
Abstract
Background:
Many athletes experience pubalgia. Although much is known about ligament injuries in other joints, the importance of ligament injuries in the pubic joint remains understudied.
Purpose:
To determine the frequency of an inferior pubic ligament (IPL) injury on magnetic resonance imaging (MRI) in a population of athletes with isolated pubic-related groin pain and to compare this group with a control group of athletes with adductor-related groin pain to assess the clinical relevance and association of an IPL injury with pubic-related groin pain.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Inclusion criteria consisted of athletes with pubic-related groin pain. All included participants were given a standardized questionnaire, a clinical examination, and a MRI examination of the pelvis. All MRI scans were reviewed to assess the IPL and other pubic-related pathologies, including pubic bone marrow edema and adductor injuries. The prevalence of an IPL lesion in patients with pubic-related groin pain is reported with the 95% confidence interval (95% CI). A control group with adductor-related groin pain was retrospectively included for comparison. Group characteristics were compared using the Pearson χ2 test, Fisher exact test, and Mann-Whitney-Wilcoxon test. Risk factors of IPL injury were analyzed by logistic regression.
Results:
A total of 60 athletes were included (56 male, 4 female); 18% showed definite MRI signs of IPL injury. In addition, 15% showed an equivocal IPL abnormality. This resulted in an IPL lesion prevalence of 33% (95% CI, 23%-46%) in this group. Of the 20 athletes with an IPL injury, 18 were soccer players and 2 were track and field athletes. All were men. The median age was 30 years (IQR, 26-36). The risk of IPL lesion was significantly higher in patients with trauma (odds ratio, 8.76; 95% CI, 2.56-29.91; P < .001). No IPL lesions were observed in the control group of 28 athletes with adductor-related groin pain (P < .001).
Conclusion:
On the basis of MRI analysis, there is a relatively high frequency of IPL injuries (33%) in athletes with pubic-related groin pain in addition to pubic bone and adductor pathology. No IPL injuries (0%) were observed in a control group of athletes with adductor-related groin pain. Our findings support the consideration of IPL injury in the diagnostic workup of pubic-related groin pain, particularly in posttraumatic cases. Further research is needed to refine the diagnostic process and to better understand the implications of IPL injury for rehabilitation and return-to-play outcomes.
The symphyseal and perisymphyseal area has become of increasing interest for sports physicians, orthopaedic surgeons, and radiologists dealing with complex pain syndromes in the groin area. Between 2% and 10% of all athletic injuries involve the groin, and up to 13% of soccer injuries are groin related.10,20 Evaluation and treatment of groin pain in athletes are challenging: the anatomy is complex, multiple pathologies often coexist, different pathologies may cause similar symptoms, and many systems can refer pain to the groin.
To create conformity in the confusing terminology of pubalgia, the Doha agreement was held in 2014. 21 The classification system has 3 major subheadings of groin pain in athletes: defined clinical entities for groin pain (adductor, iliopsoas, inguinal, and pubic related), hip-related groin pain, and other causes of groin pain in athletes. 21
State-of-the-art literature consists of research focusing on adductor-, inguinal-, and hip-related groin pain.4,7,10,18,20,21 As a result, most of the knowledge has been acquired of these pathologies. Despite the growing amount of research of the adductor-, inguinal-, and hip-related pathologies and their large list of differential diagnoses, no cause could be agreed on for a considerable amount of groin pain cases. Groin injuries often recur and may lead to the premature termination of athletic careers.7,10,20
However, until now, limited research has focused on pubic-related groin pain. In the clinic, we see a lot of athletes with groin pain who have specific (pinpoint) pain at the pubic symphysis, and recent anatomic studies have shown the importance of the symphysis and its ligaments in patients with pubalgia. 1 Yet, pathologies at the level of the pubic ligaments have rarely or never been investigated further.
