
Abstract
Background:
Athletes regularly face physical and psychological adversities that test their resilience. Consequently, resilience may play a significant role in shaping athletes' performance and overall well-being. Therefore, resilience's influence on crucial outcomes within sports medicine, such as injury rates, recovery processes, and performance metrics, has sparked significant discussion and investigation.
Purpose:
To evaluate current literature on athletes' resilience and its effects on injury incidence, recovery, and athletic performance.
Study Design:
Systematic review, Level of evidence, 3.
Methods:
A systematic review was conducted following PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. This review utilized the PubMed, Embase, and Cochrane Library databases for literature search. The search was performed in December 2023 and initially identified 1387 studies. Relevant studies were selected based on defined inclusion and exclusion criteria, with data extraction focused on study characteristics, patient demographics, and key outcomes related to resilience. Due to heterogeneity in study design and outcome measures, qualitative analysis was performed rather than formal statistical analysis.
Results:
A total of 13 studies were included, consisting of 9 cross-sectional studies and 4 cohort studies. A total of 4400 athletes were included in these studies. A qualitative synthesis of the findings highlights resilience's significant positive impact on recovery and performance. Across the studies, high resilience was associated with better psychological well-being during recovery, reduced severity and incidence of post-concussion symptoms, and improved athletic performance. However, the effect of resilience on injury incidence was inconclusive, with studies showing varied results across different sports.
Conclusion:
This systematic review supports resilience as a crucial element in athletes’ recovery and performance, suggesting that resilience training should be integral to rehabilitation and athlete development programs. Future research should focus on implementing resilience training in athletic settings to evaluate its effects on injury incidence, recovery, and performance metrics. The evidence supports the potential of such interventions to enhance athletes' overall well-being and sporting success.
Resilience has garnered more attention in recent years regarding athletic performance and the overall well-being of athletes. In general psychology, resilience is often defined as the capacity to adapt positively to adversity and stressors.21,22 However, in the context of competitive sports, resilience must extend beyond psychological adaptability to encompass an athlete’s ability to recover from setbacks, maintain motivation, and perform optimally under pressure. Gupta and McCarthy 21 defined sporting resilience as an athlete’s ability to assess and regulate one’s thoughts, emotions, and actions in response to adversity to adapt and continue to perform at a high level. While this definition aligns with traditional psychological definitions of resilience, studies investigating resilience in athletes have varied widely in their definitions of resilience, especially in their usage of measurement tools, and the impact of resilience on injury incidence, recovery, and athletic performance. This makes a systematic review of the literature imperative to characterize the definition and impact of resilience in the context of athletics.
Athletes regularly face multifaceted challenges such as injuries, performance- and organizational-related stressors, and personal life obstacles.17,38 On top of grueling training schedules and high-stakes competition, these physical and psychological challenges present a unique challenge for athletes that test their mental fortitude, emotional balance, and physical readiness. Resilience is the ability to adeptly perform in the face of these obstacles while maintaining their well-being. 7
Injuries, for instance, are not merely physical setbacks but can profoundly affect an athlete's overall well-being. A recent study found that nearly 30% of baseball players displayed symptoms consistent with post-traumatic stress disorder.1,2 In another study, 42% of patients following anterior cruciate ligament (ACL) reconstruction were found to meet the criteria for major depressive disorder. 45 Previous studies have shown that as many as two-thirds of patients do not return to their preinjury level of sport by the expected 12 months after ACL reconstruction.4,6 This is despite showing recovery of physical-based measures by >90% of their preinjury level, indicating satisfactory surgical and functional outcomes. 4 This led to several studies investigating psychological factors that influenced return to sport, including psychological readiness to return, fear of reinjury, mood/emotions, locus of control, and recovery expectations, which are associated with returning to the preinjury level of the sport. Indeed, improved mental health and psychosocial factors have improved outcomes after ACL reconstruction.3,5,10,18,35,44 It has been well-established that athletes often attribute their identity and dedicate their daily routines to their sporting careers,8,11 so it is not surprising that injuries can profoundly affect athletes’ overall well-being and that mental health can affect recovery.
The primary impact of resilience on clinical outcomes in athletes has not been well-defined. Thus, the primary objective of this systematic review is to investigate the role of resiliency in the incidence of injury, recovery, and athletic performance. By analyzing the currently available literature, this study aims to establish the importance of implementing resiliency-building programs in rehabilitation and player development protocols to improve the overall well-being of athletes. We hypothesized that greater levels of resilience in athletes would be associated with lower injury incidence, faster recovery from injury, and improved athletic performance.
