
Abstract
Background:
There is limited information regarding the long-term efficacy of techniques for surgical fixation after acromioclavicular (AC) joint dislocation.
Purpose:
To evaluate the efficacy of hook plate (HP) and TightRope (TR) fixation for acute AC joint dislocations by comparing the long-term clinical and radiological patient outcomes.
Study Design:
Cohort study, Level of evidence, 3.
Methods:
This study retrospectively analyzed data from 61 patients with acute AC joint dislocation between July 2011 and November 2015. The patients were grouped according to surgical procedure: HP (n = 36) and TR (n = 25). Clinical outcomes at final follow-up were evaluated using the visual analog scale (VAS) for pain; the American Shoulder and Elbow Surgery score; the Korean Shoulder Score; and the University of California, Los Angeles (UCLA) shoulder score. Side-to-side coracoclavicular (CC) distance on radiographs, postoperative complications, and the rate of subacromial erosion in the HP group were also assessed between procedures.
Results:
The mean follow-up period was 7.0 ± 1.0 years, and there were no significant differences in pain or outcome scores between the HP and TR groups (all P > .05). Forward flexion was better in the TR group (172.6° ± 5.6°) versus the HP group (166.0° ± 10.8°; P = .002). The percentages of patients with a difference in the side-to-side CC distance of <5 mm were 83.3% and 72.0% in the HP and TR groups, respectively (P = .288). Complications were found in 2 patients in the HP group and 1 in the TR group (P ≥ .999). Subacromial erosion was observed in 41.7% of patients after HP fixation, with no difference in VAS pain scores at the final follow-up in patients with versus without subacromial erosion (P = .719).
Conclusion:
When comparing HP with TR fixation for the treatment of acute AC joint dislocations, there were no significant differences in functional outcome scores, final CC distance, or complications. Slightly better forward flexion was seen after TR fixation. Subacromial erosion occurred in 40% of patients after HP fixation, but this did not affect long-term VAS pain scores. Both surgical techniques are effective treatment options for AC joint dislocation.
Acute acromioclavicular (AC) joint dislocation is a common shoulder injury, and various surgical methods for treating the condition have been reported. 27 Among surgical treatments, the hook plate (HP) fixation technique for AC stabilization is easy and convenient to use, and it has the merit of maintaining stiffness analogous to that of the prior AC joint before injury as the result of its rigid fixation. 17 So, it is possible to curtail the patient’s immobilization period and perform early rehabilitation programs. 5 The emergence of locking plates and screws made the HP method more popular, and good results have been reported. 28 However, there are several notable disadvantages with HP fixation. First, an implant removal surgery is required for plate removal. 7 Second, HP can cause an upward pressure of the hook under the acromion, which can lead to subacromial erosion. 8 In addition, because of the design allowing the normal biomechanics of the AC joint to be sustained, the hook can move freely when the clavicle is rotated or elevated. 15 Therefore, HP may cause bony osteolysis, arthritis of the AC joint, calcification or ossification of the CC ligament, shoulder impingement, and rotator cuff damage, leading to unfavorable functional outcome results. 6,8,15,20 Although the short- to midterm functional outcomes have been studied, 2,3,12 the long-term clinical and radiological results of subacromial erosion after HP fixation remain unclear.
In contrast, suture button fixation using TightRope (TR; Arthrex) for CC stabilization can be an alternative method of treatment. TR fixation is less invasive than open procedures and does not require implant removal surgery. Furthermore, it can be used to diagnose and treat other concomitant intra-articular injuries and a straight visualization of the inferior aspect of the coracoid’s base for the arthroscopic surgery. 24 However, it also has flaws, such as a sawing effect of synthetic material because of clavicle rotation that can result in adhesive capsulitis, and since its approach is quite invasive to the coracoid base and can cause anterior subluxation of the clavicle, it can lead to a malreduction of the AC joint postoperatively. 1,10,11
It has been reported that these 2 surgical techniques have good anatomic healing of the CC ligament 9,16,21,23 ; however, a 2020 systematic review reported better functional outcomes and pain scores for suture button fixation than HP fixation. 29 In this study, we aimed to compare the long-term clinical and radiological outcomes of HP and TR fixation for AC joint dislocations. We hypothesized that TR fixation would have better functional outcome scores, better range of motion (ROM), and fewer complication rates, as compared with HP fixation in the long-term follow-up period.
