
Abstract
Background:
Acromioclavicular (AC) dislocations are common shoulder injuries. Coracoid tunnel–free coracoclavicular (CC) sling fixation techniques using either allograft or Tightrope represent viable treatment options.
Purpose:
To (1) compare the clinical outcomes of 2 different coracoid tunnel–free CC sling fixation techniques (allograft vs Tightrope) in treating patients with acute Rockwood type 3 and 5 AC dislocations for a minimum of 24-month follow-up and to (2) identify risk factors for loss of reduction (LOR).
Study Design:
Cohort study; Level of evidence, 3.
Methods:
We compared patients treated for AC dislocations using CC sling fixation with either allograft or Tightrope. Functional outcomes (visual analog scale, American Shoulder and Elbow Surgeons score, Constant score, and return to sport) were recorded at 12- and 24-month follow-ups. CC distance (CCD) and complications were evaluated at 3, 6, and 12 months postoperatively. Univariate and multivariate analyses were performed to identify risk factors for LOR.
Results:
Of the 50 patients included, 23 were in the allograft group and 27 in the Tightrope group. Both groups demonstrated significant improvements in functional outcome postoperatively, without significant intergroup differences. Although CCD significantly decreased in both groups, CCD in the Tightrope group was significantly smaller at each follow-up. Compared with CCD immediately after surgery, CCD remained stable in the Tightrope group at 3-month follow-up (P = .13), whereas it significantly increased in the allograft group (P = .004.). The allograft group exhibited a significantly higher rate of LOR than the Tightrope group (43% vs 15%; P = .03), heterotopic ossification (48% vs 11%; P = .005), and greater tunnel widening (P < .001). The trapezoid tunnel ratio was identified as an independent risk factor for LOR in the allograft group (odds ratio, 0.033; P = .017).
Conclusion:
Despite similar functional outcome, CC sling fixation with Tightrope demonstrated superior maintenance of CCD in the early postoperative stage, a significantly lower rate of LOR and heterotopic ossification and less tunnel widening compared with allograft. Malposition of the trapezoid tunnel was an independent risk factor for LOR in the allograft group.
Acromioclavicular (AC) dislocations are common shoulder injuries with an incidence of 2 per 10,000 person-years. AC injuries typically result from traffic accidents and sports-related trauma, predominately affecting young male patients.23,26,33 Low-grade injuries (Rockwood 1-2) are generally managed nonoperatively, whereas some authors recommend surgical intervention for high-grade injuries. Although the treatment of Rockwood type 3 AC dislocations remains controversial, suggested indications for surgery in patients with type 3 injuries included unstable Rockwood 3B injury, unacceptable deformity, athletes, young patients engaged in heavy labor, and patients demanding surgical treatment.1,2,15,21
Although over 150 different methods for treating AC injuries have been described in the literature, arthroscopic coracoclavicular (CC) fixation has some theoretical advantages.1,13,15,27,31,43 Traditional CC fixation techniques, which involved drilling tunnels in the coracoid, are associated with a risk of coracoid fractures, a serious complication that can negatively affect patient surgical outcomes and often requires revision surgery.9,17,24,28 In response to this concern, the coracoid tunnel–free CC sling technique was developed to minimize the risks of coracoid-related complications.8,10,22,25 Initially, CC sling fixation was performed with allografts.10,25 However, with the widespread use of the Tightrope system (Arthrex) in clinical practice, CC sling fixation using the Tightrope system has demonstrated promising results in the management of high-grade AC joint dislocations and may simplify surgical procedures.22,29,36 To our knowledge, there is no study comparing results of 2 different arthroscopically assisted coracoid tunnel–free CC sling fixation techniques (allograft vs Tightrope) in the treatment of patients with acute Rockwood type 3 and 5 AC dislocations.
The hypothesis of this study was that CC sling fixation with Tightrope would yield superior radiological and clinical outcomes compared with the allograft. The secondary aim was to discover the risk factors for loss of reduction (LOR) for both techniques.
Methods
Patient Selection
This study was a retrospective analysis of prospectively collected data from patients who underwent arthroscopically assisted coracoid tunnel–free CC sling fixation technique using allogenous hamstring tendon (January 2015 to January 2017) or Tightrope system (January 2021 to January 2023). All procedures were performed by 2 senior surgeons (C.J. and Y.Z.). In our department, we began using allograft to treat acute AC dislocations in 2011. However, starting in 2014, the availability of allografts at our institution became inconsistent. As a result, we employed the Tightrope system to manage acute AC dislocations and observed satisfactory clinical outcomes, as shown in our previous case series. 22 By 2017, the Tightrope system had fully replaced allografts as our standard surgical technique for acute high-grade AC dislocations. Patients treated between 2017 and 2021 were not included in this study because of incomplete follow-up data and reduced surgical volume during the COVID-19 pandemic. After 2021, clinical follow-up stabilized and we resumed consistent data collection. The study protocol was approved by the institutional review board and informed consents were obtained from all patients. Patients were eligible for study if they met the following criteria: (1) Rockwood type 3 (young patients engaged in heavy labor, unacceptable deformity, athletes, and patients demanding surgical treatment) or type 5 injuries, (2) time interval from injury to surgery <3 weeks, (3) arthroscopic CC sling fixation with either allograft of Tightrope system, and (4) a minimum of 2-year follow-up. The exclusion criteria were (1) AC injury with an associated coracoid or distal clavicular fracture, (2) associated neurovascular injuries, (3) concomitant shoulder pathology (rotator cuff tear, anterior shoulder instability, superior labral anteroposterior lesion), (4) previous surgery on the same shoulder, and (5) loss to follow-up.
