
Abstract
Background:
Failure after anterior cruciate ligament (ACL) reconstruction occurs in 3% to 30% of all patients. However, not all failures necessitate a revision surgery. Revision ACL reconstruction (ACLR) presents significant challenges for both the surgeon and the patient, and limited research has been conducted regarding long-term functional outcomes and the potential increased risk of osteoarthritis (OA).
Purpose/Hypothesis:
This study evaluates the long-term radiographic and clinical outcomes after revision ACLR compared with those of primary ACLR. It was hypothesized that revision ACLR results in a higher incidence of OA and inferior functional and patient-reported outcomes.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A retrospective follow-up compared patients with revision ACLR to a matched group of primary reconstruction (matched by sex, age, and surgery date). After a median of 9.7 years, OA was assessed using the Kellgren-Lawrence (K-L) classification.
Clinical outcome assessment included Patient-Reported Outcome Measures and knee laxity testing.
Results:
A total of 273 patients were included, 140 ACL revisions and 133 primary ACLRs. Radiographic evidence of OA (K-L grade ≥2) was present in 67% of the revision group versus 33% in the primary ACL group (P < .001). A longer time from injury to follow-up, meniscal injury, and a high body mass index (BMI) at the index surgery independently increased the odds of developing OA. Although significant improvements in knee laxity measurement were seen in both groups, these were greater in the primary reconstruction group. Improvements well above the minimal important clinical change were observed for both the International Knee Documentation Committee subjective score and the Knee Injury and Osteoarthritis Outcome scores in both groups, with a higher proportion of patients meeting the patient-acceptable symptom state in the primary group.
Conclusion:
Patients undergoing revision ACLR exhibit worse long-term functional outcomes and a higher prevalence of OA compared with patients undergoing primary ACLR. A longer time from injury to follow-up, meniscal injury, and a high BMI at the index surgery independently increased the odds of developing OA. Despite the inferior results, patients undergoing revision reconstruction experience significant improvements in both subjective scores and clinical findings, and report a high level of satisfaction.
Keywords
Failure after anterior cruciate ligament (ACL) reconstruction (ACLR) is reported to occur in 3% to 30% of all patients.7,32,49 ACL failure definitions and revision surgery indications remain debated. Because not all failures lead to revision or benefit from it, revision rates remain low, ranging from 3% to 10% of primary ACL cases.18,28,33,48 New trauma, small graft size, errors in surgical technique, younger age, high BMI, and cigarette smoking have all been identified as risk factors for failure after ACLR.5,22,31,46,48
Injury to the ACL has been shown to increase the lifetime risk of developing OA of the knee compared with that of patients with an intact ACL, 43 resulting in decreased quality of life. 3 Reconstruction of the ACL may reduce this risk compared with nonoperative treatment, although reports are conflicting1,26 and little is known about the risk for OA after revision surgery, specifically. In a 5-year follow-up cross-sectional study of patients undergoing revision ACLR, including a control group of primary ACLR, Kievit et al 25 found radiographic OA in 52% and 23% of patients, respectively. In contrast, Gifstad et al 13 only found 27% and 12% radiographic OA when comparing revision with primary reconstruction at an 8-year follow-up.
Research on medium- to long-term outcomes of ACL revision is limited, primarily consisting of small case series, with few studies including control groups for comparison. 15 Noyes et al 36 reported improvements in pain, daily activities, sports participation, and patient satisfaction within their case series of 55 revisions at a mean 33-month follow-up. Similarly, Carson et al 5 found that while revision ACL patients demonstrate improved functional and subjective outcomes, their outcomes remain inferior to those of primary ACL patients. Lind et al 30 demonstrated that while revision ACL patients achieve acceptable knee stability, they report lower outcomes, particularly in the Knee injury and Osteoarthritis Outcome Score (KOOS) subscales for sports and quality of life, compared with primary ACL patients.27,29 In a recent study from the Multicenter ACL Revision Study cohort, chondral and meniscal pathology at the time of revision was found to decrease patient-reported outcomes 6 years after revision. 16 Gifstad et al 13 based on a retrospective case-control series, concluded that revision ACL reconstructions are associated with lower KOOS, Lysholm, Tegner activity scores, and reduced muscle strength. Finally, Grassi et al, 15 who defined clinical failure as a grade C or D on the International Knee Documentation Committee (IKDC) objective score, found such failure rates ranging from 0% to 82% in a review summarizing 16 case series.
The wide range in the reported outcomes after revision ACLR demonstrates the need for more knowledge on the risk of OA development and other objective and subjective outcome measures. Such knowledge is required to conduct the shared decision-making for this large and growing group of young patients. Thus, this study aimed to investigate the long-term outcomes of a case-control study comparing patients undergoing ACL revision with a matched control group of patients who had nonrevised primary reconstructions. Our primary hypothesis was that revision ACLR patients would have a higher rate of radiographic OA compared with a matched control group at 10-year follow-up. Furthermore, we hypothesized that the revision group would also exhibit worse knee laxity and patient-reported outcome measures at the follow-up.