Methods
Study Design
This retrospective cohort study was approved by the Ulsan University Hospital Institutional Review Board. The requirement for informed consent was waived. We retrospectively reviewed the records of 125 patients who underwent acute AC joint dislocation surgery between July 2011 and November 2015. Between July 2011 and July 2013, 60 consecutive patients underwent HP fixation (HP group), and between August 2013 and November 2015, 65 consecutive patients underwent TR fixation (TR group).
The study inclusion criteria were as follows: (1) patients with radiographically confirmed Rockwood type 3, 4, or 5 acute (<3 weeks after trauma) AC dislocation; (2) those who underwent primary treatment using open reduction and HP fixation or arthroscopic TR fixation; (3) age ≥18 years; and (4) those with a minimum postoperative follow-up period of 5 years. Excluded were patients with (1) osteoarthritis or rheumatoid arthritis around the injured shoulder, (2) postinfectious sequelae, and (4) combined injury of the affected shoulder (fracture or rotator cuff tear). Of the 125 initial patients, 27 were excluded and 37 were lost to follow-up, leaving 61 patients: 36 patients in the HP group and 25 patients in the TR group (Figure 1). The mean follow-up period of the 61 patients was 7.0 ± 1.0 years. Patient characteristics are summarized by group in Table 1. There were no significant differences between the groups.

Study flowchart of patient enrollment. AC, acromioclavicular; HP, hook plate; TR, TightRope.
Patient Characteristics According to Fixation Type a

a F, female; HP, hook plate; M, male; TR, TightRope.
Operative Technique and Rehabilitation
Both HP and TR operations were performed by a single surgeon (S.H.K.). All operations were performed within 3 weeks of trauma. Operative procedures using HP fixation were performed through an approximately 5 cm–long skin incision between the distal end of the clavicle and the AC joint. After AC joint reduction was confirmed under fluoroscopy, the HP was placed with the hook positioned under the acromion and fixed with screws onto the distal end of the clavicle. Then, the deltoid-trapezoid fascia was closed, and the wound was closed layer by layer. In the HP group, implant removal was performed at a mean of 5.2 ± 2.1 months.
TR fixation was performed under arthroscopic guidance in the beach-chair position. Standard arthroscopic portals (posterior viewing, anteroinferior, and anterolateral working portals) were used. Concomitant intra-articular pathology was inspected first, including labral injury and intra-articular rotator cuff tearing. Subsequently, the subacromial space was inspected, and a bursectomy was performed. The undersurface of the coracoid base was exposed through radiofrequency and a shaver. The constant guide (Arthrex) for TR fixation was inserted through the anterolateral portal. A 1.5-cm skin incision was made on the superior clavicle after placing the guide on the undersurface of the coracoid base. A 4-mm bone tunnel from the clavicle to the coracoid base was created using the guide. Subsequently, the TR device was inserted via a shuttle wire under arthroscopic control. TR was secured using 6 alternating half-hitch stitches on the superior clavicle. Intraoperative fluoroscopy was used to assess the reduction of AC joint. Finally, the wound was closed in layers over the clavicular buttons.
Rehabilitation involved wearing a Velpeau brace (StarMedic) for 6 weeks. The pendulum-like exercise began 2 weeks postoperatively, and the active ROM progressively advanced from 6 weeks postoperatively in both groups. After full ROM was achieved, shoulder muscle strengthening exercises were started at 3 months with a TheraBand (Hygenic). Return to sports and manual labor were permitted after 6 months.
