
Abstract
Background:
Few researchers have examined both psychological and physical factors simultaneously in return to sport (RTS) and reinjury.
Purpose:
To assess the role of psychological profiles and physical aspects in RTS and reinjury risk and to inform and develop innovative treatment strategies that may be beneficial after anterior cruciate ligament (ACL) reconstruction.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
During the rehabilitation process, patients (aged 18-45 years) with ACL reconstruction (using patellar tendon or hamstring autografts) were screened. A statistical analysis was conducted using the cluster method and ascending hierarchical cluster analysis (Ward method), which allowed us to highlight a 4-cluster solution (P < .001). Muscle strength (maximal isokinetic strength of the quadriceps/hamstring, single-leg hop test between 3 and 6 months) and psychological factors were measured. A follow-up call was made to patients in the second year after surgery.
Results:
The study included a total of 162 athletes to determine psychological profiles. The prospective follow-up percentage for patients who responded was 75.9% regarding RTS and reinjury. Profile 1 (intermediate) was characterized by "moderate reinjury anxiety, no depression"; profile 2 (intermediate depressive) by "moderate reinjury anxiety and minor anxious-depressive reaction"; profile 3 (confident) by "no reinjury anxiety, no depression, high confidence"; and profile 4 (negative) by "high anxiety, high depression, low confidence.” The percentage of female athletes was higher in profile 4 than in profile 3 (P < .01). Profile 4 had the lowest RTS rate with 45.8% (profile 3: 77.8%; P = .01). Profile 3 had the least strength deficit (muscular quadriceps force at 90 and 240 deg/sec between profile 3 versus 1 (P = .01; P = .02), 3 versus 4 (P = .001; P = .004), and hamstring profile 3 versus 2 (P = .006). Profile 3 was associated with difference in timing to RTS between profile 3 versus 1 (P = .0004), 3 versus 4 (P = .007), and 3 versus 2 (P = .002). Profile 3, with a more quickly achieved RTS (mean = 222 days), had a higher reinjury rate at 13.9% (compared with profile 4: 0%; P = .047). Profile 3 reported all 5 cases of reinjury before return to competition. Profiles 1 and 2 with reinjuries (P = .003) suffered a strength deficit (12.9%-22.9%), primarily in the hamstrings (P = .049).
Conclusion:
Profile 3, which was the most confident and least deficient, and recovered the fastest, had the most relapses. Reinjured athletes in profiles 1 and 2 had deficits in strength, particularly in their hamstrings. Individuals in profile 4, who rarely returned to sports, were the most anxious, the most deficient, and had the greatest difficulty returning to sports.
Injury is one of the most common and frequent negative events experienced by athletes during their career. 64 However, despite a large number of studies documenting psychological reactions due to injuries, 4 recent studies have emphasized the negative emotions that arise before RTS, which are often described as reinjury anxiety. 61 Some athletes return to sport (RTS) without worry or concern about the injury, while others express high levels of anxiety about sustaining another injury. 43 Reinjury anxiety has also been described as one of the most common reactions to injuries. 22 It has also been described in terms of fear of reinjury 2 and kinesiophobia. 23
Anterior cruciate ligament (ACL) injuries are frequently accompanied by negative emotions such as general anxiety 31 and depression, 3 which are associated with a fear of reinjury. 23 In addition, stress is one of the most common psychological reactions after an injury. 30 According to the literature, there are several factors that predict the outcome of ACL reconstruction.19,26,51,52 From a psychological perspective, the ACL–Return to Sport after Injury (ACL-RSI) is the one most frequently associated with RTS.4,11 Additionally, there are associations between RTS and self-esteem, 15 emotions, 43 motivation, 26 or self-confidence. 61 According to Xu et al, 63 personality traits may have a significant effect on rehabilitation. Psychological aspects can be related to physical aspects. As a result, surgery, injury, and pain may influence kinesiophobia and reinjury. 45 According to Bandura, 7 self-esteem and motivation are more likely to have a positive influence on rehabilitation, pain reduction, and symptoms, whereas Cohen et al 16 emphasize the importance of the individual’s social support network. It is probable that all these items can explain the differences in specific evolution from one individual to another through a fluctuating, evolving psychological dynamic influenced by the physical and clinical effects of symptoms 45 such as stiffness, pain, or further loss of muscle strength. Self-esteem and optimism have been studied as psychological outcomes 19 for ACL reconstruction, and they have also been shown to be predictors of rehabilitation compliance, RTS, and self-rated knee symptoms.