A first case study concerning an injury of the pubic ligaments was reported in 2020. 11 Mathieu et al 11 described an injury of the inferior pubic ligament (IPL) and its association with pubalgia. This injury has received more and more attention in orthopaedic and sports medicine.11-13,15 Since then, the terminology of Mathieu syndrome was internationally agreed as an umbrella term for athletes with a lesion at the IPL who were experiencing pubic-related groin pain.11-13,15 The interest in the pubic ligaments and pubic-related groin pain has grown in sport and orthopaedic medicine ever since, and few anatomic and radiologic studies have been published focusing on the pubic ligaments, in particular the IPL.12,13,15
The pubic symphysis is an amphiarthrodial joint consisting of a fibrocartilaginous disc sandwiched between the articular surfaces of the pubic bones.1,8,9,19 The pubic joint is surrounded by 4 ligaments: the anterior pubic ligament, posterior pubic ligament, superior pubic ligament, and IPL. The 4 ligaments reinforce the pubic symphysis. The connections of the ligaments with the pubic bones have been well described.1,8,9,19 Their function is to resist tensile, shearing, and compressive forces. The pubic joint is capable of a small amount of movement under physiologic conditions in most adults (angulation, rotation, and vertical displacement).1,4,8,9,19 The IPL was reported as the strongest and most important ligament to provide stability across the symphysis.1,4,15,19 The IPL was described with a width of 25 mm in men and 35 mm in women, a thickness of 6 to 12 mm, and a mean height of 10 to 12 mm.1,15,19 The most recent reported morphometric and biomechanical data confirm a role of the IPL and superior pubic ligament in vertical joint stabilization. 15 Although the IPL is thicker than the superior pubic ligament, it is more stressed by vertical forces. Biomechanical considerations suggest that in sports (walking, running, pivoting sports) the superior anguli of the pubis bones are pressed together, while the inferior anguli of the pubic bones are pushed apart. However, the IPL is constantly under stress owing to walking, running, performing sports, and so on. It is theorized that not only may the IPL rupture in the case of acute unexpected trauma, but the ligament may also be injured by chronic overload.1,11,13,15
Despite the new proposed theory, the demographic and radiologic features of IPL lesions continue to be a subject of debate. Therefore, the purpose of this study was, first, to determine the frequency of IPL injury on magnetic resonance imaging (MRI) in a population of athletes with pubic-related groin pain and, second, to explore whether IPL injury may be specifically related to pubic-related groin pain by comparing it with adductor-related groin pain in a control group. We hypothesized that IPL injury may be prevalent and associated with pubic-related groin pain.
Methods
Overall Design and Plan of Trial
This cross-sectional observational study with an embedded case-control comparison was approved by the institutional ethics committee of the Antwerp University Hospital (UZA study registration B3002020000220) and was conducted according to the principles of the 1964 Declaration of Helsinki and its later amendments. 22
The study included athletes with a confirmed clinical diagnosis of pubic-related groin pain who were recruited between August 2020 and July 2024. All participants underwent a standardized questionnaire and clinical examination, combined with an MRI examination of the pelvis.
MRI examinations were performed on a clinical whole body 1.5T or 3T MRI scanner. All participants were imaged with a standard 2-dimensional (2D) turbo spin echo (TSE)–based protocol, including coronal and sagittal intermediate-weighted fat-suppressed, coronal T1–weighted image (WI), and axial T2-WI acquisitions. Coronal and axial oblique sequences oriented about the long axis of the symphysis were also obtained in which the IPL was clearly visualized (Figure 1).
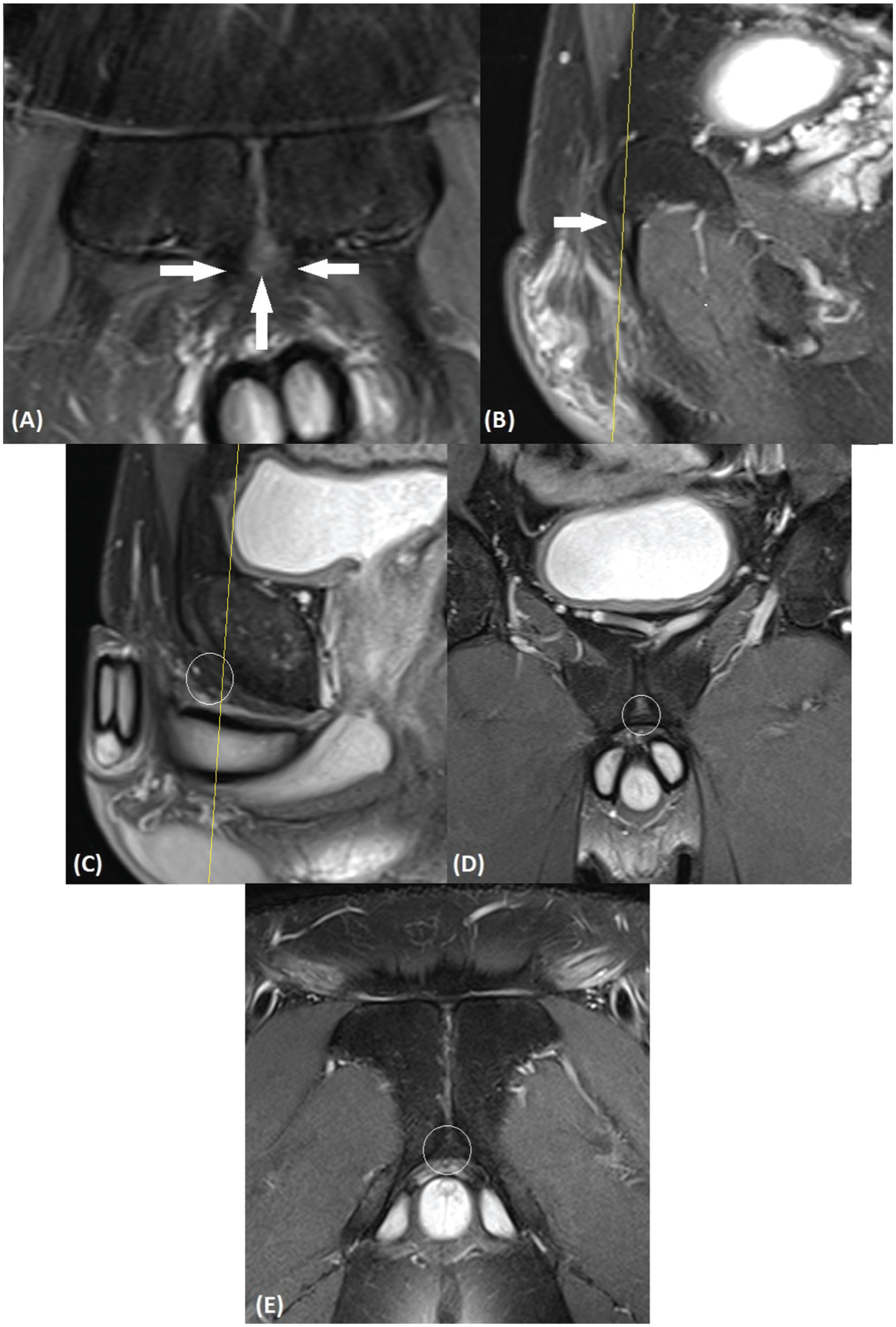
