
Abstract
Background:
It is unclear whether patients who return to preinjury sports levels 2 years after primary anterior cruciate ligament reconstruction (ACLR) have better functional outcomes than those who do not. In particular, the specific factors among functional outcomes that influence the return to preinjury and postoperative sports levels remain controversial.
Purpose:
To compare functional outcomes such as muscle and functional performances and patient-reported outcomes (PROs) between patients who returned to preinjury sports levels 2 years after primary ACLR and those who did not, as well as identify functional outcomes associated with returning to either preinjury or postoperative sports levels at 2 years postoperatively.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
A total of 50 male patients (26 successfully returned vs 24 did not return) were included in this study. The criteria for study participants were general patients with a preoperative Tegner activity level ≥6. Patients who returned to their preinjury sports levels were classified using the Tegner activity level and sports activity rating scale after surgery. At the 2-year follow-up evaluation, functional outcomes such as knee muscle strength, work fatigue, single-leg hop distance (SLHD), limb symmetry index, Lysholm score, International Knee Documentation Committee (IKDC) score, Knee injury and Osteoarthritis Outcome Score (KOOS) Sport and Recreation subscale, and KOOS Quality of Life subscale were compared between the groups. Multiple linear regression analysis was performed to identify associated factors affecting return to preinjury and postoperative sports levels.
Results:
Work fatigue of quadriceps muscles (Cohen d = −0.86; 95% CI, −12.2 to −2.5; P = .004), SLHD (Cohen d = 1.21; 95% CI, 17.8 to 48.8; P < .001), IKDC score (Cohen d = 2.14; 95% CI, 6.4 to 27.2; P < .001), and KOOS Sport and Recreation subscale (Cohen d = 1.05; 95% CI, 6.6 to 22.0; P < .001) were better in patients who returned to preinjury sports levels than those who did not. Work fatigue of quadriceps muscles (R2 = 0.110; β = −0.332) and SLHD (R2 = 0.084; β = 0.290) were associated with preoperative Tegner activity level, whereas work fatigue of quadriceps muscles (R2 = 0.157; β = −0.397), SLHD (R2 = 0.283; β = 0.532), and IKDC score (R2 = 0.452; β = 0.672) were associated with postoperative Tegner activity level.
Conclusion:
The work fatigue, SLHD, IKDC score, and KOOS Sport and Recreation subscale were better in patients who returned to preinjury sports levels than in those who did not. Work fatigue of the quadriceps muscle and SLHD were associated with return to preinjury sports levels, whereas work fatigue of the quadriceps muscle, SLHD, and IKDC score were associated with postoperative sports levels.
Keywords
The anterior cruciate ligament (ACL) is commonly injured during sports activities such as jumping, pivoting, and cutting motions. 23 The ACL plays a significant role in the stability of the knee joint, such as tibial anterior translation and internal rotation; thus, its injury causes pain, instability, and functional deficits. 29 Hence, arthroscopic ACL reconstruction (ACLR) has evolved into the gold-standard treatment for restoring knee stability,10,29 which may improve knee functions such as muscle strength, proprioception, and neuromuscular control, thereby facilitating a return to preinjury sports levels after ACLR.20,31
Despite many advances in surgical techniques for ACLR, recovery to preinjury sports levels is approximately 50% to 60% after ACLR. 12 In several studies on return to sports (RTS) after ACLR, functional outcomes such as muscle strength,20,35 hop performance,5,20,35 and patient-reported outcomes (PROs)5,7,9 were used as the criteria for RTS after ACLR; however, to our knowledge, there are limited available data directly comparing functional outcomes in patients who returned to preinjury sports levels 2 years after primary ACLR with those who did not. Hence, it is unclear whether patients who return to preinjury sports levels 2 years after primary ACLR have better functional outcomes than those who do not. While many patients expect to return to their preinjury sports levels after ACLR, 37 data on objective assessments are lacking. Furthermore, in a recent study, 5 despite a successful return to preinjury sports levels after ACLR, questions have been raised as to whether functional outcomes can predict successful RTS. Therefore, it is important to understand the functional outcomes of patients who successfully returned to their preinjury sports levels and those who did not. By identifying these clinical and functional differences, rehabilitation programs can be more effectively individualized and may include more intensive interventions tailored to each patient’s needs.
The primary aim of this study was to compare functional outcomes such as muscle and functional performances, and PROs between patients who returned to preinjury sports levels 2 years after primary ACLR and those who did not. The secondary aim was to identify functional outcomes associated with returning to either preinjury or postoperative sports levels at 2 years postoperatively. We hypothesized that patients who returned to their preinjury level of sports participation after primary ACLR would demonstrate better functional outcomes compared with those who did not.
