
Abstract
Background:
Femoroacetabular impingement (FAI) syndrome is a common cause of hip pain in elite athletes and frequently necessitates hip arthroscopy in National Hockey League (NHL) players. While high return-to-sport (RTS) rates are reported, the long-term impact of surgery on player performance using advanced analytics has not been well studied.
Hypothesis:
Players undergoing surgery would exhibit steeper performance declines in defensive performance metrics relative to matched controls, despite similar RTS rates.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
This matched cohort study identified NHL skaters who underwent hip arthroscopy for FAIS between 2000 and 2024 using publicly available databases. Surgical confirmation was established through ≥2 independent sports news outlets. Players active for ≥2 seasons between 2007 and 2025 were matched 1:1 to controls based on position and performance at age 24. Outcomes included Wins Above Replacement per 60 minutes (WAR/60) and offensive and defensive Goals Above Replacement per 60 minutes (Off GAR/60, Def GAR/60), obtained from Evolving-Hockey. Fixed-effects panel regression with joint F tests was used to model longitudinal aging curves and isolate surgical effects from natural performance decline.
Results:
A total of 63 NHL skaters (42 forwards, 21 defensemen) were included and matched to controls. Among forwards, hip arthroscopy was associated with a statistically significant decline in Def GAR/60 across the aging curve (interaction P = .04), while Off GAR/60 (P = .64) and WAR/60 (P = .40) showed no significant differences. No statistically significant performance differences were observed among defensemen.
Conclusion:
This study demonstrated that hip arthroscopy was associated with a steeper age-related decline in defensive performance among NHL forwards, while offensive metrics and overall player value remained unaffected. No significant performance differences were noted in defensemen. Integrating surgical history into performance models may improve player evaluation and recovery strategies.
Hip and groin injuries are among the most common musculoskeletal ailments in professional ice hockey, affecting up to 50% of players during their careers, with approximately 10% eventually requiring hip arthroscopy to address intra-articular pathologies such as femoroacetabular impingement (FAI) and labral tears. 22 The high biomechanical demands of ice hockey, including repetitive hip flexion, rapid acceleration, and frequent pivoting, render National Hockey League (NHL) athletes particularly vulnerable to these disorders.10,17 FAI has also been identified as a risk factor for premature hip osteoarthritis, with radiographic progression observed in up to 81% of symptomatic individuals over a 10-year period. 1
Hip arthroscopy, often including osteochondroplasty and labral repair, has become the treatment of choice for elite athletes with FAI who have failed nonoperative management, with reported return-to-sport (RTS) rates ranging from 78% to 100% in professional hockey players.7,9,11,12,18,21 However, RTS rates alone may not fully reflect the impact of surgery on a player's long-term performance or career duration. Prior studies have found that while NHL athletes may experience performance declines in the first postoperative season, many return to baseline by year 2. 7 Nonetheless, career longevity remains reduced in some players, with a mean of 5.9 years of continued play following hip arthroscopy, with lesser numbers competing beyond 10 years. 14
Historically, player performance has been assessed using basic counting statistics such as games played, goals, and assists.6,13,21 While these metrics are easily understood, they are limited by low event frequency, susceptibility to random variation, and contextual influences such as linemate quality, opponent strength, and ice time.6,13 In response to these limitations, advanced performance analytics—namely, Goals Above Replacement (GAR) and Wins Above Replacement (WAR)—have gained traction within NHL analytics departments. These composite statistics account for offensive and defensive contributions relative to a theoretical replacement-level player while adjusting for team strength, zone starts, and playing time.6,23,25
GAR and WAR offer a more predictive and context-neutral framework for assessing player value and have been widely adopted by both teams and researchers as tools for modeling player development, assessing trades, and guiding medical decision-making.8,24,25 Although prior work has characterized age-performance curves in NHL players, showing peak productivity between ages 24 and 28 followed by gradual decline,2,3 no study to date has examined how surgical treatment for FAI influences these trajectories.
Defensive contributions in hockey frequently rely on backward skating, lateral-edge control, and positional stability, all of which demand substantial hip mobility and dynamic control.5,7 As such, it is plausible that hip pathology and subsequent arthroscopy may disproportionately affect defensive performance relative to offensive production. The purpose of this study was to assess whether hip arthroscopy alters age-related performance decline in NHL players. Based on this, we hypothesized that players undergoing surgery would exhibit steeper performance declines in defensive performance metrics relative to matched controls, despite similar RTS rates.
