
Abstract
Background:
The optimal revision surgery for failed primary arthroscopic capsulolabral repair (ACR) has yet to be determined. Revision ACR has shown promising results.
Purpose:
To compare the functional, strength, and radiological outcomes of revision ACR and primary ACR for anterior shoulder instability.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Between March 2007 and April 2017, a total of 85 patients underwent ACR (revision: n = 23; primary: n = 62). Functional outcome scores and positive apprehension signs were evaluated preoperatively, at 1 year, and then annually. Isokinetic internal and external rotation strengths were evaluated preoperatively and at 1 year after surgery.
Results:
The mean follow-up was 36.5 ± 10.2 months (range, 24-105 months). There was no significant difference between the revision and primary groups in the glenoid bone defect size at the time of surgery (17.3% ± 4.8% vs 15.4% ± 5.1%, respectively; P = .197). At the final follow-up, no significant differences were found in the American Shoulder and Elbow Surgeons score (97.6 ± 3.1 vs 98.0 ± 6.2, respectively; P = .573), Western Ontario Shoulder Instability Index score (636.7 ± 278.1 vs 551.1 ± 305.4, respectively; P = .584), or patients with a positive apprehension sign (17.4% [4/23] vs 11.3% [7/62], respectively; P = .479) between the revision and primary groups. There was no significant difference between the revision and primary groups for returning to sports at the same preoperative level (65.2% vs 80.6%, respectively; P = .136) and anatomic healing failure at 1 year after surgery (13.0% vs 3.2%, respectively; P = .120). Both groups recovered external rotation strength at 1 year after surgery (vs before surgery), although the strength was weaker than in the uninvolved shoulder. In the revision group, a larger glenoid bone defect was significantly related to a positive apprehension sign (22.0% ± 3.8%) vs a negative apprehension sign (16.0% ± 3.2%; cutoff = 20.5%; P = .003).
Conclusion:
In patients with moderate glenoid bone defect sizes (10%-25%), clinical outcomes after revision ACR were comparable to those after primary ACR. However, significant glenoid bone loss was related to a positive remaining apprehension sign in the revision group. Surgeons should consider these findings when selecting their revision strategy for patients with failed anterior shoulder stabilization.
Recent developments in arthroscopic techniques and implants have led to arthroscopic capsulolabral repair (ACR) becoming a primary surgical treatment option for anterior shoulder instability, as it provides good clinical results comparable to the traditional open technique. Recurrent instability after primary ACR requires revision surgery, and several procedures have been used in this setting, such as open Bankart repair, the Latarjet or Bristow procedure, the Eden-Hybinette procedure, autogenic iliac crest bone grafting, and allogenic bone augmentation. 16,21,40,47,49 Revision ACR can also be performed, with reported recurrence rates of 8% to 22%. 24,29 Arthroscopic surgery is less invasive than open surgery, is associated with less pain, provides improved postoperative range of motion, and permits an inspection of the entire glenohumeral joint before proceeding with open surgery. 36 Furthermore, many studies 2,4,7,17,22,24,36 have described satisfactory outcomes from revision arthroscopic surgery after failed primary surgery. For example, Kim et al 22 prospectively evaluated 23 patients who underwent revision arthroscopic surgery after failed open or arthroscopic primary stabilization and reported reasonable rates of recurrence (22%) and return to sports at the preinjury level (78.2%). Franceschi et al 17 have also argued that revision arthroscopic Bankart surgery is a good treatment option for patients with glenoid bone defects of <30% after failed primary arthroscopic Bankart repair.