Normal magnetic resonance imaging anatomy of pubic bone and capsulotendinous structures. (A) Coronal and (B) sagittal (left of midline) intermediate-weighted fat-suppressed magnetic resonance images show normal attachment of adductor longus and the fibrocartilage (white arrows). Images more posteriorly also demonstrate normal magnetic resonance imaging morphology of the inferior pubic ligament (white circles) bridging the inferior pubic rami in the (C) sagittal, (D) coronal, and (E) oblique axial planes.
Selection of Athletes With Pubic-Related Groin Pain
All included athletes had pubic-related groin pain. During the clinical examination, pressure pain on the symphysis was the most painful test. The adductor, iliopsoas, and abdominal muscle test results were negative. Hip and spine provocation test results were also negative. All athletes were included from recreational to professional.
Inclusion Criteria
Inclusion criteria were as follows:
Men and women between the ages of 18 and 60 years
Clinical diagnosis of pubic-related groin pain made by a qualified sports physician
Participation in a sports activity at least twice a month or a history of sport in which the athlete experienced the groin injury
Exclusion Criteria
Exclusion criteria were as follows:
Athlete was unable to understand the study procedures, did not give oral informed consent, and/or did not wish to participate in 1 of the diagnostical protocols.
Athletes had adductor-, iliopsoas-, and inguinal-related groin pain.
Pregnancy
Diabetes mellitus
Proven and current symptomatic peripheral nerve entrapment syndrome in the groin area
Proven and current symptomatic radiculopathy at the thoracic or lumbar spine level
Fibromyalgia or chronic fatigue syndrome
Clinically significant medical abnormalities that would make the participant unsuitable for the study, as judged by the investigator (eg, mental disorder)
MRI general contraindications (eg, metal implants, MRI-noncompatible pacemakers, cochlear implant, cerebral clips)
Study Procedures
All included athletes were subjected to a standardized questionnaire (step 1), a clinical examination (step 2), and an MRI examination of the pelvis (step 3). Steps 1 and 2 were performed by a qualified sports doctor (T.M.) with 7 years of experience who subspecialized in groin pain. All pelvic magnetic resonance examinations (step 3) were analyzed by 2 reviewers in consensus—with the first reviewer (P.V.D.) being a musculoskeletal radiologist with 21 years of experience in musculoskeletal radiology and the second reviewer (T.M.) being a specialist in sports medicine with anatomic and clinical experience in pubic-related pathologies. In unclear cases or cases of disagreement, a consensus reading was organized with a third reviewer (F.V.G.; 32 years of experience in orthopaedic surgery and clinical anatomy) and a fourth reviewer (L.V.N.; 33 years of experience in anatomy) to reach a final consensus diagnosis.
MRI Analysis
Image analysis was performed on a PACS monitor with 5-megapixel resolution (Barco) in a standardized fashion. The pubic bone and its musculotendinous (adductor) attachments, along with the capsular/ligamentous tissues of the symphysis pubis, were assessed according to previously reported magnetic resonance criteria of pubic-related injury.2,14,16 Adductor tendons were assessed on T2-WI for tendinosis (enlargement and hyperintense signal) or tear (presence of a curvilinear fluid-equivalent signal undermining the insertion of the adductor longus/brevis; ie, secondary superior or inferior cleft sign). The pubic body was assessed for bone marrow edema, bone erosions, and osteophytes (osteitis pubis) with or without separation with involvement of the adductor plate.
Although no reference standard currently exists for the assessment of IPL injury on MRI, Robinson et al 16 described the evaluation of capsular structures of the pubic symphysis on MRI. In addition, recent anatomic studies have precisely localized the IPL, with its anatomic course and attachments corresponding to the structures visualized on MRI (Figure 1).12,13,15
The IPL and its injuries were classified as follows.