Methods
Patient Inclusion and Exclusion
Between July 2004 and December 2016, a total of 180 patients underwent ACL revision reconstruction at our clinic. First-time revisions, with or without concomitant meniscal surgery, minor cartilage injuries, and nonsurgically treated grades 1 or 2 medial collateral ligament injuries, were eligible for inclusion (revision group). Patients with concomitant ligament surgeries (of the posterior cruciate ligament, lateral collateral ligament, posterior lateral corner, or medial collateral ligament) at primary or previous revision surgery were excluded, as well as deceased or emigrated patients.
A control group of patients with an “uneventful” primary ACLR, which had not been revised before the inclusion, was selected from an internal quality assessment database (primary group). To account for known confounders, the patients in the primary group were matched (with the revision group) for age, sex, and date of surgery to account for changes in surgical techniques over time. If a patient in the primary group was revised later during the follow-up, they were replaced with the second-best match as a control, maintaining a 1 to 1 ratio (Figure 1).
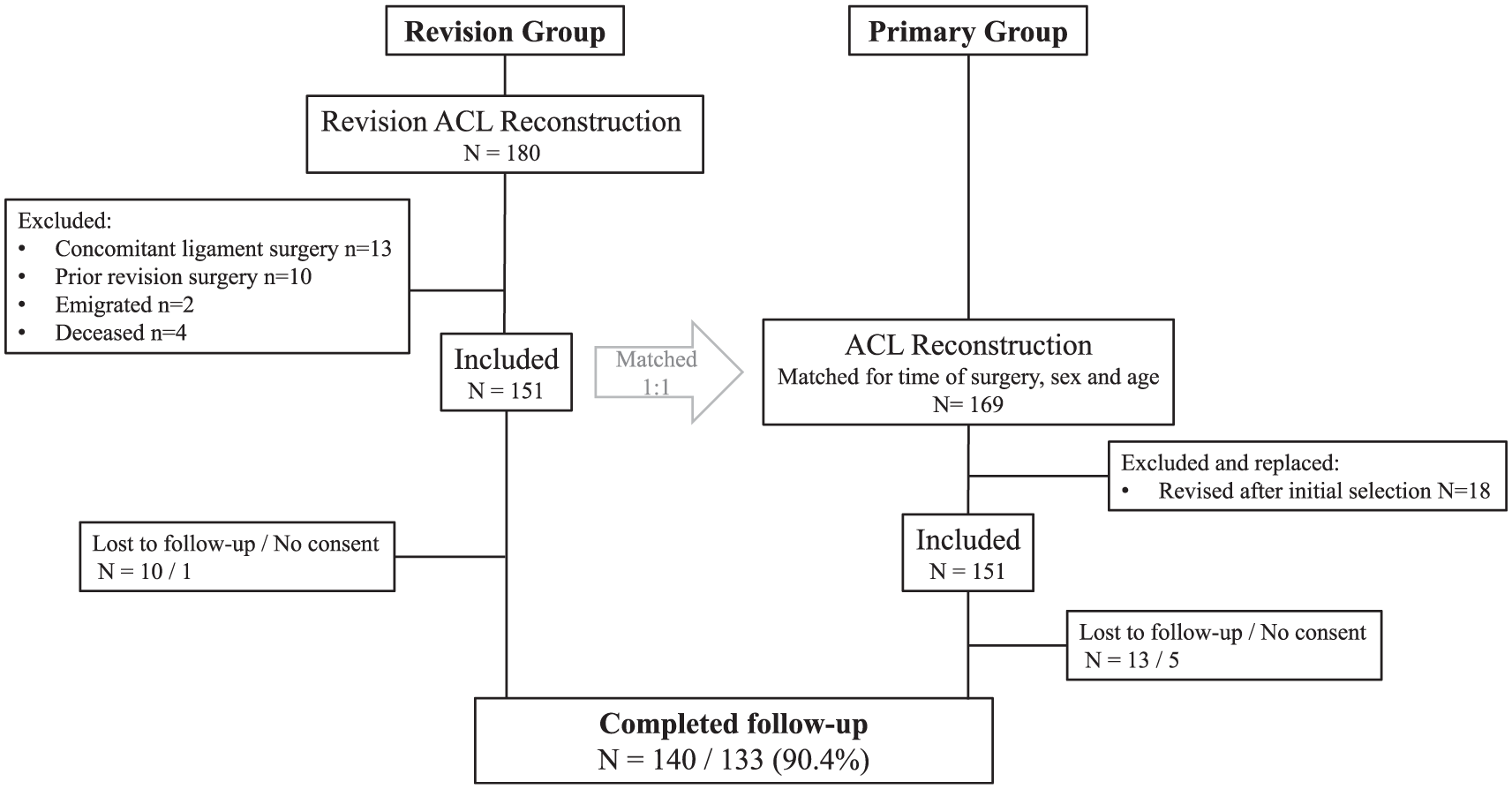
Inclusion and exclusion flowchart. ACL, anterior cruciate ligament.
The follow-up evaluation, which included a clinical examination, a radiological assessment, and the completion of the patient-reported outcome scores, was completed between November 2020 and September 2022. All patients were informed about the study and provided written consent before participation. The study was approved by the regional ethics committee (REK Vest/100644).