However, it is unclear whether revision arthroscopic surgery provides outcomes comparable to primary arthroscopic surgery, as few studies have directly compared the 2 procedures. 23,30 Krueger et al 23 compared primary and revision arthroscopic surgery in patients with glenoid bone defects of <25% and reported poorer subjective outcomes after revision arthroscopic surgery, although they did not compare radiological outcomes and muscle strength after surgery. The recovery of rotator muscle strength can be measured using the isokinetic muscle strength test, 35 and this parameter is important for evaluating functional outcomes and return to sports. 6,39
Computed tomography arthrography (CTA) is a valuable assessment tool after shoulder surgery, according to Farber and Buckwalter. 15 CTA shows high sensitivity and specificity in determining the condition before and after labral surgery. 10 Although CTA increases radiation exposure, it detects labral lesions with accuracy comparable to magnetic resonance arthrography and is cost-effective. 32
The purpose of this study was to evaluate whether revision and primary ACR provided comparable clinical outcomes (functional, strength, and radiological outcomes) among patients with moderate glenoid bone defect sizes. We hypothesized that revision ACR in patients with moderate glenoid bone defects would have outcomes comparable to primary ACR.
Methods
Patients
This retrospective study protocol was approved by our institutional review board, which waived the requirement for informed consent. We retrospectively identified 154 consecutive patients who underwent ACR for anterior shoulder instability at a single center between March 2007 and April 2017. The patients had undergone ACR for recurrent subluxations and apprehension during activities of daily living or sports because of instability or dislocations.
The inclusion criteria were as follows: (1) an anterior capsulolabral lesion confirmed on preoperative magnetic resonance imaging (MRI) or CTA, (2) a positive apprehension sign, (3) preoperative isokinetic muscle strength testing to evaluate rotator cuff strength, (4) glenoid bone defects of <25%, and (5) at least 1 year of follow-up to permit isokinetic muscle strength testing of rotator cuff strength and an evaluation of anatomic healing using CTA. The exclusion criteria were as follows: (1) bilateral involvement (n = 20 excluded), (2) open surgery (n = 2 excluded), (3) multidirectional instability (n = 4 excluded), and (4) loss to follow-up (n = 43 excluded). Therefore, the study included 85 patients: 23 in the revision group and 62 in the primary group.
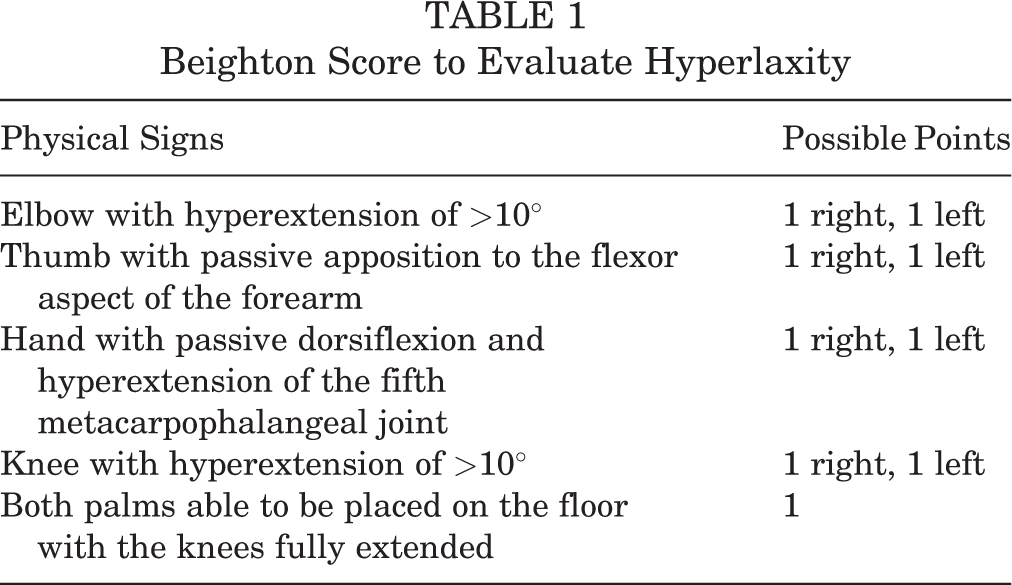
The patients’ medical records were searched to collect data regarding sex, age at surgery, age at first dislocation, number of dislocations, hand dominance, sports level (high [dynamic or contact sports], medium [static sports], or low [limited sports involvement]), and work level (high [heavy manual labor], medium [manual labor with less activity], or low [sedentary work]). 8,33 Hyperlaxity was defined as a Beighton score 3 of ≥4 on a 9-point scale (Table 1). We also evaluated concomitant superior labrum anterior to posterior (SLAP) lesions.