Outcome Assessment
The ROM was measured using a goniometer. Forward flexion (FF), external rotation of the side, and internal rotation of the back were measured. Internal rotation of the back was determined at the level of the spine at which the patient’s thumb was located (1-12 thoracic vertebrae, 13-17 lumbar vertebrae, and 18 sacral vertebrae).
The functional and radiological outcomes of all enrolled patients were evaluated at 6, 12, and 24 months postoperatively and at the final follow-up. All functional outcome assessments were performed by blinded researchers. Functional outcomes were evaluated using the visual analog scale (VAS) for pain, American Shoulder and Elbow Surgery score (ASES), Korean Shoulder Score (KSS), and University of California, Los Angeles (UCLA) shoulder score. In addition, we used the minimal clinically important difference (MCID) values for the VAS pain score, ASES, and UCLA score from the existing literature 14 (VAS pain score, 1.5; ASES, 21.0; UCLA score, 6.0) and compared the percentage of patients with postoperative improvement greater than the MCID between the study groups.
Radiologic outcome assessments were performed using clavicle posterior-anterior radiography. The coracoclavicular (CC) distance, the perpendicular distance between the coracoid process’s upper border and the clavicle’s inferior cortex, was analyzed. 25 The CC distance of the injured side was divided by that of the unaffected side and was expressed as a percentage (Figure 2). At the final follow-up, subluxation of the AC joint, AC joint arthritis, CC calcification, and subacromial erosion were assessed. Two shoulder fellowship-trained surgeons reviewed all radiological outcome assessments.
Finally, postoperative complications, including subacromial erosion in the HP group, metal failure, and infection, were evaluated.

Radiograph demonstrating measurement of the coracoclavicular (CC) distance as a percentage of the injured side (a) and uninjured side (b).
Statistical Analysis
The chi-square test was used to compare categorical variables, presented as absolute values and percentages. Continuous variables were compared using the independent t test, paired t test, or Mann-Whitney U test, as applicable, and are presented as means and standard deviations. The level of significance was set at P < .05. Power analysis was performed using PASS software (Version 11; NCSS Statistical Software) to confirm that the statistical power was sufficient. Group sample sizes of 36 and 25 achieve 82% power to detect a difference of –7.6 between the mean FFs of 166.0° ± 10.8° (HP group) and 172.6° ± 5.6° (TR group), with a significance level (alpha) of .05 using a 2-sided 2-sample t test. 22 Statistical analyses were performed using SPSS (Version 17.0; SPSS).
Results
Functional Outcomes
At the final follow-up, FF was found to be significantly better in the TR group than the HP group (172.6° ± 5.6° vs 166.0° ± 10.8°, respectively; P = .002). External rotation of the side (HP group: 69.0° ± 9.9° vs TR group: 69.4° ± 3.9°; P = .962) and internal rotation of the back (HP group: 9.1° ± 2.1° vs TR group: 8.7° ± 1.2°; P = .550) did not differ significantly between the 2 groups at the final follow-up. The functional outcome scores are shown in Table 2. In both groups, all scores improved significantly between preoperatively and the final follow-up (P < .001 for all). Only the VAS pain scores at the 6-month follow-up differed significantly between groups (P = .007). There was no difference between the HP and TR groups in the percentage of patients with postoperative improvement greater than the MCID, for any outcome score (VAS pain score, 97.2% vs 100% [P ≥ .999]; ASES, 94.4% vs 100% [P = .508]; UCLA score, 91.7% vs 100% [P = .262], respectively).
