
Abstract
Background:
Although short- to mid-term clinical data of patients undergoing arthroscopic capsulolabral revision repair (ACRR) for recurrent anterior shoulder instability are promising, evidence pertaining to long-term functional, sports- and work-related outcomes is scarce.
Purpose/Hypothesis:
The purpose was to provide prospectively collected long-term functional outcomes, sports activity, and work ability of patients undergoing ACRR for recurrent anterior shoulder instability. It was hypothesized that patients would maintain significant functional improvement, along with sufficient sports activity and work ability, at a minimum follow-up of 20 years.
Study Design:
Case Series; Level of Evidence 4.
Methods:
Patients who underwent ACRR between September 1998 and August 2003 and had a minimum follow-up of 20 years were analyzed. Functional outcome measures included the Rowe and Constant-Murley (CM) scores, as well as the visual analog scale (VAS) for pain, which were collected preoperatively, at short-term follow-up (a minimum of 2 years), and at a minimum final follow-up of 20 years. The Single Assessment Numeric Evaluation and Simple Shoulder Test (SST) scores were only collected at the final follow-up. Return to sports and work—including sports and work level and discipline—were evaluated using a custom sports and work ability assessment tool.
Results:
A total of 29 patients (mean age at surgery, 28.6 ± 9.8 years) were included in the study, with a mean follow-up of 21.1 ± 1.5 years (range, 20-24 years). The rate of recurrent instability was 27.6% (n = 8), while 10.3% (n = 3) underwent revision surgery. In those without recurrent instability, the Rowe and CM scores showed significant improvements at both the minimum 2-year and minimum 20-year follow-ups, compared with preoperatively (P < .001, respectively). Neither the CM (87.9 ± 8 vs 83.4 ± 11; P = .055) nor the Rowe (86.7 ± 18.7 vs 86.9 ± 15.8; P = .958) score differed significantly between the minimum 2-year and 20-year follow-ups. At the minimum 20-year follow-up, the VAS pain score was 0.6 ± 1.6 at rest, was 1.1 ± 1.4 during exercise, and the SST (%) was 89.3 ± 13.5. The amount of activity (P = .022) and the subjective shoulder mobility (P = .021) significantly declined from the minimum 2-year to the 20-year follow-up.
Conclusion:
Patients undergoing ACRR for recurrent anterior shoulder instability had a recurrent instability rate of 27.6% at a minimum 20-year follow-up. Those patients without recurrence maintained significant improvements in functional outcomes and achieved a favorable postoperative sport activity and work ability.
Keywords
Capsulolabral repair for anterior shoulder instability has been shown to provide reliable clinical outcomes.13,26,29,37 However, even though arthroscopic instability repair techniques have improved over the last decades with outcomes comparable with those of open repair, there remains a significant risk of recurrence after the index surgical stabilization.13,15,16,19,23,31 Rates of recurrent shoulder instability after primary anterior capsulolabral repair have been reported to range between 4% to 60% of cases, while revision surgery is performed in up to 15% of these patients.14,20,38
The most common reasons for recurrent instability after open or arthroscopic anterior capsulolabral repair include bony glenoid defects, engaging Hill-Sachs lesions, capsular redundancy, and traumatic events.3,4,7,35 There is a strong consensus from a clinical1,30 as well as health economic standpoint, 24 that bone-block transfers such as the coracoid transfer according to Latarjet are a suitable procedure in this situation. Thus, in the absence of severe glenoid bone defects and engaging Hill-Sachs lesions, arthroscopic capsulolabral revision repair (ACRR) has been proposed as a suitable surgical approach, holding the advantages of anatomic labral repair, reduced morbidity, and simultaneous treatment of concomitant intra-articular pathologies.3,4,22,38
Previous reports—predominantly limited to short- to mid-term follow-up—have shown that patients undergoing ACRR achieved favorable functional outcomes, despite a concerning rate of recurrent instability of up to 41.5% of cases at a mean follow-up ranging between 1.8 and 5.8 years.4,12,14,20,21 While evidence at the long-term follow-up is available for bone block transfers in the management of recurrent instability,9,25,36 evidence pertaining to long-term functional outcomes, sports activity, and work ability of patients undergoing ACRR is scarce, given that the earliest attempts to manage recurrent instability after a failed Bankart repair via ACRR date back 25 years. 4 Such evidence on the long-term outcomes after ACRR may inform shoulder surgeons whether this procedure, performed for the right indication, may provide durable long-term results.