Methods
This study retrospectively analyzed prospectively collected data and was approved by our institutional review board (2018AN0261). The study complied with the principles of the Declaration of Helsinki. All surgical procedures were performed by a single surgeon (K.M.J.), and informed consent was obtained from all participants.
Participants
A total of 256 patients underwent primary ACLR using hamstring autograft or allograft between January 2019 and June 2022, and eligibility criteria for study participants were as follows: (1) male patients who underwent all evaluations at the 2-year postoperative follow-up, and (2) patients from the general population who participated in recreational sports activities or more, that is, patients with a preoperative Tegner activity level ≥6, defined as participation in recreational sports activities or strenuous sports.13,41 Therefore, based on participant criteria from a previous study, 13 we included patients with at least a preoperative Tegner activity level ≥6. Based on this, we classified patients who returned to their preinjury sports levels using postoperative Tegner activity levels and sports participation type (sports activity rating scale) 2 years after ACLR and those who did not. The exclusion criteria were as follows: (1) bilateral knee injuries; (2) other concomitant intra- or extra-articular injuries (ie, posterior cruciate, collateral, and ankle ligament injuries; revisional ACLR; and fracture); (3) Kellgren-Lawrence grade >1; (4) neurological pathology; (5) preoperative Tegner activity level <5; and (6) loss to follow-up. Of the 256 patients, 206 were excluded; thus, the final assessment used the data from 50 male patients (26 successfully returned vs 24 nonreturned) (Figure 1), and none of the participants had pain.

Flowchart of patient selection for this study.
Surgical Procedure
All patients were administered general or spinal anesthesia. Standard knee arthroscopic examination was performed using a 4.0-mm arthroscope through the anterolateral and anteromedial portals, and arthroscopic ACLR was performed using hamstring autograft (HA) (n = 29; 58%) and tibialis anterior allograft (n = 21; 42%) according to the patient’s choice, after explaining the risks and benefits of the graft type. The surgical procedure performed in the present study followed the standardized protocol described in a previous study. 24
Rehabilitation Protocol
All participants followed the same rehabilitation protocol, which occurred 1 or 2 times per week for a minimum of 12 weeks and consisted of 4 phases. After 12 weeks, progressive rehabilitation exercises were delivered through exercise education and video recordings during each evaluation period. Phase 1 (≤6 weeks postsurgery) was the recovery period after the surgery and included pain control, range of motion (ROM), and initial muscle strengthening exercises. Phase 2 (from 6 to 12 weeks postoperatively) was the recovery period for general function and included full ROM, gradual muscle strengthening, and balance exercises. Phase 3 (from 13 to 24 weeks postsurgery) was the recovery period of functional performance and included running, plyometric, and agility exercises, in addition to phase 2 exercises. The final phase (24 weeks postoperatively) was the preparation period for returning to sports, including sports-specific technical training. The detailed rehabilitation protocol performed in the present study followed the standardized protocols used in a previous study. 24
In all patients, functional tests were performed at 3, 6, 12, and 18 months and 2 years postoperatively. RTS is recommended after 10 months postoperatively.2,5
Outcome Measures
Muscle Performance Test
Muscle performance, including knee muscle strength and work fatigue, was evaluated using an isokinetic device (Biodex Multi-Joint System 4; Biodex Medical Systems). Before the assessment, each patient rode a stationary bicycle lightly for 3 minutes and performed a set of submaximal 4 to 5 repetitions of flexion and extension at 60 deg/s. All patients performed a maximum set of 5 repetitions of flexion and extension (concentric/concentric action mode at 60 deg/s) in each leg to assess knee muscle strength (peak torque (PT)/body weight; N·m/kg × 100). 25 Work fatigue is the ability to continue exercising or endurance ability 1 and is defined as the ratio of the last one-third of work to the first one-third of work during maximal muscle contraction (reduced by 100%).

Therefore, a high percentage value indicates a decrease in the ability to maintain work output (consistency of muscle performance) over time, which means increased muscle fatigue. 21 In this study, work fatigue was evaluated during a maximum of 15 repetitions at 180 deg/s, and this is automatically calculated by the software system. Extensor and flexor muscles were regarded as quadriceps and hamstring muscle functions, respectively. In this study, the reliability of the isokinetic muscle performance test was measured using the coefficient of variation (CV; in percentage), with CV <15% deemed acceptable. 27 Thus, the CVs for quadriceps and hamstring muscle strength (8.6% and 9.8%, respectively) and work fatigue (12.4% and 13.3%, respectively) were acceptable.