Methods
This systematic review of the current literature was performed in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. An electronic literature search was conducted in December 2023 utilizing the PubMed, Embase, and Cochrane Library databases. Example search terms included “resilience,” “resilience training,” “resilience program,” “athlete,” “recovery time,” “performance,” “resilience effects,” “resilience impact,” “sporting resilience,” and “resilience in sport.” Search terms were combined in various permutations and combinations using Boolean operators to maximize the identification of relevant studies. The reference lists of included studies were also screened to identify additional related studies.
Eligibility Criteria
All studies reporting the outcomes of resiliency in the context of sports were included in the screening. Studies measuring the effects of resilience in nonathletes, studies that measured or implemented resiliency in athletes but did not include follow-up assessment of the impact of the resilience, and studies that measured psychological factors in athletes but did not explicitly mention resilience were not included. The inclusion and exclusion criteria are provided in Table 1.
Eligibility Criteria

Data Management
After the initial search was performed, duplicate studies were manually identified. The studies were sorted by title in a spreadsheet, and studies with identical titles, authors, and publication years were identified and removed. After removing those, the remaining studies were independently screened by 2 reviewers (B.F.T., M.A.G.). Study eligibility was first assessed by screening title and abstracts against inclusion and exclusion criteria. Articles that passed the initial screen underwent full-text review to confirm eligibility. Following inclusion, both reviewers independently performed quality appraisal for each included study using the appropriate checklists. Disagreements at any stage were resolved through a third reviewer (M.A.M).
Data Collection
The following data were extracted: study characteristics (year, authors, institution, journal, and study design), patient demographics (age, sex, sport played, and level of sport), and mean follow-up (if applicable). The following outcome measures were collected: athletic performance, recovery time, injury incidence, the Connor-Davidson Resilience Scale (CD-RISC-10), and the Characteristics of Resilience in Sports Teams (CREST) scale.
Quality Assessment
The Joanna Briggs Institute (JBI) Critical Appraisal Checklist for Analytical Cross-Sectional Studies was used to assess the quality of the included cross-sectional studies and the risk of bias. 30 In addition, the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) cohort checklist was used for the included cohort studies to assess quality and risk of bias. 43
Results
Search Results
Searching the 3 electronic databases (PubMed, Cochrane, and Embase) relevant to this investigation identified 1387 records. After 73 duplicates were removed, 1314 articles remained. Of these, 1209 articles were excluded after title and abstract screening, and another 92 were excluded after full-text review. After applying all eligibility criteria, 1374 articles were excluded, and 13 were included for analysis (Figure 1). ‡ No additional records were identified after reviewing reference lists.

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart of the study selection process.
Patient Characteristics
A total of 4400 athletes were included in these studies (Table 2). Not including the studies by Ernst et al 15 and Yang et al, 47 which did not report a mean age, the overall mean age of the athletes was 30.9 ± 12.96 years old. Of the total, 69.4% athletes were male and 30.5% were female. The level of athletes ranged from recreational to professional, and the included athletes played a wide variety of sports.
Study Characteristics of Included Studies

Quality of Included Studies
The quality of the included studies was evaluated using the JBI Critical Appraisal Checklist for Analytical Cross-Sectional Studies (Table 3) and the STROBE cohort checklist (Table 4).
JBI Critical Appraisal Checklist for Analytical Cross-Sectional Studies Results a

JBI, Joanna Briggs Institute.
Item descriptions: 1 = inclusion criteria; 2 = description of study participants and setting; 3 = measurement of exposure validity and reliability; 4 = objectivity and standardization of measurement of condition; 5 = identification of confounding factors; 6 = methods to deal with confounding factors; 7 = valid and reliable measurement of outcomes; 8 = appropriate statistical analysis.
