
Abstract
Background:
The risk of second anterior cruciate ligament (ACL) injury remains high after ACL reconstruction (ACLR), indicating the need to improve rehabilitation and return-to-sport assessment. Because ACL injuries frequently occur in cognitively demanding situations, dual-task screening provides a promising opportunity to detect movement impairments by testing cognitive and motor skills simultaneously.
Purpose/Hypothesis:
The purpose was to evaluate cognitive-motor impairments that persist after ACLR. It was hypothesized that jump landing biomechanics would be impaired in athletes with previous ACLR versus controls and that these impairments would be exacerbated when the jump landings were performed with a cognitive challenge.
Study Design:
Controlled laboratory study.
Methods:
A total of 35 individuals who underwent primary ACLR (ACLR group) and 35 healthy controls (HC group), matched by sex, age, dominant limb, body mass index, sports activities, Tegner score, and Marx activity score, participated in this study. Participants performed jumping tasks under a variety of conditions, including with and without visual constraint, rapid decision-making, and visual-spatial challenges. Primary dependent variables included second ACL injury factors such as asymmetry of knee extensor moment at initial contact (KEM-Asym-IC). Second-level analysis focused on other variables associated with ACL loading and injury (eg, peak knee flexion angle [pKFA]). Mixed-effect models were tested for group and condition interactions as well as group and condition main effects.
Results:
A total of 35 individuals (25 women and 10 men) who underwent ACLR (ACLR group) (age, 19.9 ± 1.7 years; height, 1.7 ± 0.1 m; mass, 69.9 ± 13.1 kg; years after ACLR, 1.5 ± 0.6 years; Tegner score, 6.8 ± 1.8; and Marx score, 10.6 ± 3.8) were matched with 35 (25 women and 10 men) HC individuals (HC group) (age, 20.1 ± 1.9 years; hight, 1.7 ± 0.1 m; mass, 67.1 ± 8.4 kg; Tegner score, 6.6 ± 1.6; and Marx score, 11 ± 3.9). No significant group and condition interactions were detected. A group effect for KEM-Asym-IC (HC group, –0.005 ± 0.8 % bodyweight–height vs ACLR group, 0.43 ± 0.82 % bodyweight–height; P < .001) indicated relatively more knee extensor moment in the uninvolved limb at initial contact for the ACLR group, regardless of condition. In addition, a condition effect for pKFA indicated that both groups demonstrated decreased knee flexion in response to rapid decision-making challenges (anticipated conditions, 79°-80° vs rapid decision-making conditions, 76°-78°; P < .001).
Conclusion:
After return-to-sport clearance, the ACLR group showed increased presence of mechanics associated with second ACL injury compared with the HC group during jump landing movements, with rapid decision-making conditions also eliciting reduced pKFA during landing for both groups.
Clinical Relevance:
The extent to which these multivariable outcomes may compound injury risk after ACLR requires further research to more precisely understand opportunities for neurocognitive challenges to augment ACLR return-to-sport assessment.
Keywords
About half of all children and adolescents in the United States are involved in team sports. 10 However, within these sports, musculoskeletal injuries are common and significantly reduce participation.15,48 Anterior cruciate ligament (ACL) injury is a common musculoskeletal injury among athletes, with about 250,000 annual injuries in the United States. 22 The most common treatment for this injury is ACL reconstruction (ACLR). Although many adolescents return to sports after ACLR, nearly a quarter of athletes who are <25 years and return to sports sustain a second ACL injury. 58 The high risk of a second ACL injury may indicate that current return-to-sport approaches do not fully capture the risk for a second injury.
Many ACL injuries occur when an athlete's attention is directed externally (opponent, ball, etc). 57 Furthermore, poorer cognitive performance is linked to riskier biomechanics and altered muscle activation patterns during cognitively challenging movements8,20,26,40,50 as well as risk of ACL injury. 54 Despite the evidence for the relevance of visual-cognitive challenges to injury risk and biomechanics, athletes’ cognitive-motor function (ie, the ability to meet simultaneous cognitive and motor demands) is not routinely used as a criterion for return-to-sport (RTS) after ACLR. 12 The disconnect between isolated physical RTS tests and attention-demanding real-world sport scenarios likely contributes to the inconsistent association between passing RTS criteria and second ACL injury risk.12,33
Previous research on musculoskeletal injuries has explored a variety of stimuli, such as unexpected directional cues,9,11 visual targets, 26 sport-specific tasks, 38 and arithmetic tests, 14 primarily in healthy populations. 2 Although dual-task protocols have been used with ACLR patients,1,17,45,52,53 they have primarily focused on standing balance,37,41 weight-shifting tasks, 13 and gait,44,45 revealing impaired cognitive-motor performance after ACLR. More recent studies have begun to incorporate sport-relevant tasks such as jumping and cutting in dual-task paradigms.17-19,42,53 However, these efforts remain limited by using only singular cognitive tasks,17-19 not involving reactive challenges, 42 or lacking a control group. 53 Recently, Strong et al 52 reported magnified cognitive-motor interference in those who had ACLR compared with controls; however, the motor outcomes (eg, jump height) had unclear relevance to injury risk. 52 Building upon existing evidence to demonstrate the injury relevance of cognitive-motor interference after ACLR remains an important knowledge gap.