Thus, the purpose of the present study was to provide comprehensive, prospectively collected long-term clinical outcomes, including sports activity and work ability, of patients undergoing ACRR for recurrent anterior shoulder instability, with a minimum follow-up of 20 years. It was hypothesized that patients undergoing ACRR who did not experience recurrence would maintain significant functional improvement, along with sufficient sports activity and work ability, at a minimum follow-up of 20 years.
Methods
Patient Selection
The present study was approved by the institutional review board (IRB) of the Technical University of Munich before commencement (IRB approval No. 5197/11). Patients who underwent ACRR for recurrent anterior shoulder instability at a single institution after a failed index repair between September 1998 and August 2003 were prospectively analyzed.
Patients were included if they met the following inclusion criteria: recurrent anterior instability after open or arthroscopic capsulolabral repair with an anatomic index procedure (Bankart repair, transglenoid repair, or capsular shift), a glenoid bone defect of <20% of the inferior glenoid width measured intraoperatively, absence of an engaging Hill-Sachs lesion, and willingness to complete the rehabilitation program. A subpopulation of the patient collective was included in a previous study conducted at the institution. 4 Patients with nonanatomic index procedures (Bristow, Latarjet, Putti-Platt, Du Toit, Magnuson-Stack, or other bone bloc procedures) as well as those with concomitant full-thickness rotator cuff tears and multidirectional or voluntary instability were excluded from the study.
Patient characteristics as well as information regarding the index operative procedure, number of previous surgeries, time interval, history of recurrent instability, and hand dominance were collected from the medical records.
Patients were classified as those whose treatment failed if they experienced a recurrent subluxation, recurrent frank dislocation postoperatively, or underwent a revision procedure after discharge. Patients whose treatment failed were included in the descriptive reporting, reporting of minimal clinically important difference (MCID), patient acceptable symptom state (PASS), and failure analysis; however, they were excluded from the outcomes assessment. The decision was made to exclude these patients to precisely evaluate patient-reported outcomes, as well as sports- and work-related outcomes of the ACRR investigated, thereby avoiding confounding of the data with subsequent reconstructive procedures.
Surgical Technique
All surgeries were performed by a single surgeon (A.B.I.) with the patient in the beach-chair position using a 3-portal technique. The capsulolabral lesion and anteroinferior glenoid bone loss were inspected via the anterosuperior portal and graded accordingly. Measurements were performed using a calibrated probe via the posterior portal according to the bare-spot technique, as described by Burkhart and DeBeer. 8 ACRR was abandoned in the presence of significant glenoid bone loss of >20% of the inferior glenoid width8,10 or the presence of an engaging Hill-Sachs lesion in abduction and external rotation during dynamic intraoperative examination. 4