Surgical Technique and Rehabilitation
Revision and matched primary ACLRs were performed between June 2004 and December 2016. Therefore, variations in surgical techniques, including tunnel placement, graft choice, and fixation methods, were seen. Revision surgeries also had to account for previous procedures, taking into consideration graft selection, bone stock, and retained hardware. Surgical techniques were primarily based on what was perceived as the “gold standard” procedure at the time of surgery, and to a lesser degree, individualized based on patient characteristics. All surgeries included in the study were performed or supervised by experienced surgeons specializing in knee ligament surgery. In some cases, the same surgeon was involved in both primary and revision cases.
The rehabilitation protocol recommended crutches for partial weightbearing on the operated leg for the first 2 to 6 weeks, while still allowing free range of motion (ROM) exercises. Patients with concomitant meniscal repair in both groups were recommended partial weightbearing for 6 weeks and ROM restricted to 0° to 90°. Rehabilitation supervised by a physical therapist in an outpatient clinic for the first 6 to 9 months was recommended for all patients. A standardized follow-up included visits with both a physical therapist and a knee surgeon at the surgical clinic. All patients were offered functional testing, including a hop test and an isokinetic strength test, 9 to 12 months after surgery, and were advised accordingly regarding their return to sports based on the results.
Radiographic Assessment
Standardized bilateral weightbearing radiographs, using a Synaflexer positioning frame (BioClinica (formerly Synarc Inc), were obtained at the follow-up evaluation. The patients’ knees were placed in 45° of flexion in the frame, with a 15° craniocaudal radiographic beam for a posteroanterior view of the tibiofemoral joint. A lateral view of both knees in maximum extension was also obtained. The radiographs were evaluated by an experienced musculoskeletal radiologist (A.P.P.). Intra- and interrater reliability were established using Cohen's weighted Kappa, with at least a 6-week interval between evaluations. Interrater reliability was established by a second radiologist (I.M.B.A.). Both inter- and intrarater assessments were performed using 50 randomly selected radiographs (100 knees) from the same dataset. Both radiologists were blinded to previous evaluations. Radiographic OA was graded using the Kellgren-Lawrence (K-L) classification, 23 with OA defined as grade ≥2 for analysis.
Clinical Evaluation
At the final follow-up, all patients were examined by an independent, experienced knee surgeon (S.V.). Evaluation of knee laxity included arthrometer measures (KT-1000; MEDmetric), Lachman test, and pivot-shift testing. The maximum manual side-to-side difference between the injured and normal knees was used for the analysis of the arthrometer testing and recorded in millimeters mm). 8 The Lachman test 45 was graded according to the IKDC classification as normal, <3 mm; nearly normal, 3 to 5 mm; abnormal, 6 to 10 mm; and severely abnormal, >10 mm. 17 Anterolateral rotational instability was assessed using the pivot-shift test 11 and graded as 0, negative; 1+, glide; 2+, clunk; or 3+, gross, or as “guarding” if muscular tension prevented proper classification.
Patient-Reported Outcomes
Patient-reported outcome measures were obtained from the patients’ medical records immediately before the index surgery and reassessed before the final follow-up. The KOOS 39 was used. A KOOS quality of life subscale <44 is considered indicative of failure after ACLR. 10 A change of 8 to 10 points in the subscale is regarded as the minimal perceptible clinical improvement. 39 The International Knee Documentation Committee Subjective Knee evaluation Form (IKDC-SKF), 19 was collected before the index surgery for patients included after November 2006 (82%), and for all patients at the final follow-up. A score of ≥76.2 has been suggested as a patient-acceptable symptom state at 10 years after ACLR. 47 The Tegner activity scale 44 was used to assess the ability to perform sport- and work-related activity. Patient satisfaction with the current knee function was graded using a 5-point Likert scale 21 as either Excellent, Good, Satisfactory, Less good, or Poor.
Variables and Statistical Analyses
All statistical analyses were performed using IBM SPSS Statistics Version 29.0 (IBM Corp). An a priori P value of .05 was used to denote statistical significance. As measures of central location and spread of data, the mean and standard deviation, or the median and interquartile range, were used. Normality of continuous variables was confirmed using quantile-quantile plots and Shapiro-Wilk tests. If normality was found, independent-samples t tests were used; if not, independent samples median tests or the Mann-Whitney U test were used. Chi-square statistics were used to test categorical variables. When testing paired categorical data, the McNemar test was used. The Cohen weighted Kappa was used to test the intra- and interrater reliability of the radiographic assessment of the degree of OA. Logistic binomial regression was used for both univariate and multivariate analysis, employing a backward stepwise model to confirm the findings.
Results
A total of 273 patients (90.4%) participated in the follow-up. Eleven completed only an electronic questionnaire and a telephone interview. A total of 29 were unavailable for radiographic evaluation (n = 23), did not consent to radiographs (n = 2), or had undergone knee replacement surgery (n = 4). These patients were evenly distributed between groups; however, all knee replacements occurred in the revision group and were classified as having OA for analysis.