Surgical Technique
The patients were placed in a beach-chair position under general anesthesia and interscalene block. Initially, diagnostic arthroscopy was performed through the standard posterior portal to identify intra-articular pathologies. A complete debridement of the rotator interval was performed to expose the undersurface of the coracoid with radiofrequency device inserted from the anterolateral portal. The arthroscope was switched to the subacromial space through the primary posterior portal. A lateral subacromial portal was created and an examination of the bursal side of the rotator cuff was performed. Then, the arthroscope was subsequently placed in the lateral subacromial portal, and a bursectomy using a shaver inserted from the anterolateral portal was performed to expose the lateral margin of the conjoint tendon, anterior margin of the coracoacromial ligament, and superior surface of the coracoid. The AC joint was then exposed at the superior end of the coracoacromial (CA) ligament. The torn AC capsule was resected and the distal end of the clavicle was exposed. A trial reduction of the distal end of the clavicle was performed. If the reduction was affected by any torn ligament or articular disc within the AC joint, then this tissue was resected completely.
While maintaining the arthroscope in the lateral portal, an anteromedial portal was created using an outside-in technique with a spinal needle to ensure access to the medial side of the coracoid. A small portion of the pectoralis minor insertion was carefully removed from the coracoid. A right-angle clamp with a shuttle suture was then introduced through the anteromedial portal from medial to lateral beneath the coracoid. The shuttle suture was pulled out from the lateral side of the coracoid, posterior to the CA ligament and through the anterolateral portal. Two spinal needles were inserted percutaneously just anterior to the clavicle to mark the mediolateral position of the 2 tunnels on the clavicle, with the medial needle located next to the conoid ligament remnant and the lateral needle located next to the trapezoid ligament remnant. A 2- to 3-cm incision was made along the clavicle, and further exposure to the bony surface was performed. Two 4.0-mm tunnels were drilled along the marking needles and perpendicular to the surface of the clavicle. The 2 ends of the shuttle sutures were pulled out of the 2 clavicular tunnels.
Allograft group: the allograft tendon (semitendinosus) and 4 No 2. FiberWire sutures (AR-7200; Arthrex) were then passed sequentially through the lateral tunnel, underneath the coracoid and the medial channel. The clavicle was pressed down to reduce the AC joint under direct visualization arthroscopically. Then the high-strength sutures were tied on the superior surface of the clavicle. Subsequently, the allograft tendon was tightened and sutured (Figure 1A).
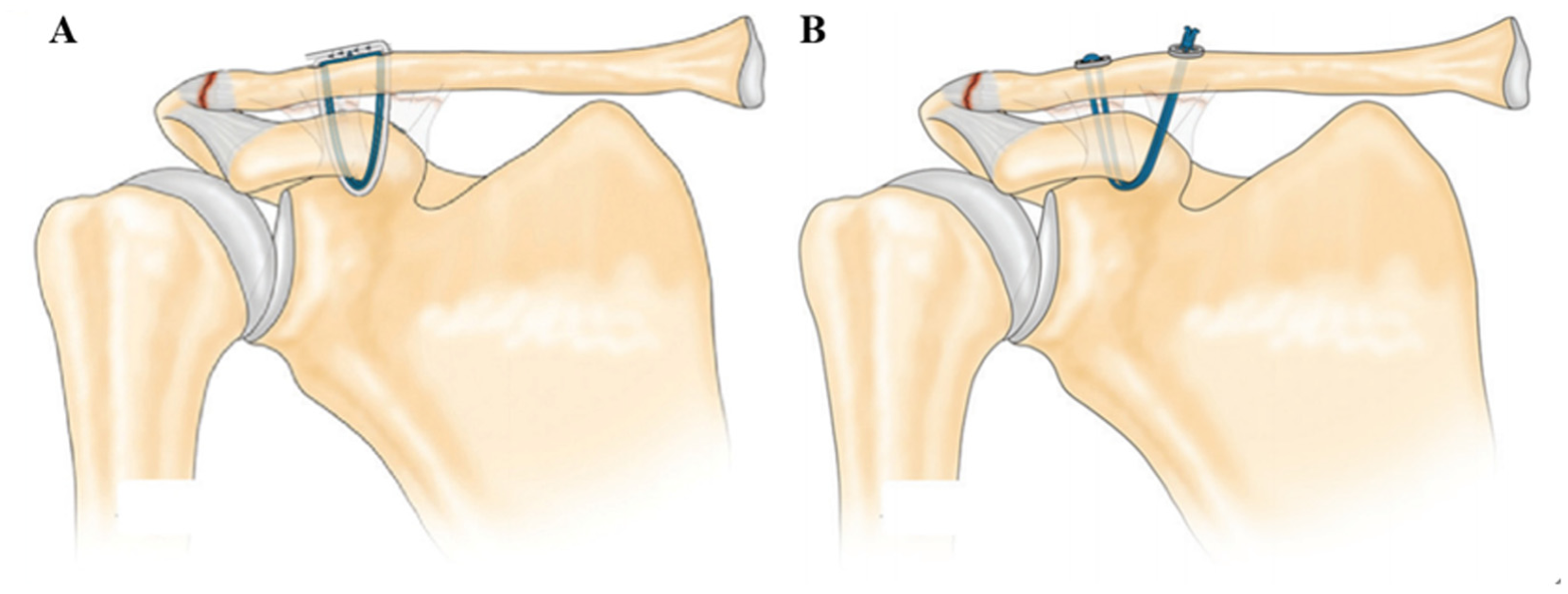
(A) Coracoclavicular sling fixation with allograft. (B) Coracoclavicular sling fixation with Tightrope. Reprinted with permission from American Journal of Sports Medicine (Li et al 22 ).