In spite of the fact that many studies have examined psychological factors after ACL injury, studies do not usually take into account the relationship between psychological and functional muscle assessment with regard to RTS and recurrences.12,14,33,34,35,60 Our study aims to investigate the presence of psychological profiles among athletes with an ACL injury based on negative cognitions and emotions with a statistical method. In addition, the second goal of the study is to compare the differences between the different profiles 32 in terms of sociodemographic characteristics (age, sex, practice level, and sport type), surgery type, psychological resources (optimism, self-efficacy, and coping), and clinical evolution with pain scores, muscular strength, and hop tests. Finally, we intend to determine whether profiles (psychological and physical) can predict RTS and risk of reinjury.
Methods
The study was approved by an ethics committee. Participants in this cohort study were athletes who underwent ACL autograft reconstruction.
When athletes arrived at the rehabilitation center 3 to 6 months after surgery for physical therapy, they had been informed regarding the study and the follow-up. After the completion of questionnaire assessments and functional assessments upon inclusion, prospective follow-up began. Athletes were not selected before and had the choice to participate. After athletes gave their consent, their data were entered into a computerized database that included complete surgical and medical information as well as data related to sports. In this time, patients were excluded to provide the population for follow up. A variety of sports were analyzed according to discipline and grouped based on individual or team sports. Competitive athletes (≥1 competition during the preceding calendar year before the injury occurred) were classified as regional, national, or international, while noncompetitive athletes were classified as other athletes, such as a sports teacher, coach, or monitor.
The study included patients aged 18 to 45 years old who underwent 1 of 2 types of surgery for a first ACL reconstruction. Each of the surgeries utilized arthroscopy. The first type of surgery used a patellar tendon autograft, involving transplantation of the patellar tendon (bone–patellar tendon–bone) with a single bundle and 2 tunnels (a femoral and a tibial tunnel). 10 Interference screws were used for femoral and tibial fixation. The second type of surgery was hamstring autograft requiring 2 hamstring muscles (semitendinosus and gracilis), folded over, with a single bundle and 2 tunnels (a femoral and a tibial tunnel). 10 A single bundle consisted of 4 strands. The femoral and tibial fixations were made with Endobuttons or screws. Patients with osteotomy, bone fracture, or chondroplasty, an associated medial or lateral ligament surgery, and a history of ACL surgery or a ruptured contralateral ACL rupture were not included in the study (Figure 1).

Flowchart summarizing the study design. ACL, anterior cruciate ligament; RTS, return to sport.
Postoperative rehabilitation included knee extension and flexion exercises, quadriceps contractions against gravity, and walking without crutches from 3 to 6 weeks after surgery, based on the findings of previous publications.38,40 In accordance with the surgeon’s recommendation, a brace was worn for a period of 3 to 6 weeks. A variety of cardiovascular activities were introduced gradually, including cycling, step machines, and rowing machines. Swimming (crawl) was also introduced during this period. Following the surgeon’s recommendation, a return to running was initiated around the third or fourth month. Based on the results of the muscular and functional evaluation (limb symmetry index [LSI]), recommendations were made regarding RTS. An approval from the surgeon was required before returning to the original activity.