No statistically significant differences were found between the revision and primary groups in terms of mean age at index surgery, sex distribution, or time from index surgery to follow-up (116.4 months [range, 91.8-163.2 months] vs 117.7 months [range, 90.9-155.7 months]). The overall median time from surgery to follow-up was 9.7 years (5.2-17.7). Across the groups, 60% of patients were females. Age at both primary injury and primary surgery was lower in the revision group (20.3 and 20.6 years, respectively) compared with the primary group (25.4 and 27.2 years, respectively). The time from injury to primary surgery was shorter in the revision group (5.9 months) than in the primary group (7.8 months). Because of the study design, the time from the primary injury to the follow-up was higher in the revision group (Table 1).
Demographic Data in Revision and Primary Groups a

Data are presented as median (IQR) or n (%). BMI, body mass index; IQR, interquartile range; NS, not significant.
Independent samples median test.
Chi-square test.
Independent samples Mann-Whitney U test.
Surgical Considerations
A total of 77 (55%) surgeries in the revision group were done as a 1-stage procedure. The remaining procedures were 2-stage revisions, with bone grafting of the graft tunnels in the first stage, followed by revision reconstruction with a new graft in the second stage. The recommended interval between the 2 stages was 6 months. Ipsilateral hamstring or patellar tendon autografts were the primary choices for both the primary and revision cases. In the revision group, a contralateral hamstring or patellar tendon autograft was used in 12 cases (8.6%), a quadriceps tendon in 3 cases (2.1%), and an allograft in 2 cases (1.4%). In 5 cases (3.6%), patients opted out of the planned reconstructive surgery after the first-stage bone grafting.
Meniscal and Cartilage Injuries
No significant difference was found in the distribution of concomitant meniscal procedures at the time of primary surgery between the groups. However, over the entire follow-up period, the revision group had a significantly higher incidence of meniscal injuries (78.8% vs 62.9%; P = .012). Additionally, the revision group had a higher incidence and severity of cartilage injuries at index surgery compared with the primary group.
Surgical Burden
The revision group had a significantly higher total mean number of surgeries on the ipsilateral knee over the follow-up period (4.1 ± 1.7) compared with the primary group (1.8 ± 1; P < .001). Before primary reconstruction, surgery was performed in 29 patients (20.7%) in the revision group, including 2 patients who had undergone multiple surgeries, and in 31 patients (23.3%) in the primary group, including 4 patients (3%) who had undergone multiple surgeries.
Between primary and revision reconstruction, 81 patients (57.9%) in the revision group underwent additional surgery, with 10 (7.1%) having ≥2 procedures. After the index surgery, 57 patients (40.7%) in the revision group underwent further surgery, with 23 (16.4%) requiring ≥2 procedures, the highest being 8 surgeries. In the primary group, 52 patients (39.1%) underwent additional surgery, with 16 patients requiring ≥2 methods (Table 2).