Beighton Score to Evaluate Hyperlaxity
Surgical and Rehabilitation Procedures
All patients underwent ACR in the lateral decubitus position by a single senior surgeon (J.H.O.) while their arms were pulled using a traction device (SPIDER Limb Positioner; Smith & Nephew) with an approximate weight of 4 kg. An additional lateral traction device was used to easily access the anterior capsulolabral structure. Then, 3 or 4 drill holes were made at 2- to 6-o’clock positions for the suture anchors, and a suture hook was passed through the capsule (1 cm distal and 1-2 cm lateral to the drill hole) for volume reduction. 28 The capsule and the anterior labrum (when present) were sutured and tacked down using 3 to 4 evenly spaced knotless suture anchors (Bioknotless [DePuy Mitek] and Bioraptor Knotless [Smith & Nephew]). All previously placed suture materials were removed during revision ACR. When the anchors in primary ACR were inserted into the scapular neck rather than in the over-the-top position or were not inserted at the 5-o’clock or 5:30 clock position, they were assessed as being in an inappropriate position. In revision ACR, the tissue quality was often poor, so the procedure was carried out more carefully when a suture hook was passed. In addition, we focused more on capsular plication than on labral repair. Otherwise, surgical principles and techniques were the same between primary and revision surgery, including the number or position of anchors.
Any glenoid bone fragment was always incorporated into the soft tissue shift. Rotator interval closure was performed according to the acromiohumeral distance on stress radiography. The rotator interval acts as a restraint to inferior translation of the humeral head in external rotation, 18 so we routinely checked the shoulder on stress radiography both in external rotation and in a neutral position to decide whether the rotator interval would be closed. In cases of a wider acromiohumeral distance on stress radiography in external rotation than in a neutral position, the rotator interval was regarded as incompetent, and we closed the rotator interval using an additional suture anchor. If Hill-Sachs lesions were consistently visible after ACR, arthroscopic remplissage was performed. However, arthroscopic remplissage was not performed in all patients in the present study. Patients who had a SLAP lesion underwent concomitant SLAP repair. The trans–rotator cuff portal was used to repair SLAP lesions with 1 to 2 knotless anchors. 34
Postoperatively, an immobilizing abduction pillow brace was applied for 6 weeks, and active-assisted shoulder range of motion exercises were initiated after the brace was removed. After the patient recovered full passive range of motion, shoulder muscle strengthening exercises were initiated at 3 months using a TheraBand (Hygenic). Return to sports was permitted after 6 months.
Functional Assessments
All patients completed assessments preoperatively, at 1 year after surgery, and then annually thereafter. The assessments included shoulder range of motion, the visual analog scale for pain, the American Shoulder and Elbow Surgeons (ASES) score, and the Western Ontario Shoulder Instability Index (WOSI). Passive shoulder range of motion measurements were obtained using a goniometer (forward flexion, external rotation at the side), and internal rotation at the back was identified based on the vertebral level that corresponded to the patient’s thumb placement (1-12 for thoracic vertebrae, 13-17 for lumbar vertebrae, and 18 for the sacrum). Each follow-up appointment included evaluations for recurrence, the apprehension test, and return to preoperative sports level. For the apprehension test, the patient’s scapula was placed on the edge of the table in the supine position with the elbow at 90° and the shoulder abducted to 90°. A positive apprehension sign was considered when the patient felt apprehension after external rotation force was gradually applied in this position. All functional assessments, including the apprehension test, were performed by a clinical researcher who was blinded to whether the patient had undergone primary or revision ACR.