STROBE Cohort Checklist Results a
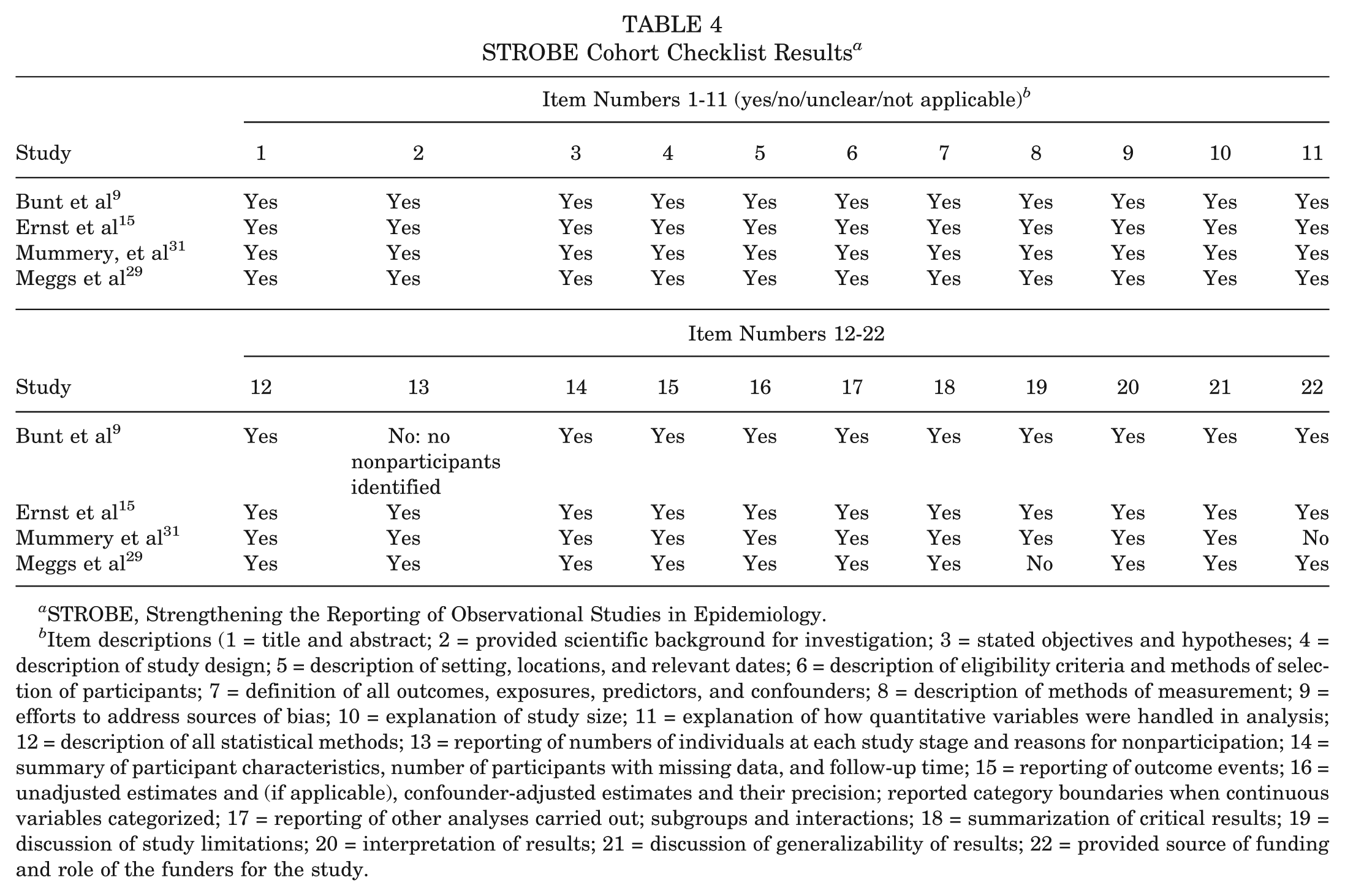
STROBE, Strengthening the Reporting of Observational Studies in Epidemiology.
Item descriptions (1 = title and abstract; 2 = provided scientific background for investigation; 3 = stated objectives and hypotheses; 4 = description of study design; 5 = description of setting, locations, and relevant dates; 6 = description of eligibility criteria and methods of selection of participants; 7 = definition of all outcomes, exposures, predictors, and confounders; 8 = description of methods of measurement; 9 = efforts to address sources of bias; 10 = explanation of study size; 11 = explanation of how quantitative variables were handled in analysis; 12 = description of all statistical methods; 13 = reporting of numbers of individuals at each study stage and reasons for nonparticipation; 14 = summary of participant characteristics, number of participants with missing data, and follow-up time; 15 = reporting of outcome events; 16 = unadjusted estimates and (if applicable), confounder-adjusted estimates and their precision; reported category boundaries when continuous variables categorized; 17 = reporting of other analyses carried out; subgroups and interactions; 18 = summarization of critical results; 19 = discussion of study limitations; 20 = interpretation of results; 21 = discussion of generalizability of results; 22 = provided source of funding and role of the funders for the study.