Surgical Details and Interoperative Findings a
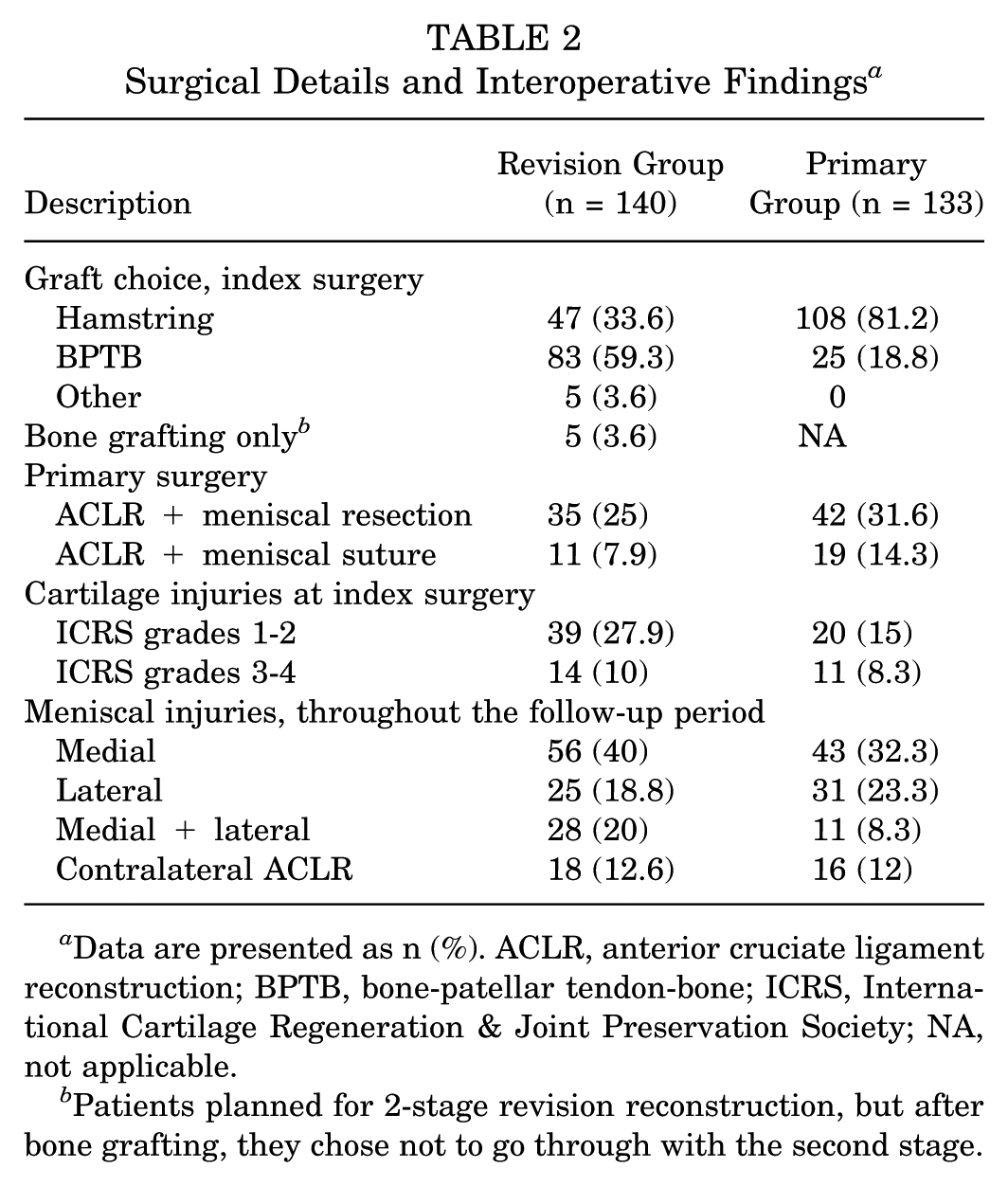
Data are presented as n (%). ACLR, anterior cruciate ligament reconstruction; BPTB, bone-patellar tendon-bone; ICRS, International Cartilage Regeneration & Joint Preservation Society; NA, not applicable.
Patients planned for 2-stage revision reconstruction, but after bone grafting, they chose not to go through with the second stage.
Additional ACL Reconstructive Surgery
A total of 34 patients (12.5%) underwent contralateral ACLR during the follow-up, including 18 (12.8%) patients in the revision group and 16 (12%) in the primary group. In the revision group, 7 patients (5%) required rerevision (a second ACL revision), and 2 (1.4%) underwent 3≥ modifications. Two patients (1.4%) underwent revision before later undergoing knee replacement, while another 2 (1.4%) patients had total knee replacement without a previous revision.
Development of OA
The intra- and inter-rater reliability tests for radiographic evaluation using the K-L classification showed substantial agreement, with weighted kappa values of 0.72 and 0.64, respectively. For radiographic OA development, the weighted kappa was 0.79 for intra-rater reliability and 0.81 for inter-rater reliability. When defining OA as a K-L grade of ≥2, the revision group had a significantly higher incidence of OA (n = 83 patients, 67%) compared with the primary group (n = 42 patients, 33%; P < .001). No significant difference was observed in the contralateral knee (revision: 13 [10%], primary: 18 [15%]), with 8 patients in each group having undergone ACLR and developed OA (Table 3).
Incidence of Radiological Osteoarthrosis Based on the Kellgren-Lawrence Classification a

Values are presented as n (%). TKA, total knee arthroplasty.
Patient-Related Factors Associated With OA
The univariate and multivariate analyses of factors associated with the development of OA at the follow-up are presented in Tables 4 and 5. In the unadjusted analysis, the time from injury to follow-up, meniscal injury, cartilage injury at index surgery, cigarette smoking, BMI at index surgery, revision surgery, and the total number of surgeries all increased the odds of developing OA at the follow-up. After adjusting for possible confounders, the multivariate analysis demonstrated that the adjusted odds ratio (OR) for time from injury to follow-up was 1.14 (95% CI, 1.06-1.22; P≤ .001), meniscal injury was 3.55 (95% CI, 1.71-7.40; P≤ .001), and BMI at index surgery was 1.14 (95% CI, 1.05-1.25; P = .003). The remaining factors no longer presented significant ORs in the adjusted analysis.
Odds Ratio for Developing Osteoarthrosis (K-L ≥2) at the Follow-up a

BMI, body mass index; K-L, Kellgren-Lawrence; OR, odds ratio.
Patients planned for 2-stage revision reconstruction, but after bone grafting, chose not to go through with the second stage.