Isokinetic Muscle Strength Testing
Isokinetic muscle strength was evaluated using a System 3 PRO (Biodex Medical Systems) at 1 week preoperatively and at 1 year after surgery. The patient assumed a seated position and was restrained using 2 bands across the chest and shoulders to minimize unnecessary movements. The test was performed with the shoulder in a neutral position, abduction of 45° in the scapular plane, and elbow flexion of 90°. Peak torque (PT) was measured with a 60-degree/s load during external rotation and internal rotation, and the value was normalized to the patient’s body weight (N·m/kg). The PT deficit (PTD) was calculated as PT of the uninvolved shoulder minus PT of the involved shoulder. The PT ratio (PTR; the ratio of PT during external rotation to PT during internal rotation), which reflects rotator cuff muscle balance and stability, was calculated for the involved shoulder. 9,12,14,19,48 The PTR range is typically 0.57 to 1.19 in different populations, 44 and values of 0.66 to 0.75 (2:3 to 3:4) are recommended to prevent shoulder injuries. 14
Radiological Assessment
The proportion of glenoid bone defects was calculated using the best-fit circle method, which compares the diameter of the affected region to the normal glenoid diameter using the en face view on MRI or CTA. 45 Hill-Sachs lesions were evaluated using axial MRI or CTA and were classified as an engaging or nonengaging lesion based on the system proposed by Di Giacomo et al. 11 A nonengaging Hill-Sachs lesion is considered within the glenoid track, whereas an engaging Hill-Sachs lesion is considered outside the glenoid track. There were 2 fellowship-trained shoulder surgeons (Y.D.J. and H.S.K.) who separately evaluated the radiological measurements, and repeated measurements were collected approximately 6 weeks later. Interobserver and intraobserver reliability was assessed for the radiological measurements. Healing of the anterior capsulolabral complex at 1 year after surgery was evaluated using CTA. Healing was assessed by a senior musculoskeletal radiologist with over 15 years of expertise who was blinded to whether the patient had undergone primary or revision ACR.
Statistical Analysis
Categorical variables were compared using the chi-square test, and continuous variables were compared using the independent t test, paired t test, or Mann-Whitney U test, as appropriate. Intraobserver and interobserver reliability of the radiological measurements was evaluated using Cohen kappa values for categorical variables (>0.8 indicated excellent reliability) and intraclass correlation coefficients for continuous variables (>0.8 indicated excellent reliability). All statistical analyses were performed using SPSS software (version 25.0; IBM), and differences were considered statistically significant at P values of <.05.
Results
Demographic Characteristics
The 85 study patients had a mean age at the time of surgery of 30.4 ± 9.1 years (range, 15-43 years) and a mean follow-up period of 36.5 ± 10.2 months (range, 24-105 months). The mean age at the time of the first dislocation was 20.1 ± 7.8 years (range, 15-42 years), and the mean number of dislocations/subluxations was 10.2 ± 8.7. The revision group included 21 men and 2 women, while the primary group included 47 men and 15 women. All patients in the revision group had their primary procedure performed elsewhere.
The revision group was significantly older at surgery (mean, 34.5 ± 8.2 years [range, 23-43 years]) than the primary group (mean, 25.3 ± 7.5 years [range, 15-35 years]), although there were no other significant differences in the demographic characteristics and no significant between-group differences in clinical characteristics (Table 2). Among the patients with concomitant SLAP lesions (revision: n = 13; primary: n = 30), SLAP repair was performed in 3 (23.1%) patients in the revision group and 11 (36.7%) patients in the primary group (P = .491).
Demographic and Clinical Characteristics of Study Patients (n = 85) a

a Data are reported as mean ± SD unless otherwise stated. Bolded P value indicates a statistically significant difference between groups (P < .05). ACR, arthroscopic capsulolabral repair; SLAP, superior labrum anterior to posterior.
b After primary surgery.