Injury Incidence
After assessing all of the relevant articles, resilience was investigated in terms of the incidence and severity of sports-related injuries, physical and psychological recovery after injury, and athletic performance. Of the available studies, only 3 looked at the relationship between resilience levels and the incidence and severity of sports-related injuries.16,24,34 The relationship between these variables remains unclear. Sanni’s 34 study investigated collegiate athletes who had suffered an injury that prevented them from playing their sport for ≥3 weeks. Measuring resilience with the CD-RISC-10, the study found no significant correlation (P > .05) between the athletes’ resilience levels and the severity of their injuries. The athletes missed varying amounts of time, and the study hypothesized that resilience is beneficial in the athletes’ recovery once they have suffered an injury, regardless of its severity. Still, they concluded that resilience did not reduce the severity of the injury itself. 34 Again measuring resilience levels via CD-RISC-10, Etayo-Urtasun et al 16 conducted a study involving ski mountaineers and found no significant difference (P = .28) in resilience levels between skiers who suffered injuries and the group that had not suffered injuries. In contrast, León-Guereño et al, 26 who also utilized CD-RISC-10, found a negative correlation (P < .05) between resilience levels and injury incidence in recreational runners. Runners with higher resilience levels were significantly less likely to suffer injuries. 26 Thus, the results regarding the impact of resilience on injury incidence vary, and if resilience does have an impact in reducing injury incidence, it may only be for specific sports.
Recovery
Regarding recovery, studies consistently highlighted how resilience facilitates a more favorable recovery experience, influencing both psychological well-being and physical rehabilitation.9,12,15,24,34 Sanni 34 used CD-RISC-10 to measure resilience in collegiate athletes of various levels (National Collegiate Athletic Association, National Association of Intercollegiate Athletics, and National Junior College Athletic Association) and found that athletes with higher resilience levels were more likely to possess beliefs conducive to recovery. In particular, they were more likely to believe that the treatment outlined by their health professional precisely outlined exactly what they needed to do to have a full recovery, that they had the self-efficacy to complete their rehabilitation program, and that they were less susceptible to reinjury. Resilience was also positively associated with the athletes’ perceptions that their overall rehabilitation process was effective in helping them return to sport. 34
Two separate studies by Jaiyeoba et al 24 and Codonhato et al 12 also used CD-RISC-10 to assess resilience levels in elite athletes. Both studies found that resilience was positively correlated with factors of recovery and negatively correlated with aspects of stress. Jaiyeoba et al investigated athletes in the National Sports Festival in Nigeria, while Codonhato et al investigated athletes in the Parana Open Games. However, they found that resilience positively correlated with recovery factors such as general well-being, sleep quality, fitness, success, physical recovery, and social recovery. Conversely, resilience was negatively correlated with stress factors, such as burnout, conflict, lack of energy, general anxiety, emotional stress, social stress, and somatic complaints.12,24
The significance of resilience in the context of sport-related concussions (SRCs) offers additional insights. The studies by Ernst et al 15 and Bunt et al 9 both found that lower resilience levels were associated with a more significant number and severity of postconcussion symptoms, as well as higher levels of mood symptoms, such as depression and anxiety. In addition, Ernst et al, utilizing CD-RISC-10, found that concussed athletes with lower levels of resilience had a more extended recovery period. In contrast, Bunt et al utilized the Brief Resilience Scale (BRS) to measure resilience levels in concussed athletes, which has a less comprehensive definition of resilience. The BRS is focused on resilience as the ability to recover quickly from stress, rather than as an overarching personality trait. However, Bunt et al had similar findings to Ernst et al, as they found that patients with lower resilience levels were less likely to report feeling back to normal after 3 months of recovery. Lower resilience was also associated with greater reaggravation of symptoms from physical and cognitive activity even when athletes had returned to sports/physical activity. While the other studies suggested that resilience provides athletes with traits and beliefs that improve their recovery process and speed, these 2 concussion-specific investigations distinctly quantified recovery duration and the number and severity of symptoms due to injury. They offered evidence that higher resilience tangibly shortens the path to recovery and lessens the amount and severity of symptoms due to injury.