ACRR was performed according to a previously described technique4,15 (Figure 1). In brief, following the placement of the anterosuperior portal, an anteroinferior 5:30-o’clock portal was created with a switching stick, perforating the anteroinferior capsule bluntly under arthroscopic visualization.4,15 The retracted labrum and the scarred capsule were mobilized from the scapular neck down to the 6 o’clock position. Previous suture material and loose anchors were removed. The glenoid rim was then debrided using a shaver, and the anchor insertion sites were prepared with light decortication to allow healing of the capsulolabral complex. The first anchor was placed via the anteroinferior portal at the 5:30 o’clock position. The repair was then completed by placing additional anchors approximately 5 to 10 mm apart until the capsulolabral tissue was shifted and reapproximated enough to eliminate the anterior redundant capsular pouch. All anchors were placed about 2 mm from the articular rim. In all cases, titanium FASTak or Bio-FASTak anchors (Arthrex), loaded with nonabsorbable sutures (Ethibond No. 2, Ethicon; Arthrex), were used. Usually, 3 to 5 anchors were used, depending on the size of the lesion. 4
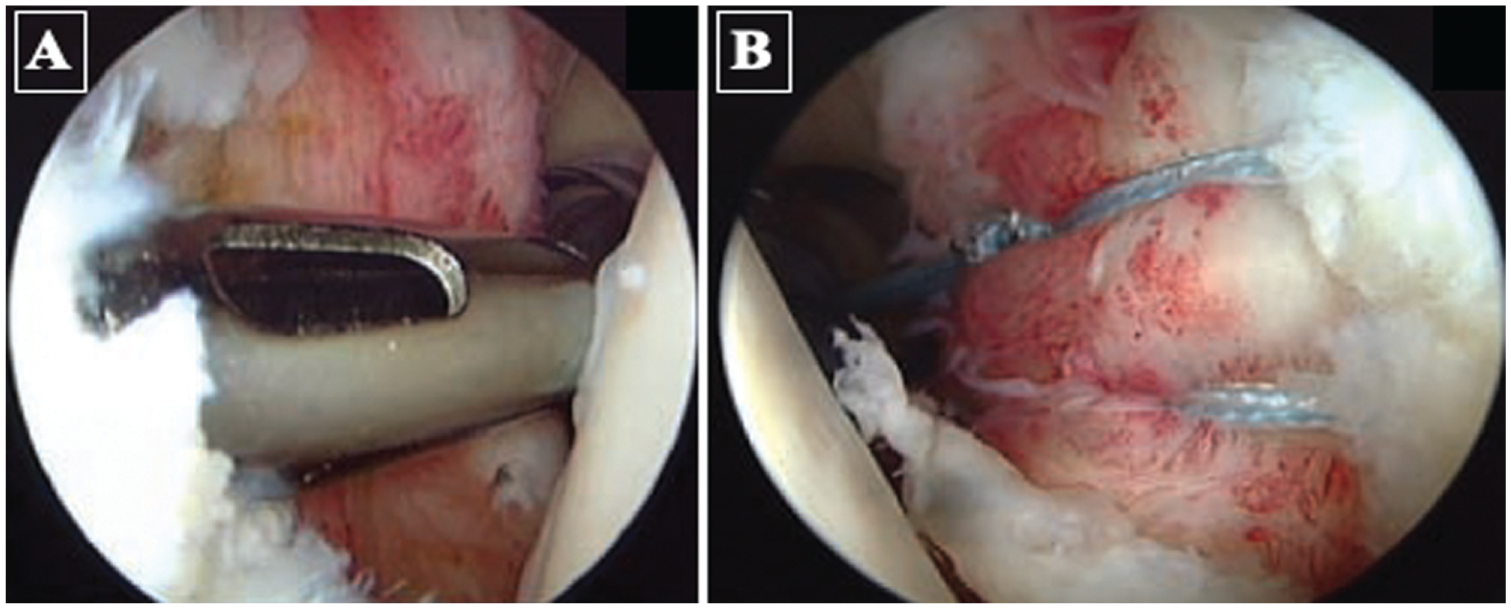
Capsulolabral repair technique. (A) Positioning of the lowest anchor via the 5:30 o’clock portal. (B) Capsulolabral repair with creation of an anterior capsulolabral bumper.
In patients with clinical signs of hyperlaxity or significant capsular laxity remaining after capsulolabral repair, an arthroscopic rotator interval closure was performed using 1 or 2 plication stitches that incorporated the anterior capsule, with the knots placed extracapsular. 4
Postoperative Rehabilitation
Postoperatively, patients were placed in a shoulder sling for 6 weeks, with external rotation restricted to 0° along with limitation of flexion and abduction to 90° during this period. After 6 weeks, free range of motion was allowed. As part of a staged rehabilitation program, patients started with passive exercises, subsequently progressing to active-assisted and active exercises. After 6 months, a return to sports activity was allowed.
Functional Outcome Measures
Functional outcome measures—including the Rowe, Constant-Murley (CM), and age-adjusted CM score—were collected preoperatively as well as postoperatively at short-term (minimum 2 years) and final (minimum 20 years) follow-ups, respectively.4,11,31 The CM was collected as previously validated by Boehm et al 5 based on self-evaluation by the patients. Additionally, the Single Assessment Numeric Evaluation (SANE), Simple Shoulder Test (SST), expressed as a percentage, the visual analog scale (VAS) for pain at rest and during motion (activities of daily living) were collected only at the final 20-year follow-up. 39 The MCID and the PASS were calculated for the Rowe score at the minimum 2-year and minimum 20-year follow-ups according to previously established threshold values (MCID, 8.9 points; PASS, 80 points). 27
These functional outcomes scores were the primary outcome measures of the study, while sports- and work-specific outcomes were also evaluated as secondary outcome measures. Outcomes, as well as recurrence and rerevision rates, were collected using a survey sent via mail.
Sport-Specific Outcomes
The sports activity level before the initial instability event, the level after the index procedure, the level at short-term, and the level at the final follow-up were evaluated using a custom-made sports activity assessment tool. The assessment tool 4 comprised the sports activity level (professional, semi-professional, or recreational), sports discipline (overhead sports, contact sports, or other sports), individual sports activity level (as a percentage), sports participation (days/week), patients’ subjective shoulder strength, mobility, and endurance compared with the prerevision status, and as a percentage of the preinjury status with full shoulder stability (100%).