Functional Outcome Results a
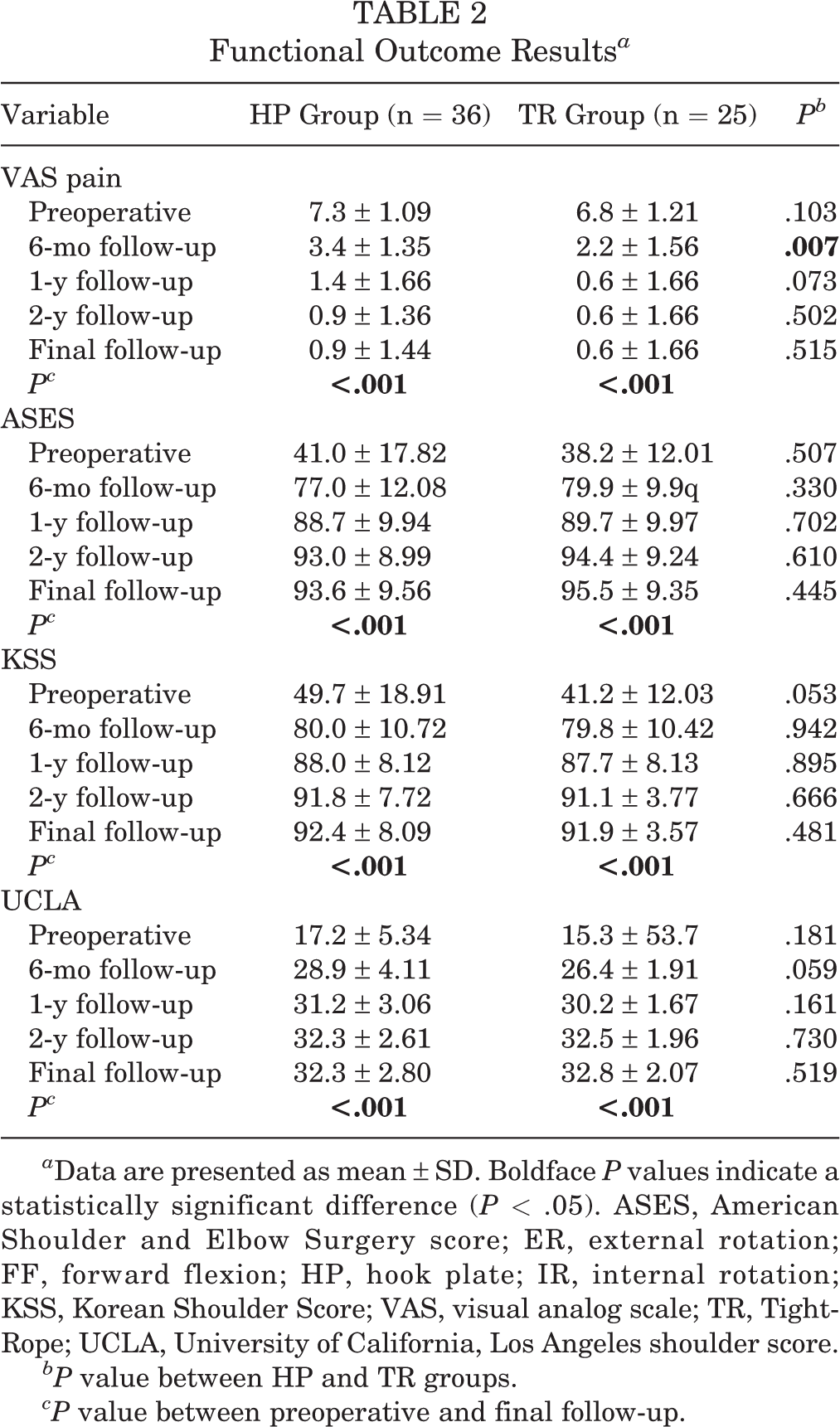
a Data are presented as mean ± SD. Boldface P values indicate a statistically significant difference (P < .05). ASES, American Shoulder and Elbow Surgery score; ER, external rotation; FF, forward flexion; HP, hook plate; IR, internal rotation; KSS, Korean Shoulder Score; VAS, visual analog scale; TR, TightRope; UCLA, University of California, Los Angeles shoulder score.
bP value between HP and TR groups.
cP value between preoperative and final follow-up.