During the period of contact and inclusion (90-180 days after ACL reconstruction), participants completed measurements of reinjury anxiety (the Re-Injury Anxiety Inventory [RIAI]; French adaptation), 13 fear of reinjury (ACL-RSI; French adaptation 11 ), kinesiophobia (Tampa Scale of Kinesiophobia [TSK]; French adaptation 23 ), perceived stress, anxiety (Perceived Stress Scale [PSS]; French adaptation 44 ), depression (Hospital Anxiety and Depression Scale [HADS]; French adaptation 58 ), knee confidence (International Knee Documentation Committee Subjective Knee Form [IKDC Subjective] 29 ; validated in French 30 ), self-esteem (Rosenberg Self-Esteem Scale; French adaptation 59 ) optimism (Life Orientation Test–Revised [LOT-R]; French adaptation55,56), coping (Ways of Coping Checklist–Revised [WCC-R]; French adaptation 17 ), composite score of the Psychological Physical Ligament Predictive score (PPLP; validated in both French and English 40 ), and pain (visual analog scale for pain). During the inclusion phase, we also conducted muscle functional assessments (strength and jumps). The maximal isokinetic strength of the quadriceps and hamstring was assessed using a Biodex System 4 Isokinetic Dynamometer (Biodex Medical Systems, Inc). Before the muscle strength test, patients warmed up with 10 minutes of cycling, followed by 5 repetitions of the movement for warm-up purposes for each side. Following the warm-up, the muscle strength test was performed in a seated position with 90° of hip flexion and 90° of knee flexion, with the trunk fixed to the seat. 31 The test was first performed on the contralateral leg, followed by the operated leg. Three maximal effort knee flexion–extension contractions were performed at 90 deg/s, and 5 maximal effort knee flexion–extension contractions were performed at 240 deg/s with continuous verbal encouragement from a physical therapist; the peak extension torque and peak flexion torque were recorded. 40 The LSI was calculated as the ratio of the operated side to the unoperated side 47 and, to obtain a percentage, this result was multiplied by 100. In the single-leg hop test, participants stood on 1 leg behind a line representing the starting point and hopped as far as possible before landing on the same leg. If the landing was stable, the test was considered successful. 50 There was no restriction on the participant’s arm movement during the jump landing. A total of 3 practice jumps were performed by each participant, followed by 2 successful trials. Hops that were unsuccessful were defined as performing an additional hop on landing, landing with an early touchdown of the contralateral limb, and/or losing balance on landing. Upon completion of the single hop, the distance between the starting line and the point at which the back of the participant’s heel hit the ground was measured. A mean distance (cm) for each trial was recorded and LSI was calculated. 50
In the first year, patients were prospectively monitored every 2 months and were contacted by telephone the last time at the beginning of the second year to clarify the precise date of RTS and/or recurrence. There was an evaluation of the RTS (resumption of competitive matches) as well as the possibility of recurrence (with verification of the new surgery).
Statistical Analysis
Cluster analysis was used to identify different groups and classify similar members within those groups. In other words, cluster analysis is part of a geometric approach in which clusters are defined based on Euclidean distances (ie, geometric proximity in a space). 25 A cluster analysis with a 2-step procedure was performed to identify psychological profiles. 32 In the first step, z-scores were applied for the following variables: reinjury anxiety, fear of reinjury, general anxiety, depression, kinesiophobia, stress, and confidence. Then, these variables were subjected to an ascending hierarchical cluster analysis (Ward method) based on squared Euclidean distances. To identify a cluster solution, 3 criteria were considered: theoretical predictions, parsimony of the cluster solution, and power of explanation. 46 The second step consisted of an iterative k-means clustering procedure integrating barycentric coordinates of the previously chosen solution. A chi-square test was also used to investigate differences between the 4 emotional profiles by sex, age, level of sport, and type of ACL graft. In order to test the differences between profiles obtained and personality (self-esteem, optimism), coping (problem-focused, emotions-focused, and social support-seeking), and pain, we carried out analyses of variance (ANOVA) with Tukey post-hoc tests. And to analyze the differences between profiles and scores, muscular force, hop tests, reinjury, and RTS, chi-square tests were conducted. All analyses were performed with SPSS software (Version 23.0), and all P values were considered at ≤.05. Demographic data were summarized using frequencies in percentage and number of athletes. A mean and standard deviation were used for quantitative variables.