Work-Specific Outcomes
The work ability level was evaluated before the initial instability event and at the final follow-up using a custom-made work ability assessment questionnaire. Patients were asked to indicate their occupation (eg, employment, self-employed, housework, retired, or unemployed) and their level of physical strain of their occupation according to the classification of the German Institute for Work Studies and Industrial Organization Association (REFA) (eg, occupation without specific physical strain or with either small, moderate, hard, or most heavy physical strain, as defined by specific criteria), both pre- and postoperatively and at the final follow-up. 17 Finally, the working ability from before the first instability event and at the postoperative state was compared, using an ordinal scale consisting of “excellent,” “good,” “satisfactory,” or “deteriorated.”
Statistical Analysis
Descriptive statistics—including the mean ± standard deviation for continuous variables and frequency and proportion for categorical variables—were calculated to characterize the study groups. The normality of the continuous data was assessed using the Shapiro-Wilk test. The t test or the Mann-Whitney U test was used to compare independent groups, and the paired t test or the Wilcoxon test was used to compare the paired preoperative and postoperative data, as statistically indicated by the distribution. Categorical variables were compared by performing the binary Fisher exact test or the chi-square test, as statistically appropriate. Results of the inferential analysis are presented as 95% CI. P < .05 was considered statistically significant. All statistical analyses were performed using commercial software, Statistical Package for the Social Sciences (SPSS; IBM).
Results
Between September 1998 and August 2003, 39 patients underwent arthroscopic revision repair for recurrent anterior shoulder instability after a failed index repair, of whom 10 patients were lost to follow-up. Finally, 29 patients were included in the final analysis with a mean follow-up of 21.1 ± 1.5 years (range, 20-24 years). The inclusion and exclusion process is detailed in Figure 2.

A flow chart visualizing the patient population for this study after accounting for the inclusion criteria, exclusion criteria, failures, and those lost to follow-up. PRO, patient-reported outcomes; FU, follow-up.
The index surgery was performed as an arthroscopic procedure in 20 patients (69%) and an open procedure in 9 patients (31%). Three patients had already received a second surgery at the time of the arthroscopic revision repair evaluated in this study, which had been performed arthroscopically in 1 patient and in an open fashion in 2 patients. Descriptive data are presented in Table 1.
Descriptive Data on Patient-Specific Variables, Indication, and Concomitant Procedures a

Continuous data are presented as mean ± SD, and categorical variables are presented as n (%).
Certain patients had undergone 2 stabilization procedures before the revision repair evaluated in this study.
Adequate trauma during contact sports, a forced external rotation, or a fall.
Noncontact overhead activity (throwing, volleyball, etc) or during activities of daily living with external rotation.
Intraoperative Findings
During arthroscopic revision surgery, Bankart lesions were observed in 21 patients, an anterior labral periosteal sleeve avulsion lesion in 6, a Perthes lesion in 1, and a dysplastic labrum in 1 patient. A humeral avulsion of the glenohumeral ligaments was not noted in any of the shoulders included. An additional partial supraspinatus tear was detected in 4 shoulders.
Based on a circle concept of 360°, the size of the capsulolabral lesion averaged 115° ± 39° (range, 30°-180°). In all cases (n = 29), the main pathologic changes were observed in the anteroinferior quadrant. In lesions >90°, a cranial extension of the lesion (eg, superior labrum anterior and posterior lesion) was observed in 4 patients, but no posteroinferior extension of the lesion was noted. Signs of capsular laxity were found in 6 patients (21%), and this was addressed by modifying the amount of capsular shift to restore physiological capsular volume.
A mean of 4 ± 0.8 anchors (range, 2-5) was used for the revision procedure. A persistent remaining capsular laxity was noted in 6 shoulders (20.7%), which was addressed by a closure of the rotator interval to reduce the capsular volume further.
Recurrence and Revisions
The rate of recurrent instability after the arthroscopic revision repair was 27.6% (8/29 patients). There were 5 (17.3%) frank shoulder dislocations caused by trauma and 3 (10.3%) subluxations caused by inadequate trauma. At the minimum 20-year follow-up, 3 patients (10.3%) had undergone a revision labral repair.
Functional Outcomes
Of the entire patient population, 23 patients (79.3%) had achieved the MCID of the Rowe score at a minimum of 2 years and a minimum of 20 years follow-up, respectively. Furthermore, 51.7% of the patients had surpassed the PASS of the Rowe score at a minimum of 2 years and 48.3% at a minimum of 20 years of follow-up.