Adjusted Multivariate Analysis of Odds Ratio for Developing Osteoarthrosis (K-L ≥2) at the Follow-up a
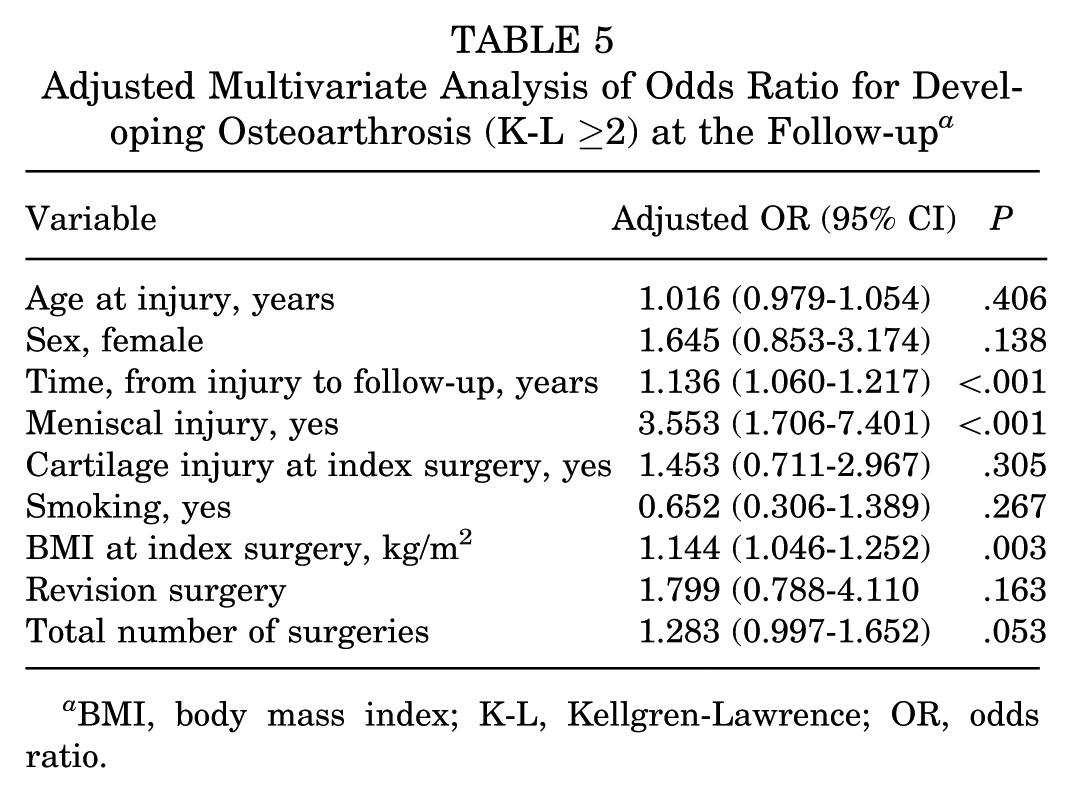
BMI, body mass index; K-L, Kellgren-Lawrence; OR, odds ratio.
Knee Laxity Evaluation at Clinical Examination
Preoperative knee laxity data were similar between the groups for KT-1000 arthrometer testing, the Lachman test, and the pivot shift test. At the follow-up, both groups showed significant improvement in knee laxity across all 3 measures, with the primary group demonstrating a greater improvement (Table 6).
Clinical Findings Before Index Surgery and at Follow-up a

Values are presented as n (%). IKDC, International Knee Documentation Committee; Preop, preoperative; STS, side-to-side.
Patients with guarding at examination were excluded from the analysis.
According to the IKDC classification.
Patient-Reported Outcomes
There was no statistically significant difference between the revision and primary groups in mean preoperative IKDC-SKF scores at the time of the index surgery. The primary group, however, had a significantly higher score at the follow-up (79.7 ± 15.4) compared with the revision group (71.7 ± 14.6) (Table 7). Furthermore, the primary group more frequently reached the Patient-Acceptable Symptom Score (PASS) value (67.7% vs 43.6%) as defined by Urhausen et al. 47 The KOOS profiles are presented in Figure 2. No differences were found in preoperative scores for the Symptoms, Pain, and Activities of Daily Living subscales; however, the revision group scored significantly lower on the Sports and Recreation and Quality of Life subscales. At the follow-up, the primary group had significantly higher KOOS scores across all 5 subscales compared with the revision group. Additionally, the primary group had a higher percentage of patients reporting satisfied or better knee function at the follow-up (85%) compared with the revision group (72.2%).
Patient-Reported Outcomes a

Data are presented as mean (SD) or n (%). IKDC-SKF, International Knee Documentation Committee Subjective Knee Evaluation Form; NS, not significant.
Independent samples t test.
Chi-square test.

The KOOS scores at the preindex surgery and at the follow-up for the revision and primary groups. Values are presented as means. The MPCI of the KOOS represents a difference of 8 to 10 points.ADL, activities of daily living; KOOS, Knee injury and Osteoarthritis Outcome Score; MPCI, minimal perceptible clinical improvement; QoL, quality of life.
Discussion
The main finding of this study was a higher incidence of radiographic OA, defined as a K-L grade of ≥2, among ACL revision reconstructions (67%) compared with “uneventful” primary ACL reconstruction (33%) at a mean of 10 years after surgery. Meniscal injury, time from injury to follow-up, and BMI at index surgery all independently increased the odds of developing radiographic OA. Both the revision and primary groups exhibited clinically significant improvements in knee stability, as measured by the Lachman test, the KT-1000 arthrometer, and the pivot-shift test. Significant improvements, well above minimal clinically important changes, were also observed in IKDC-SKF and KOOS scores for both groups. The relative improvement, both for objective and subjective outcomes, was larger in the primary group than in the revision group.
