
Abstract
Background:
It remains unclear whether results differ between a Latarjet procedure performed after a failed arthroscopic Bankart repair and one performed as the primary operation.
Purpose:
To compare the postoperative outcomes of the Latarjet procedure when performed as primary surgery and as revision for a failed arthroscopic Bankart repair.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A multicenter retrospective comparative case-cohort analysis was performed for all patients undergoing a Latarjet procedure for recurrent anterior shoulder instability. Patients were separated into 2 groups depending on if the Latarjet procedure was performed after a failed arthroscopic Bankart repair (group 1) or as the first operation (group 2). Outcome measures included recurrent instability, reoperation rates, complications, pain, Walch-Duplay scores, and Simple Shoulder Test.
Results:
A total of 308 patients were eligible for participation in the study; 72 (23.4%) did not answer and were considered lost to follow-up, leaving 236 patients available for analysis. Mean follow-up was 3.4 ± 0.8 years. There were 20 patients in group 1 and 216 in group 2. Despite similar rates of recurrent instability (5.0% in group 1 vs 2.3% in group 2; P = .5) and revision surgery (0% in group 1 vs 6.5% in group 2; P = .3), group 1 demonstrated significantly worse pain scores (2.56 ± 2.7 vs 1.2 ± 1.7; P = .01) and patient-reported outcomes (Walch-Duplay: 52 ± 25.1 vs 72.2 ± 25.0; P = .0007; Simple Shoulder Test: 9.3 ± 2.4 vs 10.7 ± 1.9; P = .001) when compared with those patients undergoing primary Latarjet procedures.
Conclusion:
Functional outcome scores and postoperative pain are significantly worse in patients undergoing a Latarjet procedure after a failed arthroscopic Bankart repair when compared with patients undergoing primary Latarjet. The assumption that a failed a Bankart repair can be revised by a Latarjet with a similar result to a primary Latarjet appears to be incorrect. Surgeons should consider these findings when deciding on the optimal surgical procedure for recurrent shoulder instability.
The 2 most common surgical interventions for recurrent anterior shoulder instability are arthroscopic Bankart repair 30 and the Latarjet procedure. 21 However, indications for each procedure remain debated among surgeons, with 90% of surgeons outside of France initially preferring soft tissue Bankart repair.6,33 Balg and Boileau 3 proposed a scoring system relying on clinical and radiological criteria to help the surgeon decide between these procedures (Instability Severity Index Score); however, this has not been widely implemented in practice. 16 Several procedures have been described for the management of a failed arthroscopic Bankart repair. These include revision arthroscopic Bankart repair, ¶ open Bankart repair,8,9,32 and a Latarjet procedure.8,11,31 However, a patient with failed arthroscopic Bankart repair is at increased risk of recurrent instability after revision arthroscopic Bankart surgery as compared with conversion to a Latarjet procedure.8,11,31 The redislocation rate after arthroscopic Bankart repair has been proven to be higher than that after a Latarjet procedure (28.4% vs 3%).1,38 This has led some surgeons, especially in Europe, to recommend performing a Latarjet procedure in all primary cases of recurrent anterior shoulder dislocation. However, Bankart repairs are associated with a very low complication rate when recurrent dislocations are excluded. Given this lower nondislocation complication rate, other surgeons recommend performing an arthroscopic Bankart repair for patients with recurrent shoulder instability with noncritical bone loss, regardless of the Instability Severity Index Score, as it can easily be revised to a Latarjet in case of failure. We hypothesized that the results of a Latarjet procedure performed after a failed arthroscopic Bankart repair would differ from those performed for primary cases. The purpose of our study was to compare the postoperative outcomes between the Latarjet procedure when performed as primary surgery and those when performed as revision for a failed arthroscopic Bankart repair.
