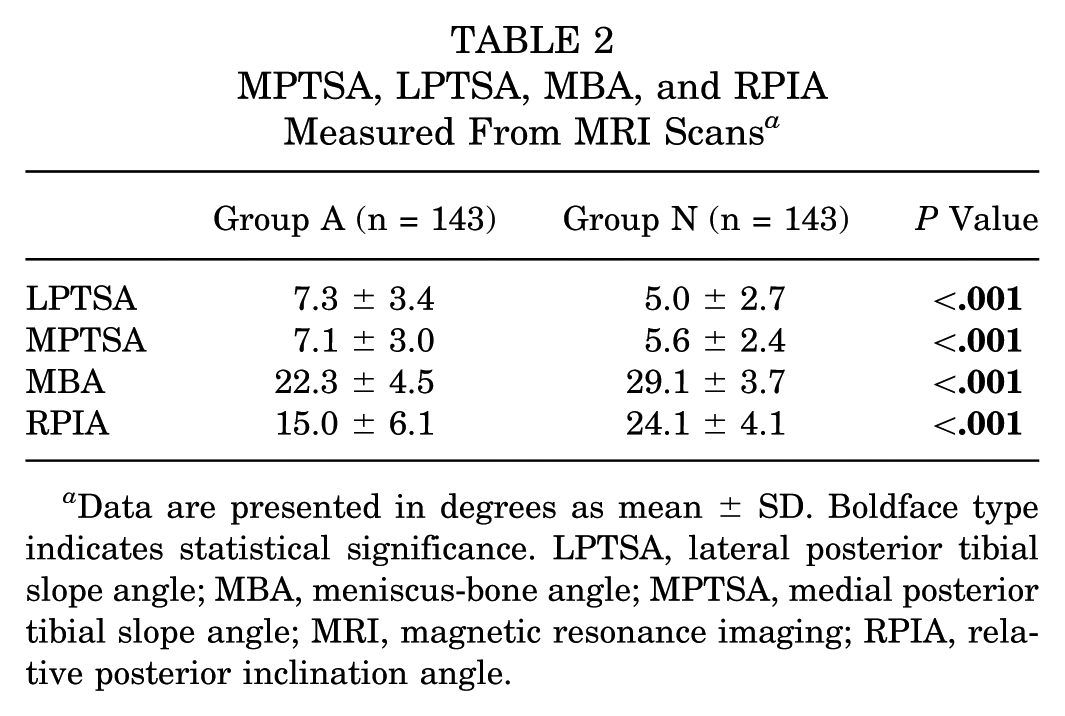
Data are presented in degrees as mean ± SD. Boldface type indicates statistical significance. LPTSA, lateral posterior tibial slope angle; MBA, meniscus-bone angle; MPTSA, medial posterior tibial slope angle; MRI, magnetic resonance imaging; RPIA, relative posterior inclination angle.
Multivariate logistic regression analysis with the presence of ACL injury as the dependent variable and BMI, MPTSA, LPTSA, MBA, and RPIA as the independent variables revealed that MBA (OR, 0.645; 95% CI, 0.579-0.718; P < .001) and LPTSA (OR, 1.3; 95% CI, 1.14-1.48; P < .001) were independent factors associated with ACL deficiency (Table 3). This analysis did not find RPIA to be a significant independent factor associated with ACL deficiency as it was excluded as a confounding factor.
Results of Multivariate Logistic Regression Analysis a

Boldface type indicates statistical significance. BMI, body mass index; LPTSA, lateral posterior tibial slope angle; MBA, meniscus-bone angle; MPTSA, medial posterior tibial slope angle.
Data (LPTSA, MPTSA, and MBA) are presented in degrees as mean ± SD.
The ROC curves for MBA and LPTSA are shown in Figure 4.