Few studies have reported on the development of OA at medium- to long-term after revision ACLR.2,13,25,35 Previous studies are small and often lack a control group. In the present study, including 140 revision and 133 primary “uneventful” (nonrevised) controls, the incidence of radiographic OA (K-L ≥2) at a 10-year follow-up was 67 % in the revision group compared with 33% in the primary group. This rate is higher than that reported by Gifstad et al, 13 who compared 56 first-time revisions with 52 uneventful primary controls at a median follow-up of 7.7 years. They found radiographic OA (K-L ≥2) in 27% of revision patients and 12% of controls. 13 Their radiographs were nonweightbearing, which may explain the lower rate of radiological OA, as joint space narrowing is central to the K-L classification. 24 Additionally, their mean follow-up time was shorter (7.5-8 years, range 2.8-13.3 years) compared with a median of 9.7 years (range, 5.2-17.7 years) in the present study.
In a smaller retrospective study, including 20 revision patients and 20 primary controls, Niki et al 35 found a higher incidence of radiographic OA in the revision group at the 3-year follow-up. However, the lesser-used Fairbanks classification cannot be directly compared with the currently applied K-L classification. Secondly, the primary surgeries leading to revision were all failed synthetic ligament reconstructions. In a cross-sectional study evaluating 25 revisions and 27 primaries at a median follow-up of 5 years, Kievit et al 25 found radiographic signs of OA in 52% of revision patients and 23% of primaries, which aligns more closely with the present study. Their shorter follow-up time could explain the lower rate of OA.
Because of the scarcity of studies on medium- to long-term follow-up after revision ACLRs, recent studies on primary reconstructions provide valuable insight. Lindanger et al, 30 in a 25-year follow-up of 235 primary reconstructions, found radiographic OA in 60% of the involved knees and 18% in the contralateral knees using the K-L classification. Similarly, in a 10- to 15-year follow-up of 210 primary reconstructions, Oiestad et al 37 found radiographic OA in 71% of the involved knees and 25% in the contralateral knees.
Overall, a higher incidence of OA appears to be found in revised cases compared with primary, uneventful ACLRs and compared with the uninjured contralateral knee. The implication is that the early onset of OA in young patients results in many years with reduced quality of life. Preventing OA development is imperative, yet limited research identifies factors contributing to OA after revision ACLR.2,40 In this study, logistic regression analysis was used to determine independent factors associated with radiographic OA. The final multivariate analysis identified 3 such factors.
First, the time from injury to follow-up showed an adjusted OR of 1.14 (95% CI, 1.06-1.22; P < .001), indicating a 14% increased risk of radiographic OA per year. This aligns with a 2018 systematic review on primary ACLRs, which found a rising incidence of posttraumatic osteoarthritis over time—21% at 10 years and 52% at 20 years after surgery. 6 Battaglia et al 2 demonstrated a correlation between time spent with an unstable knee and OA development, although without quantifying the risk. Because their study relied on retrospective medical record reviews and lacked a control group, the time with instability may not accurately reflect the total follow-up time. Their findings could support more aggressive revision surgery to minimize time with an unstable knee. However, as the present study is adjusted for revision surgery, which was not an independently significant factor for the development of OA, this relationship is less clear. Nonetheless, it underscores the importance of ACL injury prevention.
Patients with a meniscal injury at any point during the follow-up had a more than 3-fold increased risk of developing radiographic OA (adjusted OR, 3.55 [95% CI 1.71-7.40]; P <.001). In recent decades, there has been a significant shift in the diagnosis and treatment of meniscal injuries in patients with ACL injuries. Data from the Norwegian Knee Ligament Registry show a shift from 2004 to 2016, with a decrease in partial meniscus resection from 85% to 45%, and an increase in meniscal repair from 5% to 40% reflecting this change in practice. 18 This trend has continued from 2016 until the present, illustrating the communal change in the orthopaedic society embracing meniscal preservation as an important part of knee joint preservation.
In the present study, meniscal injury was diagnosed and treated concurrently with ACLR in 107 of 273 patients (39.2%), with suture repair performed in only 30 cases (11%). The low repair rate may have contributed to the high incidence of radiographic OA observed at the follow-up. This, combined with the fact that the analysis was done with meniscal injury and not partial resection or repair, highlights the importance of the meniscus for joint preservation. Meniscal repair is indisputably important in restoring knee function, together with ACLR.34,42 The increased attention to meniscal repair over resection, as well as the growing recognition of meniscal ramp lesions and posterior root tear repairs, has emerged primarily over the past decade. In our study, these procedures were only performed during the latter years of the inclusion period, which helps explain the seemingly low rates of meniscal repair. Overall, 194 out of 273 patients (71%) underwent meniscal surgery at some point during the follow-up period. Further research is needed to determine whether this shift in meniscal treatment will influence the long-term development of OA.
