
Abstract
Background:
The 12-item Anterior Cruciate Ligament–Return to Sport after Injury (ACL-RSI) scale was developed to assess the psychological readiness of patients to return to sports after ACL reconstruction (ACLR). A short (6-item) English version was also developed, which has shown to have good reliability and validity.
Purpose/Hypothesis:
We aimed to develop and validate a French version of the short ACL-RSI scale. We hypothesized that the same questions would remain in the selection as the English version and that the French version of the scale would have the same psychometric properties.
Study Design:
Cohort study (diagnosis); Level of evidence, 3.
Methods:
The full 12-item French ACL-RSI scale was administered to 1000 patients who had undergone ACLR surgery. Reliability (Cronbach alpha) and factor analysis of the full scale were determined. Item selection and elimination process was conducted to develop a short (6-item) version. The same methodology was used to develop the English short ACL-RSI scale. A minimal (3-item) version was also developed and assessed.
Results:
Internal consistency of the full version of the French ACL-RSI was found to be high (Cronbach alpha = .95), suggesting item redundancy. The short (6-item) version was also found to have high internal consistency (Cronbach alpha = .92) and was strongly correlated with the full version (r = 0.98). The minimal (3-item) version was also found to have high internal consistency, as well as a strong correlation with the full version (r = 0.94).
Conclusion:
The French version of the short (6-item) ACL-RSI scale was valid, discriminant, consistent, and reproducible. The minimal (3-item) version was also found to be useful and more efficient to collect the information provided by the full ACL-RSI in a French-speaking population.
An anterior cruciate ligament (ACL) tear is a common sports-related knee injury17,18 and has an important impact on return to sports (RTS). 5 Psychological readiness for RTS is important to address, should be incorporated during rehabilitation, and should be included as one of the RTS clearance criteria.3,8,23 In recent years, more attention has been paid to psychological factors after ACL reconstruction (ACLR).16,19 RTS after injury is the main goal of the treatment.
The Anterior Cruciate Ligament–Return to Sport after Injury (ACL-RSI) scale was developed in 2008 by Webster et al 22 to assess the psychological readiness of patients to RTS after ACLR. This 12-item scale evaluates 3 areas that affect a patient's ability to RTS—emotions, confidence in performance, and risk appraisal. Each item is scored from 0 to 100, and the total is divided by 12, with higher scores indicating a higher degree of readiness. It is frequently used in both research and clinical settings in English-speaking countries. 22 Also, it has been translated, cross-culturally adapted, and validated into many languages, including French by Bohu et al. 6 Poor psychological readiness has been shown to predict the risk of a second ACL injury. 6
The same authors who developed the ACL-RSI scale developed a short version (6 items), which has been shown to have good reliability and validity. 21 The main goal of this short version is to be more practical and less time-consuming without losing any inherent properties or capacities. The authors developed the short version after an item-reduction process of the full version and performed a cohort study, concluding that the short version of the ACL-RSI has psychometric proprieties equal to those of the full version. Shorter questionnaires are efficient but at risk of losing their internal consistency.
Our study aimed to develop and validate a reliable French short version (6-item version) of the ACL-RSI scale. We hypothesized that the same questions would remain in the selection as the English version and that the score would have the same psychometric properties. The minimal version (3-item version) of the scale and its influence on the psychometric properties of the test were also evaluated. This minimal version has never been tested before.
Methods
This was a prospective, single-center cohort study, with repeated evaluations 6 and 12 months after surgical ACLR during a routine follow-up consultation, including a review of sports activities and reinjuries. The study protocol received institutional review board approval.
Participants
Patients who had ACLR surgery were consecutively included to participate in the scale reduction component of the study. Patients were eligible if it was their first ACL tear. Patients were excluded if they underwent additional surgery within the first 12 months after primary reconstruction or had another medical reason for being unable to play their preinjury sport. Inclusion continued until a final number of 1000 consecutive patients was reached—672 men and 328 women, with a mean age of 29.6 ± 9.8 years. The following data were recorded for each patient: age, sex, preoperative level of sport, time to RTS, and the level and type of sport (eg, line sport, pivot, and contact-pivot). The level of sport was classified as follows: professional—if the primary income was from playing sports or if the patient played at least at the national level; competitive—if the patient had participated in competitions at the regional level at least within the previous 12 months; regular—if the patient participated at least 3 times a week with no national competition; and occasional. 11 All included patients completed the full (12-item) French version of the ACL-RSI 6 at 6 and 12 months.
A postoperative rehabilitation protocol was designed to allow patients to return to a pain-free and fully functional daily life. Early rehabilitation focused on the recovery of full active knee extension and quadriceps function as soon as possible. This protocol continued until the patient could RTS. The return to a noncontact sport was not allowed before 6 months. Return to contact sport was allowed at 9 months. Lower limb function, good control of single-leg squat jumps, jump full turn, and normal running were evaluated.