Functional Performance Test
Functional performance was evaluated using the single-leg hop distance (SLHD; in cm) and limb symmetry index (LSI; in percentage). In the SLHD test, participants were instructed to stand on 1 leg at the starting line, jump forward as far as possible, and land on the same leg, with testing conducted after 2 practice attempts. 24 Landing with early touchdown of the contralateral leg or loss of balance was considered a failure. The mean distance between 2 trials was used for the analysis. The LSI was calculated as the mean score for operated limb divided by nonoperated limb × 100. 24 The LSI consisted of the LSI in quadriceps (LSI–quadriceps), hamstring muscle strength (LSI–hamstring), and SLHD (LSI–SLHD).
Patient-Reported Outcomes
The PROs were evaluated for Lysholm score, 3 International Knee Documentation Committee (IKDC) score,9,19,32 and Knee injury and Osteoarthritis Outcome Score (KOOS).7,16,19 The Lysholm and IKDC scores consisted of 8 activities (limping, support, restraining, instability, pain, swelling, climbing stairs, and squatting) and 3 items (symptoms, function, and sports activities), respectively; a low score (points) indicated severe symptoms and poor level of functioning. The KOOS included 5 items (Pain, Symptoms, Activities of Daily Living, Sport and Recreation, and Quality of Life [QoL]), but in the present study, the KOOS Sport and Recreation and QoL subscales were used to evaluate physical functions6,19 and psychological impairments, 22 where a high percentage indicated better knee function and psychological readiness.
Sample Size Estimation and Statistical Analysis
To estimate the sample size at an alpha level of .05 and power of 0.8, an a priori power analysis was performed using the 2-sided hypothesis test. Based on a previous study, 39 an SLHD difference of >14% between patients who successfully returned to their preinjury sports level and those who did not was assumed to indicate a clinical difference. Therefore, sample size estimation was based on our pilot study of 5 knees in each group, which found that 32 patients (effect size dz, 0.518) would be required to detect the SLHD difference of >14% between patients who returned to preinjury sports levels 2 years postoperatively and those who did not. The power for detecting this SLHD difference of >14% between the 2 groups was 0.810.
The Shapiro-Wilk test was used to determine whether continuous variables followed a normal distribution. Independent t and chi-square tests were used to compare continuous and categorical variables of demographic characteristics between the groups. Independent t tests with Bonferroni corrections were used to compare functional outcomes such as muscle and functional performances and PROs between patients who returned to preinjury sports levels 2 years after primary ACLR and those who did not. Pearson correlation analysis was performed to evaluate the associations between demographic data, muscle and functional performances, and PROs. Multiple linear regression analysis was used to identify the influence of the associated variables on the dependent variable (pre- or postoperative Tegner activity levels) using the significant variables of the Pearson correlation coefficients. Cohen d was assessed as a measurement of effect size. Statistical analysis was performed using SPSS Version 21.0 (IBM), with the significance level set at .05.
Results
In the present study, the primary outcomes were differences in functional outcomes between the 2 groups, and the secondary outcomes were factors related to the return to preinjury (preoperative Tegner activity levels) and postoperative (postoperative Tegner activity levels) sports levels 2 years after primary ACLR.
Table 1 summarizes the demographic data between the 2 groups, showing that sex, age, height, weight, body mass index, injured leg, preoperative Tegner activity levels, pain, graft type, concomitant surgery, and sports and activity levels did not differ significantly between groups (P > .05), except postoperative Tegner activity levels (Cohen d = 2.41; 95% CI, 1.8-3.0; P < .001).