Results
Study Population
During May 2018 through November 2018, 162 athletes (excluding 8 patients) were screened for ACL autograft reconstruction (Figure 1).
A total of 74.1% (n = 120) of the athletes included underwent ACL reconstruction using hamstring tendon autograft, while 25.9% (n = 42) underwent patellar tendon autograft (Table 1). The follow-up percentage for patients who responded to the phone call to assess RTS and reinjury during the second year after the ACL reconstruction was 75.9% (n = 123).
Patient Characteristics (N = 162) a
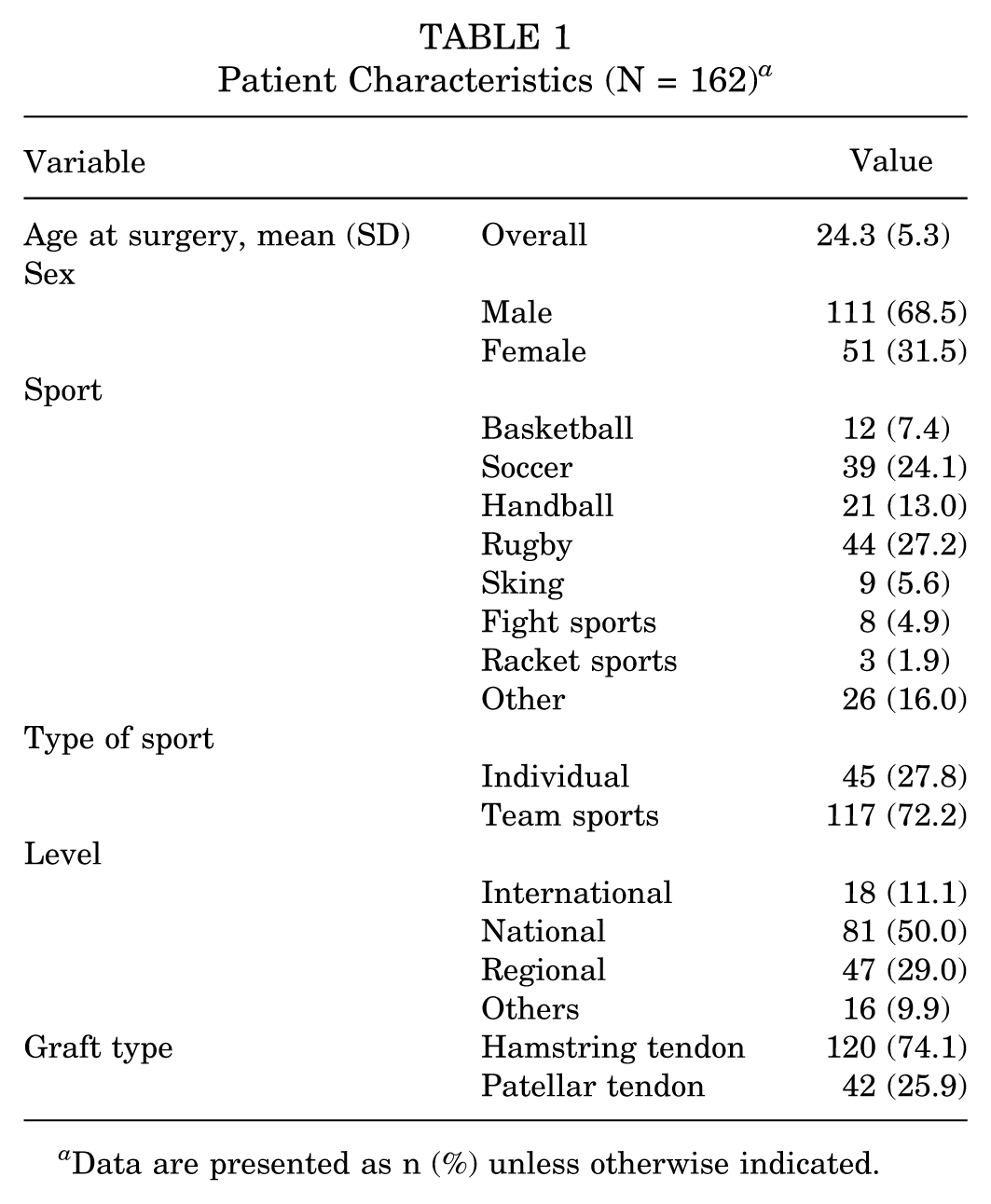
Data are presented as n (%) unless otherwise indicated.