Methods
A retrospective study was conducted and ethics permission was waived by the institutional local review board of the Maussins Clinic in Paris. A comparative case-cohort analysis was performed for all patients who underwent a primary Latarjet procedure or a Latarjet procedure after a failed arthroscopic Bankart repair for recurrent anterior shoulder instability in 1 of 5 institutions. Patients were included if they were 18 years or older at the time of surgery, if they had undergone surgery between January 1, 2013, and December 31, 2015, and if they had a minimum follow-up of 2 years. Patients were excluded if they had additional shoulder pathology at the time of surgery, including posterior or multidirectional instability, pathological involvement of the long head of the biceps requiring tenotomy/tenodesis, rotator cuff tear, or symptomatic acromioclavicular joint arthritis. Patients were also excluded if they could not speak or read French. Patients eligible for the study were identified with a computerized database of all patients undergoing surgery for shoulder instability at 5 institutions. Medical records of all the eligible patients were reviewed by 3 independent reviewers (V.S., L.A., A.H.) to collect the following data: patient demographics, number of episodes of dislocation before surgery, the time between the first dislocation and surgery, arm dominance, shoulder hyperlaxity, level of sport, type of sport, and Instability Severity Index Score. Shoulder hyperlaxity was defined as passive external rotation ≥85° or a Gagey test >95°, as described by Balg and Boileau. 3 An episode of dislocation was defined as a glenohumeral dislocation that required reduction by someone else. The level of sport was categorized as “competitive,” “recreational,” or “none.” The type of sport was categorized as “contact/collision,” “throwing sports,” and “other.” Standard preoperative anteroposterior radiographs of the shoulder were assessed for a Hill-Sachs lesion with the arm in external rotation. Similarly, the glenoid contour was assessed for loss of contour as described by Balg and Boileau.
Surgical Procedure
All surgical procedures were performed by 5 fellowship-trained shoulder surgeons (G.N., J.K., J.D., N.S., P.H.). Two techniques were used, depending on the surgeon’s choice:
A mini-open technique with a commercially available drill guide (Arthrex) and two 4-mm cannulated cancellous screws as based on the modified Latarjet procedure described by Walch and Boileau 36
An arthroscopic technique described by Lafosse et al, 20 with a specific guide (DePuy Mitek) and two 3.5-mm cannulated cancellous screws
Postoperative Management
All patients had a similar postoperative protocol and wore a sling with the upper limb in internal or neutral rotation during the first postoperative week. At the beginning of the second week, patients were encouraged to discontinue their sling and start self-assisted passive range of motion for 3 weeks. After 1 month postoperatively, patients were referred to a physiotherapist to start active elevation and external rotation. Patients were allowed to return to full activity at 4 months postoperatively.
Assessment at Latest Follow-up
After the initial chart review, all remaining eligible patients were contacted via phone and mailed or emailed a questionnaire to assess shoulder function and instability at a minimum of 2 years after their Latarjet procedure. Patients were given a month to respond from the time that the initial questionnaire was mailed before being contacted again by a member of the study team via phone. After 2 attempts, patients were considered lost to follow-up. Included in the questionnaire were the Walch-Duplay score, 35 the Simple Shoulder Test, questions regarding recurrent dislocation and revision surgery, and a visual analog scale for pain.
Statistical Analysis
Categorical variables were summarized with percentages and continuous variables with means and standard deviations. Fisher exact test was used to compare categorical variables and Wilcoxon test for continuous variables.
Recurrence and reoperation were estimated with the Kaplan-Meier method, and curves were compared with the log-rank test. All statistical analyses were performed with SAS (v 9.4; SAS Institute). P values were assessed at the level of 5%.
Results
Patient Demographics
A total of 308 patients were eligible for participation in the study. Of these, 72 patients (23.4%) did not answer and were considered lost to follow-up, leaving 236 patients available for analysis. Twenty patients had undergone an arthroscopic Bankart repair before the Latarjet procedure (group 1), and 216 were treated initially with a Latarjet (group 2). Both populations were comparable regarding preoperative data except for preoperative Instability Severity Index Score and the presence of a Hill-Sachs lesion, both of which were significantly higher in group 2 (3.8 ± 2.5 vs 4.9 ± 2 [P = .05] and 47.4% vs 75.8% [P = .01]). The characteristics of the 2 groups are detailed in Table 1.