Characteristics of Participants a
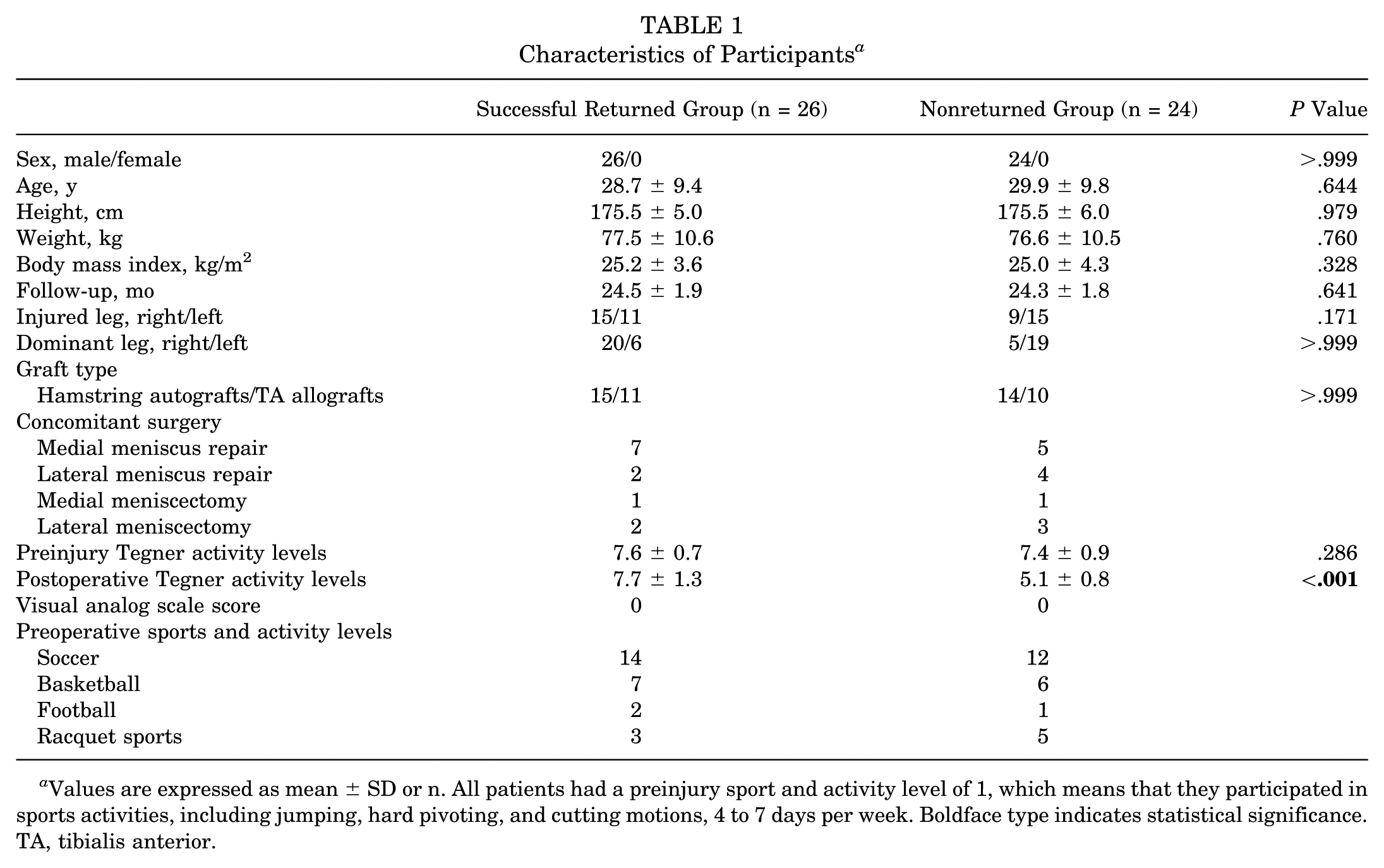
Values are expressed as mean ± SD or n. All patients had a preinjury sport and activity level of 1, which means that they participated in sports activities, including jumping, hard pivoting, and cutting motions, 4 to 7 days per week. Boldface type indicates statistical significance. TA, tibialis anterior.
Functional Outcomes
Table 2 shows a comparison of the muscle and functional performance outcomes, and PROs between the 2 groups. Two years postoperatively, the knee muscle strengths of the quadriceps and hamstring muscles did not differ significantly between the groups (all P > .05). Work fatigue of quadriceps muscles (Cohen d = −0.86; 95% CI, −12.2 to −2.5; P = .004) was better in patients who returned to preinjury sports levels than those who did not. However, work fatigue for hamstring muscles did not differ between the groups (P > .05). The SLHD (Cohen d = 1.21; 95% CI, 17.8 to 48.8; P < .001) was better in patients who returned to preinjury sports levels than those who did not. However, LSI–quadriceps, LSI–hamstring, and LSI–SLHD did not differ between the groups (all P > .05). The IKDC score (Cohen d = 2.14; 95% CI, 6.4 to 27.2; P < .001) and KOOS Sport and Recreation subscale (Cohen d = 1.05; 95% CI, 6.6 to 22.0; P < .001) were better in patients who returned to preinjury sports levels than those who did not, except for the Lysholm score and KOOS QoL subscale (P > .05).