Study Protocol
A previously validated protocol was used to define and validate the French short version (6 items) and the minimal version (3 items).13,14,15,24
Item Eligibility Assessment
Before proceeding to the item selection, 30 patients (15 men and 15 women) were randomly selected among 1000 included patients and asked to rate each of the 12 items between 1 and 3 (1 = unimportant; 2 = somewhat important; 3 = very important). The mean of these ratings was known as the “relevance score”: Only items obtaining a mean of at least 2 and the ratings of at least 2 by two-thirds of the respondents were kept for the short version.14,15,24
Item Reduction and Validation Process
At least 1 question from each of the 3 ACL-RSI domains—emotions; confidence in performance; and risk appraisal—had to be included in both the short and minimal versions. Items were selected if they met the following criteria: (1) a mean response score as close as possible to 50/100; (2) the highest standard deviation; and (3) a mean relevance score of at least 2. The objective was to select items closest to the center of the response range and with the greatest variance.7,24 After selecting the items for the short and minimal versions, the correlation between the versions was evaluated.
Predictive Validation Process
After developing the 2 new versions of the scores, the results of scores for 6 months after surgery were analyzed to determine their predictive power for the actual RTS at 12 months for the 3 versions of the scale—full, short, and minimal. Two analyses were performed: (1) prediction of RTS at the same or higher level at 12 months—return vs no return at least at the same level; and (2) prediction of RTS regardless of level at 12 months—return to at least 1 sport activity versus no RTS. The objective was to try to define the sensitivity and specificity of these 2 score variants and determine whether there was a difference in predictive power between these 2 types of scores for predicting RTS and/or the level of RTS.
Statistical Analysis
All item scores were reported between 0 and 100, at increments of 10, and the mean score was reported for each item as mean ± standard deviation. Reproducibility analysis was performed using the Cronbach alpha test to look for possible redundancies in each of the analyzed versions—full, short, and minimal. The minimum acceptable value of the Cronbach alpha is 0.70, and if the value is below this number, the internal consistency is low. The maximum expected value is 0.90, and if the value is above this number, it indicates redundancy or duplication, meaning that >1 question evaluates the same element. 20 The Spearman test was used to validate the presence of a correlation between the full version and the short and minimal versions. The comparison of the final score of each version according to the level of play was analyzed as 2 × 2 using the Mann-Whitney U test. The 5% threshold was used to determine the statistical significance of the hypotheses. The statistical analysis was performed using the R software of the Sorbonne University (INSERM UMR S1136). The predictive validity of each score was assessed using receiver operating characteristic (ROC) curve statistics (ie, area under the ROC curve) and their Youden index. The ROC curves were determined, interpreted, and compared using the online software EasyROC Version 1.3.1 (EasyROC).
Results
Internal consistency of the 12-item ACL-RSI was found to be high (Cronbach alpha = .95), suggesting item redundancy. The mean ACL-RSI scores for each domain and item number for the study participants are presented in Table 1.
ACL-RSI Scores at 6 Months and Relevance Scores in the Study Cohort (N = 1000) a

The scores for each question ranged from 0 to 100. Boldface questions (including those in italics) were selected for the short (6-item) version. Questions in boldface italics were selected for the minimal (3-item) version because their means were closest to 50, with the highest standard deviations. ACL-RSI, Anterior Cruciate Ligament–Return to Sport after Injury.
Short (6-Item) Version
Three items—1, 2, and 5—from the Emotions Domain were selected for the short and minimal versions. Item number 5 was selected over item number 4 because of a higher relevance score. Of item numbers 6, 7, and 8 in the Confidence in Performance Domain (ie, confidence while playing sports), item number 7 was selected because its mean was closest to 50/100. Item numbers 9 and 10 are related to the confidence that athletes have in their ability to perform well at their sport, and of these, item number 9 was selected because it had the largest standard deviation. This item also specifically mentions returning to the preinjury level of play, which has been shown to be an important outcome after ACLR. 8 Item number 11 in the Risk Appraisal Domain was selected because its mean was closest to 50/100 and it had the better relevance score.
The short (6-item) version of the ACL-RSI was also found to have high internal consistency (Cronbach alpha = .92), suggesting that item redundancy was still present. The short (6-item) version was strongly correlated with the full 12-item version (r = 0.98).
Minimal (3-Item) Version
In the minimal version, only 1 item per domain was kept. Item numbers 5, 7, and 11 were kept because they were closest to 50/100, with large standard deviations and good relevance scores. The minimal version was also found to have a high internal consistency (Cronbach alpha = .90), suggesting that there was no redundancy (Cronbach alpha ≤ 0.90). This version of the ACL-RSI was also strongly correlated with the full 12-item version (r = 0.94).