IPL injury grading
Grade 0 (normal): IPL shows continuous low–signal intensity (SI) deep capsular fibers spanning the inferior pubic rami.
Grade I (minor sprain): T2-WI shows high SI surrounding the IPL (mild periligamentous edema), which has normal SI and continuity.
Grade II (severe sprain or partial tear): T2-WI shows high SI in the IPL, which has partial discontinuity.
Grade III (complete tear): T2-WI shows high-fluid SI in the IPL, which has (near) complete discontinuity.
Diagnostic confidence score (DCS) on a 5-point Likert scale for the probability of an IPL lesion 1: Definitely no IPL lesion 2: Probably no IPL lesion 3: Equivocal 4: Probably IPL lesion 5: Definitely IPL lesion/tear
17
Associated MRI findings related to the pubic area, including injuries to the adductor tendons, capsular tissues, and pubic bone
After all participants completed the 3 steps, all the collected data were analyzed. Along with the MRI findings, qualitative analysis was made of the anamnestic and clinical characteristics of all athletes. The following demographic and clinical variables were recorded: type of groin pain (pubic vs adductor), sex, age, sport type, trauma history, and duration of symptoms.
Control Group
For comparison, a retrospective control group was included to assess the specificity of IPL injury for pubic-related groin pain and to explore the relationship between IPL injury and pubic-related groin pain. This control group consisted of athletes who met the same inclusion and exclusion criteria as the study group, with the only difference being that they were clinically diagnosed with adductor-related groin pain instead of pubic-related groin pain. The control group underwent the same standardized MRI protocol and was clinically evaluated by the same sports physician during the same period. The MRI data of this group were reassessed for the presence of IPL lesion using the same classification and review process.
Sample Size
The prevalence of IPL lesion in patients with pubic-related groin pain was initially assumed to be 0.2. To produce a 2-sided 95% confidence interval (95% CI) with a width of no more than 0.2 using the Agresti-Coull formula (as recommended by Brown et al 3 when n > 40.9), 58 patients with pubic-related groin pain were needed. 17 This calculation was performed in the MKpower package in R Version 4.2.3.
Statistical Analysis
The Agresti-Coull formula was used to calculate the confidence interval for the prevalence of IPL lesion in patients with pubic-related groin pain. We compared the characteristics of the patients with or without pubic-related groin pain, as well as with or without an IPL lesion, using a Pearson χ2 or Fisher exact test for categorical data, depending on the expected frequencies, and a Mann-Whitney-Wilcoxon test for continuous data. 17 We used binomial logistic regression to analyze the risk of IPL lesion according to potential risk factors. If separation was present (ie, when no IPL lesion occurred in 1 level of a categorical variable), we used Firth penalized logistic regression. Data were reported as odds ratios (ORs) with 95% CI. The level of statistical significance was set at .05. The analyses were performed with StataNow/BE 19.5.
Results
Demographics and Clinical Characteristics
A total of 60 athletes with a confirmed clinical diagnosis of pubic-related groin pain were included in the study group. Of these, 93% (n = 56) were male and 7% (n = 4) were female. The patient population consisted of athletes from various sport levels, from the recreational athlete to the professional athlete. The main sports of most participants were soccer (n = 42; 70%) and track and field (n = 10; 17%). The other athletes’ (n = 8) main sports were volleyball, hockey, tennis, golf, and trail running. The median age of the population group was 31 years (IQR, 24-42.5). An extended overview of the patients’ demographics is provided in Table 1. All included participants, referred to as “athletes” in this study, were involved in sports activities at least once a week before their injury. No distinction was made between recreational and professional athletes.
Characteristics of the Athletes of the Pubic-Related Groin Pain Group a

Data are presented as No. (%) or median (IQR). DCS, diagnostic confidence score; IPL, inferior pubic ligament.
No athletes had a DCS of 4 (probably IPL lesion).
A total of 28 athletes with a confirmed clinical diagnosis of adductor-related groin pain were retrospectively included as control group. Demographic comparisons showed that the control group included a significantly higher proportion of female athletes (32% vs 7%; P = .003) and fewer soccer players (46% vs 70%; P = .03). The age range and practice of sports were otherwise comparable between groups. A complete comparison of clinical and imaging characteristics between groups is presented in Table 2.
Comparison of Data Between Patients With Pubic- and Adductor-Related Groin Pain a

Data are presented as No. (%) or median (IQR). Adductor related indicates tendinopathy or lesion; pubic related indicates degenerative alterations at pubic symphysis. IPL, inferior pubic ligament.