Among the 23 patients in the revision group, the mean time from primary surgery to revision surgery was 3.4 ± 1.8 years (range, 1-7 years), and the mean number of dislocations after primary surgery was 11.8 ± 6.1 (range, 4-20). The reasons for primary ACR failure were new trauma (n = 16; 69.6%), inappropriate anchor positioning (n = 4; 17.4%), hyperlaxity (n = 2; 8.7%), and use of <3 anchors (n = 1; 4.3%). In patients with hyperlaxity without other reasons for failure (eg, new trauma or surgical technique problem), hyperlaxity was considered as the cause of recurrent instability.
Functional Outcomes and Recurrent Instability
At 1-year follow-up, patients in both groups exhibited slightly reduced but nonsignificant range of motion postoperatively compared with preoperatively, and there were no significant differences between the groups on any functional outcome measure (Table 3). In addition, the ASES and WOSI scores in the revision group did not vary according to the reason for primary surgery failure. No recurrent dislocation was observed at the final follow-up in either group; subluxations occurred in 2 of 23 (8.7%) in the revision group and 7 of 62 (11.3%) in the primary group (P ≥ .999). Because there was no subluxation affecting activities of daily living, all patients underwent nonoperative treatment with rotator cuff muscle strengthening. Patients in the revision group tended to be more likely to have a positive apprehension sign at the final follow-up (4/23 [17.4%] vs 7/62 [11.3%], respectively; P = .479) (Table 3). Of the 7 patients in the primary group with a positive apprehension sign, 2 (28.6%) had hyperlaxity; there was no difference in the positive apprehension sign according to the presence of hyperlaxity.
Functional Outcomes a

a Data are reported as mean ± SD unless otherwise stated. ACR, arthroscopic capsulolabral repair; ASES, American Shoulder and Elbow Surgeons; deg, degree; VAS, visual analog scale; WOSI, Western Ontario Shoulder Instability Index.
b Vertebral level that corresponded to the patient’s thumb placement.
Isokinetic Muscle Strength
The results of isokinetic muscle strength testing are shown in Table 4. The PTD during external rotation did not improve in either group at 1 year after surgery; however, the PTD during internal rotation improved significantly in both groups (revision: from 11.9% ± 21.0% to 1.2% ± 23.4% [P = .032]; primary: from 12.0% ± 22.5% to 0.9% ± 26.6% [P = .012]). The amount of improvement was not significant between the 2 groups (P = .356). In addition, the PTR of the involved shoulder improved significantly in both groups (revision: from 0.99 ± 0.19 to 0.78 ± 0.19 [P = .030]; primary: from 0.89 ± 0.27 to 0.74 ± 0.18 [P = .001]). The difference between the 2 groups was not statistically significant (P = .493) (Table 4).
Isokinetic Muscle Strength Results a

a Data are reported as mean ± SD. Bolded P values indicate a statistically significant difference (P < .05). ACR, arthroscopic capsulolabral repair; PTD, peak torque deficit; PTR, peak torque ratio.
b Comparing the same group preoperatively versus at 1-year follow-up.
c Comparing the revision and primary groups at 1-year follow-up.
Radiological Outcomes
All radiological findings had excellent interobserver and intraobserver reliability. Preoperative glenoid bone defects were considered moderate in the revision group (mean, 17.3% ± 4.8% [range, 10%-25%]) and the primary group (mean, 15.4% ± 5.1% [range, 0%-25%]). The difference between the 2 groups was not statistically significant (P = .197). CTA at 1 year after surgery revealed that anatomic healing failure of Bankart lesions tended to be more common in the revision group than in the primary group (3/23 [13.0%] vs 2/62 [3.2%], respectively; P = .120). No arthropathy was found in either group.
Positive Apprehension Sign and Glenoid Bone Defects
In the revision group, the 4 patients with a positive apprehension sign at the final follow-up had larger glenoid bone defects than the 19 patients without a positive apprehension sign (22.0% ± 3.8% vs 16.0% ± 3.2%, respectively; P = .003). However, no difference in the glenoid bone defect size according to a positive apprehension sign was seen in the primary group (16.3% ± 4.0% vs 14.1% ± 6.2% in those with a positive and a negative apprehension sign, respectively; P = .663) (Figure 1). The cutoff value for a glenoid bone defect to predict a positive apprehension sign in the revision group was 20.5% (sensitivity: 75.0%; specificity: 94.7%; area under the curve, 0.895 [95% CI, 0.712-1.000]) (Figure 2).