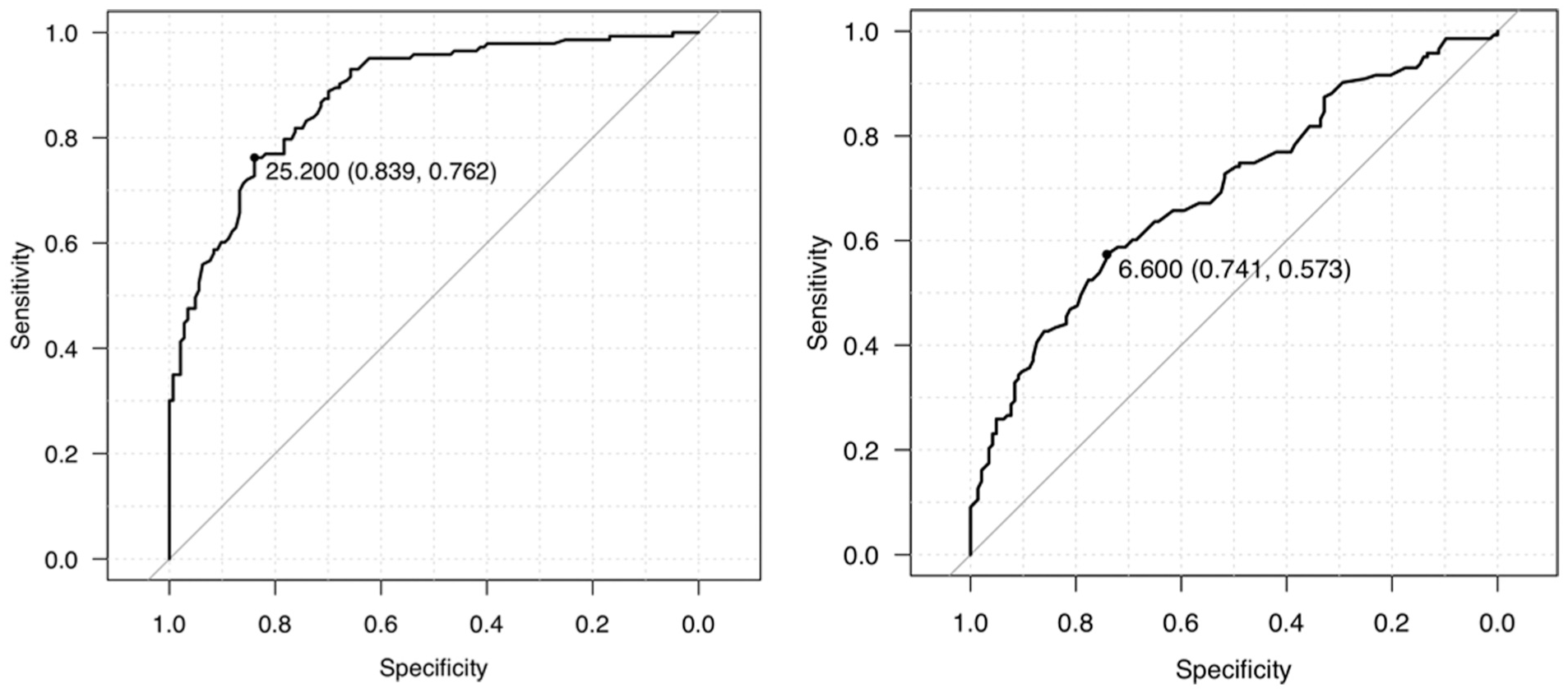
Receiver operating characteristic curves for the meniscus-bone angle (MBA) and lateral posterior tibial slope angle (LPTSA).
The AUC of MBA was higher than that of LPTSA. The optimal cutoff values for MBA and LPTSA were 25.2° and 6.6°, respectively. The corresponding sensitivities and specificities are shown in Table 4.