RTS and 12-Month Prediction
The ACL-RSI score was significantly increased in all 3 ACL-RSI versions regarding RTS at any sports level (P < .001) and return at the same level as before injury (P < .001) compared with patients who did not RTS. The results of the different versions of the scale according to the level of RTS 12 months after surgery are shown in Figure 1 and Table 2.

(A) ROC curves on the prediction of return to the same sport at the same level at 1 year and (B) any sports activity at 1 year according to the different versions of the ACL-RSI completed at 6 months. ACL-RSI, Anterior Cruciate Ligament–Return to Sport after Injury; ROC, receiver operating characteristic.
Comparison of Different Versions of the ACL-RSI According to Sports Activity at 1 Year in a Consecutive Cohort (N = 1000) a

Data are reported as mean ± SD. ACL-RSI, Anterior Cruciate Ligament–Return to Sport after Injury.
P < .0001, no return versus return to inferior level.
P < .0001, no return versus return to preinjury level.
P < .0001, return to inferior level versus return to preinjury level.
With respect to return to the preinjury level of sport or higher, the ACL-RSI had a cut-off of 65/100, a sensitivity of 68%, and a specificity of 74%. The short ACL-RSI and minimal ACL-RSI versions had a cut-off of 55/100 and 70/100, respectively, with sensitivity values of 77% and 54% and specificity values of 65% and 83%, respectively. No significant difference in predictive power was found between the 3 different versions of the ACL-RSI (Table 3).
Prediction of Return to the Same Sport at the Same Level of Play at 1 Year According to Different ACL-RSI Versions a

The full ACL-RSI comprises 12 questions; the short ACL-RSI comprises 6 questions; and the minimal ACL-RSI comprises 3 questions. Dashes indicate areas not applicable. ACL-RSI, Anterior Cruciate Ligament–Return to Sport after Injury; AUC, area under the receiver operating characteristic curve.
With respect to RTS at any level, the full ACL-RSI had a sensitivity of 64% and a specificity of 77% for a cut-off of 53/100. The short ACL-RSI and minimal ACL-RSI versions had a cutoff of 48/100 and 53/100, respectively, with sensitivity values of 62% and 52% and specificity values of 78% and 83%, respectively. No significant difference in predictive power was found between the 3 different versions of the ACL-RSI (Table 4).
Prediction of Returning to at Least 1 Sport at 1 Year According to the Different Versions of the ACL-RSI a
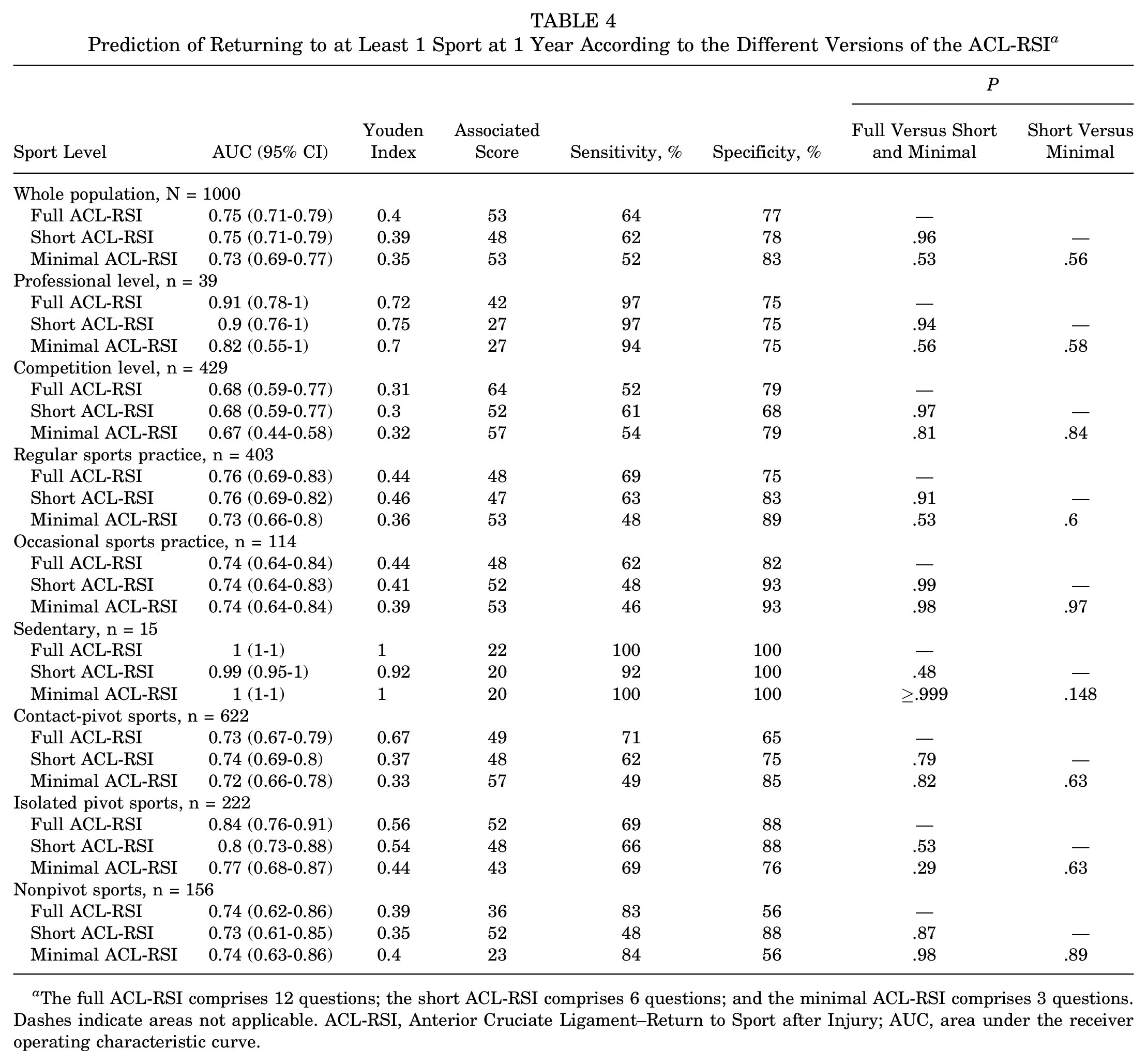
The full ACL-RSI comprises 12 questions; the short ACL-RSI comprises 6 questions; and the minimal ACL-RSI comprises 3 questions. Dashes indicate areas not applicable. ACL-RSI, Anterior Cruciate Ligament–Return to Sport after Injury; AUC, area under the receiver operating characteristic curve.
Discussion
The main result of this study was that the French version of the ACL-RSI can be shortened to a short (6-item) or even a minimal (3-item) version without losing its intrinsic qualities. Compared with the English short version, the reduction process showed that only 1 question changed.