The patient-reported outcomes (PROs) of patients who had not failed significantly improved at both the minimum 2-year and 20-year follow-ups, compared with preoperative values (P < .001, respectively (Table 2). Neither the Constant Score (P = .055), nor the age-adjusted Constant Score (P = .110), nor the Rowe Score (P = .958) differed significantly between the minimum 2-year follow-up and the minimum 20-year follow-up. No significant difference was observed between the SANE score of the operated shoulder and the SANE score of the nonoperated shoulder at the minimum 20-year follow-up (95% CI, –12.4 to 11.3; P = .917).
Patient-Reported Outcomes a

Data are presented as mean ± SD (range). Min, minimum; Preop, preoperative; PRO, patient-reported outcomes. P values indicate the difference in preoperative PROs at baseline compared with those at each follow-up time point.
At the minimum 20-year follow-up, the VAS pain at rest was 0.6 ± 1.6 (range, 0-6), while the VAS pain during exercise was 1.1 ± 1.4 (range, 0-5). Furthermore, patients reported an SST (%) of 89.3 ± 13.5 (range, 58.3-100) at the final 20-year follow-up.
A large majority (n = 20; 95%) of patients whose treatment did not fail indicated that they were either “satisfied” or “very satisfied” with the procedure, both at the minimum 2-year and the minimum 20-year follow-up (Table 3).
Presentation of the Patient-Reported Satisfaction Rate and Willingness to Undergo the Arthroscopic Capsulolabral Revision Surgery Again a

Categorical variables are presented as n (%). Min, minimum.
Sport-Specific Outcomes
All patients (100%) participated in sporting activities before the onset of shoulder instability. While all patients who did not fail (n = 21; 100%) returned to sports after surgery, 2 patients (11%) had discontinued activity at the minimum 20-year follow-up time point. A total of 17 patients (81%) had returned to their previous level of activity, with little or no limitation at the 2-year follow-up, compared with 42.9% (n = 9) at the 20-year follow-up. Overall, sports activity level was graded as 84% at the minimum 2-year follow-up and 62% at the minimum 20-year follow-up, compared with the activity level when the shoulder was stable (100%). Details pertaining to the patients’ subjective sports level are presented in Table 4.
Patients’ Subjective Sports Level Before Injury, After Index Surgery, and After Revision Surgery at Minimum 2-Year and Minimum 20-Year Follow-ups a

Categorical variables are presented as n (%). Min, minimum.
At the 20-year follow-up, a minimum of 10 (47.6%) patients returned to a lower level of competition or transitioned from overhead or contact sports to a lower-demand sports discipline. In those patients, at the minimum 2-year follow-up, the most common reason for decline was the operative shoulder (n = 6; 26%), followed by fear of recurrent instability (n = 5; 24%), while other reasons, such as the lack of motivation and time, were the most common reason at the minimum 20-year follow-up (Table 5).
Reasons for Decline in Athletic Activity After Surgery at 2-Year and 20-Year Follow-ups a

Categorical variables are presented as n (%). Numbers may not add up to the total study population, as not all patients experienced a subjective decline in activity. Min, minimum.
The patients reported sport-specific measures, including days of activity per week, hours per day of activity, amount of activity, strength, endurance, and mobility, at the 2-year and 20-year follow-ups, which were significantly lower than those preoperatively (Table 6). Most sport-specific measures did not differ substantially between the 2-year and 20-year follow-ups (days of activity per week, P = .912; hours per day of activity, P = .145; strength, P = .594; and endurance, P = .250). However, the amount of activity (P = .022) and the subjective mobility (P = .021) significantly declined from the minimum 2-year to the 20-year follow-up.
Patients’ Sport-Specific Measures Concerning Sports Participation, Subjective Strength, Endurance, and Range of Motion in the Shoulder Sport Activity Assessment Tool a

The data were collected at the preinjury level, during rehabilitation, at a minimum 2-year follow-up, and at the final 20-year follow-up. Continuous data are presented as the mean ± SD (range) from the minimum to the maximum. Min, minimum; Rehab, rehabilitation.
Furthermore, the patients longitudinally reported their involvement in different sport discipline categories after surgery (Table 7). Most categories did not show significant differences between the minimum 2-year and minimum 20-year follow-ups; however, participation in endurance sports was significantly higher at the minimum 20-year follow-up (Table 7).
Overview of the Sports Categories that Patients Participated in After the Revision Repair at the Medium- and Long-Term Follow-up a

The categorical variables are presented as n (%). Numbers may not add up to the total study population, as certain patients participated in >1 sports discipline. Min, minimum.
Overhead sports: Swimming, triathlon, tennis, throwing, golf, kayak, basketball, et cetera (etc).
Contact sports: Rugby, handball, judo, ice hockey, boxing, etc.