Tightrope group: a Tightrope system was loaded on the wire. The round button remained at the medial tunnel outlet, whereas the oblong button was then shuttled through the medial clavicular tunnel, beneath the coracoid, and exited through the lateral clavicular tunnel. The buttons were correctly flipped and seated on the top of the clavicle. The clavicle was pressed down to reduce the AC joint under direct visualization arthroscopically. Then the 4-strand continuous loop of No 5. FiberWire sutures (Arthrex) was tightened and tied on the superior surface of the clavicle (Figure 1B).
Finally, in both groups, the superior incision was closed in layers. Fluoroscopy was performed at this stage to confirm reduction.
Postoperative Rehabilitation
After surgery, the shoulder was protected in a sling for 6 weeks. Passive range of motion exercises started at 3 weeks postoperatively, and active range of motion exercises started at 6 weeks postoperatively. Strengthening exercises began at 3 months postoperatively. Participation in overhead or contact sports was allowed at 9 to 12 months after surgery when full range of motion and strength were restored.
Radiological Evaluation
Plain radiographs (bilateral anteroposterior view, axillary view, and lateral view) were performed preoperatively and at 3-, 6-, and 12-month follow-up (Figures 2 and 3). All radiographic measurements were done on a picture archiving and communications system (General Electric) by 2 independent investigators (a fourth-year orthopaedic resident [J.X.]) and an attending shoulder surgeon [M.Z.]). Nonweightbearing bilateral anteroposterior radiographs were used for measurements. We measured 8 parameters: (1) CC distance (CCD): shortest distance from the most inferior cortex of the clavicle to the most superior cortex of the coracoid (Figure 4), (2) total clavicular length, (3) trapezoid distance: distance between lateral end of the clavicle and center of the lateral tunnel, (4) conoid distance: distance between of lateral end of the clavicle and the center of the medial tunnel, (5) tunnel distance: distance between the center of 2 tunnels (Figure 5), (6) lateral tunnel area, (7) medial tunnel area (Figure 6), and (8) tunnel angle: the angle formed by the 2 lines connecting the centers of the medial and lateral clavicular tunnels and the midpoint of the base of the coracoid process (Figure 7). The following values were then calculated: (1) conoid ratio: conoid distance divided by total clavicular length, (2) trapezoid ratio: trapezoid distance divided by clavicular length, and (3) tunnel distance ratio: tunnel distance divided by clavicular length.12,30

Sequential radiograph films of a 24-year-old male with an acute Rockwood type 5 acromioclavicular dislocation treated with coracoid tunnel–free coracoclavicular sling fixation technique using allograft. Post-op, postoperatively.

Sequential radiograph films of a 25-year-old male with an acute Rockwood type 5 acromioclavicular dislocation treated with coracoid tunnel–free coracoclavicular sling fixation technique using Tightrope. Post-op, postoperatively.

Coracoclavicular distance (CCD) was defined as the shortest vertical distance from the most inferior cortex of the distal clavicle to the most superior cortex of the coracoid.
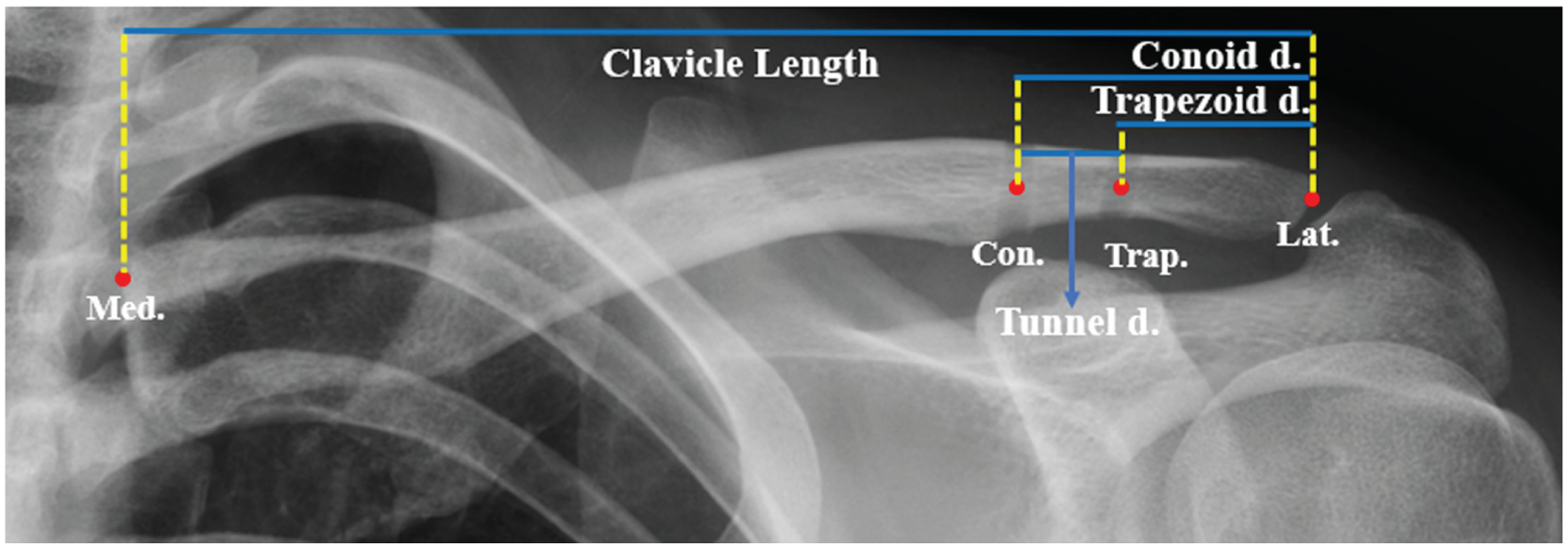
Immediately postoperative anteroposterior radiograph of a patient in the allograft group. The lateral clavicular point (Lat.) was the most lateral point, and the medial clavicular point (Med.) was the most medial point. Total clavicular length was the distance between the Lat. and Med. The trapezoid (Trap.) and conoid (Con.) points were placed in the center of the tunnel. Trapezoid distance (Trapezoid d.) was the distance between Trap. and Lat.; conoid distance (Conoid d.) was the distance between Con. and Lat.; tunnel distance (Tunnel d.) was the distance Trap. and Con.