Athletic Performance
While the amount of research into resilience’s effect on athletic performance is limited, the available literature suggests that resilience may improve performance, or at least the perception thereof. Yang et al 47 measured resilience with a scale developed by Shin et al 40 and found that resilience was positively correlated with perceived performance in taekwondo athletes, measuring perceived performance through a survey about their skills, timing to get points, and their actual performances in competitions. The study by Mummery et al 31 had similar results but did not utilize any scales to measure resilience. Instead, they labeled swimmers as resilient if they failed to beat their qualifying time for the national championship competition in the first event but managed to win it in the second. Swimmers who failed to beat their qualifying time in the first and second events were labeled as nonresilient because they could not overcome their first disappointing result. The researchers found that resilient swimmers had higher perceptions of their swimming endurance, but the study’s definition of resilience raises concerns about the validity of these findings. 31
The study by Meggs et al 29 also measured the resilience of swimmers, but they added a physiological dimension to the investigation by measuring the cortisol response of the swimmers before the race. They found a significant cortisol spike, suggesting that the race was stressful. They then used the Academic Resilience Scale, a validated questionnaire, to measure resilience levels and found a significant positive correlation with performance, meaning that more resilient swimmers achieved better times. 29 López-Gajardo et al 28 utilized the CREST scale to measure both individual and teamwide resilience. They reported that higher levels of individual and team resilience were positively correlated with perceived performance in soccer players and teams. Building on this, Hosseini and Besharat 23 found that athletes with resilience, based on CD-RISC-10 assessment, were positively correlated with sports achievement. Achievement was measured through a Sport Achievement Scale, which consists of 16 items for coaches to answer about their players’ sports achievements. This avoids any individual bias in asking athletes to self-rate their performance. The study found that coaches rated players with higher resilience as better performers.
Gameiro et al 20 offer a quantitative measure of athletic performance and its relationship to resilience. They utilized the CD-RISC-10 scale and measured performance based on the International Trail Running Association Performance Index, a scale that compares the performance of trail runners worldwide. The study found a significant positive association between resilience levels and performance rating.
Discussion
The findings of this systematic review provide valuable insights into the complex relationship between resilience and athlete well-being. The review investigated the impact of resilience on the incidence of injury, recovery after injury, and athletic performance. The evidence supports resilience’s beneficial effects on recovery and performance. Resilience plays a role in recovery from injury by helping athletes adopt a positive mindset about their recovery programs and encouraging them to follow their rehabilitation program closely. Higher resilience in athletes was also found to correlate with subjective and objective sports performance, emphasizing the importance of promoting resilience in recovering and actively playing athletes.
The finding that more resilient athletes are more likely to adopt positive feelings about their rehabilitation programs after injury is supported by Sarkar and Fletcher’s 36 resilience model, which suggests that athletes with high levels of resilience are more likely to demonstrate facilitative responses. The belief that their rehabilitation program is precisely what they need to do to recover and that they have the self-efficacy to accomplish that is critical for efficient recovery. Nonresilient athletes who disagree with their recovery programs or do not believe they can return to health may be less likely to make a total effort toward recovery. It is thus critical for sports medicine providers to provide resources and strategies for building resilience and self-efficacy in athletes during their recovery.
Moving forward, the observed associations between resilience and positive outcomes in injury recovery and athletic performance warrant the development and implementation of resilience training modules tailored for athletes. The positive association between resilience and recovery outcomes emphasizes the potential for resilience-based interventions to potentially shorten and enhance recovery protocols by integrating them into existing rehabilitation programs to support athletes' well-being and recovery. Moreover, the association between resilience and performance underscores the value of resilience training as part of broader player development programs to optimize performance under pressure and in the face of adversity, such as during performance slumps or playing in hostile away environments.
Numerous studies have developed resilience training programs across various fields, showing promise in enhancing resilience, performance, and well-being in the context of the workplace as well as academics.25,27,32,37 Despite these advances, research into the implementation and effectiveness of such programs within the context of athletics remains limited, albeit promising. A handful of studies have crafted resilience training programs specifically tailored for athletes. Solomon and Sun 41 implemented mindfulness training in elite football players and found that it successfully increased resilience compared with a control group. Similarly, Sullivan et al 42 developed a resilience training program for college student-athletes, and while the athletes’ knowledge of resilience skills did not significantly improve, their intention to use resilient coping strategies, such as seeking social support and self-control, significantly improved. This encouraging progress highlights the potential for resilience training programs to foster resilience and positively affect athlete recovery and overall performance.
Currently, no studies have implemented resilience training for athletes and longitudinally followed the athletes to assess the program’s effectiveness in increasing resilience and its impact on the athletes’ injury incidence, recovery, and performance. Future prospective studies should attempt to implement resilience training and measure these effects. However, there have not been many studies that developed their own resilience training programs, and of these studies, even fewer shared what the training consisted of. Therefore, this study synthesizes the existing literature to outline the important aspects of an effective resilience training program.