Comparison of Preoperative Characteristics Between Patients With a Failed Previous Bankart Repair and No Previous Bankart Repair a
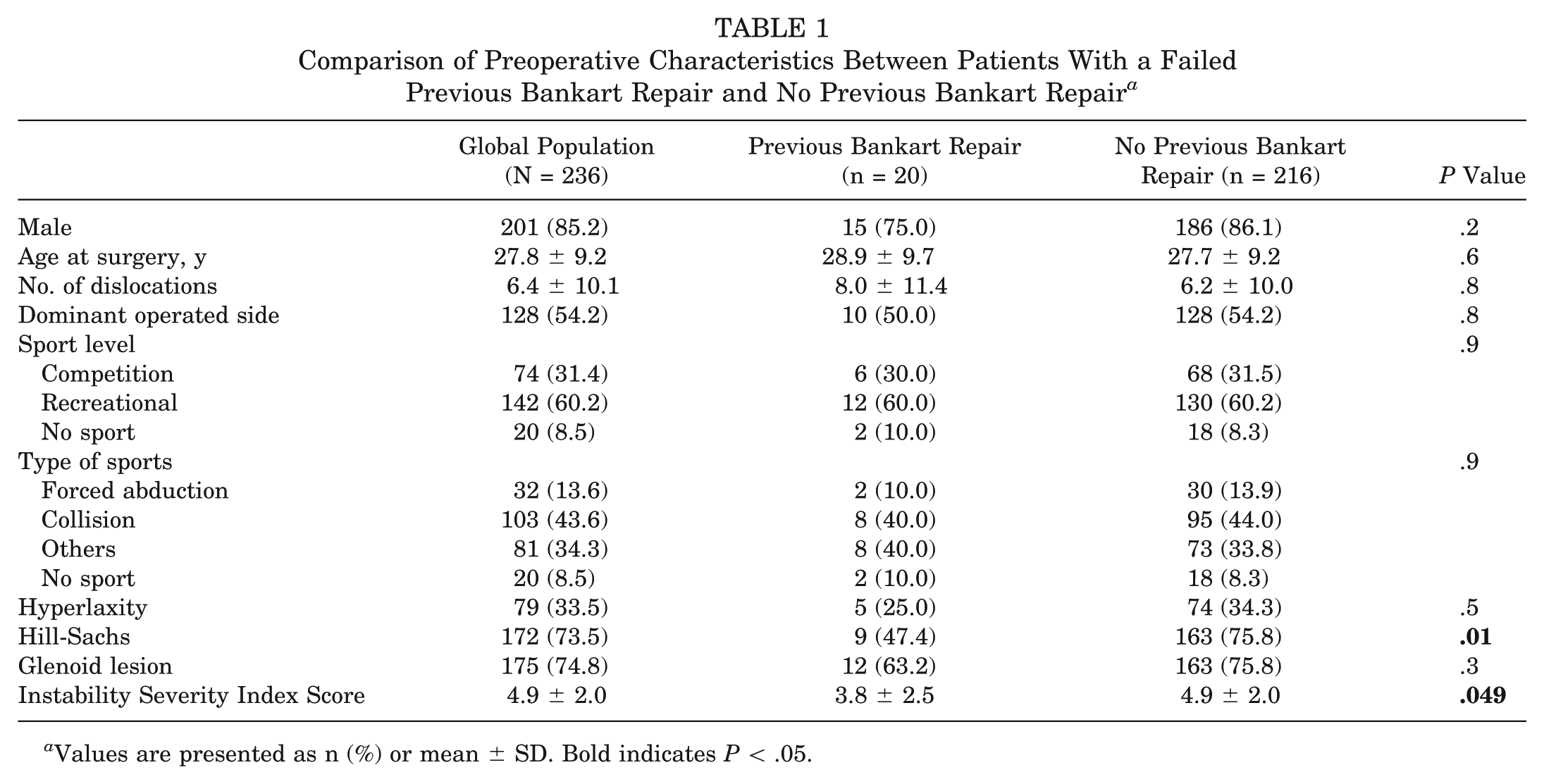
Values are presented as n (%) or mean ± SD. Bold indicates P < .05.
Outcomes
Mean follow-up was similar in both groups (3.6 ± 0.9 years in group 1 vs 3.4 ± 0.8 years in group 2; P = .3). The postoperative recurrence rate was 2.5% in the overall population, with no significant difference between groups in either recurrence rate (5.0% in group 1 vs 2.3% in group 2; P = .5) or revision rate (0% in group 1 vs 6.5% in group 2; P = .3).
Despite similar rates of recurrent instability and revision surgery, group 1 demonstrated significantly worse pain scores and patient-reported outcomes as compared with patients undergoing primary Latarjet procedures. The mean postoperative visual analog scale score in group 1 was 2.6 ± 2.7, as compared with 1.2 ± 1.7 in group 2 (P = .01). The mean Walch-Duplay score was 52.0 ± 25.1 in group 1 versus 72.2 ± 25.0 in group 2 (P = .0007). The mean Simple Shoulder Test score was 9.3 ± 2.4 in group 1 and 10.7 ± 1.9 in group 2 (P = .001). These results are detailed in Table 2.