Although prospective studies provide the strongest evidence to demonstrate relevance to injury risk, these study designs are time-intensive and costly. These studies require strong preliminary data to obtain the necessary resources to conduct an extensive, prospective study. Alternatively, previous studies have identified potential biomechanical risk factors that can ground cross-sectional studies in clinically relevant outcomes related to the risk of second ACL injury. For example, in a study of 56 young male and female athletes, Paterno et al 46 found that less external rotator moments at the uninvolved hip (odds ratio [OR], 8.4), greater asymmetry in knee extensor moments at initial contact (OR, 3.3), and increased frontal plane knee motion (OR, 3.5) were associated with a higher likelihood of sustaining a second ACL injury. More recently, King et al 28 conducted a larger study into jump landing biomechanical predictors of a contralateral ACLR injury in male athletes 9 months after ACLR. Several biomechanical variables distinguished between participants who did and did not sustain a contralateral ACL injury within the 2-year follow-up of the study, including contact time, center of mass stiffness, and sagittal plane kinematics at the hip and knee. Although replicating the predictive value of these outcomes is needed to demonstrate the robustness of the findings and demonstrating generalizability requires additional work (eg, do King et al 28 findings extend to female patients?), these biomechanical risk factors for second ACL injuries provide feasible outcomes for a cross-sectional study that can provide preliminary clinical relevance of cognitive-motor function after ACLR that can then be explored more rigorously through a prospective study.
To understand the extent to which cognitive-motor deficits go undetected and/or unaddressed in standard ACLR rehabilitation, this cross-sectional study was conducted to evaluate dual-task impairments that persist after ACLR. We hypothesized that jump landing biomechanics would be impaired in athletes with previous ACLR versus controls and that these impairments would be exacerbated when the jump landings were performed with a cognitive challenge.
Methods
Participants
A total of 36 athletes who had undergone primary ACLR surgery and cleared to RTS (ACLR group) and 36 healthy controls (HC group) who were matched at an individual level on sex, age, dominant limb, body mass index (BMI), sports activities, Tegner score, 55 and Marx activity score 36 participated in this study. Eligibility for the ACLR group required having a single ACLR that occurred within 2.5 years of participating in the study, completing rehabilitation, and being cleared to return to unrestricted activity. HC participants were targeted to match an individual in the ACLR group for sex, dominant limb, sport activity, and match an ACLR individual within ~2 units for age, BMI, Tegner, and Marx activity scales. HC participants had no previous lower-extremity surgeries, no time-loss lower body injuries within the previous year, no concussions in the last year, no known neurologic or lower body musculoskeletal disorder, and no pain during movement. All the participants signed a consent form approved by the institutional review board of Montana State University (protocol No. SM081818). One pair was omitted because they were an outlier regarding agreement in age compared with the rest of the pairs (3.8 years age difference compared with the mean age difference of 0.8 ± 0.6 years), leaving data for 35 matched pairs. This analysis is based on data collected in a single ~2.5-hour data collection.
Those with a primary ACLR were recruited from orthopaedic and physical therapy clinics in the Bozeman area. Matched healthy control participants were recruited from the university campus and surrounding community, including recreational and collegiate sports teams, local fitness centers, and teammates of enrolled ACLR participants. To support effective matching on key demographic and activity-level criteria, a prescreening survey was distributed widely, with approximately 1400 individuals responding. From these responses, control participants who matched the ACLR group on sex, age, dominant limb, BMI, sports activities, Tegner score, and Marx activity score were selected.
Jump-Land-Jump Task
A total of 75 reflective markers were attached to the participants to measure their whole-body motion. This marker set included a point-cluster distribution of markers on the thighs and shanks, covering a large area of the respective segments. It was designed to reduce the influence of soft tissue motion artifact on segment pose estimation.4,40 Four medial markers were removed (left/right medial femoral epicondyle, and the left/right medial malleolus) after capturing the static calibration trial. A 10-camera motion capture system was used to record the kinematic data at 250 Hz (Motion Analysis Corp) and 4 force plates to record ground-reaction force data at 1000 Hz (OPT464508-2K; Advanced Mechanical Technology Inc). Before starting the jump-landing protocol, participants did 2 sets of 8 bodyweight squats and 5 maximal effort vertical jumps as a warm-up. 3
For the jumping protocol, participants jumped from a 30-cm box over a distance of half of their height to land bilaterally on force plates, where they immediately performed a secondary bilateral jump in 1 of 3 directions (straight up, 45° to the right, or 45° to the left). 