Methods
Study Design and Data Source
Institutional review board approval was not required, as this study exclusively utilized publicly available data. NHL players who sustained intra-articular hip injuries requiring arthroscopic surgery were identified using previously described methodologies.7,21 Publicly accessible data from the NHL Injury Viz database were searched from its inception (2000-2001) through the 2023-2024 season. 16 To maximize case capture and account for potential misclassification, injuries listed as “hip,”“groin,” or “lower body” were included. Confirmation of hip arthroscopy was established through ≥2 independent sports news outlets, including The Sports Network (Canada) and Entertainment and Sports Programming Network.
Players were included if they were placed on the NHL injured list and had their hip arthroscopy verified by ≥2 public sources. Athletes with concurrent injuries requiring surgery were excluded to minimize confounding. The NHL began collecting the tracking data necessary for advanced performance metrics during the 2007-2008 season; thus, only players who underwent hip arthroscopy and competed in ≥2 seasons between 2007-2008 and 2024-2025 were eligible. Players were followed longitudinally for up to 9 seasons after surgery. Goaltenders were excluded, as their performance metrics differ substantially from skaters and are not captured by GAR/WAR models.
Demographic and Injury Characteristics
Extracted data included player height, weight, position, injury laterality (unilateral or bilateral), years of NHL experience at the time of surgery, diagnosis subtype, and nationality. Laterality data were extracted where available; however, insufficient detail regarding the timing and sequencing of bilateral procedures precluded a meaningful subgroup analysis.
Outcome Measures
Performance data were obtained from Evolving-Hockey, a publicly available platform widely used in sports analytics research.4,7 Outcome definitions are summarized in Table 1. Advanced statistics were selected over traditional metrics because of their superior reliability, ability to adjust for contextual factors (eg, linemates, opponent strength, deployment), and more meaningful representation of player value.6,23,25
Description of Advanced Analytic Metrics in National Hockey League Players a

Def GAR/60, defensive Goals Above Replacement per 60 minutes; Off GAR/60, offensive Goals Above Replacement per 60 minutes; RAPM, Regularized Adjusted Plus-Minus; WAR/60, Wins Above Replacement per 60 minutes played.
The primary outcome was WAR per 60 minutes played (WAR/60), a composite statistic quantifying the number of team wins a player contributes per 60 minutes of ice time compared with a replacement-level player. A replacement-level player was defined as all forwards below the top 13 and defensemen below the top 7 per team in time on ice per season.23-25 A WAR/60 value above zero indicates a contribution above replacement level, while negative values indicate below-replacement performance. This measure is adjusted for teammate/opponent quality, schedule difficulty, and team success (eg, playoff qualification).
Secondary outcomes included offensive and defensive GAR per 60 minutes (Off GAR/60 and Def GAR/60), which isolate a player's offensive and defensive contributions, respectively. These are derived similarly to WAR but focus on specific dimensions of performance. The sum of Off GAR/60 and Def GAR/60 equals total GAR, which is then scaled to estimate WAR.23-25 Outcome data were collected for every available season from 2007-2008 through 2024-2025.
Cohort Matching
Players who underwent hip arthroscopy were matched 1:1 with controls based on position and performance at age 24 (or the closest available age if not active during that season). Age 24 was selected as the matching point because prior literature has established it as the onset of a player's peak performance plateau, typically lasting through age 28. 2 Each matched pair was then followed longitudinally using WAR, Off GAR/60, and Def GAR/60 to evaluate postoperative performance trends relative to nonsurgical counterparts. Controls were verified via the NHL Injury Viz database to confirm no history of hip injuries or surgical intervention during their careers. 16
Statistical Analysis
All statistical analyses were conducted using Stata (Version 19.0; StataCorp LLC). Aging curves, which are performance trajectories by age, can be estimated using several methods.2,3 Traditional approaches, which average performance at each age across all active players, may underestimate the true effect of aging, as only higher-performing athletes tend to remain in the league at older ages. 2 To address this, fixed-effects panel regression was used to estimate aging curves and isolate the effect of hip arthroscopy from natural aging trajectories. This technique adjusts for unobserved, time-invariant player characteristics (eg, baseline skill level), allowing for more accurate estimation of within-player changes over time. Panel regression is appropriate for longitudinal data, where multiple observations per player are available across seasons. 2 Aging curves were modeled separately for players with and without a history of hip arthroscopy.