Determining Psychological Profiles
A 2-step cluster analysis identified 4 psychological profiles. The solution explained 69.2% of the variance in reinjury anxiety, 55.7% for perceived stress, 32.7% for kinesiophobia, 56.8% for fear of reinjury, 43.7% for anxiety, 30.4% for depression, and 36.9% for confidence in the knee. A discriminant function analysis supported this final cluster solution (χ2(21) = 428.59; λ = .064; P < .001; 96.9% of cross-validated grouped cases correctly classified). The first profile (profile 1; intermediate) was characterized by intermediate scores for reinjury anxiety and fear of reinjury and low scores for kinesiophobia, stress, anxiety, depression, and knee confidence and was interpreted in terms of “moderate reinjury anxiety without depression” (Table 2). The second profile (profile 2; intermediate depressive) was characterized by intermediate levels of reinjury anxiety and fear of reinjury and medium/high levels of stress, anxiety, and depression. This profile was interpreted in terms of “moderate anxiety and minor anxiety/depressive reaction.” The third profile (profile 3; confident) was characterized by the absence of negative emotions (low reinjury anxiety and kinesiophobia, absence of fear of reinjury, low stress, anxiety, and depression and by high knee confidence). This profile was interpreted in terms of “no reinjury anxiety, no depression, great confidence." Finally, the fourth profile (profile 4; negative) was characterized by high reinjury anxiety, kinesiophobia, severe fear of reinjury, high stress, anxiety, depression, and low knee confidence.
Comparison Between Psychological Profiles With Elements of Determination Profiles a

Data are presented as mean ± SD. Bold P values indicate significant difference with p < .05. Profile 1, intermediate: moderate reinjury anxiety without depression (n = 45/162; 27.8%). Profile 2, intermediate depressive: moderate anxiety and minor anxiety/depressive reaction (n = 37/162; 22.8%). Profile 3, confident: no reinjury anxiety, no depression, great confidence (n = 50/162; 30.9%). Profile 4, negative: high anxiety, high depression, low confidence (n = 30/162; 18.5%). ACL-RSI, Anterior Cruciate Ligament–Return to Sport after Injury scale; HADS, Hospital Anxiety and Depression Scale; IKDC, International Knee Documentation Committee; PSS, Perceived Stress Scale; RIAI, Re-Injury Anxiety Inventory; TSK, Tampa Scale of Kinesiophobia.
Relationship of Psychological Profiles With Characteristics, Type of Surgery, and Psychological Resources
There were no significant differences in demographic, sport, and surgical characteristics (Table 3). Results showed a higher percentage of men in profile 3 (84%) and a lower percentage (46.7%) in profile 4 (P < .001).
Demographics of Injured Athletes and Psychological Profile (excluding elements of determination profile) a

Data are presented as n (%) or mean ± SD. Bold P values indicate significant difference with p < .05. HT, hamstring tendon; LOT-R, Life Orientation Test–Revised; PT, patellar tendon; RSES, Rosenberg Self-Esteem Scale; WCC-R, Ways of Coping Checklist–Revised.