26 The movement was performed under 6 conditions. The convention of the condition abbreviation uses the first character to indicate the stimulus type (N, no stimulus; A, auditory stimulus; and V, visual stimulus). The second character indicates whether the condition was anticipated (A) or unanticipated (U). The third letter indicates whether participants’ gaze was fixed (F) at a fixation target in front of them, directed toward a visual-spatial memory (M) cue in front of them, or unconstrained so they could look down (D) at their landing area. Conditions included were as follows: (1) baseline (NAD, no cognitive task; anticipated direction; no visual gaze constraint); (2) baseline with visual constraint (NAF, same as NAD but with constraining visual gaze forward); (3) visual unanticipated with visual constraint (VUF, secondary jump direction cue (arrow) was presented ~250 ms before initial contact while looking at the fixation cross [Figure 1]); (4) auditory unanticipated (AUD, secondary jump direction verbal cue was completely played ~250 ms before initial contact [Figure 1]); (5) auditory unanticipated with visual constraint (AUF, same as AUD but with constraining visual gaze forward); (6) and visual memory16,56 (VAM, anticipated secondary direction with visual working memory task) (Figure 1). In addition, 250 ms of available time to react was chosen for unanticipated conditions to align with previous research16,26 and with evidence that available time to react being <300 ms facilitates jump landing tasks to be unplanned. 51 The visual constraint factor was chosen because of previous reports of altered visual reliance after ACLR23-25 and potential for visual stimuli to alter neuromuscular control. 24 The auditory component was chosen to enable decoupling of the visual constraint and rapid decision-making factors. The unanticipated factor was included because of the large body of literature identifying deleterious effects of rapid decision-making on knee mechanics,3,7,8,16,26,49 lack of literature on the response of those who had ACLR to rapid decision-making challenges during demanding sport movements, and evidence of visual-cognitive compensatory strategies after ACLR that could exacerbate cognitive-motor impairments in this clinical population. The visual memory task was used to decouple cognitive domain-specific effects (ie, visual-cognitive challenge from rapid decision-making versus working memory). Although additional conditions could be feasible, we chose this set of conditions because it targeted the factors of interest, provided several levels of control (eg, visual gaze vs stimulus modality), and was feasible to be completed within a ~3-hour collection period.

Jump-land-jump task progression for all conditions. AUD, auditory unanticipated; AUF, auditory unanticipated looking at the fixation; NAD, baseline, no visual constraint; NAF, visual unanticipated looking at the fixation; auditory unanticipated looking at the fixation; VAM, visual memory; VUF, visual unanticipated looking at the fixation.
Five successful trials for the “straight up” secondary jump direction were collected for each participant and condition (Supplemental Table 1). Successful trials were defined as those in which participants responded correctly to the cognitive task and both feet made contact with separate force plates (ie, feet did not share the same plate). The focus of analysis for this study was on the landing from the initial jump off the box for trials with a straight-up secondary jump direction. Five-trial averages for each biomechanical outcome variable for each condition and participant were used for statistical analysis.
Data Processing
Motion capture and force plate data were analyzed using Visual3D (HAS-Motion). Marker and force data were filtered using a fourth-order, zero-lag, low-pass Butterworth filter with a 15 Hz cutoff frequency. 30 Kinematic and kinetic data were computed using a Quasi-Newton optimization method and an inverse kinematics model. 33 The CODA pelvis definition was applied, and hip joint centers were estimated using the Visual3D implementation of the equations of Bell et al. 6 The knee and ankle joint centers were identified as the midpoints between markers placed on the femoral epicondyles and the malleoli, respectively. The lower extremity segments were defined with the z-axis oriented from the distal to the proximal joint centers, the y-axis pointing anteriorly, and the x-axis directed to the participants' right. An inverse kinematics model was employed, constraining lower-extremity degrees of freedom to 3 rotational degrees at the hip and knee and 2 rotational degrees at the ankle. 16 A Cardan x-y-z rotation sequence, corresponding to (+) flexion/(-) extension, (+) adduction/(-) abduction, and (+) internal/ (-) external rotation, respectively, was used to calculate the hip and knee joint angles. Net reaction moments were resolved within the proximal joint segment. For kinetic variables, forces were normalized to participant weight, and moments were normalized to both weight and height. Initial contact was defined as the first frame in which the force plate reading exceeded 10 N after the initial jump off the box. Custom MATLAB code Version R2022b (MathWorks) was used to calculate the second ACL injury risk factors and prepare outcome variables for statistical analysis.
Outcome Variables
Primary outcomes for the study were based on biomechanical predictors of second ACL injuries that were published at the time of design/onset of the present study. 46 To provide a more comprehensive understanding of biomechanical adaptations regarding cognitive-motor function after ACLR, additional outcomes were also included.
Primary Outcomes—Second ACL Injury Predictors
Previously reported biomechanical predictors of a second ACL injury were used as the primary outcomes. 46 Specifically, these outcomes were (1) uninvolved hip rotation net moment impulse during the initial 10% of landing (Uni-HRot-Imp); (2) knee extensor moment asymmetry at initial contact (KEM-Asym-IC) normalized to body weight and height, calculated as involved limb minus uninvolved limb variables (internal extensor moment defined positive, with more uninvolved extensor moments leading to negative values for KEM-Asym-IC); and (3) range of knee abduction angle for the involved limb, defined as the absolute difference between the maximum and minimum values from initial contact to the point of minimum center of mass (Inv-KAbA-range). In summary, the previous study 46 found that lower external rotation moments at the uninvolved hip, increased asymmetry in knee extensor moments at initial contact (indicating relatively lower extensor moments at the involved knee), and increased frontal plane knee motion were associated with a higher risk of sustaining a second ACL injury. These findings correspond to greater Uni-HRot-Imp and Inv-KAbA-range and lower KEM-Asym-IC values using our convention, which were interpreted as “risky” in our study.