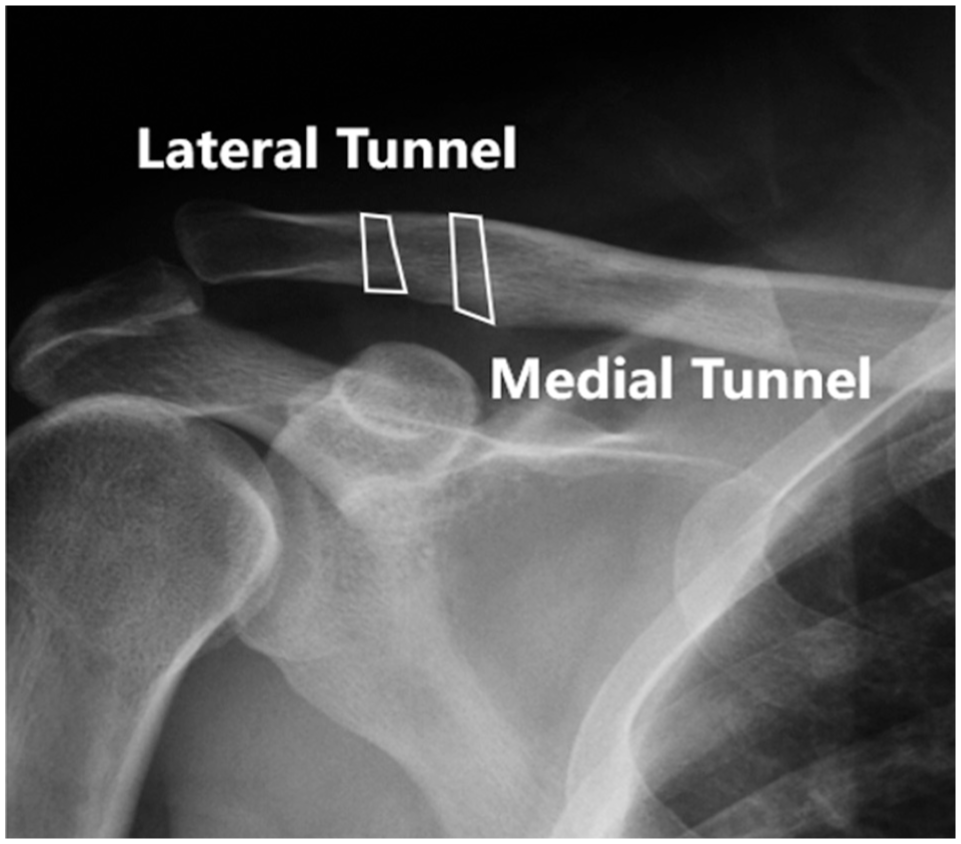
Area measurements of the medial and lateral clavicular tunnel. Immediately postoperative anteroposterior radiograph of a patient in the allograft group.

Tunnel angle was defined as the angle formed by the 2 lines connecting the centers of the medial and lateral tunnel and the midpoint of the base of the coracoid process. Immediately postoperative anteroposterior radiograph of a patient in the Tightrope group.
The reference ratio of 20% to 25% for the conoid tunnel and the upper limit of 16% for the trapezoid tunnel was selected based on a previous case series study by Eisenstein et al. 12 Given a minimum of 15 mm between the trapezoid tunnel and the lateral edge of the clavicle recommended by Mazzocca et al 23 and mean clavicular length of 139.9 mm in an anatomic study reported by Xue et al, 44 the lower limit for the trapezoid tunnel was calculated to be approximately 11% (15/139.9).
LOR (Figure 8) was defined as a >25% increase in the CCD compared with the contralateral side. 38 Other radiological findings, such as clavicular tunnel widening, clavicular/coracoid fracture, and heterotopic ossification, were also recorded (Figures 9 and 10).