Lastly, high BMI at index surgery was independently associated with an increased risk of radiological OA. Each unit increase in BMI raised the risk by 14% (adjusted OR, 1.14 [95% CI 1.05-1.25]; P = .003). This aligns with findings from Brophy et al, 4 who reported an OR of 1.08 for medial OA but no significant association with lateral OA. This finding is important given the fact that BMI is a potential modifiable factor, and has been shown to increase risk of OA, 9 whereas a reduction in BMI has been shown to improve pain and function for patients with OA, 38 making it a key consideration for surgeons counseling potential revision ACL patients.
Both the revision and primary groups showed significant improvements in knee laxity from preoperative values to the follow-up. However, a substantial proportion of patients in both groups still had abnormal knee laxity. In the revision group, 52.1% had an IKDC Objective score of C or D, compared with 28% in the primary group, indicating worse outcomes than in other studies. Lind et al 29 reported a 34% rate of C or D scores at a median of 9 years, although without a control group. A meta-analysis by Grassi et al. 14 found lower rates (22% in revision, 5% in primary) but with a shorter median follow-up (2.1-6.1 years), which raises the possibility that the outcome may worsen over time.
Concomitant lateral extra-articular procedures (LEAP) have been shown in recent decades to decrease graft failure after ACLR. 12 Revision ACLR is considered an indication for this concomitant procedure, with the rationale that secondary instability over time will also affect secondary restraint, yielding a residual laxity. In the present study, anterolateral procedures were only used in the 2 most recent of the 140 revisions, and in none of the primaries. The current increasing use of LEAP may have potential future effects on outcomes after revision ACL. However, a recent study by Sørensen et al 41 was unable to find improved clinical outcomes after adding this procedure.
The present study demonstrates significant improvements in IKDC-SKF scores for both the revision and the primary groups (15.4 and 21.1), and well above the matrix-induced autologous chondrocyte implantation (MPCI) of the IKDC-SKF of 11.5. 20 However, assessing the MPCI at a group level does not account for individual variability, where some patients experience substantial improvements while others show little to no change or even deterioration. The PASS provides an alternative method for assessing change, based on patient satisfaction. While no studies specifically evaluating PASS in revision patients were identified, a recent 10-year prospective cohort study 47 on ACL tears reported a PASS threshold for the IKDC-SKF of 76.2. In this study, 43.6% of the revision group and 67.7% of the primary group reached the PASS threshold of 76.2 for the IKDC-SKF (P < .001). However, 72.2% and 85%, respectively, reported being satisfied or better with their knee function at the follow-up, suggesting that the PASS threshold may not be directly applicable to this cohort. Similar trends were observed for KOOS scores, with both groups exceeding the MCPI threshold of 8 to 10 points. Using the KOOS QoL of <44 as an indicator of ACLR failure, 29.9% of the revision group and 14.3% of the primary group met this criterion at the follow-up. 10
Satisfaction can indicate surgical success; nonetheless, it is also influenced by patient expectations and whether these expectations are set realistically. While revision patients show improvements, their outcomes are generally less favorable than those undergoing primary ACLR. Still, a large proportion report satisfaction with their knee function despite knee laxity and radiographic OA. However, 28% of the revision group were not satisfied, compared with 15% in the primary group. Future improvements in patient selection, surgical techniques—including meniscal repair and other concomitant procedures (LEAP)—as well as enhanced rehabilitation and guidance on return to sports, may lead to better outcomes.
Strengths and Limitations
A key strength of this study is the inclusion of 140 revision patients, making it one of the largest mid- to long-term evaluations of radiographic OA development after revision ACLR, with a 90% follow-up rate. The study captures a diverse and representative spectrum of revision ACL cases, likely reflecting the general population of revision patients more accurately.
The primary limitation of this study is its retrospective design. Additionally, variations in surgical methods—including graft choice, tunnel placement, meniscal treatment, and concomitant procedures—are challenging to account for in the analysis. The orthopaedic surgeon conducting follow-ups was not blinded due to practical constraints, which may introduce bias. However, because the same experienced knee surgeon (S.V.) performed all evaluations, we believe the clinical results maintain high validity.
The matching process introduced both strengths and limitations to the study. While the matched design of the primary group may create a crossover type error, potentially making the primary group appear better than expected, it also provides a comparable control group for the revision group, which is a key strength. Additionally, data on meniscal injury and treatment were recorded at the treatment level; however, information on resection size and suture type was unavailable, which may have introduced bias. Another limitation was that the radiographic evaluation was performed using only anteroposterior and lateral views—including the Merchant view—which could possibly improve the accuracy of OA assessment.
Conclusion
High rates of radiographic OA were present at a median of 10 years after revision ACLR, and significantly higher than in a group of primary uneventful controls. Meniscal injury, the time from injury to follow-up, and a higher BMI all increased the odds of OA development. Significant improvements in clinical findings and subjective scores were observed in both groups, with greater improvements in the primary reconstruction group. Despite the superior outcome of primary reconstructions, patients undergoing revision ACLR achieve substantial improvements, and most importantly, report a high level of satisfaction.
Footnotes
Final revision submitted July 5, 2025; accepted July 21, 2025.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the regional ethics committee Regional Etisk Kommitee Vest (REK Vest/100644).