Secondary Outcomes—General ACL Injury Risk Factors
Previous video analysis has identified additional biomechanical factors linked to primary ACL injuries that occur within the first 100 ms after initial contact with the force plate during jump landing tasks. 31 Three additional outcomes were added as secondary outcomes to provide a more complete evaluation of the data. Specifically, the secondary outcomes were peak knee flexion angle (pKFA), peak knee abduction angle (pKAbA), and externally defined peak knee abduction moment. Less knee flexion and increased abduction were interpreted as risky given their association with increased ACL loading.32,35,36
Exploratory Outcomes—Contralateral ACL Injury Risk Factors After ACLR
A post-hoc analysis, including biomechanical risk factors for contralateral injury after ACLR 28 that were reported during the progress of our study, was also incorporated for broader insight. Specifically, we included the mean of contralateral limb knee and hip flexion angles (CL-KFA and CL-HFA, respectively) during the portions of the stance phase of the initial jump landing that were delineated between the contralateral injured and the no contralateral injury groups. 28 To define the phases, variables were first normalized to 101 women corresponding to the initial contact to the minimum center of mass position (0%-100%). Then, time-normalized ranges of 14% to 94% for CL-KFA and 14% to 95% for CL-HFA were extracted. Additionally, vertical center of mass stiffness was calculated as the peak ground-reaction force measured from the force plate solely in contact with the contralateral limb during the stance phase, divided by the magnitude of change in the vertical position of the center of mass from initial contact to its minimum vertical position. Finally, contralateral limb contact time for the first jump (ie, elapsed time with ground-reaction force >10 N) was also included.
Power Analysis
GLIMMPSE (Version 3.1.3, SampleSizeShop.org) 29 was used for the power analysis to obtain 80% statistical power to detect within-within interactions of Group (ie, matched pairs) and condition factors with a repeated-measure design using the Hotelling-Lawley trace test. Given the paucity of data for our primary outcome variables across the novel set of experimental conditions of this study, we based our sample size on available, but sparse, information to inform expected group and condition means. Literature values from Paterno et al 46 were used as a basis for the baseline (NAD) condition estimates, with the previously published “first injury” and “second injury” group values used as approximations for anticipated baseline (NAD) performance for our HC and ACLR groups, respectively. We then scaled this clinically meaningful difference (ie, no injury vs second injury from Paterno et al 46 ) to inform group-specific condition estimates in response to visual gaze fixation, visual memory, and rapid decision-making challenges, with the ACLR group hypothesized to be more greatly impacted by visual and unanticipated difficulties. Standard deviation and covariance across groups and conditions were based on actual variability in our dataset. Percent changes for anticipated versus unanticipated conditions of 8% to 310% were within previously reported9,11 ranges (6%-370%). Specific inputs regarding the means and standard deviations used in the power analysis are provided in the supplemental content.
Statistical Analysis
The primary analysis was done using linear mixed-effect statistical models, with matched pairs as a random factor and group, condition, and group × condition interaction as fixed factors. The primary comparison of interest was in the group × condition interaction. Significance level was set at α = .0166 to account for multiple comparisons across 3 primary dependent variables (0.05/3). Dependent variables related to second ACL injuries were given the highest priority, with general and contralateral ACL injury risk factors included for additional context.
To evaluate the robustness of the findings from the primary analysis to statistical assumptions, we performed an additional sensitivity analysis using variations of this approach. Specifically, we included clinical and performance covariates (age, sex, height, time since surgery, Marx activity score, and jump height) and repeated the analyses (with and without covariates), with individual participants as random effects rather than matched pairs. Outcomes of the primary analysis are reported in the manuscript alongside a summary of the sensitivity analysis, with details of the sensitivity analyses provided in Supplemental Tables 4, 5, and 6.
Upon completion of the primary and sensitivity analyses, a post-hoc analysis was deemed necessary to evaluate potential additive effects that spanned primary and secondary outcome variables. A post-hoc multivariable analysis was done to provide greater context on the collective relationships. Specifically, the means of KEM-Asym-IC and pKFA were subtracted from individual values in their respective data sets. Then, these zero-mean data sets were normalized by their respective standard deviations, yielding z-scores for the 2 variables. The component z-scores were then averaged to obtain a composite outcome based on both KEM-Asym-IC and pKFA. The “riskiest” combined outcome corresponded to the most negative values, resulting from asymmetric extensor moments and decreased knee flexion. The post-hoc multivariable analysis is provided in Supplemental Tables 8 and 9.
Results
The available data included 210 means (35 participants × 6 conditions) for the HC group and 207 for the ACLR group, as 3 means were removed due to a taring issue with the force plates during the data collection. The total available dataset was based on approximately 97% of the total expected trials (Supplemental Table 1). The timing of the directional cues was verified in a post-hoc test (Supplemental Table 2). Paired t tests indicated no significant group differences for matched pairs in age, height, body mass, Tegner values, or Marx activity values between ACLR and HC groups (all P > .05) (Table 1).
Cohort Characteristics a

Data are presented as mean ± SD or number. Some participants played multiple sports. ACLR, anterior cruciate ligament reconstruction; HC, healthy controls.