AUC, 95% CI, Sensitivity, and Specificity of MBA and LPTSA a
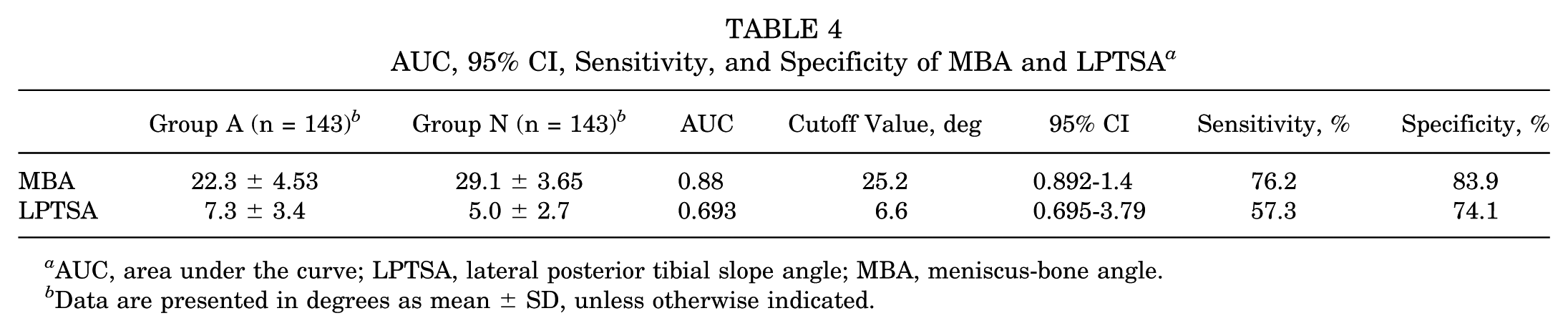
AUC, area under the curve; LPTSA, lateral posterior tibial slope angle; MBA, meniscus-bone angle.
Data are presented in degrees as mean ± SD, unless otherwise indicated.
Discussion
The most important findings of the current study were that low MBA and high LPTSA, MPTSA, and RPIA were independent intrinsic factors associated with ACL deficiency. Among these, low MBA and high LPTSA were significant and independent factors, and cutoff values of 25.2° and 6.6°, respectively, were associated with an increased likelihood of ACL deficiency, with sensitivities of 76.2% and 57.3% and specificities of 83.9% and 74.1%, respectively. Furthermore, MBA was thought to be the most significant independent factor associated with ACL deficiency because the AUC of MBA was higher than that of LPTSA (0.88 and 0.693, respectively). Therefore, our findings partially validated our hypothesis.
The previously reported intrinsic factors associated with ACL injury include sex, BMI, hormone levels, joint laxity, neuromuscular control, and anatomic factors such as intercondylar notch width and anatomic bone morphology.2,19,27,30,31,34,35 Many studies have demonstrated the relationship between ACL injury and tibial slope as an intrinsic factor. # Stijak et al 28 first reported the importance of evaluating MPTSA and LPTSA separately. Their results revealed that there was difference between MPTSA and LPTSA; LPTSA was significantly larger in the ACL-injured group, while MPTSA was significantly larger in the control group. Zeng et al 41 showed higher MPTSA and LPTSA among patients with ACL injury compared with those of the control group and a stronger association between ACL injury and LPTSA than MPTSA. Although these studies evaluated MPTSA and LPTSA separately and suggested the importance of measuring PTSA using MRI, there were no data on the cutoff value of PTSA. De Sousa Filho et al 7 proposed a PTSA cutoff value of ≥8° on plain radiographs, which was associated with a 3-fold increased risk of noncontact ACL injury. Dare et al 6 evaluated MPTSA and LPTSA separately using MRI and suggested an LPTSA cutoff value of >4°, which demonstrated 76% sensitivity and 75% specificity for predicting ACL injury.
Although influence of sex differences on ACL injury has been reported, no unified consensus has yet been reached. Todd et al 33 demonstrated significantly greater PTSA among female patients with ACL injury compared with control groups, whereas no significant difference was observed in males. Similarly, Beynnon et al 3 reported a 21.7% increased risk of noncontact ACL injury with each degree increase of the LPTSA among females but not among males. In contrast, Wang et al 37 showed that a steeper coronal slope of the medial tibial spine was a significant predictor of noncontact ACL injuries in males but not in females. Additionally, DePhillipo et al 8 reported a significantly higher LPTSA in patients with ACL injury regardless of sex. Thus, we evaluated the anatomic intrinsic factors excluding other intrinsic factors by matching sex and age in this study.