Comparison of Postoperative Outcomes Between Patients With a Failed Previous Bankart Repair and No Previous Bankart Repair a
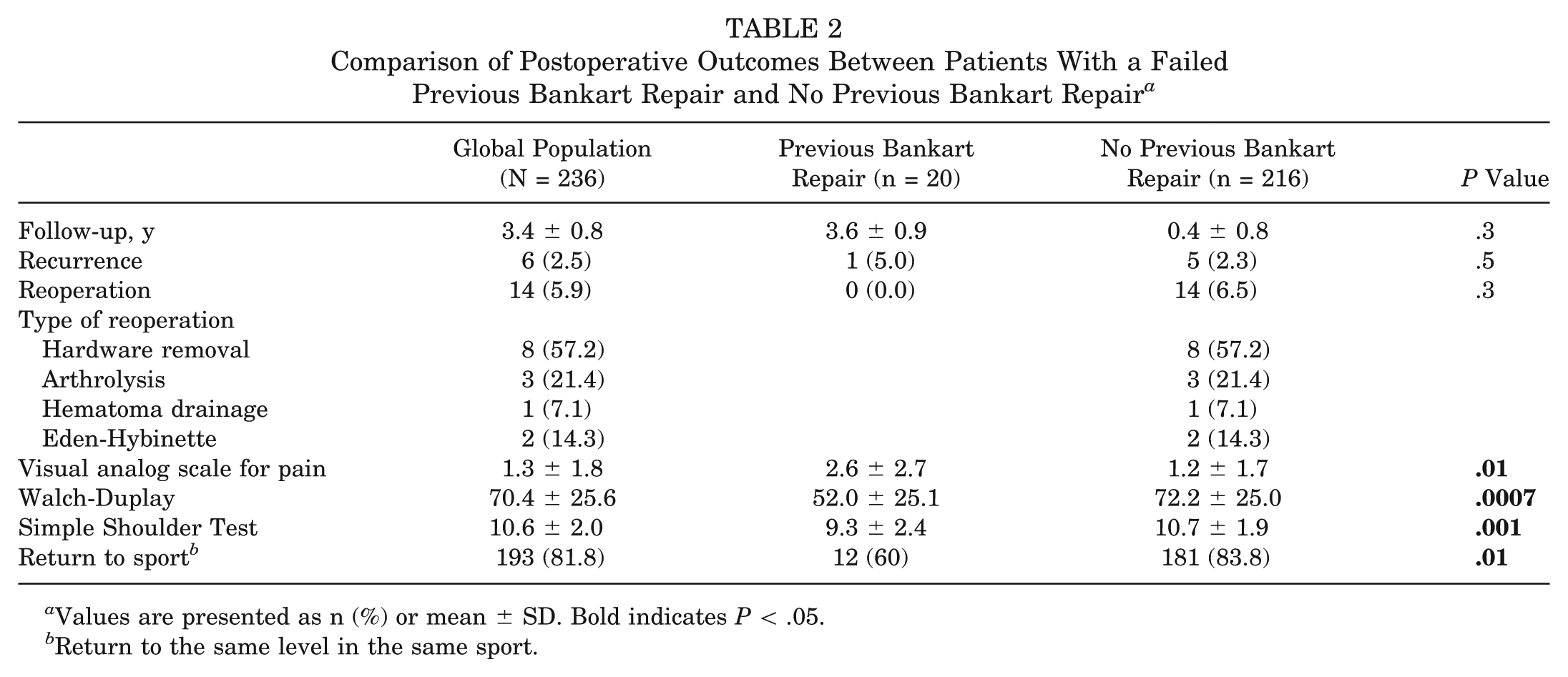
Values are presented as n (%) or mean ± SD. Bold indicates P < .05.
Return to the same level in the same sport.