For the primary outcome variables, the most robust finding was a significant group effect for KEM-Asym-IC (HC group, 0.005 ± 0.8 [% bodyweight–height]; ACLR group, –0.43 ± 0.82 [% bodyweight–Height]; P < .001) (Supplemental Table 3), with the ACLR group having greater asymmetry than the HC group (Table 2 and Figure 2). This finding persisted regardless of including covariates and using a paired versus unpaired analysis approach (Supplemental Table 4). Additionally, a significant group effect was observed for Uni-HRot-Imp for the primary analysis (HC group, 0.006 ± 0.003 [N.m.s/Kg]; ACLR group, 0.005 ± 0.004 [N.m.s/Kg]; P < .001) with the HC group having relatively more internal rotation moment (Table 2 and Figure 2); however, this result was sensitive to the statistical model and did not persist when using an unpaired analysis (Supplemental Table 4). There were no significant group and condition interactions for any primary outcome variables.

Left: Violin plots for the second ACL injury predictors for ACLR and HC groups for each condition. Right: Main effects of group showing ACLR and HC groups’ means and standard deviations for each second ACL injury predictor. The asterisk indicates significant differences. ACLR, anterior cruciate ligament reconstruction group; AUD, auditory unanticipated; AUF, auditory unanticipated with visual constraint; HC, healthy control group; NAF, baseline with visual constraint; NAD, baseline, no visual constraint; VAM, anticipated secondary direction with visual working memory task; VUF, visual unanticipated.
P Values for Linear Mixed Effect Models for the Second ACL Predictors a

Presented outcomes are based on statistical models with “pair” as a random effect and not including covariates. Bold P values indicate statistical significance. Inv-KAbA-range, range of knee abduction angle for the involved limb; KEM-Asym-IC, limb asymmetry in knee extensor moment at initial contact normalized to body weight and height; Uni-HRot-Imp, uninvolved hip rotation net moment impulse.