A resilience training program can be centered around 3 core components: cognitive and emotional restructuring, coping strategies, and social resilience reinforcement.
Cognitive and emotional restructuring focuses on modifying maladaptive thought patterns and developing effective coping mechanisms. An example of why this is important is that athletes who catastrophize setbacks are more likely to experience hindered rehabilitation and stronger pain response. 9 Therefore, training athletes to recognize and challenge destructive thought patterns such as catastrophizing, mainly through the A-B-C framework established by Ellis and Ellis, 13 aids in reshaping their explanatory styles toward more adaptive outcomes and reduces pessimism. Similarly, Ellis 14 created a resilience program to address various psychological factors in certain situations. This program attempts to improve upbeat personality and optimism through techniques such as Seligman et al’s 39 “3 Good Things,” which encourages athletes to identify and reflect on positive daily occurrences to foster a more optimistic outlook and gratitude, further shifting their explanatory styles away from pessimism. Athletes would also engage in structured goal setting, creating short- and long-term performance or rehabilitation goals to reinforce a sense of agency throughout the recovery process.
Coping strategies have been positively associated with resilience and are an essential component of stress regulation.33,46 Specifically, problem-focused and emotion-focused coping enables athletes to navigate adversity more effectively. 14 Athletes would be trained to use problem-focused coping, which emphasizes taking proactive steps to resolve the stressor itself. But they would also be equipped to utilize emotion-focused coping, which emphasizes managing the response to adversity. Emotion-focused coping strategies involve reframing negative experiences, practicing positive self-talk, and utilizing relaxation techniques. Additionally, exercises focusing on attention control and physiological regulation, such as mindfulness and breathing techniques, would be included to provide athletes with options to maintain focus and manage stress under pressure. 14
Although coping strategies are important to develop, sometimes athletes require mental health evaluation, with studies showing high rates of mental health problems that arise after injury. 2 In the studies reviewed, there was no regular follow-up with a mental health professional that was described. The introduction of questionnaires such as the Tampa Scale of Kinesiophobia and the Horowitz Impact of Event Scale–Revised, along with injury-specific scales such as the ACL Return to Sport after Injury scale, during the follow-up of major injuries is vital and can help identify individuals at risk of mental health problems after surgery. Future studies should attempt to implement resources for professionals that can help athletes cope following injury, and when appropriate, should include referral and regular follow-up with mental health professionals.
Research has shown that establishing mentorship and support groups within teams enhances perceived social support, 14 while perceived social support can influence an athlete’s appraisal of a stressful situation, thus affecting performance or recovery. 19 Furthermore, incorporating coping strategies that involve seeking social support enables athletes to navigate adversity more effectively. 14 To accomplish this, mentorship programs can be implemented, pairing athletes together to foster a sense of community, provide role modeling, and encourage discussion of fears and goals. This is especially critical in areas where sport psychologists are rare, emphasizing the importance of developing training programs that can be utilized by team members and support staff such as athletic trainers and coaches. Between the 3 core foci, there is enough information available to create a resilience training program that can be widely utilized.
Limitations
This study is not without limitations. Namely, the inconsistent measurement and definitions of resilience across studies have proven to be a challenge in making comparisons between studies and may contribute to the variability in findings for resilience research in athletes. It is also difficult to distinguish between lack of resilience and mental health conditions, as well as whether baseline mental health conditions can predispose to lack of resilience or vice versa. While these are likely interrelated, the scales used in this study were validated measures of resilience and are the best available metrics we can use to evaluate this. The CD-RISC-10 scale is the most widely used measurement, but it was designed for general populations, without taking into account the unique stressors that may be encountered in competitive sports. Other studies used the BRS, another scale designed for the general population rather than athletes. While the CREST scale was specifically designed for athletes, this further complicates the interpretation of resilience’s impact, as resilience in team sports is aided by factors that are not applicable to individual sports that were included in this study, such as swimming or trail running. Standardizing resilience assessment methods across studies is essential to determine the impact of resilience on athletes or whether previous findings reflect inconsistencies in measurement approaches.
Conclusion
This systematic review supports resilience as a crucial element in athletes' recovery and performance, suggesting that resilience training should be integral to rehabilitation and athlete development programs. Future research should focus on implementing resilience training in athletic settings to evaluate its effects on injury incidence, recovery, and performance metrics. The evidence supports the potential of such interventions to enhance athletes' overall well-being and sporting success.
Footnotes
Final revision submitted May 26, 2025; accepted July 8, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: C.S.A. has received royalties and consulting fees from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.