Alpine sports: Alpine ski, snowboard, touring ski, ice dancing, etc.
Endurance sports: Running, biking, aerobics, trampolining, hiking, horse-riding, classical dance, etc.
Ball sports: Soccer, etc.
Weight training at the gym or other sports: Weightbearing (climbing, bouldering, windsurfing, motocross, etc).
Shoulder-straining Sports: Table tennis, bowling, fencing, etc.
Work-Specific Outcomes
Patients reported the type of employment and physical strain in their work preoperatively and at the final 20-year follow-up after revision surgery, which did not change significantly over time. After surgery, patients retrospectively reported their working ability as “excellent” (n = 15; 71%) and “good” (n = 5; 24%), compared with the prerevision level, while none of the patients graded their working ability as “satisfactory” or “unsatisfactory.” The work-specific parameters are detailed in Table 8.
Work-Specific Parameters Assessed Preoperatively and at a Minimum 20-Year Follow-up a

Categorical variables are presented as n (%). Min, minimum; Preop, preoperatively.
Failure Analysis
According to the failure analysis, a young age at surgery was significantly associated with the failure of the ACRR procedure (P = .042). Factors such as hyperlaxity (defined as a positive Gagey test), the cause of recurrent instability, the number of dislocations after the initial surgery but before revision, frequency of activity per week, and hours of daily activity, along with the sports level before and during the pathology, and the physical strain load at work before the surgery. Preoperative PROs, such as the Constant-Murley Score and Rowe Score, were also not significantly associated with the outcome of the surgical procedure in terms of either its success or failure (P > .05, respectively) (Table 9).
Comparing the Preoperative Patient-Specific Parameters of the Success Group Versus the Failure Group After ACRR a
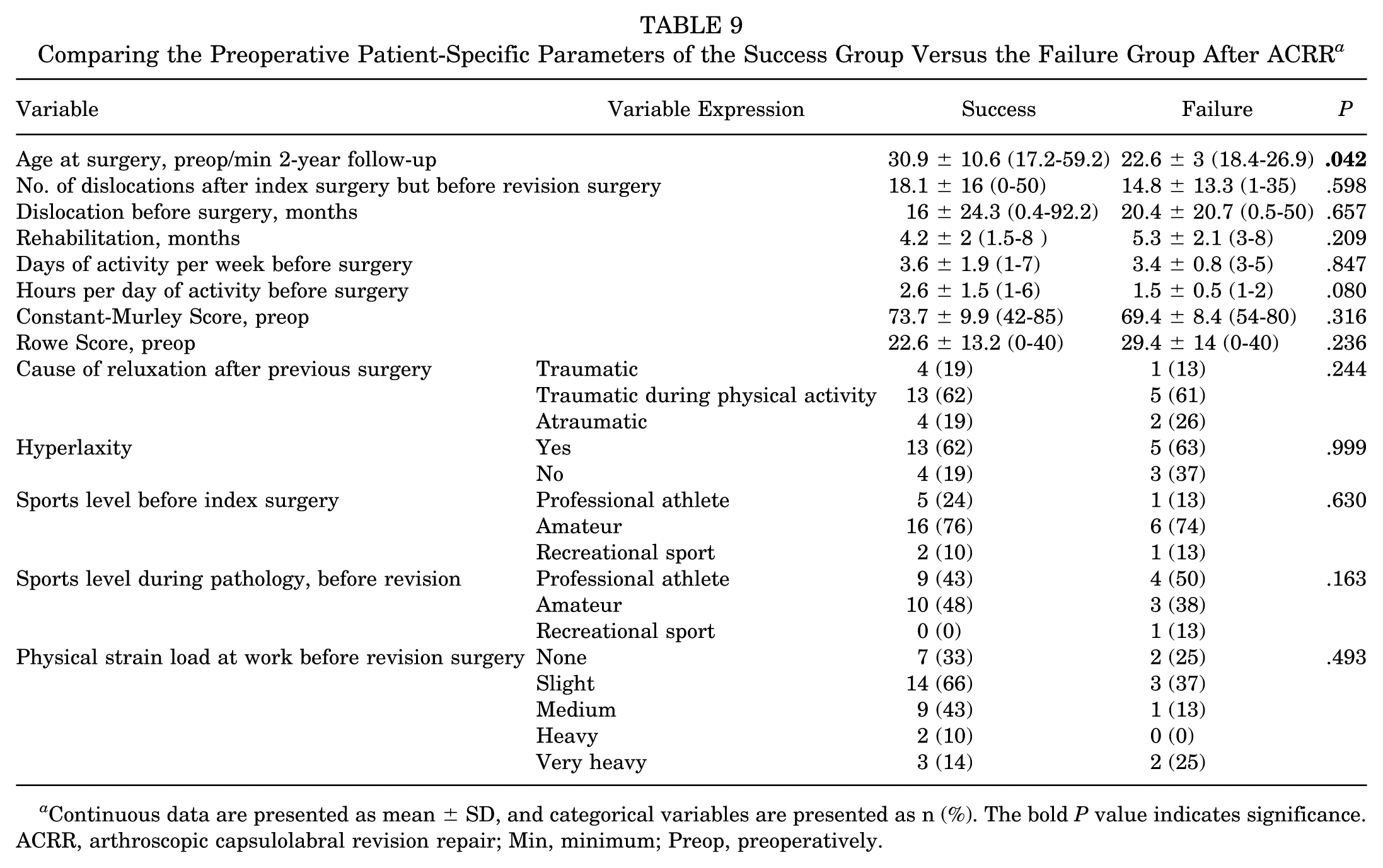
Continuous data are presented as mean ± SD, and categorical variables are presented as n (%). The bold P value indicates significance. ACRR, arthroscopic capsulolabral revision repair; Min, minimum; Preop, preoperatively.