For the general ACL injury outcomes, the most robust finding was a significant condition effect for pKFA, in which a post-hoc test revealed a significant decrease in knee flexion for rapid decision-making conditions, with a range of 76° to 78°, compared with anticipated conditions, with a range of 79° to 80° for all participants, regardless of group (Table 3 and Figure 3). Other initially significant findings (group effects for pKFA and pKAbA) did not remain through the iterative statistical analysis (Supplemental Table 5).
P Values for Linear Mixed-Effect Models for General ACL Risk Factors a

Presented outcomes are based on statistical models with “pair” as a random effect and not including covariates. Bold P values indicate statistical significance. pKAbA, peak knee abduction angle; pKAbM: peak knee abduction moment normalized to body weight and height; pKFA, peak knee flexion angle.
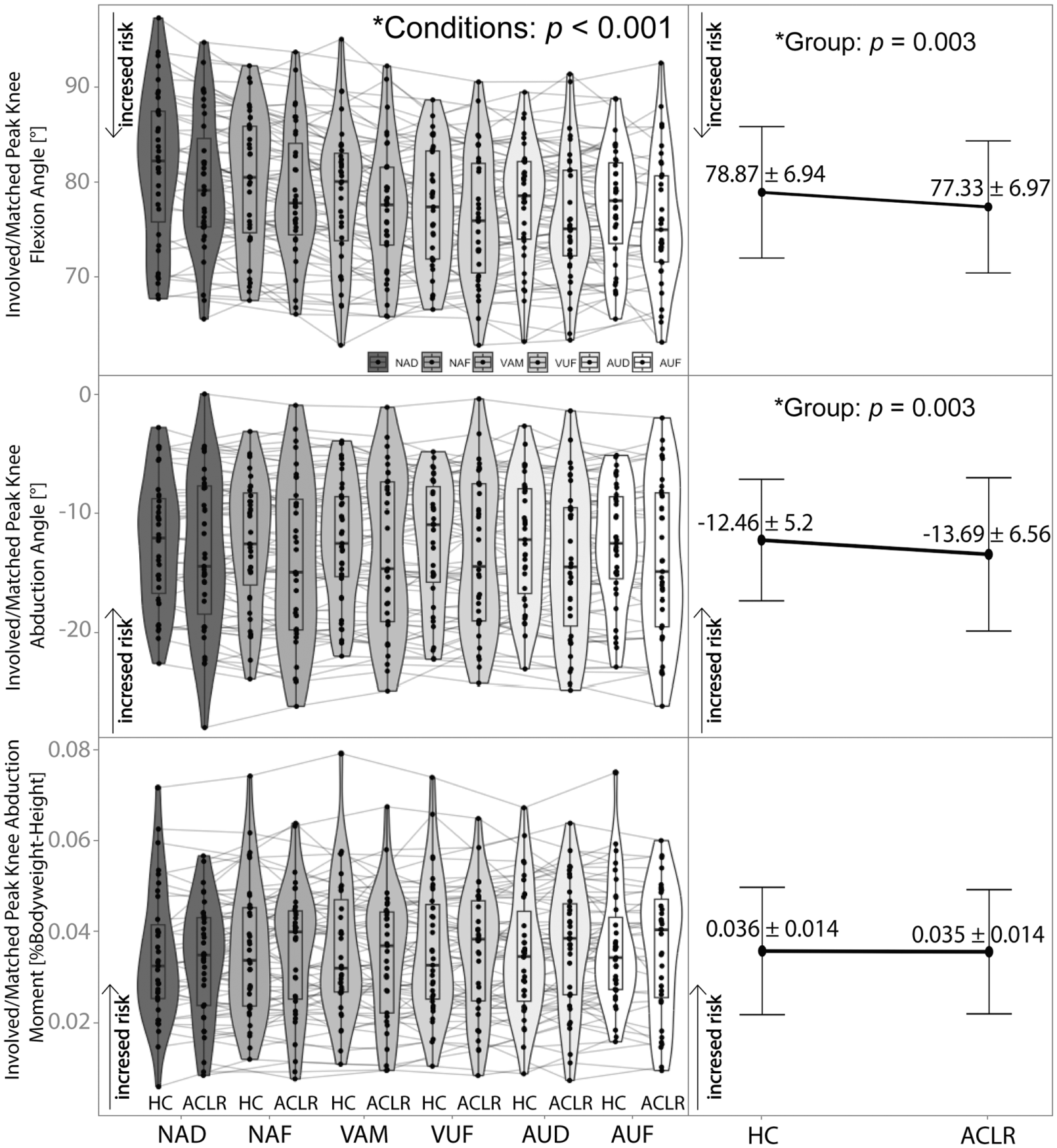
Left: Violin plots of ACLR and the HC group for means of each condition for primary ACL injury predictors. Right: Main effects of group for each primary ACL injury predictor (means and standard deviations). The asterisk indicates significant differences in conditions for pKFA.
For the exploratory outcomes, the most robust findings were a condition effect for all variables and a group effect for CL-HFA (Table 4, Supplemental Tables 6 and 7). Post-hoc analysis revealed that anticipated conditions had higher values for CL-KFA, CL-HFA, and contact time compared with cognitively challenging conditions. In contrast, the difference between conditions was opposite for vertical stiffness, with higher values for cognitively challenging conditions. For group differences, the ACLR group had more contralateral limb hip and knee flexion compared with the HC group (Table 4, Supplemental Tables 6,7). Other initially significant findings did not persist through the iterative statistical analysis (Supplemental Table 7).
P Values for Linear-Mixed Effect Model Analysis for Contralateral ACL Risk Factors and Multivariable Perspective of Injury Risk a
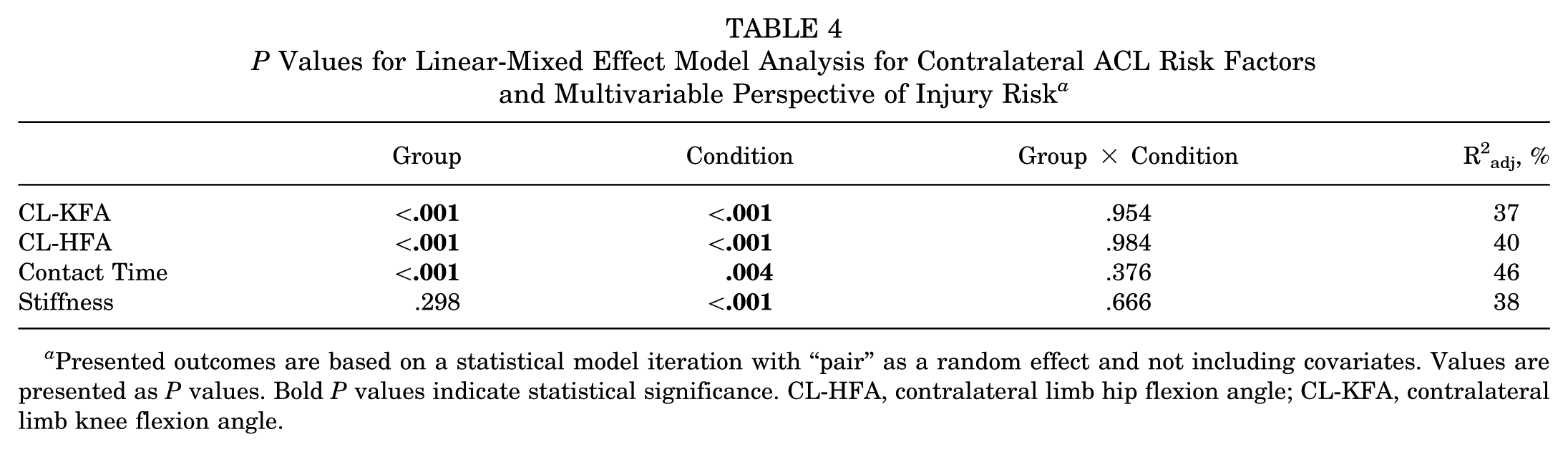
Presented outcomes are based on a statistical model iteration with “pair” as a random effect and not including covariates. Values are presented as P values. Bold P values indicate statistical significance. CL-HFA, contralateral limb hip flexion angle; CL-KFA, contralateral limb knee flexion angle.