MRI Findings
In the pubic-related groin pain group, 18% (n = 11) of the participants were rated a DCS of 5 (definitely IPL lesion/tear); 15% (n = 9), DCS of 3 (equivocal); 2% (n = 1), DCS of 2 (probably no IPL lesion); and 65% (n = 39), DCS of 1 (definitely no IPL lesion) (Table 1). No athletes had a DCS of 4 (probably IPL lesion). A representative image of an athlete with an IPL lesion associated with adductor tendinopathy and pubic bone marrow edema on MRI is shown in Figure 2. In the context of further statistical and qualitative analysis, participants with a DCS ≥3 were classified into the “IPL injury group” and those with a DCS <3 into the “no IPL injury group” (Table 1). The prevalence of IPL injury on MRI was 33% (95% CI, 22%-46%; n = 20). In contrast to the study group, no IPL injuries were observed on MRI in the adductor-related groin pain group, whereas 33% (n = 20) of the pubic-related groin pain group demonstrated definite or equivocal IPL lesions (P < .001). This finding suggests a strong association between IPL injury and pubic-related groin pain (OR, 41.01; 95% CI, 2.22-757.45).
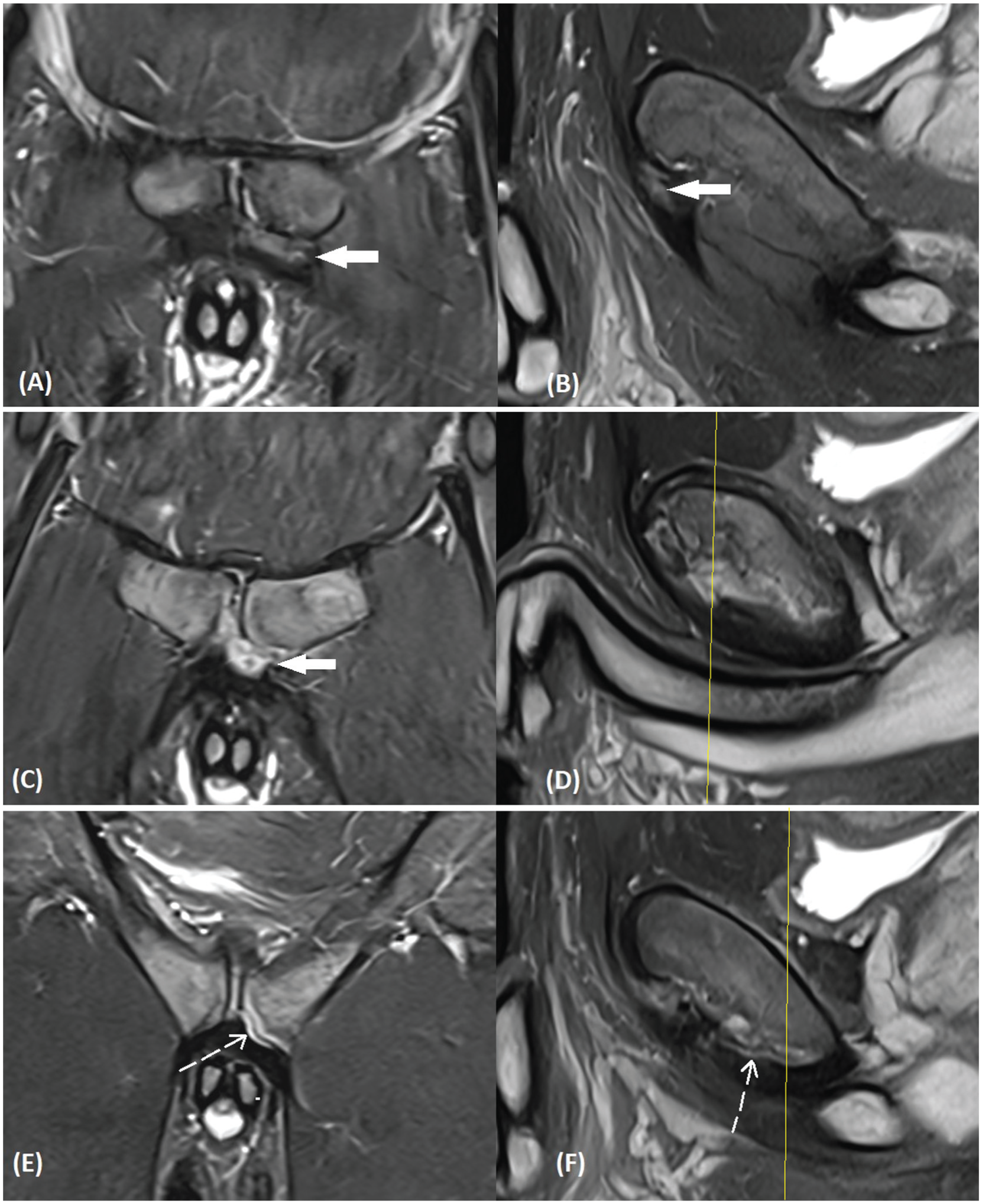
Magnetic resonance imaging of adductor injury with associated inferior pubic ligament lesion. (A, C, E) Coronal and (B, D, F) corresponding sagittal intermediate-weighted fat-suppressed magnetic resonance images show hyperintense (fluid) signal intensity (white arrows) at the level of the (A, B) adductor longus and (C) brevis insertions. Note far posterior extension of abnormal signal in the inferior pubic deep capsular structures/inferior pubic ligament, with a strip of ligament torn from pubic attachment on the left side (white dotted arrow at images E and F). Also note bone marrow edema surrounding the symphyseal joint.