Athletes were followed from their index season (hip arthroscopy for cases, age-24 season for controls) until career end or the 2024-2025 season, whichever occurred first. When one member of a matched pair retired earlier than the other, all available data for the active player continued to contribute to the regression analysis. The fixed-effects panel regression framework accommodated unbalanced longitudinal data, allowing for differing lengths of follow-up across players. 2
The regression model included age and age2 to capture the known nonlinear aging trajectory (initial improvement followed by decline) and interaction terms between FAI status and both age terms to assess differential effects:

In this model, β (B) represents the estimated regression coefficients. The subscript i identifies individual players, and t represents each season (time point) for that player; thus, the term it denotes an observation for player i in season t. The dependent variable (Performanceit) corresponds to the player's WAR/60, Off GAR/60, or Def GAR/60 in a given season. Age was the player's age at the start of that season, and Age2 captured the nonlinear aging trajectory (improvement followed by decline). Surgery was a binary variable coded as 1 for players who underwent hip arthroscopy at any point in their career and 0 for matched controls. The interaction terms (Age × Surgery and Age2× Surgery) tested whether performance trajectories differed between surgical and nonsurgical cohorts. αi was the player-specific fixed effect, which accounted for unobserved, time-invariant characteristics unique to each player (eg, baseline skill level), and εit was the error term.
To evaluate whether performance trajectories differed significantly by surgical status, a joint F test was performed on the FAI-age interaction terms. A P value <.05 was considered statistically significant and interpreted as evidence that players who underwent hip arthroscopy experienced a different age-related performance trajectory compared with those who did not.
Results
Participant Selection
A total of 4838 NHL player injuries were screened, including 472 hip injuries, 1276 groin injuries, and 3090 lower body injuries. After excluding 4761 injuries that did not meet inclusion criteria, 77 NHL players were identified as having undergone arthroscopic hip surgery. Of these, 21 goaltenders and 9 players not active between the 2007-2008 and 2024-2025 seasons were excluded (n = 30). An additional 16 eligible players were identified and included through media and public reporting. Thus, 63 skaters were ultimately included in the final analysis, comprising 42 forwards and 21 defensemen (Figure 1).

Flowchart of National Hockey League player selection for inclusion following hip arthroscopy.
Demographic and Injury Characteristics
Baseline characteristics of the included players are presented in Table 2. Each cohort comprised 63 individuals, including 42 forwards and 21 defensemen. The mean age at the time of surgery was 29.1 years for both forwards (SD, 4.5) and defensemen (SD, 4.7). Players who underwent surgery had a mean of 8.6 years (SD, 4.3) of NHL experience at the time of surgery for forwards and 8.7 years (SD, 4.4) for defensemen. The mean number overall of seasons played after surgery was 3.0 (range, 1-9 seasons), with defensemen averaging 3.0 (SD, 2.0) seasons and forwards averaging 3.1 (SD, 2.0) seasons.
Baseline Characteristics of NHL Players Undergoing Hip Arthroscopy Surgery Compared With Matched Controls a

Data are presented as n or mean (SD). NA, not applicable; NHL, National Hockey League. Dashes indicate no values.
The control group had slightly greater mean height and weight, but there were no statistically significant differences between groups across any demographic variable. No conclusions could be drawn regarding the effect of laterality on outcomes. A diverse range of nationalities was represented, with comparable distributions across surgical and control cohorts (Table 2).
Forward Performance Trajectories
The aging curves for NHL forwards are depicted in Figure 2. Among players who underwent hip arthroscopy, offensive performance (Off GAR/60) initially exceeded that of controls and remained higher through the mid-20s to early 30s. However, defensive performance (Def GAR/60) was consistently lower in the surgical cohort compared with controls across all ages, with a visible widening deficit beyond age 28. This persistent decline in defensive output may have contributed to the overall lower WAR/60 observed in surgical cases, which declined more steeply than in controls after age 27 (Figure 2).

Age-performance curves for National Hockey League forwards following hip arthroscopy compared with matched controls. GAR, Goals Above Replacement; WAR, Wins Above Replacement.
Regression modeling results for forwards are summarized in Table 3. Statistically significant nonlinear relationships were observed between age and all 3 performance metrics, with both age and age2 terms reaching significance for Off GAR/60 (P = .002 and .001), Def GAR/60 (P = .002 and .001), and WAR/60 (P < .001 for both), respectively, confirming the expected rise and fall of player performance over time. For defensive performance, significant interaction effects between surgical status and both age (P = .013) and age2 (P = .015) were observed.