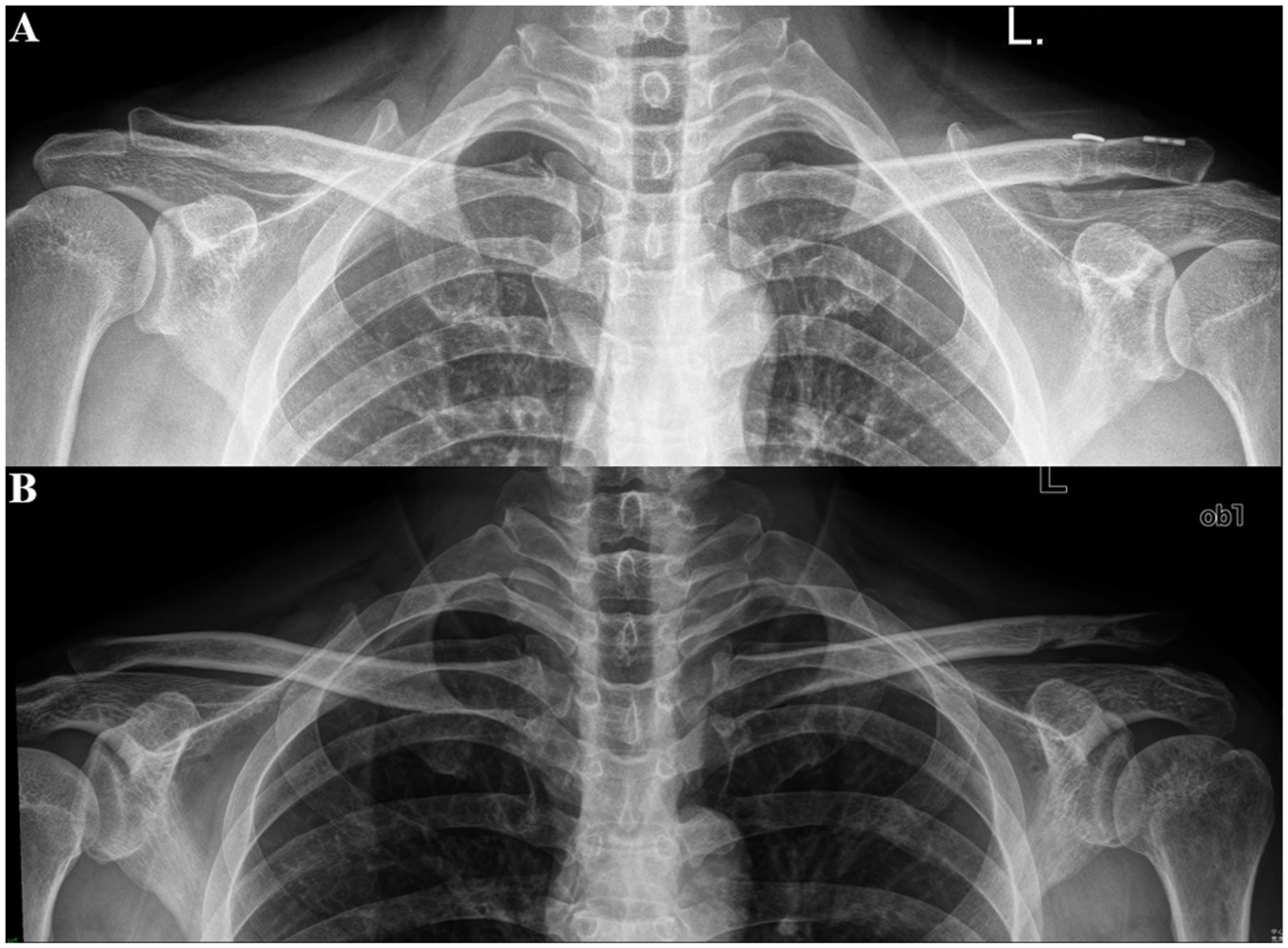
Anteroposterior radiograph at the 12-month follow-up shows loss of reduction. (A) Tightrope group. (B) Allograft group.

Anteroposterior radiographs at (A) immediate postoperative period and at (B) 12-month follow-up show medial and lateral clavicular tunnel widening.

Anteroposterior radiograph at 12-month follow-up shows heterotopic ossification (white arrow).
Clinical Evaluation
Clinical examination was performed preoperatively and at 12- and 24-month follow-ups by 2 independent shoulder surgeons (Y.Z. and F.L.) who were not involved during surgery. Functional outcomes included visual analog scale for pain, American Shoulder and Elbow Surgeons (ASES) score, Constant score, and return to sports.
Statistical Analysis
All data were analyzed with SPSS software Version 27.0 (IBM). The normality of continuous variables was assessed using the Shapiro-Wilk test. Normally distributed variables were reported as mean ± SD, whereas nonnormally distributed variables were presented as the median (25%, 75%). The χ2 test or Fisher exact test was used for categorical variables. An independent t test was used for continuous variables, while the Mann-Whitney U test was used for noncontinuous variables. A paired t test or Wilcoxon signed-rank test were applied to compare pre- and postoperative variables. Multivariate analysis was performed to determine the risk factors associated with LOR by inputting the significant variables derived from the univariate analysis. All statistical tests were 2-tailed, and a P value of < .05 was considered statistically significant. An a priori power analysis using the rate of LOR in previous studies12,22 found that to obtain 80% power, with an alpha of .05, a minimum of 17 patients for each group was required to detect a significant difference in the rate of LOR between the allograft group and the Tightrope group. The intraclass correlation coefficient (ICC) was used to assess intraobserver and interobserver reliability for radiological measurements.
Results
Patient Characteristics
All patients with acute AC dislocation underwent arthroscopic CC sling fixation with allograft before 2017 in our hospital, and with Tightrope thereafter. A total of 103 patients were initially identified, with exclusions made for chronic injury (n = 25), loss to follow-up (n = 16), concomitant shoulder pathology (n = 8), and refusal to participate (n = 4) (Figure 11).