Radiologic Outcomes and Postoperative Complications
Table 3 shows the radiologic outcomes at the final follow-up. There were no significant differences on any variable between groups. Regarding complications, subacromial erosion was present in 15 of 36 patients (41.7%) in the HP group. One patient with implant breakage and another patient with acromial fracture recovered with nonoperative treatment after implant removal. In the TR group, button migration was identified in 1 patient on the final follow-up radiograph; however, there were no symptoms. Infection was absent in both groups. Except for subacromial erosion, the overall complication rate was not statistically different between groups (HP group: 2/36 patients [5.6%] vs TR group: 1/25 patients [4%]; P ≥ .999).
Radiologic Outcomes at Final Follow-up

Data are reported as mean ± SD or n (%). AC, acromioclavicular, CC, coracoclavicular.
Subgroup Analysis According to the Rockwood Type
The subgroup analysis was performed according to the Rockwood type of AC joint dislocation. In patients with Rockwood type 3 dislocation, the TR group had significantly better FF compared with the HP group (172.8° ± 5.4° vs 165.3° ± 11.2°, respectively; P = .029); however, there were no between-group differences in the other functional outcomes or the CC distance (Appendix Table A1).
Subgroup Analysis of Subacromial Erosion in the HP Group
In the HP group, subacromial erosion was confirmed in 15 of the 36 patients (41.7%). The HP group was further classified into 2 groups according to the presence or absence of subacromial erosion. In the patients with subacromial erosion, VAS pain was significantly worse at 6 months postoperatively, immediately after implant removal (erosion: 2.65 ± 1.2 vs no erosion: 1.3 ± 0.9; P = .045). At 1 year postoperatively, the pain score was worse among patients with subacromial erosion (P = .037), but at the final follow-up, there was no significant difference in pain scores (P = .719) (Figure 3). The subacromial erosion–related changes were radiologically verified in the final follow-up; the erosion was sclerosed in 7 of 15 cases (47%), decreased in 5 of 15 cases (33%), and unchanged in 3 of 15 cases (20%) (Figure 4).

Pain visual analog scale scores in patients with (+) versus without (–) subacromial erosion in the hook plate group. VAS, visual analog scale.

Changes in subacromial erosion (arrows) in a patient from the hook plate group. (A) Two months after hook plate fixation, subacromial erosion was found. (B) After implant removal, the subacromial erosion persisted. (C) However, 7.2 years after surgery, the subacromial erosion was sclerosed.
Discussion
This retrospective study demonstrated that excellent long-term clinical results can be achieved in patients with acute AC joint dislocation undergoing either HP or TR fixation. The CC distance was improved compared with that preoperatively, without any difference between the 2 groups at the final follow-up. In particular, FF was significantly better in TR fixation than HP fixation. Subacromial erosion was seen in 41.7% of the HP group, and if there was erosion, the VAS for pain in patients with erosion was worse until 1 year postoperatively, but there was no effect on pain at the final follow-up.
Wang et al 29 performed a meta-analysis of 8 studies to compare the outcomes of suture buttons and HPs, in which 204 suture button cases and 195 HP cases were analyzed, and the follow-up period was 12 to 48 months. In their study, the short-term clinical results showed that the VAS pain and functional outcome scores were better in the suture button group, and there was no difference in complications between the 2 surgical methods. Our study had a follow-up period of 7.0 ± 1.0 years, and both the HP and TR groups showed excellent ASES, KSS, and UCLA score at the final follow-up. To our knowledge, a long-term clinical study comparing the 2 surgical methods for acute AC joint dislocation has not yet been reported. Therefore, these excellent long-term clinical results are expected to provide important information to surgeons when selecting the appropriate surgical method.