In profiles 1 and 3, self-esteem scores were higher than in profiles 2 and 4 (P < .001). Profile 3 reported the highest optimism scores, while profiles 2 and 4 reported the lowest scores (P < .001). Profile 3 reported higher scores for problem-focused coping than all other profiles (P < .001), while profile 4 reported the highest scores for emotion-focused coping and profiles 1 and 3 the lowest (P < .001). There was no significant difference in social support seeking.
Relationship Between RTS and Psychological Profiles, Physical Evaluation (Pain, PPLP Score, Muscle Strength)
Profile 4 had the lowest RTS rates (Table 4) with 45.8% (profile 1: 85.7%, P = .001; profile 2: 75.0%, P = .03; profile 3: 77.8%, P = .01). Profiles 3 and 1 had the highest RTS rates of 77.8% and 85.7%, respectively.
Comparison Between Psychological and Physical Profiles of Injured Athletes a

Data are presented as mean or n (%) unless otherwise indicated. Bold P values indicate significant difference with p < .05. LSI, limb symmetry index; P1, Profile 1; P2, Profile 2; P3, Profile 3; P4, Profile 4; PPLP, Psychological Physical Ligament Predictive score.
In addition, profile 3 reported RTS more quickly (mean, 226 days [7.4 months]) than profile 1 (mean, 319 days [10.5 months]; P = .0004), profile 2 (mean, 270 days [8.8 months]; P = .002), and profile 4 (mean, 337 days [11 months]; P = .007).
Furthermore, profile 3 reported less pain than profile 4 (P = .02) and had the highest PPLP score (P = .006) compared with profile 1. Profile 3 had the least amount of muscular deficit. In contrast, profile 4 exhibited the greatest deficit in quadriceps (compared with profile 3: quadriceps 90 deg/s, P = .001; quadriceps 240 deg/s, P = .004). Profiles 1 and 2 were deficient in all muscle groups, with a significant difference predominating in the quadriceps for profile 1 (vs profile 3: quadriceps 90 deg/s, P = .01; quadriceps 240 deg/s, P = .02) and the hamstrings for profile 2 (vs profile 3: hamstring 90 deg/s, P = .006). In addition, the jump tests appear to be less discriminating, with no significant difference between the profiles being observed.
Relationship Between Reinjury and Psychological Profiles, Functional Evaluation (Pain, PPLP Score, Muscle Strength)
It is noteworthy that reinjury was significantly different (P = .047) between athletes in profile 3 (13.9% of reinjury) and athletes in profile 4 (0% of reinjury). Profile 3, which was more likely to RTS faster (mean, 222 days), had more reinjuries. However, in profile 3, all reinjuries (5 cases) were reported before the resumption of competition (P = .003). Profile 3 results can be categorized into 2 populations: those who relapsed before returning to competition, and those who did not relapse and returned to competition. With regard to reinjury from profiles 1 and 2, the time to RTS was intermediate with 300.7 days (Table 5). Profiles 1 and 2 also showed a tendency for a deficit in the quadriceps (from 13.7% to 22.9%) and the hamstrings (from 12.9% to 22.4%), respectively, with significant differences in both the hamstring (P = .049) and the PPLP scores (P = .03).
Comparison Between Characteristics of Reinjury in Different Profiles (profile 1 and 2 vs profile 3 in RTS function) a

Data are presented as mean or n(%). Bold P values indicate significant difference with p < .05. ACL-RSI, Anterior Cruciate Ligament–Return to Sport after Injury scale; IKDC, International Knee Documentation Committee; LSI, limb symmetry index; PPLP, Psychological Physical Ligament Predictive score; RTS, return to sport.