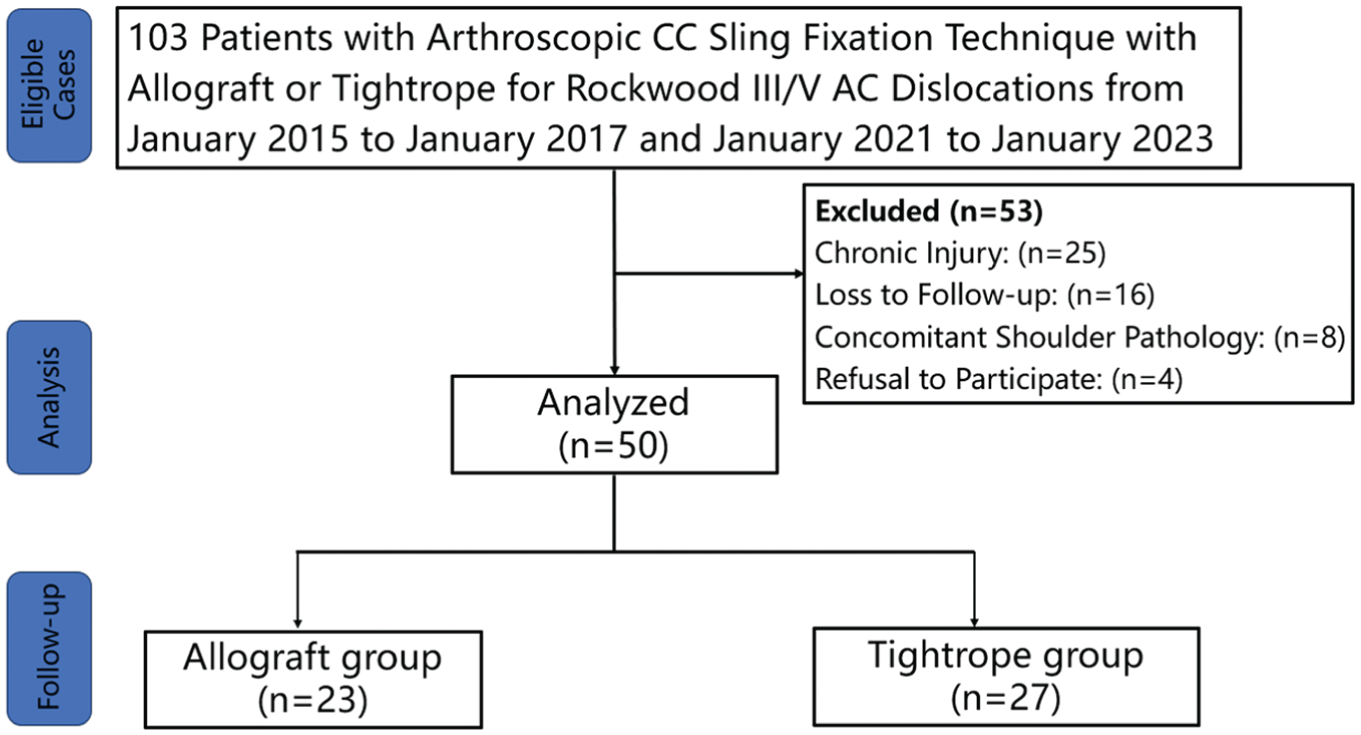
Flowchart of the study population. CC, coracoclavicular; AC, acromioclavicular.
The final study cohort consisted of 50 patients with a mean follow-up of 26.1 months. The majority of patients were male (38; 76%). The mean age of the patients at surgery was 40.82 ± 9.13 years. A total of 23 patients were in the allograft group, while 27 were in the Tightrope group. The median days to surgery were 7 (allograft group) and 8 days (Tightrope group), respectively. Surgical indications included 18 Rockwood 3 injuries and 32 Rockwood 5 injuries. No significant differences were found in baseline parameters (P > .05) (Table 1).
Preoperative and Intraoperative Findings a

Data are presented as n, mean ± SD, or median (Q1-Q3). MVA, motor vehicle accident.
Functional Outcomes
Significant improvements in all shoulder outcome scores were observed for both groups after surgery (P < .001). However, no significant intergroup differences were found in any of the shoulder outcome scores postoperatively. A total of 16 (70%) patients in the allograft group returned to sports and 22 (81%) patients in the Tightrope group returned to sports, with no significant differences between the 2 groups (Table 2).
Comparison of Clinical Outcomes a

Data are presented as n, mean ± SD, or median (Q1-Q3). Bold P values indicate statistical significance (P < .05). ASES, American Shoulder and Elbow Surgeons; Postop, postoperative; Preop, preoperative; VAS, visual analog scale.
Radiological Outcomes
CC Distance
Comparing the preoperative and postoperative CCDs, significant improvements were found in both groups (P < .05). Regarding intragroup differences, a significant increase in CCD was observed between each consecutive follow-up time point for both groups (P < .05), except when comparing the CCD measured immediately after surgery and at the 3-month follow-up in the Tightrope group (P = .13). In terms of intergroup differences, all the postoperative CCDs were significantly higher in the allograft group (P < .001) (Table 3).
Comparison of Radiological Outcomes a

Data are presented as n or mean ± SD. Bold P values indicate statistical significance (P < .05). CCD, coracoclavicular distance; postop, postoperative; preop, preoperative.
Significant difference from preop level.
Significant difference from immediately postop level.
Significant difference from 3-month postop level.
Significant difference from 6-month postop level.
Loss of Reduction
In the allograft group, a total of 10 (43%) patients experienced LOR with 6 cases identified at 3-month follow-up, 2 cases at 6-month follow-up, and 2 cases at 12-month follow-up. In the Tightrope group, 4 (15%) patients experienced LOR, with 1 case identified at 3-month follow-up and the rest at 12-month follow-up. Patients in the allograft group had a significantly higher rate of LOR (P = .03) (Table 3).