The adductor-related groin pain group showed the following MRI-observed abnormalities: 32% (n = 9) had adductor tendinopathy, 11% (n = 3) had degenerative changes at the symphysis pubis, and 21% (n = 6) had both findings. A representative image of an athlete with an adductor lesion and intact IPL is shown in Figure 3.

Magnetic resonance imaging of adductor longus pathology without an IPL lesion (control group). (A, C) Coronal and (B, D) corresponding sagittal intermediate-weighted fat-suppressed magnetic resonance images show high signal intensity at the level of (A, B) the adductor longus insertions (white arrow at images A and D). Normal signal intensity at the inferior pubic capsular structures/IPL, indicating a normal IPL (white dotted circle at images B and C). IPL, inferior pubic ligament.
Subgroup Analysis: Athletes With IPL injury
Of the 20 athletes with a lesion at the IPL, 20% had a grade I injury, 70% had grade II, and 10% had grade III (total rupture of the IPL). Of the 20 IPL injuries, 10 (50%) occurred without an adductor injury, with only associated degenerative alterations at the pubic symphysis diagnosed on MRI. In 5 (25%) athletes, the IPL lesion was combined with adductor tendinopathy. The other associated injuries were a combination of osteitis pubis and adductor conjoint tendon injury (15%) and aponeurotic injury (10%). Representative images of an athlete with an IPL lesion and associated injuries on MRI are shown in Figures 2, 4, and 5.

Magnetic resonance imaging of pubic bone injury with associated inferior pubic ligament lesion. (A, C, E) Coronal and (B, D, F) corresponding sagittal intermediate-weighted fat-suppressed magnetic resonance images show normal signal intensity at the level of (A, B) the adductor longus insertions (white dotted line at image A). Irregularity can be seen at the symphysis pubis. (C, D) Mid and (E, F) posterior sections (indicated by solid yellow line in images D and F) show posterior extension of abnormal signal in the inferior pubic capsular structures/inferior pubic ligament, as partially torn from the pubic attachment on the left side (white circle at images C and E) with an intact symphyseal cleft. (A, C) Also note bone marrow edema surrounding the symphyseal joint.

Magnetic resonance imaging of pubic bone injury with associated inferior pubic ligament lesion. (A, C) Coronal and corresponding (B, D) sagittal and (E) oblique axial intermediate-weighted fat-suppressed magnetic resonance images show evident abnormal signal intensity in the inferior pubic ligament (mid/posterior deep capsular disruption) centrally at the (A, B) mid and (C-E) posterior sections of the symphysis pubis (white circles). Also note bone marrow edema surrounding the symphyseal joint (white arrows).
Of the 20 athletes with an IPL injury, 18 were soccer players and 2 were athletics in track and field. All were men. The median age was 30 years (IQR, 26-36). The mean duration of pubic-related pain was 31 months for the athletes with an IPL lesion, as compared with 7.5 months for the athletes without an IPL lesion. A total of 13 (65%) athletes with an IPL injury had experienced a trauma injury mechanism; 12 of these were soccer players. The 2 most common trauma situations were that the knee got stuck in the ground during a tackle and an unexpected splitting movement occurred during a pivoting movement. An incorrect, uncontrolled turning movement when kicking the ball was also cited twice as a trauma mechanism. One hurdler experienced an IPL injury when he fell after hitting a hurdle.
To identify independent risk factors for the presence of an IPL lesion, multivariable logistic regression analysis was performed. Several demographic and clinical variables were examined, including type of groin pain (pubic vs adductor), sex, age, sport type, trauma history, and associated MRI findings.
In unadjusted (univariable) analysis, athletes with a clinical diagnosis of pubic-related groin pain had significantly higher odds of IPL injury as compared with athletes with adductor-related of groin pain (OR, 28.85; 95% CI, 1.67-496.81; P = .02). Similarly, participation in soccer was associated with increased odds of an IPL lesion (OR, 7.54; 95% CI, 1.62-35.06; P = .01), as was a history of trauma (OR, 6.04; 95% CI, 2.06-17.71; P = .001). Sex and age were not significantly associated with the presence of an IPL lesion (Table 3).
Univariable Analysis of the Risk of Inferior Pubic Ligament Lesion

Once we adjusted for the type of groin pain (pubic related or not) and the presence of trauma, the association between soccer and IPL lesion was no longer statistically significant (OR, 3.74; 95% CI, 0.79-17.66; P = .10). In a separate model, type of groin pain and the presence of trauma remained significantly associated with an IPL lesion; specifically, the odds of an IPL lesion were 41.01 (95% CI, 2.22-757.45; P = .01) in athletes with pubic-related groin pain and 8.00 (95% CI, 2.43-26.36; P = .01) in those with trauma.