Discussion
A major finding of this study was that psychological profiles were associated with muscle recovery, time to RTS, and injury recurrence. We identified 4 psychological profiles that were related to their RTS capability and reinjury risk. As a result, profile 4 had high anxiety, depression, and low self-esteem, which led to more pain, significant quadriceps weakness, and low RTS. Alternatively, profile 3 had very low reinjury anxiety and no associated depressive symptoms. This profile seemed very optimistic, having the least pain and the best muscle recovery; however, they returned to sport faster with the highest reinjury rate. In profile 1, there was some concern about RTS, but there was no depressive factor associated with it. Although there may be some pain and a deficit in general muscular strength, there was no hurry to RTS (319 days), enabling the athlete to achieve the highest RTS rates with very little reinjury (5.7%). This was an ideal profile for rehabilitation as the athlete maintained an ability to follow instructions (WCC-R: focusing on the problem and listening to others. The characteristics of profile 2 “intermediate depressive” were quite similar to those of profile 1 “intermediate”, with depressive tendencies associated with it. It should be noted that profile 2 “intermediate depressive” had a faster RTS (270 days) than profile 1 “intermediate”, which was likely because of the psycological difficulties to be patient.
Furthermore, it should be noted that the differences in quadriceps force recovery between profiles 1 “intermediate” and 3 “confident”, as well as between profiles 3 “confident” and 4 “negative”, corresponded to differences in the time to RTS. Hence, the quadriceps appear to be associated with both RTS 41 and reinjury for both profiles 1 “intermediate” and 2 “intermediate depressive”. As Grindem et al, 27 found, a deficit in quadriceps strength may even be a risk factor for injury. It is possible that muscle strength contributes to recurrence in profiles 1 “intermediate” and 2 “intermediate depressive”; however, in profile 3, where muscle recovery is the best, we still observe a high rate of recurrence, which suggests that another factor may be involved in this case (such as ligamentization).
In light of these reasons, we suggest an altered approach to rehabilitation that may be useful (Figure 2). First of all, stakeholders might focus on the HADS3,58,65 instrument to assess athletes’ risk of developing anxiety and depression and to implement psychological follow-ups that are suitable for athletes in profiles 2 “intermediate depressive” and 4 “negative” (high level of anxiety and depression). As a second step, we could rely on the ACL-RSI and the IKDC Subjective 20 for better delineation of rehabilitation needs. In the event these scores are low, it could be worthwhile to look for organic causes (profile 4 “negative” and which was adapted to physical symptoms). 21 In fact, the ACL-RSI and the IKDC Subjective can be low due to pain,24,66 which indicates a problem that should be treated organically (joint, muscular, tendon pain, etc). In spite of the fact that the cause of the problem is organic, we can still provide psychological support that may enable the patient to better cope with the situation. In cases of arthrogenic motor inhibition, 53 it may be possible to provide specific treatment. It may, however, be a maladapted psychological reaction to the injury if there are no organic symptoms,5,36 more appropriately referred to as excessive, which corresponds to an individual’s prudence, 55 particularly in some female patients (profile 4, negative and excessive). For this type of profile, it could be interesting to consider that RIAI, ACL RSI and TSK, which investigate reinjury anxiety13 and kinesiophobia, 54 also provide information about risk of no RTS. 21 To provide mental preparation support, the scores of the WCC-R, self-esteem, RSES and LOT-R optimism could be beneficial to better direct advice, either with regard to goal setting or managing emotions. In contrast, a high ACL-RSI and IKDC Subjective could result in the search for excess confidence (high LOT-R and Self-Esteem, RSES, as in profile 3 “confident”). ACL-RSI scores are higher and the time to RTS is shorter among men and young people with high levels of sport.37,42 It would be prudent to defer RTS in the subgroup of men and young people of high level competence which are most of time in the profile 3 “confident”, while waiting for additional imaging studies that may provide greater clarity about the graft healing and incorporation process.18,28,49 For the other patients "intermediate" ACL-RSI and IKDC Subjective scores could represent profiles (profile 1 “intermediate” and profile 2 “intermediate depressive”) with general muscular weakness, whether on an isokinetic muscle strength deficit test 28 or jump test1,34,57 with an LSI <10% to 15%. In this case, the rehabilitation objectives would be focused on recovering the deficit; however, it would also be necessary to respect a minimal operating time based on the “risk/RTS” balance 47 (6-9 months: caution, ideally >9 months9,27,39,37,48).