Multivariable Regression Output for Aging Curves in National Hockey League Forwards a

Regression coefficients represent the estimated change in the performance metric (Off GAR/60, Def GAR/60, or WAR/60) associated with a 1-unit increase in the predictor variable. For example, a negative coefficient for age2 reflects the expected curvilinear decline in performance with advancing age. A negative coefficient for an Free agent injury-age interaction term suggests that players with a history of hip arthroscopy experience steeper declines in performance as they age, relative to controls. R2 values indicate the proportion of variance explained by the model. Bold P values indicate statistical significance at P < .05. Age, player age at the start of the season; Age2, quadratic term capturing nonlinear aging trajectory (initial improvement then decline); Def GAR/60, Defensive Goals Above Replacement per 60 minutes played; Free agent injury age, age at which player first became a free agent after injury; Off GAR/60, offensive Goals Above Replacement per 60 minutes played; WAR/60, Wins Above Replacement per 60 minutes played.
However, no significant Free agent injury-age interaction terms were identified for Off GAR/60 (P = .51 and .47) or WAR/60 (P = .32 and .37), respectively, and the overall F test for the joint significance of these interaction terms was not statistically significant for Off GAR/60 (P = .64) or WAR/60 (P = .40). Model R2 values were low across all outcomes (Table 3).
Defensive Performance Trajectories
The aging curves for NHL defensemen are illustrated in Figure 3. Among players who underwent hip arthroscopy, offensive and defensive performance metrics (Off GAR/60 and Def GAR/60) closely paralleled those of matched controls across all ages, with minimal separation between groups. Likewise, WAR/60 values remained comparable between surgical and control cohorts throughout the aging curve. No statistically significant differences were identified between groups for any performance metric (Figure 3).

Age-performance curves for National Hockey League defensemen following hip arthroscopy compared with matched controls. GAR, Goals Above Replacement; WAR, Wins Above Replacement.
Regression modeling results for defensemen are presented in Table 4. No statistically significant associations were identified between age, age2, and any performance outcomes, including Off GAR/60 (P = .10 and .05), Def GAR/60 (P = .36 and .29), or WAR/60 (P = .18 and .11), respectively. These findings indicate no observable age-related changes in performance among defensemen based on the current sample.
Multivariable Regression Output for Aging Curves in National Hockey League Defensemen a
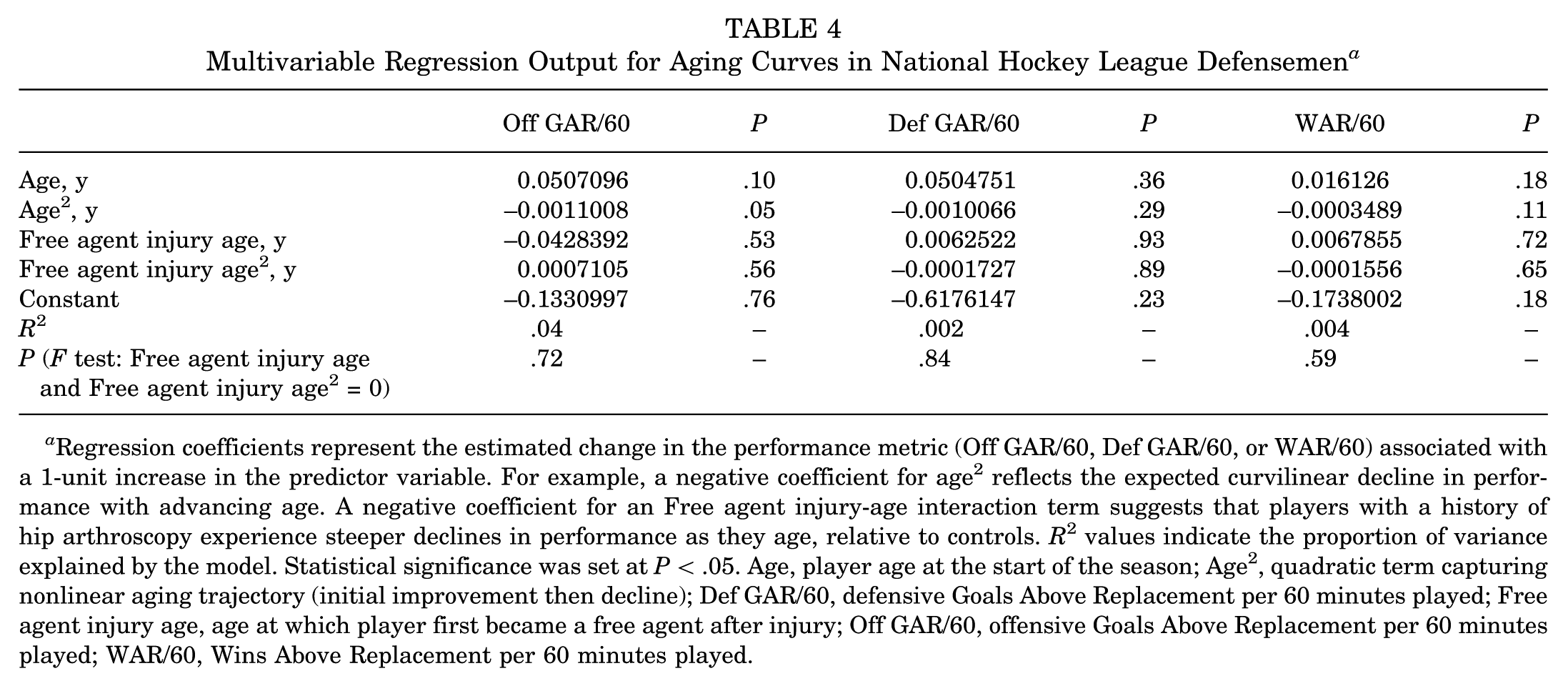
Regression coefficients represent the estimated change in the performance metric (Off GAR/60, Def GAR/60, or WAR/60) associated with a 1-unit increase in the predictor variable. For example, a negative coefficient for age2 reflects the expected curvilinear decline in performance with advancing age. A negative coefficient for an Free agent injury-age interaction term suggests that players with a history of hip arthroscopy experience steeper declines in performance as they age, relative to controls. R2 values indicate the proportion of variance explained by the model. Statistical significance was set at P < .05. Age, player age at the start of the season; Age2, quadratic term capturing nonlinear aging trajectory (initial improvement then decline); Def GAR/60, defensive Goals Above Replacement per 60 minutes played; Free agent injury age, age at which player first became a free agent after injury; Off GAR/60, offensive Goals Above Replacement per 60 minutes played; WAR/60, Wins Above Replacement per 60 minutes played.