Discussion
This study provides the first MRI and clinical evaluation of IPL injury in athletes with pubic-related groin pain, as strengthened by comparison with a control group with adductor-related groin pain. The results demonstrate a relatively high prevalence of IPL injuries among athletes with pubic-related groin pain (33%) and suggest a specific association between IPL lesions and pubic-related groin pain, as no IPL lesions were observed in the adductor-related groin pain group.
This is a significant addition to the current knowledge. Until now, IPL injury had been described in only a case report and anatomic studies.11-13,15 By demonstrating that these lesions are absent in athletes with clinical types of adductor-related groin pain, the specificity of IPL involvement in pubic-related groin pain is supported.
Furthermore, the data show that trauma is a key risk factor and that MRI-detected IPL injury is associated with degenerative changes at the pubic symphysis. These findings support the inclusion of IPL injury in the differential diagnosis of groin pain in athletes, especially after trauma.
Pain Mechanism
It is conceivable that IPL injury contributes to pubic-related groin pain in 2 ways.
First, ligaments have nerve fibers within them, and injury/inflammation results in pain. The reason why an injury of the IPL may cause pubic-related groin pain is explained on the basis of Hilton's law. 6 Hébert-Blouin et al 5 clarified in a thorough review of Hilton's law that a muscle or ligament insertion to the bone relates to bone pain and to muscle pain (ie, the pain of the connectives; no nerves in the muscle). Because of development, spaces occur related to nerves and subspaces to subnerves, in which each space refers to a distinct nerve. This is topographic thinking, which explains, for example, that bone pain refers to the muscles (their connectives) of the same innervation of the same space and that an IPL injury refers to pubic pain.
Second, ligament injury causes pubic symphysis instability and overload of attached muscles. An injury to the IPL will cause reduced stability in the pubic joint. As a result, the tendons that attach to the pubic joint (conjoint tendon adductors, rectus abdominis) become overloaded more quickly.4,16 The data of this study show that athletes with concomitant adductor tendinopathies were often well trained in physical therapy. But they kept relapsing because of the reduced stability attributed to the IPL tear.
Clinical Features
Of the athletes who sustained an IPL lesion, 65% had a history of a trauma incident in which they suddenly felt a stabbing pain in their pubic bone. Three soccer players said that the complaints started after they threw a tackle in which their knee got stuck in the ground and their other leg slid down. Three other athletes reported feeling a painful click in their pubic joint when they did an unexpected split—for example, a goalkeeper who comes out and can just stop the ball with his foot with an extreme split movement. Most of the described causal traumas of an IPL injury had the same biomechanical impact: a high passive load/force on the symphysis in the opposite craniocaudal direction after unexpected trauma, which probably puts pressure on the IPL resulting in a tear in the ligament fibers.
A noteworthy observation in the data of this study was that athletes with an IPL lesion reported a longer duration of pubic-related pain as compared with athletes with an intact IPL. Specifically, the mean duration of symptoms was 31 months in athletes with an IPL lesion, as compared with 7.5 months in those without. Anatomic studies stated that the IPL has poor blood circulation; this may affect healing of the IPL.1,9,19 Repetitive stresses from normal or continued athletic participation could also affect the healing process of the ligament.
Palpatory pain at the level of the symphysis is the most prominent clinical sign. It should be mentioned that many other causes of pubic pain have this finding (eg, osteitis pubis). Pinpoint pain is often most pronounced at the angulus inferior of the pubic bones, where the IPL runs. Another positive clinical test for IPL injury cannot yet be extracted from the data of this study.
However, an IPL injury is suspected when an athlete presents with pubic-related groin pain after a trauma, with pressure pain at the pubic symphysis being prominent during clinical examination. In isolated IPL injuries, all adductor and abdominal tendon–related clinical test results will be negative. Yet, it must be considered that over a longer period, overload injuries to these tendons may be due to the loss of the stabilizing function of the IPL on the pubic symphysis.
MRI Features of IPL Injury in Athletes With Pubic-Related Groin Pain
In athletes with pubalgia, MRI has been used extensively to investigate the pubic bone, the symphysis, and its surrounding capsulotendinous structures, including the aponeurotic tissues of the rectus abdominis/pyramidalis and adductor muscles.2,14,16 Common MRI findings in these patients include pubic bone degenerative remodeling changes (marrow edema, spurs, erosions, sclerosis, cyst formation), manifestations of symphyseal disc degeneration (irregularity with “primary” fluid cleft), and adductor pathology (tendinosis/tear with “secondary” fluid cleft sign). Although previous MRI studies have found a number of changes that correlate with clinical symptoms, such changes may also be seen in asymptomatic athletes.