Clinical use of psychological scores and physical results. 1. First time of analysis; 2. second time; 3. third time. ACL-RSI, Anterior Cruciate Ligament–Return to Sport after Injury scale; AMI, arthrogenic motor inhibition; HADS, Hospital Anxiety and Depression Scale; LOT-R, Life Orientation Test revised; LSI, limb symmetry index; PSS, Perceived Stress Scale; RIAI, Re-Injury Anxiety Inventory; RSES, Rosenberg Self-Esteem Scale; TSK, Tampa Scale of Kinesiophobia; WCC-R, Ways of Coping Checklist revised; ++, important results for recurrence risk.
According to our study, differences between men and women were associated with the psychological profile of the participants included in studies of reinjury anxiety, supporting the general statement that women are more anxious than men.6,8,62 There is a possibility that women have more cautious behavior compared with men, corresponding to profile 4 of our study, which shows a higher proportion of women than men. It is possible that these differences in reinjury rates among men and women are because of the ability of women (more in profile 4 “negative”) to react to an injury differently from men (more in profile 3 “confident”).
Beyond the use of scores, which may seem difficult and time-consuming to some clinicians, the proposed model allows for a better understanding of patient support based on the various types of profiles that we recognize very well when interacting with them.
Limitations
Because individual sports were less prevalent than team sports in this study, these results cannot be generalized to all sports. To enhance data on psychological profiles associated with an injury, studies should focus on individual sports. One of limitations of the study remains its statistical limitations; a larger sample size would have been required to control the different variables more effectively and appreciate their relationships. The fact that patients respond about RTS could limit the precision of the resumption time, but they are usually precise on the item that directly concerns them. 37 Monitoring of the patients within the first year every 2 months allowed for greater and more accurate recall and even to specify the exact date of RTS. The loss to follow-up rate (24.1%) may also be a limitation, although it is comparable with that of most studies of this nature. 38
Caution should be taken when interpreting the model because it needs to be tested on other populations of injured athletes. It is also possible that psychological support will influence an athlete’s ability to RTS in the future. Finally, if statistically it is probable that there is multicollinearity, the model contribution is more theoretical than purely explanatory if we rely on exploratory modeling by cluster analysis. 25
Conclusion
The various profiles are likely to affect the percentage of RTS and the operating time for RTS, as well as the risk of reinjury only in the case of profile 3 and 4. Quadriceps strength varies depending on the profile and time taken to RTS. Reinjury of profiles 1 and 2 is more associated with overall muscular weakness, while profile 3 does not display any muscular weakness or deficit in jumping. With regard to rehabilitation management, it will likely be necessary to moderate the patients with profile 3, mainly men, and provide psychological support to those with profile 4. Additionally, we may be able to provide psychological care for those with depressive affects (profiles 2 and 4) and develop particular rehabilitation programs "on demand" for each profile. It is also recommended that profiles 1 and 2 be strengthened muscularly while delaying RTS and rehabilitation for profile 3 pending use of tools to evaluate ligamentization quality in the decision-making process.
Footnotes
Acknowledgements
The authors thank the societies that contributed to this work: French Society of Sports Traumatology (SFTS) CERS Capbreton, Groupe Ramsay Santé and the Laboratory of Psychology from the University of Bordeaux.
Final revision submitted July 12, 2025; accepted July 26, 2025.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Comité de Protection des Personnes du Sud-Ouest et Outre-Mer 4, Limoges (CPP18-025a/2017-A03659-44).