Tunnel Widening
No significant difference was found between the 2 groups regarding the medial and lateral clavicular tunnel area measured immediately after surgery. As for intragroup difference, postoperative tunnel area demonstrated a similar trend to the postoperative CCD. Significant tunnel widening was observed between each consecutive follow-up time point for both groups, except when comparing the tunnel areas measured immediately after surgery and at the 3-month follow-up in the Tightrope group. When considering intergroup differences, medial and lateral clavicular tunnel areas were significantly larger in the allograft group at the 3-, 6-, 12-month follow-ups (P < .001). Significantly greater tunnel widening was found in the allograft group (Table 3).
Heterotopic Ossification and Other Complications
Patients in the allograft group had a significantly higher rate of heterotopic ossification compared with the Tightrope group (48% vs 11%; P = .005). None of the patients in either group experienced infection, coracoid or clavicular fractures, or postoperative stiffness (Table 3).
The intraobserver and interobserver reliabilities of the radiological measurements were excellent, with all ICCs exceeding 0.972 (P < .001) (AppendixTable A1).
Univariate and Multivariate Analysis for LOR
Allograft
Univariate analysis revealed that a trapezoid tunnel ratio of 11% to 16% was associated with a stable reduction and a lower tunnel angle was associated with LOR. However, only the trapezoid tunnel ratio (11%-16%) was the independent risk factor for LOR in the multivariate analysis using logistic regression (odds ratio, 0.033; 95% CI, 0.002-0.541; P = .017) (Tables 4 and 5).
Risk Factors for LOR in the Allograft Group a

Data are presented as n or mean ± SD. Bold P values indicate statistical significance (P < .05). LOR, loss of reduction.
Based on previous studies by Eisentein et al, 12 conoid tunnel ratio range from 0.20 to 0.25 was selected as the cutoff.
Multivariate Analysis for Loss of Reduction in the Allograft Group a

Bold P value indicates statistical significance (P < .05) OR, odds ratio.
Tightrope
When univariate analysis was performed to determine the risk factors for LOR in the Tightrope group, no variables were found to be statistically significant for LOR (Table 6).
Risk Factors for LOR in Tightrope Group a

Data are presented as n or mean ± SD. LOR, loss of reduction.
Discussion
The most important finding of this study was that coracoid tunnel–free CC sling fixation with either allograft or the Tightrope system demonstrated excellent and equal clinical outcomes without major complications. However, CC sling fixation using the Tightrope system demonstrated superior maintenance of CCD in the early postoperative stage, a significantly lower rate of LOR and heterotopic ossification, and less tunnel widening compared with the allograft technique. Additionally, this study found that malposition of the trapezoid tunnel was an independent risk factor for LOR with the allograft technique.
Significant increase in CCD from the instant postoperative period to subsequent follow-up periods is commonly reported in the literature.10,14,22 In our study, a similar phenomenon was observed with both CC sling fixation techniques using either Tightrope or allograft at the 12-month follow-up. Given that a gradual increase in CCD is likely inevitable due to progressive shoulder activity during rehabilitation and after, we tend to achieve overreduction during the surgery in an attempt to minimize the final side-to-side difference in CCD between the operated and contralateral shoulders. Interestingly, we found that CCD continually increased over time in the allograft group, whereas CCD in the Tightrope group began to increase at 3 months postoperatively. Previous studies have found that the CC sling technique with the allograft possessed inferior biomechanical properties compared with the native CC ligament, whereas the Tightrope technique demonstrated equal or even superior fixation strength to the native state. 41 Given that the patients in the allograft group exhibited a significantly higher rate of LOR, with the majority occurring within 3 months (6/10; 60%), we believe that the initial fixation strength of the allograft was inadequate to sustain allograft healing. Factors such as suture cutout, allograft elongation/rupture and loosening of the knots may contribute to the early LOR in the allograft group.5,22,35,42
Although the patients in the Tightrope group had significantly smaller CCD and lower rate of LOR at final follow-up, there were no significant differences in functional outcome scores at the final follow-up. Furthermore, no significant differences in functional outcomes were found between patients with reduction loss and those with maintained reduction within either group (AppendixTable A2). This aligns with previous clinical studies indicating that LOR is not associated with general clinical shoulder scores such as University of California Los Angeles, ASES, and Constant scores.10,22 However, persistent subluxation or dislocation of the AC joint can lead to deformity, pericapsular muscle fatigue, and scapular dyskinesia.18,37 Tauber et al 38 attributed this lack of significance to the insensitivity of the general shoulder scores in reflecting AC joint-related daily problems and recommended AC joint-specific function evaluations such as Acromialclavicular Joint Instability score and Taft score. Additionally, Çarkçı et al 7 found significantly worse ACJI scores in patients with LOR, despite similar Constant scores. Therefore, further studies with AC joint specific functional evaluations are required.
Clavicular tunnel widening is a common phenomenon, starting immediately after surgery and progressing over time.3,4,11,39 The mechanical theory of tunnel widening is based on findings from anterior cruciate ligament reconstruction, where micromotion of the graft or the suture within the tunnel leads to the windshield wiper effect. 39 Additionally, Bellmann et al 3 regarded tunnel widening as a potential marker for suture-bone friction. In our study, although both medial and lateral clavicular tunnel areas significantly increased between each consecutive follow-up time points for both techniques, the tunnel area remained stable from immediately after surgery to 3 months postoperatively in the Tightrope group. This suggested that greater micromotion within the tunnel occurred earlier in the allograft group, leading to greater extent of abrasion and an increased risk of graft/suture wear-out. The difference in clavicular tunnel widening in the early postoperative follow-up reinforces the notion that the initial fixation strength was stronger with the Tightrope technique.