Similarly, no statistically significant Free agent injury-age interaction terms were found for any of the 3 performance outcomes. For Off GAR/60, interaction term P values were .53 and .56; for Def GAR/60, .93 and .89; and for WAR/60, .72 and .69. The joint F tests for overall interaction significance also failed to reach significance: P = .72 for Off GAR/60, P = .84 for Def GAR/60, and P = .59 for WAR/60. Model R2 values were low across all outcomes (Table 4).
Discussion
The major findings of this matched cohort study were that forwards who underwent hip arthroscopy demonstrated a statistically significant steeper age-related decline in defensive performance (Def GAR/60; P = .04), whereas offensive performance (Off GAR/60; P = .64) and overall value (WAR/60; P = .40) were not significantly different compared with controls. No significant differences were observed among defensemen across any performance metric.
The finding of a statistically significant interaction between surgical status and age for defensive performance among forwards suggests that hip arthroscopy may impair the ability to contribute defensively as players age. Def GAR/60 was consistently lower in the surgical cohort, with a widening deficit relative to matched controls. This may reflect lingering biomechanical or proprioceptive deficits postsurgery that affect backward skating, edge control, positional play, or penalty-kill effectiveness, which are skills more critical to defensive contributions than raw offensive output. 15 It also raises the possibility that compensatory movement patterns or subtle declines in mobility after surgery may disproportionately affect defensive effectiveness. These changes could influence a player's role, ice time, and long-term value to teams, especially in situations requiring strong defensive reliability.
Importantly, several performance metrics showed no statistically significant differences between surgical and control cohorts. Among forwards, neither Off GAR/60 nor WAR/60 demonstrated meaningful divergence between groups over time, despite visual trends. For defensemen, all 3 metrics, Off GAR/60, Def GAR/60, and WAR/60, remained statistically nonsignificant across the aging curves. These findings may reflect the multifactorial and context-dependent nature of player performance, which is influenced by a range of factors including linemates, coaching strategies, role assignments, and concurrent injuries unrelated to the hip.6,13,23,25 Defensemen often rely on structured, positional play and may be less dependent on explosive movements and directional changes than forwards, who frequently engage in high-intensity transitions, cuts, and zone entries that place greater demands on hip mobility and power. 20 Collectively, the nonsignificant findings and low model R2 values highlight the challenges in isolating the specific impact of hip arthroscopy on long-term performance.