The MBA in the sagittal plane alignment has recently been proposed as a new intrinsic anatomic factor associated with ACL injury. Alves et al 1 evaluated MBA, LPTSA, and the LPTSA/MBA ratio and demonstrated that an MBA ≤22° was significantly associated with increased ACL injury. Sauer et al 22 demonstrated that low MBA was an independent factor associated with graft failure after ACL reconstruction, regardless of the surgical technique or graft insertion position. However, they did not show the cutoff value of MBA in their reports, and few studies have shown the cutoff value of MBA for ACL injury. Although these studies have been conducted in adult populations, Edwards et al 9 reported similar results in a pediatric population: the lateral tibial slope (LTS) and LTS/MBA ratio were significant factors associated with ACL injury.
In the present study, MPTSA and LPTSA were significantly larger and MBA and RPIA were significantly smaller in patients with ACL injury. Thus, large MPTSA and LPTSA and low MBA were associated with ACL injury, a finding consistent with those reported previously. Furthermore, RPIA was significantly smaller in the ACL injury group, indicating that low RPIA was associated with ACL injury. However, logistic regression analysis did not find RPIA to be a significant independent factor associated with ACL deficiency as it was excluded as a confounding factor, and the results of the analysis identified MBA and LPTSA as significant independent factors associated with ACL deficiency. Comparing the ROC curves of MBA and LPTSA, the AUC was higher in MBA compared with that of LPTSA. Thus, MBA was more strongly associated with ACL deficiency compared with LPTSA. The cutoff values for MBA and LPTSA in the present study were ≤25.2° and ≥6.6°. Although these cutoff values differed from those reported previously, notably, nearly all previous reports were from Western countries, which raises a question as to whether skeletal differences may influence these values.
To our knowledge, all previous studies on the factors for ACL deficiency, compared with the control group, evaluated intrinsic risk factors without matching of any sports activity level, such as the TAS score. Although intrinsic risk factors other than anatomic factors, such as muscle strength, body weight, and muscle balance, have been compared between the ACL injury and control groups after matching according to TAS score,30,31 no study has compared the anatomic factors between ACL injury and control groups matched by TAS score. This is possibly the first study to evaluate the anatomic factors between ACL injury and control groups with matching TAS scores.
After identifying the independent significant factors associated with ACL injury, special attention may need to be given to educating patients on exercise instructions and post-ACL reconstruction rehabilitation. MPTSA, LPTSA, and MBA may have the possibility of being addressed by correcting the sagittal plane alignment. Based on these factors, future post-ACL surgery rehabilitation may need to be tailored to individual risks rather than providing uniform exercise instruction. Furthermore, obtaining baseline knee MRI data in the athletic population may be useful as these data may be able to suggest and provide the appropriate exercise instruction for the athletic population to avoid primary ACL injury.
Limitations
There are several limitations in this study. First, this was a retrospective study using radiological data. Second, only MBA of the LM was evaluated because MBA of the medial meniscus was not previously mentioned as a risk factor associated with ACL injury. Third, the changes in the tibial position and traumatic slight changes in the LM after injury may have affected the measurement values. Thus, it is necessary to evaluate the correlation between MBA and anterior tibial subluxation in a future study. Measurements of the uninjured side without a history of trauma would have allowed more accurate identification of intrinsic risk factors. A further limitation was the MRI protocol, where the thickness and angle of the slice were not unified, which could have led to a measurement error. Additionally, although MRI has high sensitivity and specificity in diagnosing meniscal tears, misdiagnosis was possible, especially in the control group, as the diagnoses were not confirmed using arthroscopy. Finally, the findings of this study may not be generalizable to other populations because our study was conducted in an Asian cohort.
Conclusion
This study suggested that low MBA and RPIA and high LPTSA and MPTSA were significant factors associated with ACL deficiency. Among these, low MBA and high LPTSA were significant and independent factors associated with the presence of ACL deficiency. The MBA was the most significant intrinsic factor, with high sensitivity and specificity after controlling for activity level.
Footnotes
Final revision submitted July 28, 2025; accepted August 26, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.T. has received grants from Smith & Nephew, Zimmer Biomet, and Stryker; consulting fees from Smith & Nephew and Arthrex; and speaking fees from Smith & Nephew and Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Institutional Review Board of the Clinical Research Support Center of JR Tokyo General Hospital (R06-10).