Whereas most imaging studies have focused on the anterior pelvis and adductor muscles in patients with adductor-related groin pain, very few have investigated the MRI appearance of the capsule and ligaments of the symphysis pubis. In an anatomic study of MRI performed in 17 cadaver specimens and 10 asymptomatic professional athletes, Robinson et al 16 found an intimate relationship between the symphysis pubis capsular structures and the anterior soft tissues, receiving contributions from the adductor longus, adductor brevis, and rectus abdominis tendons and muscles. However, the IPL was not specifically mentioned in this study, nor were IPL injuries assessed.
According to recent anatomy studies focusing on the pubic ligaments, the IPL, which lies on the inferior rami of the pubic symphysis, has attachments only from the adductor brevis and gracilis muscles, whereas the rectus abdominis and adductor longus are not attached to the IPL. In all of our patients, MRI evaluations were performed on far posterior slices through the symphysis pubis, for which great care was taken to evaluate the thick, deep inferior capsular tissues of the symphysis pubis.
This study used standard orthogonal-based 2D TSE MRI sequences, the backbone of clinical (pelvic) MRI, owing to its excellent tissue contrast. Although the additional oblique axial and coronal imaging planes help to better visualize the IPL, the relatively larger slice thickness (2-3 mm) of 2D images comes with a major disadvantage—partial volume effects. Alternatively, 3-dimensional TSE sequences acquire thin slices to obtain submillimeter isotropic voxel resolution, compensating for partial volume effects and thereby enabling multiplanar reformations to better display obliquely running complex anatomic structures (eg, IPL). However, traditional drawbacks of current clinically available 3-dimensional sequences include lower image quality and longer scan times as compared with 2D TSE sequences. In this regard, there are ongoing technological advancements in the field of MRI by all major vendors regarding acceleration and image quality enhancement by means of advanced deep learning image reconstruction based on supervised learning and convolutional neural networks. These are promising methods to better assess the complexity of anatomy and pathology of the pubic ligaments in the near future.
Limitations
This study has several limitations. First, spatial resolution may be limited by use of a clinical MRI protocol with 2D TSE at relatively thick slices (2-3 mm) as performed at various institutions (fat suppressed vs short tau inversion recovery) at different field strengths (1.5T vs 3T). As a result, it may not be possible to reliably differentiate between superficial adductor aponeurotic fibers and deeper capsuloligamentous structures. However, the MRI-based assessment of the IPL in this study aligns well with current anatomic understanding. We wanted to obtain a decent sample size in the inclusion period of 4 years to have sufficient power for epidemiologic study. Most athletes who presented in this period with groin pain had adductor- or hip-related injuries, and athletes with clinical adductor- or hip-related groin pain were excluded from the study group.
In addition, athletes put pressure on getting imaging as soon as possible. As such, some scans were taken on a different MRI machine because of a shorter waiting list. Second, consensus readings were used instead of independent evaluations. As independent ratings were not retained, no formal measure of interobserver agreement was calculated. Yet, we combined all the expertise of the radiologist, anatomists, and clinicians to obtain the best result of analyzing the MRI scans. Another limitation was that both reviewers were aware of the clinical information and outcomes of the patients. This introduces potential bias in the interpretation of MRI findings, which might affect the reliability of the results. Third, the pubic-related groin pain population is predominantly male (93%; n = 56), with only 4 female athletes included. This gender imbalance limits the generalizability of the findings to female athletes with pubic-related groin pain and may not adequately represent the full spectrum of IPL injuries across genders. Additionally, the sample size to analyze the risk of IPL lesion with logistic regression was small in different subgroups, as reflected by the large confidence intervals. There could also be bias for the type of sports. The sports that the included athletes practice likely depend on those that are most popular in the country where the study was conducted (Belgium). There is also the possibility that the investigators saw only chronic injuries because some/many acute injuries may heal.
Conclusion
This study is, to the best of our knowledge, the first to systematically investigate IPL injuries in athletes with pubic-related groin pain using clinical and MRI evaluation. The findings reveal that IPL injury is not uncommon: 18% exhibited definite MRI signs of IPL injury and an additional 15% showed equivocal findings, resulting in a total of 33% with potential IPL involvement. MRI findings demonstrated that IPL injuries frequently co-occur with degenerative changes in the pubic bone and with adductor tendinopathy.
No IPL injuries were observed in a control group of athletes with adductor-related groin pain on MRI. These findings suggest that IPL lesions are not only associated with pubic-related groin pain but may also play a contributing causal role in its development.
Given the frequency and specificity of IPL lesions in athletes with pubic pain, clinicians should consider this ligamentous injury in the differential diagnosis of pubic-related groin pain, especially after trauma. Future studies will be needed to clarify its treatment, impact on prognosis, rehabilitation strategies, and return-to-play outcomes.
Footnotes
Final revision submitted July 18, 2025; accepted August 1, 2025.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Antwerp (UZA study registration B3002020000220).