Complications
In addition to the failures, 1 patient had a loose titanium anchor that was diagnosed on routine postoperative radiographs and was revised 1 day after the procedure. No additional neurologic deficits were observed after the revision procedure, especially regarding the axillary nerve.
Discussion
The most significant finding of the present study was that patients undergoing ACRR for recurrent anterior shoulder instability had a recurrence rate of 27.6% at a long-term follow-up of 21.1 ± 1.5 years, with 10.3% requiring revision surgery. Patients without recurrence maintained significant improvements in their functional outcomes. In these patients, functional outcomes significantly improved both at the minimum 2-year follow-up and at the minimum 20-year follow-up, compared with preoperative values, while there were no significant differences between the minimum 2-year and 20-year follow-ups. In addition, patients achieved a favorable postoperative shoulder function, including sports ability, activity, return to preinjury sports participation, and work ability. These findings, with follow-up of up to 20 years, are among the first to investigate ACRR at long-term follow-up and are consistent with previous studies reporting on clinical short- to mid-term outcomes. The present study further provides insights pertaining to remaining postoperative impairments during sports and work participation after ACRR.14,20,21
The high failure rate after primary anterior shoulder stabilizations underscores the need for high-level outcome studies after subsequent revision capsulolabral repair to manage patients’ expectations adequately.14,18,20,34,38 In a recent systematic review 14 analyzing clinical outcomes after ACRR, the authors found that 79.7% of patients reported experiencing good to excellent functional outcomes. Postoperatively, the included patients had a mean Rowe score of 84.2 (n = 191), a mean Constant score of 87.9 (n = 137), a mean SST score of 10.8 (n = 127), and a VAS score of 1.9 (n = 101). However, the follow-up in the included studies was only 3.1 years on average, ranging from 0.8 to 5.5 years. 14 Despite the significantly longer follow-up of patients in the present study with 21.5 years on average, the present functional outcome data are consistent with this previous work, including a mean Rowe of 86.9, a CM of 83.4, an age-adapted CM of 90, and an SST of 89.3 at the final follow-up. Notably, no significant difference was observed in PRO scores between the minimum 2-year and minimum 20-year follow-up periods. While a high fraction of the study population still had an improvement equivalent to the MCID both at the short- and long-term follow-up, only 48% of the patients still surpassed the PASS at the final follow-up. While this number may be artificially low because of the method of calculation of the MCID and the PASS that was applied, which automatically categorizes each patient with a new event of subluxation or dislocation as a failure to reach the MCID and the PASS, it highlights the complexity of this patient population, which already failed the index stabilization procedure.
Another important outcome measure for postoperative success is the assessment of return to sports and level of play after surgery, especially in these young and physically active patients, who are usually suffering from recurrent shoulder instability.2,6,21,28 In a systematic review 14 evaluating sports activity after ACRR, the authors found an overall return to sports rate of 78.5%, with only 47.5% of patients returning to their preinjury level of play. In addition, in a more recent systematic review comprising 7 studies with 153 athletes, Lau et al 21 showed that the weighted mean rate of return to play was 84% (range, 56.3%-100%) after a mean follow-up of 39.1 ± 8.3 months, while the reported time to return to play showed a weighted mean of 7.8 months (range, 5.7-9 months). Interestingly, in the 2 studies that differentiated the level of return to play, the overall weighted mean return to play rate was 96.8%, with a weighted mean of 69.7% returning to the same level and 27.3% returning to a lower level of play. These return to sports data are consistent with the findings pertaining to sports activity in the present study, in which all patients (100%) without failed treatments returned to sports after surgery. However, 47.6% of patients returned to a lower level of competition or changed from overhead or contact sports to a lower-demand sports discipline at the final 20-year follow-up. Interestingly, only the amount of activity and the mobility significantly declined from the minimum 2-year to the 20-year follow-up, while the remaining sport-specific measures remained similar over time.