Discussion
The study confirms that the Latarjet procedure is effective in restoring glenohumeral stability in the setting of primary chronic anterior instability (even in cases with an Instability Severity Index Score ≥4) and in the setting of a failed arthroscopic Bankart repair. This is in agreement with previous studies, which found recurrence rates between 1% and 11.6% after primary Latarjet1,6,14,15,26,38 and around 4% when performed as a revision procedure. 31
Ninety percent of surgeons outside of France initially prefer soft tissue Bankart repair,6,33 as it is associated with a very low rate of severe complications. Additionally, Latarjet remains an option should an arthroscopic Bankart repair fail. By comparison, a failed Latarjet remains very challenging to manage, with recurrence rates around 12% after an Eden-Hybinette procedure 23 and with 33% of patients reporting fair or poor results. 13
While many surgeons argue that Bankart procedures have lower complication rates, several recent studies showed higher recurrent instability with similar complication rates as compared with the Latarjet.1,38 Furthermore, recent studies showed no significant difference in postoperative osteoarthritis rates.17,37 In 2007, Balg and Boileau 3 proposed the Instability Severity Index Score to help the surgeon decide between arthroscopic Bankart repair and Latarjet. Initially, a score >6 was used to recommend a Latarjet. In later work, Phadnis et al 29 recommended lowering this threshold to 3, and more recently Thomazeau et al 34 reported that this threshold should even be lowered to 2. In a study of 141 consecutive patients, Phadnis et al showed that those with an Instability Severity Index Score ≤3 had a 4% risk of failure, as compared with a 70% risk of failure if the score was ≥4. In this series, the preoperative Instability Severity Index Score was significantly lower in the patients who had undergone a previous Bankart repair (mean, 3.8), suggesting that patients had been appropriately selected initially.
The assumption that a failed Bankart repair can be revised by a Latarjet with a similar result to a primary Latarjet appears to be incorrect relative to postoperative pain and functional scores in the setting of future Latarjet procedure. In shoulders with a history of failed arthroscopic Bankart repair, functional scores and postoperative pain were significantly worse. This supports the results reported by Schmid et al, 31 who showed that the Latarjet restored stability after a failed Bankart repair but was associated with persistent pain and worse functional results as compared with prior reports on primary Latarjet from the same institution 38 (mean subjective shoulder value, 79% vs 88.77%).
Our study has several limitations. First, it was a retrospective cohort study with 77% follow-up. The results may be affected by nonresponse bias, as it is possible that patients who had stable and pain-free shoulders did not take time to answer our questionnaire. On the contrary, it is possible that patients who experienced postoperative instability and/or dissatisfaction after the index surgery were preferentially lost to follow-up. Second, the definition of recurrence was limited to a new episode of dislocation that required closed reduction by a second party. This did not allow us to include episodes of subluxation or apprehension, which is considered failure in other published studies. Because we were unable to assess apprehension clinically with this study design, we chose to use frank redislocation as our definition of failure, which would be more memorable when assessed through a questionnaire. With an identical definition of failure in both groups, a comparison between these groups was possible. Third, there exists the possibility for performance bias in surgical technique secondary to differing techniques across 5 fellowship-trained surgical practices. However, sampling across 5 fellowship-trained practices with different surgical techniques may help better reflect general practice. Fourth, preoperative computed tomography scans were not obtained for all patients; therefore, we were unable to precisely quantify humeral and glenoid bone loss, which may have affected the rate of recurrent instability. Furthermore, we were not able to evaluate bone loss before shoulders underwent primary Bankart repair to assess if critical bone loss was present, where Latarjet may have been the preferred initial operation. Additionally, the study was not designed to evaluate graft osteolysis or graft positioning; as such, no postoperative computed tomography scans or radiographs were analyzed. Finally, given the rarity of recurrent surgery after a failed Bankart repair, the study group of shoulders undergoing a Latarjet after a prior Bankart repair was quite small. This means the study was underpowered to detect a difference with regard to recurrent instability. However, this limitation is likely unavoidable given the infrequency of this problem.
Conclusion
Functional outcome scores and postoperative pain are significantly worse in patients undergoing a Latarjet procedure after a failed arthroscopic Bankart repair when compared with patients undergoing a primary Latarjet. The assumption that a failed Bankart repair can be revised by a Latarjet with a similar result to a primary Latarjet appears to be incorrect. Surgeons should consider these findings when deciding on the optimal surgical procedure for recurrent shoulder instability.
Footnotes
Submitted April 30, 2019; accepted September 27, 2019.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.-D.W has received royalties for shoulder implants from FH Orthopedics. B.S. has received royalties for shoulder implants from Exactech. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.