In the current study, the FF at the final follow-up was better in the TR group than the HP group (166.0° ± 10.8° vs 172.6° ± 5.6°). We guessed that the worse FF in the HP group was because of rotator cuff irritation from the hook limiting early motion. Since the difference in FF was only 7°, the clinical significance may be less important. Further research will be needed on this. Other functional outcome scores at the final follow-up were not significantly different between HP and TR fixation (Table 2, Appendix Table A1). Stein et al 26 reported that high-grade AC joint dislocation (Rockwood types 4 and 5) showed significantly better functional outcomes than double-row suture fixation. In TR group, all patients underwent single-row TR, so direct comparison of single-row versus double-row TR was not performed. Further study would be needed to determine functional outcomes in high-grade AC joint dislocation.
Single- or double-row TR fixation is an important issue in type 4 or 5 AC joint dislocation. Double-row TR provides horizontal and vertical stability compared with single-row TR. 19 Some authors argue that double-row TR is reqsuired for high-grade AC joint dislocation (Rockwood types 4 and 5). 26,30 In the present study, all patients in the TR group underwent single-row fixation of types 3, 4, and 5. We found excellent functional results from single-row TR in type 4 and 5 patients (Appendix Table A1). These results may be because of the small sample size. Further randomized comparative studies regarding the single- or double-row TR in high-grade AC joint dislocation would be needed to evaluate long-term clinical outcomes.
Recurrent AC joint dislocation after surgery is an important complication. In the present study, the CC distances at the final follow-up were 131.4% and 133.2% in the HP and TR groups, respectively. These results are worse than the CC distance of 106.1% for HP reported by Yoon et al. 31 In their study, there were no cases of subluxation, but in the present study, there were 6 (HP group) and 4 (TR group) cases of subluxation.
HP fixation can cause subacromial impingement after surgery; therefore, implant removal should be performed. 7 In addition, hook stress concentration and change in joint kinematics can cause acromial erosion and distal clavicle or acromial fracture. 4,13 Subacromial erosion after HP fixation is reported in 5.3% to 38.5% of cases. 16,18 In the present study, subacromial erosions were seen in 41.7% of cases, similar to the results of Oh et al. 18 Subacromial erosion can cause pain, but the long-term pain results have not been reported. In the present study, the VAS for pain was worse in patients with subacromial erosion from 6 months to 1 year postoperatively. However, the difference in pain decreased over time, and there was no difference in pain because of erosion at a mean follow-up of 6.8 ± 1.0 years. In addition, we first reported an imaging change in erosion itself, and it was found that erosion developed sclerosis or decreased in 80% of cases. Therefore, when performing HP fixation for AC joint dislocation, subacromial erosion may be significant in the short-term follow-up period, but the clinical significance of subacromial erosion decreases in the long-term follow-up period.
Limitations
This study has several limitations. First, it was a retrospective study with a small sample size. The study groups were not equally distributed even though the patient characteristics were not statistically different. A randomized controlled trial is needed to validate the results of the 2 surgical methods in the future. In addition, a large sample size is needed to devise a classification for subchondral bone erosion. Second, we could not explain the reasons for subluxation in either group. Third, cost analysis could not be performed for either surgical method. Fourth, there is a limit to the simple radiographic analysis of radiological changes in subacromial erosion. Erosion analysis using computed tomography can more accurately identify radiological changes. Finally, in the TR group, the reduction quality using intraoperative fluoroscopy could not be evaluated. Future studies will be needed to confirm the AC joint reduction quality using TR.
Conclusion
When comparing HP with TR fixation for the treatment of acute AC joint dislocations, there were no significant differences in functional outcome scores, final CC distance, or complications. TR fixation did result in slightly better FF. Subacromial erosion occurred in 40% of patients after HP fixation, but this did not affect long-term VAS pain scores. Therefore, both surgical methods are effective treatment options for AC joint dislocation.
Footnotes
Acknowledgment
Final revision submitted November 30, 2022; accepted January 17, 2023.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Ulsan University Hospital (reference No. 2021-03-029).