When examining return to work and work ability after ACRR, the current literature remains very limited in terms of evidence.17,33 The present study found that most patients reported their working ability as “excellent” (71%) or “good” (24%), while all patients returned to work. In contrast, among a young military population, only 56% of patients returned to duty without recurrent instability after ACRR, while 44% experienced recurrent instability after returning to duty, which raises questions about the indication of ACRR in this subpopulation. 33 Interestingly, the similar amounts of glenoid bone loss between the successful (6.2%) and the failure (5.7%) group indicated that bone loss is not the primary determinant of failure in ACRR. 33 Interestingly, Kraus et al 17 evaluated incapacity of work after primary arthroscopic anterior shoulder stabilization and found that the overall mean incapacity of work was 2.7 months. At the same time, 17.5% of patients experienced problems completing their work, and 4.1% had to change their job postoperatively. Further, patients with low physical strains at work (REFA 0-1; 2.1 months) returned significantly earlier to work than those with a heavy workload (REFA 2-4; 3.4 months).
In a recent systematic review 20 that included 20 studies with a total of 531 patients undergoing ACRR, the authors reported that the recurrence of instability ranged from 0% to 41.5% of cases, with a mean follow-up of 39.5 months. More specifically, the weighted mean recurrent instability rate was 16%, along with a weighted mean revision surgery rate of 9%. In addition, Haskel et al 14 found an overall rate of recurrent instability of 26.2% of cases at a mean follow-up of 37.6 months. Interestingly, the number of previous surgeries and hyperlaxity have been shown to be significant risk factors for failure. 32 Further, the presence of off-track lesions, age >22 years, and ligamentous laxity has been described as independent predictors of recurrence. 34 In an analysis of a subgroup with these risk factors excluded, the failure rate dropped significantly from 42% to 19% of cases. 34 The rates of recurrent instability (27.6%) and revision surgery (10.3%) in the present study are consistent with these previous studies, despite the significantly longer follow-up of a minimum of 20 years. Notably, a young age at the time of surgery was significantly associated with failure of the revision procedure.
In general, previous studies on functional outcomes, return to sports, and failure and revision rates after ACRR have been limited to short- to mid-term follow-ups, ranging from 1.8 to 5.8 years.4,12,14,20,21 The present data offer insights into the long-term outcomes of patients undergoing ACRR, with functional scores, sports activity, as well as failure and revision rates being consistent with those of previous work. The data also demonstrated that patients were able to maintain sufficient outcomes over the period, from a minimum of 2 years postoperatively to the final follow-up, which averaged 21.5 years. However, this may in part be explained by the fact that patients may become less active and more conscious as they age, which may have influenced failure and revision rates.
Limitations
The study had several limitations. First, the sample size was limited due to the rarity of ACRR procedures at that time. Second, because of the radiation protection guidelines in place at the study site, radiographic imaging was not performed at either the minimum 2-year or the 20-year follow-up. Thus, the integrity of the repair or degenerative changes of the glenohumeral joint could not be assessed. Third, mobility and strength were subjective reports by the patient, rather than objective measures. Furthermore, of the patients who failed before the 2-year follow-up time point, not all patients agreed to participate in the 20-year follow-up. Finally, the retrospective assessment of preinjury data regarding the patients’ activity levels may pose a risk of recall bias.
Conclusion
Patients undergoing ACRR for recurrent anterior shoulder instability had a recurrent instability rate of 27.6% at a minimum follow-up of 20 years. Those patients without recurrence maintained significant improvements in functional outcomes and achieved a favorable postoperative sport activity and work ability.
Footnotes
Final revision submitted June 13, 2025; accepted July 1, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.B.I. is a consultant for Arthrex Inc, Arthrosurface-Anika, and medi GmbH & Co. KG and receives royalties from Arthrex Inc and Arthrosurface-Anika. B.S. is a consultant for Arthrex GmbH. S.S. is a consultant for Arthrex GmbH, KLS Martin Group, and medi GmbH & Co. KG. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Technical University of Munich before commencement (IRB approval No. 5197/11).