Knee Muscle and Functional Performances, and Patient-Reported Outcomes Between the Groups a

Values are expressed as mean ± SD unless otherwise indicated. Boldface type indicates statistical significance. IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; LSI, limb symmetry index; QoL, Quality of Life; SLHD, single-leg hop distance.
Correlations and Associated Factors
The results of Pearson correlation and multiple linear regression analyses are presented in Tables 3 and 4, respectively. For the related factors in Pearson analysis, multiple linear regression analysis was performed to identify associated factors for pre- or postoperative Tegner activity level, and the results revealed that work fatigue of quadriceps muscles (R2 = 0.110; β = −0.332; P = .018) and SLHD (R2 = 0.084; β = 0.290; P = .041) were closely associated with preoperative Tegner activity level. In addition, work fatigue of quadriceps muscles (R2 = 0.157; β = −0.397; P = .004), SLHD (R2 = 0.283; β = 0.532; P < .001), and IKDC score (R2 = 0.452; β = 0.672; P < .001) were closely associated with postoperative Tegner activity level, not KOOS Sport and Recreation subscale (P > .05). These findings indicate that work fatigue of the quadriceps muscle and SLHD were closely associated with return to preinjury sports levels, and work fatigue of the quadriceps muscle, SLHD, and IKDC score were closely associated with the postoperative sports levels.
Correlations Between Parameters and Preinjury and Postoperative Tegner Activity Levels a

Boldface type indicates statistical significance. IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; PCC, Pearson correlation coefficient; SLHD, single-leg hop distance.
Multiple Linear Regression Analysis of Associated Factors for the Return to Preinjury and Postoperative Sports Levels

Boldface type indicates statistical significance. IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; SLHD, single-leg hop distance.
Discussion
The most important finding of the present study was that, 2 years after primary ACLR, the work fatigue of the quadriceps muscles, SLHD, IKDC score, and KOOS Sport and Recreation subscale were better in patients who returned to preinjury sports levels than in those who did not, whereas knee muscle strength, LSI, Lysholm score, and KOOS QoL subscale did not show notable differences. Work fatigue of the quadriceps muscles and SLHD were closely associated with return to preinjury sports levels, whereas knee muscle strength, LSI, and PROs were not. In addition, work fatigue of the quadriceps muscles, SLHD, and IKDC score were closely associated with the postoperative sports levels.
Most patients expect to return to their preinjury sports levels after primary ACLR. 37 Thus, various RTS test batteries, such as muscle strength, function (hop), and movement quality, are introduced for objective assessment of return to preinjury sports levels.11,13,35 Among various RTS test batteries, muscle strength evaluation is the most basic and primarily used. In the present study, 2 years postoperatively, knee muscle strength did not significantly differ between patients who returned to preinjury sports levels and those who did not. However, Welling et al 39 reported that only hamstring strength differed between patients who returned to preinjury sports levels 1 year after ACLR versus patients who did not. In contrast, Hamrin Senorski et al 13 reported that at 10 months after ACLR, only quadriceps strength differed between female patients who returned to preinjury sports levels and those who did not; however, a difference was not observed in male patients. The knee muscle strength is affected by age and sex (female). 28 In our study, there was no difference in age between the 2 groups, and all study participants were male; however, the above 2 studies had differences in age and sex between the groups that successfully returned and those who did not. In particular, the follow-up periods in the previous studies were 10 months 39 and 1 year, 13 respectively, which were shorter than that in our study. Additionally, in the present study, the reliability of the isokinetic muscle strength test was excellent (CV, <10%), 27 but it has not been evaluated in previous studies. Furthermore, Faleide et al 9 reported that the LSI of isokinetic strength did not differ between patients who returned to preinjury sports levels 2 years after ACLR and those who did not. Similar results were obtained in this study. Therefore, assessments of muscle strength and LSI may not be sufficient to differentiate between patients who return to their preinjury sports levels and those who do not.