The post-hoc multivariable analysis using a composite z-score derived from both pKFA and KEM-Asym-IC yielded significant group (P < .001) and condition (P = .002) effects, but not a group × condition (P = .28). The ACLR group had lower composite z-scores than the HC group (P < .001), and unanticipated conditions had lower composite z-scores than anticipated conditions (P < .03) (Table 4, Supplemental Tables 8–9).
Discussion
This study evaluated cognitive-motor impairments that persist after ACLR rehabilitation, even after RTS clearance was achieved using standard criteria. A robust group main effect, but not group and condition interaction, was detected, with the ACLR group demonstrating more asymmetry in knee extensor moments during landing compared with the HC group. Counter to our hypothesis, the primary outcomes were not impacted by the presence or absence of a cognitive challenge. In contrast, unanticipated conditions elicited a reduced pKFA for landing compared with anticipated conditions, regardless of group. Also, the unanticipated conditions caused significant differences for contralateral ACL injury factors when compared with conditions expected, with the most robust effect indicating increased contralateral hip flexion angle for the ACLR group, which has previously been linked to elevated contralateral injury risk. 28 Therefore, rapid decision-making may represent a particularly salient challenge to neuromuscular control. Further prospective studies are required to determine the different aspects of cognitive-motor function and the most meaningful sets of outcomes that can serve as a therapeutic target in assessing second ACL injury risk.
Findings across outcome variables suggest that a multivariable perspective may provide insight into high-risk scenarios. Considering the main significant findings, the ACLR group exhibited riskier loading patterns based on greater knee extensor moments asymmetry across all conditions. One plausible reason for the lack of a group × condition effect for this variable is that the asymmetric landing strategy was already demonstrated in the baseline conditions and may indicate that the ACLR group was already at a performance “floor,” making further increases in asymmetry less likely even under the other condition challenges. Alternatively, unanticipated conditions elicited reduced pKFA during landing patterns for both groups. The post-hoc test for pKFA revealed a significant decrease in this variable for rapid decision-making conditions compared with anticipated conditions for all participant regardless of their group. Notably, the interaction between group and condition was not significant, suggesting that the ACLR group did not demonstrate an exaggerated detrimental response to the unanticipated conditions. However, it may be insightful to consider that their effects could be additive. When considered concurrently from a multivariable perspective (ie, pKFA and KEM-Asym-IC on the same plot), the riskiest combination of outcome variables occurs for the ACLR group under unanticipated conditions (Figure 4). Therefore, even though unanticipated conditions elicit stiffer landing strategies for both ACLR and HC groups, this added effect may be particularly problematic for those in the ACLR group who already have other biomechanical patterns associated with second ACL injury risk (ie, asymmetric knee extensor moment) across a range of conditions.

Multivariable perspective of injury risk of the current dataset. pKFA and asymmetry of KEM-Asym-IC during anticipated and unanticipated conditions (means of 3 unanticipated conditions) for the ACLR and HC groups. Arrows indicate group-specific shifts in outcome variables between anticipated and unexpected situations. ACLR, anterior cruciate ligament reconstruction; HC, healthy control; KEM-Asym-IC, knee extensor moment at initial contact; pKFA, peak knee flexion angle.
Precedence for multivariate interactions in the context of ACL loading exists, where the most significant risk of ACL injury occurs from a combination of high knee flexion moments, knee compression forces, internal tibial torque, and knee abduction moments during movements such as jump landings or sudden direction changes. 5 However, future work is needed to validate the extent and nature of potential multivariable interactions with respect to second ACL injury risk. Alternatively, estimating loading in the ACL graft may enable more direct outcomes related to potential graft failure. 43 Despite ongoing opportunities to refine the outcome measures, the current findings provide novel data to support the potential value of cognitive-motor function as a therapeutic target to enhance rehabilitation outcomes after ACLR.
The riskier performance of the ACLR group compared with the HC group for KEM-Asym-IC at initial contact is consistent with previous research reporting that patients who underwent ACLR demonstrate high-risk knee mechanics even after RTS. An earlier study observed asymmetry in sagittal-plane knee moments at initial contact among participants who later suffered a second ACL injury compared with those who underwent ACLR but did not sustain a second injury within 1 year. 46 This observation highlighted that unbalanced force absorption strategies during the initial phase of the drop vertical jump task may contribute to an increased risk of future injuries. Our results extend this analysis to compare the ACLR group with the matched HC group, which indicates that those in the ACLR group still tend to adopt riskier landing strategies even after they are cleared to RTS. This finding further supports the potential need for further rehabilitation or more sensitive RTS testing to address these unresolved neuromuscular adaptations.
Previous research has shown that the risk of ACL injury to the contralateral limb is higher than to the ipsilateral limb. 59 Our exploratory analysis of contralateral limb ACL injury parameters aligns with findings from a previous study on male participants 28 that found that those with a contralateral ACL injury exhibited lower stiffness, longer contact time, and greater CL-HFA and CL-KFA. Similarly, our results showed that the ACLR group had higher CL-KFA and CL-HFA values and longer contact times compared with the HC group. However, unlike King et al, 28 we did not observe significant group differences in vertical stiffness. Instead, we observed that these stiffness values can vary by condition, with lower stiffness values in anticipated conditions compared with rapid decision-making conditions. These findings suggest that cognitive load may influence parameters related to contralateral ACL injury risk. Further studies are needed to determine whether these findings apply to a broader population and whether they align with the higher risk observed in the contralateral limb.