The authors of the short version of the ACL-RSI explained that they developed this version because certain items in the long version were redundant. 21 The internal consistency of the short and minimal versions of the ACL-RSI was high and reliable, even though the scale was reduced. Similar to the full version, the short and minimal versions were also found to discriminate between athletes who did and did not RTS. The ROC curves also confirmed these properties in different versions of the ACL-RSI that were completed in 6 months for the prediction of the return to the same sport at the same level at 1 year or of any sporting activity at 1 year. A strong correlation was found between the full ACL-RSI and the short and minimal versions. Overall, the short and minimal versions were robust substitutes for the full version of the ACL-RSI.
The main characteristic of the short and minimal versions is that they reduce patient burden and save time. Patients are often asked to complete a large number of self-report outcome questionnaires. Although including a comprehensive set of outcomes is important, clinicians must decide how many and which patient-reported outcomes can be reasonably used. The ACL-RSI was recently included in a battery of tests to ensure a safe RTS after ACLR. 10 One feature of the short and minimal versions is that some knee-specific items have been removed, making the score more adaptable to other injuries on a larger scale.23,24
One systematic review showed that an athlete's readiness to RTS is mainly psychological and combines confidence in the operated knee and the lack of fear of reinjury. 9 Although it is multifactorial, psychological readiness is largely influenced by emotions and confidence. 12 Confidence is thought to be based on 2 elements: confidence in the injured body part and confidence in the ability to perform well.1,22 This item is one of the most commonly evaluated psychological factors in RTS. A systematic review published by Ardern et al 2 evaluated the psychological factors associated with RTS after injury. This study showed that motivation, confidence, and low fear were associated with an increased likelihood of returning to the preinjury level of sport. Moreover, fear was shown to be the strongest negative emotion preventing a rapid and full RTS. It has been shown that RTS was better in patients with positive psychological responses before ACLR surgery 4 and at the start of rehabilitation, suggesting that attention to both psychological and physical recovery may be justified. According to Forsdyke et al, 9 determining psychological readiness remains a challenge.
Limitations
Our study does have some limitations. First, only patients who had undergone primary ACLR were included. In previous studies, first-time injured athletes have been shown to be less confident and to find rehabilitation more stressful than those having been injured multiple times.15,22 Also, our sample included more male than female patients, which is representative of our clinical population but may not be for others.
Conclusion
The French version of the short ACL-RSI scale was valid, discriminant, consistent, and reproducible. The minimal version was also found to be useful and more efficient to collect the information provided by the full version of the ACL-RSI in a French-speaking population, and it may be considered for large-scale use to evaluate the psychological impact of RTS.
Footnotes
Final revision submitted July 11, 2023; accepted July 31, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.H. has received consulting fees from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Groupe Hospitalier Pitié-Salpêtrière.