Recent studies have reported that SLHD was better in patients who returned to their preinjury sports levels after ACLR than in patients who did not, 39 but there was no difference in LSI–SLHD.9,14,39 Our results support these previous findings. In addition, our results also showed that the IKDC score and KOOS Sport and Recreation subscale were better in patients who returned to preinjury sports levels than in patients who did not. Several studies have reported that patients with high IKDC score (>90) after ACLR can return to their preinjury levels,32,38 with scores ≥90 and ≤80 classified as excellent and fair, respectively. 15 In our study, patients who successfully returned to their preinjury sports levels had an IKDC score of 95.0 ± 3.7, whereas those who did not had an IKDC score of 78.6 ± 10.2. Furthermore, Faleide et al 9 reported that patients who were unable to return to preinjury sports levels had low psychological readiness, and Cronström et al 7 reported that low psychological readiness for RTS was associated with short hops and worse KOOS Sport and Recreation subscales. Similar results were obtained in this study. Taken together, these results suggest that SLHD, IKDC score, and KOOS Sport and Recreation subscale may be important factors in distinguishing between the patients who successfully returned to preinjury sports levels and those who did not. However, the KOOS QoL subscale (psychological readiness status) may reflect knee osteoarthritis more than ACL; hence, there was no difference between the groups. 22
Previous studies have reported that age, psychological readiness, LSI–SLHD, and LSI–muscle strength are associated with successful return to preinjury sports levels.9,13,40 However, the most notable finding of the present study was that work fatigue of the quadriceps muscles and SLHD were better in patients with successful return to their preinjury sports levels, and were associated with return to preinjury and postoperative sports levels. These discrepancies in results are difficult to determine, but this may be due to differences in the criteria for returning to preinjury sports levels among participants. The criteria for returning to preinjury sports levels vary across studies. Many studies have used Tegner activity levels to assess resumption of preinjury sports participation.13,14,18 In the present study, the criteria for return to preinjury sports levels were also assessed using Tegner activity level ≥6 and postoperative current sports participation type. Klasan et al 18 suggested that patients with low preoperative Tegner activity levels return to low-level sports 2 years after ACLR. Wan et al 36 reported that muscle fatigue affects neuromuscular control, resulting in negative knee joint biomechanics26,34 and physical performance. 36 In particular, altered neuromuscular control may contribute to increased reinjury risk and failure to perform RTS. 4 Therefore, patients with high muscle fatigue and low SLHD after ACLR may have limited sports participation, which may affect their return to preinjury and postoperative sports levels. Hence, we suggest that work fatigue and SLHD assessment should be considered.33,35 Furthermore, muscle strength and LSI may not have as significant an effect on returning to preinjury sports levels as previously assumed. Therefore, greater emphasis should be placed on quadriceps endurance and neuromuscular training in postoperative rehabilitation programs to facilitate a successful RTS.
Limitations
The present study has some limitations. First, this study was a retrospective observational study, which does not permit inferences as to cause and effect. Second, the number of patients who participated in the study was small because a high percentage of eligible patients were lost to follow-up; thus, high-quality studies with large sample sizes may be needed. Third, there was no normal (control) group; thus, further study with comparison with a normal group may be needed to clarify the results of this study. Fourth, there was a lack of movement quality and psychological readiness assessment, which may be associated with RTS after ACLR.8,9 However, the appropriate movement quality and optimal amount of psychological readiness for RTS remains unknown. 5 Fifth, the results of the present study compared functional outcomes between general patients with and without return to preinjury sports levels, rather than athletes; thus, there may be differences in the qualitative assessment of RTS. However, we tried to clarify the criteria for returning to preinjury and postoperative sports levels using the Tegner activity levels and sports activity rating scale. Sixth, we did not perform isokinetic eccentric muscle testing. Eccentric activity of the quadriceps and hamstring muscles may be important for functional aspects of the knee. 30 Finally, in the present study, ACLR was performed using 2 different graft types (hamstring autograft or tibialis anterior allograft), but no comparative analysis was performed. A systematic review and meta-analysis by Kay et al, 17 however, reported that there was no significant difference in the rate of return to preinjury sports levels between graft choices (hamstring autografts or allografts).
Conclusion
Two years after primary ACLR using either hamstring autograft or tibialis anterior allograft, patients who returned to their preinjury sports levels demonstrated better outcomes in work fatigue, SLHD, IKDC score, and the KOOS Sport and Recreation subscale compared with those who did not. Notably, quadriceps work fatigue was closely associated with both return to preinjury sports levels and postoperative sports participation levels.
Footnotes
Final revision submitted July 22, 2025; accepted August 11, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported by the Korea Medical Device Development Fund grant funded by the Korea government (the Ministry of Science and ICT, the Ministry of Trade, Industry and Energy, the Ministry of Health & Welfare, the Ministry of Food and Drug Safety) (Project Number: 1475013503, RS-2023-00210209). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Anam Hospital, Korea University (2018AN0261).