More recently, research has supported that adding a secondary cognitive task to drop jump landing on ACLR group assessments may enhance the identification of movement patterns linked to increased ACL injury risk and insufficient rehabilitation.39,53 Our study expanded these findings of reduced pKFA by showing the same results when adding not only visual cognitive challenges, but also auditory cognitive tasks during jump landing movement. Notably, rapid decision-making appeared to be the dominant challenge that elicited differences in pKFA, regardless of the directional cues being implemented with visual or auditory stimulus modalities. Decision-making and divided attention have been identified as key factors influencing several biomechanical risk factors for ACL injury. 27 Biomechanical adaptations in response to rapid decision-making in an ACLR cohort performing a jump landing task have also been reported by others. 53 The present study provides novel data supporting this point in the context of second ACL injury risk, with performance during rapid decision-making demands representing a particularly salient scenario to target rehabilitation and assessment efforts.
When considering Uni-HRot-Imp, we found a lower rotational impulse at the hip in the ACLR group compared with the HC group, corresponding with less risky biomechanics for the ACLR group. However, the significance of this finding was contingent upon the statistical analysis approach, specifically losing significance when using an unpaired analysis. Although many factors were intentionally matched, considerable person-specific variance cannot be completely accounted for in a case-control study design. The iterative statistical analysis aimed to evaluate the robustness of our findings to statistical assumptions, with robust findings being those that persisted regardless of assumption and inclusion of covariates. The source of the sensitivity of the Uni-HRot-Imp to the paired versus unpaired assumption is not known; however, it may be related to the enhanced statistical power of the paired analysis or other person-specific variability that is not adequately modeled through a paired design. In contrast, findings for KEM-Asym-IC were more robust, which may partially result from the KEM-Asym-IC outcome targeting asymmetry rather than a limb-specific metric. By comparing relative values between limbs, aspects of overall performance (eg, higher jump height) may be mitigated, supporting broader evaluation across ACLR and HC groups.
It is important to acknowledge the limitations of this study. We focused on specific jump landing tasks with a variety of cognitive challenges; however, these are not representative of all movements related to second ACL injury, including single-limb landings and cutting maneuvers. Notably, the group comparisons used in this study do not allow for potential patient-specific responses to be determined. For example, a subset of ACLR patients may demonstrate more detrimental responses to certain cognitive challenges, which are averaged out through group analyses. Future work that elucidates individualized injury risk profiles is warranted. Although the sample size was sufficient for this study's purposes, it may limit the generalizability of the findings. We examined second ACL injury predictors with high sensitivity and specificity from a previous study; however, these variables are now without their critiques (eg, unknown reliability of small knee extensor moments at initial contact, Supplemental Table 3). 46 Further research is necessary to investigate the ability of cognitive-motor function to predict injury recurrence and athletic performance prospectively, which is not feasible through our cross-sectional study design. However, our findings provide novel data to corroborate growing perspectives on the relevance of cognitive-motor function as an area that can augment ACLR rehabilitation efforts.12,21,47
Conclusion
The study results suggest that those in the ACLR group exhibit riskier biomechanics compared with those in the HC group during jump landing movements, regardless of the presence of additional cognitive challenges. Real-world demands, such as rapid decision-making, adversely influence landing kinematics. The extent to which these multivariable outcomes may compound injury risk after ACLR requires further research to more precisely understand the opportunities for neurocognitive challenges to impact ACLR return-to-sport assessment, ensuring that ACLR patients are adequately prepared for the demands of their sport environment.
Supplemental Material
sj-docx-1-ojs-10.1177_23259671251378761 – Supplemental material for Cognitive-Motor Function During Jump Landings After Anterior Cruciate Ligament Reconstruction
Supplemental material, sj-docx-1-ojs-10.1177_23259671251378761 for Cognitive-Motor Function During Jump Landings After Anterior Cruciate Ligament Reconstruction by Fatemeh Aflatounian, James N. Becker, Keith A. Hutchison, Janet E. Simon, Dustin R. Grooms and Scott M. Monfort in Orthopaedic Journal of Sports Medicine
Footnotes
Acknowledgements
The authors gratefully acknowledge the orthopaedic and physical therapy clinics in the Bozeman area for their invaluable assistance in participant recruitment. The authors also thank Ezekial Barden for his dedicated time and effort on this project.
Final revision submitted June 12, 2025; accepted July 8, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was funded by the Eunice Kennedy Shriver National Institute of Child Health & Human Development of the National Institutes of Health (award No. R03HD101093). This study was also supported in part by the United States Department of Defense Congressionally Directed Medical Research Program Peer Reviewed Orthopedic Research Program (research award No. W81XWH-18-1-0707) and the National Institutes of Health/National Institute of Arthritis and Musculoskeletal and Skin Diseases (R01AR076153, R01AR077248). The views expressed in this publication are those of the authors and do not necessarily reflect the official policy or position of the National Institutes of Health or the Department of Defense. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Montana State University (protocol No. SM081818).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.