These results align with prior studies showing high RTS rates in NHL players after hip arthroscopy, but raise concerns about the quality of performance upon return. While LaPrade et al 11 and Hayes et al 7 demonstrated a return to baseline statistics by year 2, they focused primarily on traditional metrics such as games played, points, and time on ice. By contrast, this study used WAR and GAR metrics, which offer greater sensitivity and adjust for team context, deployment, and strength of opponents.6,23,25
The statistical decline in defensive performance among forwards aligns with biomechanical studies demonstrating residual asymmetries in hip strength and range of motion following arthroscopic management of FAI. While the clinical significance of this performance decrement remains uncertain, similar trends have been reported in other professional sports. For example, in Major League Baseball, Schallmo et al 19 found that pitchers who underwent hip arthroscopy, particularly on their lead leg, returned to play at high rates but showed measurable reductions in performance, including fewer pitches thrown and decreased fastball velocity. These findings suggest that, despite successful RTS, subtle postoperative mobility deficits may persist and affect athletic output over time. In the present cohort, it is plausible that comparable deficits could contribute to the observed differences in defensive performance, although further research is needed to clarify the biomechanical and functional correlates of these changes.
In addition to biomechanical limitations, persistent hip-related discomfort or apprehension may reduce a player's willingness to engage fully in defensive tasks such as backchecking or sustained play in the defensive zone. These behavioral adaptations could further amplify declines in defensive performance among forwards, independent of measurable deficits in hip mobility or strength. While speculative, this perspective highlights the multifactorial nature of performance outcomes following hip arthroscopy and warrants further investigation.
Strengths and Limitations
This study offers several strengths. It is the first to apply advanced hockey analytics, specifically WAR and GAR, to assess longitudinal performance following hip arthroscopy in professional hockey players. As advanced analytics continue to gain prominence, incorporating medical history into WAR/GAR-based models may allow for more accurate forecasting of a player's future contributions and monetary value. The matched cohort design, using performance at age 24 as the anchor point, minimizes confounding by natural variation in career trajectory. Furthermore, fixed-effects regression modeling controls for player-specific, time-invariant factors, allowing a more accurate estimation of within-player changes over time. The inclusion of both offensive and defensive components also provides a more nuanced view of postsurgical performance across roles.
That being said, this study has several limitations that should be acknowledged. First, although matched controls were selected based on position and performance at age 24, unmeasured confounders such as player role, usage, injury burden, and playing style may have influenced outcomes. Second, surgical laterality, specific procedure details (eg, labral repair vs debridement), and time to return were not available, which limits the ability to stratify outcomes by surgical technique. Future studies incorporating direct surgical and rehabilitation data are needed to refine these comparisons. Moreover, surgical techniques and indications for hip arthroscopy have evolved over the study period; earlier cases were more likely to involve labral debridement or prophylactic procedures on minimally symptomatic players, which are less common in current practice. Third, R2 values were low across all regression models, suggesting that the predictors used explain only a small portion of the variance in performance. This reflects the highly individualized nature of athletic performance and the influence of contextual factors such as linemates, special teams deployment, and coaching strategy. Fourth, the identification of surgical cases was based on publicly available reports and media sources, which introduces the potential for selection and reporting bias. Similarly, goaltenders were excluded given the incompatibility of their performance statistics with WAR/GAR models. As hip pathology is also common among goalies, future research using position-specific analytics (eg, save percentage, expected goals against) is needed to evaluate this population. Last, the relatively small sample size, particularly among defensemen, limited the statistical power to detect subtle differences in performance and may restrict the generalizability of the findings.
Future studies should incorporate biomechanical assessments, surgical technique data, and in-game tracking to better characterize recovery patterns and refine rehabilitation protocols. Expanding this approach to other sports or larger cohorts may help generalize findings and enhance return-to-play strategies.
Conclusion
This study demonstrated that hip arthroscopy was associated with a steeper age-related decline in defensive performance among NHL forwards, while offensive metrics and overall player value remained unaffected. No significant performance differences were noted in defensemen. Integrating surgical history into performance models may improve player evaluation and recovery strategies.
Footnotes
Acknowledgements
The authors acknowledge and thank Nicole Simunovic, MSc, for her contributions in reviewing and assisting with the final edits of the manuscript.
Final revision submitted August 26, 2025; accepted September 2, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: O.R.A. has received speaker fees from Stryker Canada and research funding from the Canada Research Chair. J.T. serves as the medical director and head team physician for the Toronto Maple Leafs. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not required for this study.