Despite no significant difference in medial and lateral tunnel area between the 2 techniques immediately after surgery, significantly greater tunnel widening was observed in the allograft group at the final follow-up. The close interaction between tunnel widening and postoperative fractures was highlighted by Thangaraju et al 40 who noted that fracture lines predominately ran through the tunnel. A recent meta-analysis also revealed a significantly greater fracture rate with tendon grafts. 17 Although we did not observe any clavicular fractures in either group, patients in the allograft group may be at greater risk of fracture, particularly when subjected to direct impact on the clavicle.
Several clinical studies have shown that higher-grade AC joint dislocation, previous AC joint surgery, osteoporosis, tunnel widening, tunnel angle, and tunnel position are risk factors for LOR.3,6,32,34 Our multivariate analysis, however, revealed that only the trapezoid tunnel ratio was an independent risk factor for LOR for the allograft technique. Further stratification of our data demonstrated a significantly higher LOR rate (6/7) in patients with trapezoid tunnel ratio >0.16 (P = .003) (AppendixTable A3 and A4). Interestingly, despite no significant difference in the LOR rate, all patients (2/2) with trapezoid tunnel ratio <0.11 experienced LOR (P = .05) (AppendixTable A3). These findings suggest that trapezoid tunnel position is of significant importance for LOR.
Previous studies have confirmed that medialized trapezoid tunnel was associated with increased risk of LOR and presented comparable cutoff values for the medial trapezoid tunnel position, such as Eisenstien et al 12 (0.16) and Rojas et al 30 (0.15). However, no existing clinical studies have proven that lateralized trapezoid tunnel position contributes to LOR. Geaney et al 16 reported that bone mineral density of the cadaveric clavicles decreased from medial to lateral, with lower bone mineral density correlating with decreased load to failure and increased risk of clavicular fractures for CC reconstruction with grafts.8,24 In this regard, we believe excessively lateralized trapezoid tunnel position could also be detrimental. However, we failed to give an optimal lateral position of the trapezoid tunnel based on our findings. Given a minimum of 15 mm between the lateral tunnel and lateral edge of the clavicle recommended by Mazzocca et al 23 and a mean clavicular length of 139.9 ± 9.4 mm in an anatomic study, the lateral trapezoidal ratio was set as 0.11 in our study.8,44 Therefore, either medialized or lateralized trapezoid tunnel should be avoided during surgery. The optimal range for trapezoid tunnel ratio in our study appears to be between 0.11 and 0.16.
Heterotopic ossification in the CC space was observed in 28% of our patients (14/50), and even though some studies have listed heterotopic ossification as a complication, others do not.4,10,20,31 In our study, heterotopic ossification had no effect on functional outcomes or maintenance of reduction. Therefore, it was not considered as a complication. Interestingly, the significantly higher incidence of heterotopic ossification in the allograft group may be attributed to several factors. In the Tightrope technique, the sutures passing through the bone tunnels are relatively thin and generate minimal friction along the tunnel walls, with significant contact occurring only at the titanium button interface. In contrast, allografts have a larger diameter and remain in continuous contact with the entire bone tunnel during insertion and fixation, resulting in greater mechanical irritation to the tunnel and increased production of bone debris. Furthermore, we observed more pronounced clavicular tunnel widening in the allograft group postoperatively, suggesting greater micromotion within the tunnel. This increased micromotion may also contribute to the generation of more bone debris, thereby promoting the development of heterotopic ossification. Last, as an implanted biological material, the allograft may elicit a stronger inflammatory response, which could also play a role in the higher incidence of heterotopic ossification. 19
Limitations
This study has several limitations. First, functional outcomes were assessed using the ASES score and Constant score, rather than AC joint−specific outcome measures such as the Taft score or AC joint instability score. Second, all radiological measurements were conducted on bilateral anteroposterior radiographs. Although this is a commonly used method, it may be subject to variability because of differences in radiographic technique and patient positioning. Third, the minimum follow-up time in this study was only 24 months; longer follow-up is necessary for a more comprehensive evaluation of both techniques. Fourth, all the surgeries were performed by 2 senior surgeons, which could introduce performance bias. Fifth, the temporal sequence of transitioning from allograft to Tightrope technique may have introduced a learning curve effect, which could influence the comparability of outcomes between the 2 groups. Finally, the retrospective design and relatively small sample size present inherent weaknesses.
Conclusion
Despite similar functional outcomes, CC sling with Tightrope demonstrated superior maintenance of CCD in the early postoperative stage, a significantly lower rate of LOR and heterotopic ossification, and less tunnel widening compared with allograft. Malposition of trapezoid tunnel was an independent risk factor for LOR in the allograft group.
Footnotes
Appendix
Outcomes Analyzed by Conoid Tunnel Ratio a

| Conoid Tunnel Ratio | Failure | |||
|---|---|---|---|---|
| Allograft |
P | Tightrope |
P | |
| <0.20 | 1/1 (100) | .33 | 0/2 (0) | ≥.99 |
| 0.20-0.25 | 4/14 (28.6) | / | 2/9 (22.2) | / |
| >0.25 | 5/8 (62.5) | .19 | 2/16 (12.5) | ≥.99 |
Data are presented as n/n (%). Values are presented as number of patients with loss of reduction/total number of patients in each conoind tunnel ratio group (n/n).
Acknowledgements
Special thanks are given to Hui Yu for the schematic illustrations.
Final revision submitted June 28, 2025; accepted July 21, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study received funding from the Beijing Natural Science Foundation (Youth Program No. 7244358). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Beijing Jishuitan Hospital (202005-10-01).