Comparison of patients with and without a positive apprehension sign. A significant difference in the glenoid bone defect size was found in the revision group (22.0% ± 3.8% vs 16.0% ± 3.2% for positive and negative apprehension signs, respectively; P = .003) but not in the primary group (16.3% ± 4.0% vs 14.1% ± 6.2%, respectively; P = .663).

Receiver operating characteristic (ROC) curve of glenoid bone defects in the revision group. The cutoff value for a positive apprehension sign was 20.5% (sensitivity: 75.0%; specificity: 94.7%; area under the curve, 0.895 [95% CI, 0.712-1.000]).
Discussion
The present study revealed satisfactory functional outcomes at the final follow-up for the revision and primary groups. Both groups exhibited improved PTR values for the involved shoulder at 1 year after surgery, with similar rates of anatomic healing failure (3/23 patients in the revision group and 2/62 patients in the primary group). There was no recurrent dislocation after surgery in both groups, and the rates of positive apprehension signs were not different (17.4% in the revision group and 11.3% in the primary group). However, unlike in the primary group, a larger glenoid bone defect was related to a positive remaining apprehension sign in the revision group (22.0% ± 3.8% vs 16.0% ± 3.2% for negative apprehension sign; cutoff = 20.5%; P = .003). Therefore, revision ACR seems to be an acceptable option in patients with moderate glenoid bone defect sizes.
Yon et al 52 reviewed 14 articles and 339 patients who underwent revision ACR and reported that 15.3% of patients experienced recurrent instability, including positive apprehension signs and dislocations. Another systematic review revealed a recurrence rate of 14% to 21% after primary ACR, 27 and Murphy et al 31 reported rates of 31.2% for recurrent instability and 17% for overall revision at >10-year follow-up after primary ACR. The present study revealed a positive apprehension sign in 17.4% of patients in the revision group, which agrees with the results reported by Yon et al, 52 although various studies 2,6,17 in that systematic review excluded patients with a glenoid bone defect of >20%. In the present study, there was no dislocation, and good results were obtained. We focused more on capsular plication rather than labral repair during revision ACR, and it is thought that the emphasis on external rotator strengthening exercises may have affected the good results. Also, the fact that the mean age of the patients in the revision group was 34.5 years and that they showed a relatively low activity level suggests that there was a possibility of no dislocation.
Revision surgery for recurrent shoulder instability can be performed using various strategies, which include open capsulolabral repair, ACR, and bony procedures. 16,24,29,40 However, the optimal strategy for revision surgery remains controversial because there are no related prospective randomized controlled studies. Kim et al 22 performed a prospective nonrandomized study and reported satisfactory results at an average follow-up of 21 months after revision arthroscopic Bankart surgery. We are also only aware of one study that has directly compared arthroscopic and bony procedures as revision surgery, which was performed by Elamo et al 13 (revision surgery using arthroscopic Bankart repair or the Latarjet procedure). That study revealed a higher recurrence rate in the group that underwent revision arthroscopic Bankart repair (43% vs 0% for Latarjet procedure) and poorer patient-reported outcomes. Those findings appear to contradict our findings, although Elamo et al 13 did not analyze glenoid bone defects and a well-designed prospective randomized controlled study is needed to address this issue.
Several factors are associated with recurrent instability after primary ACR, including repeated trauma, a poor surgical technique, hyperlaxity, severe glenoid bone defects, the number of dislocations, and off-track Hill-Sachs lesions. 5,26 Regarding the surgical technique, 1 patient in the revision group had only 2 suture anchors at the time of primary ACR. During revision ACR, 4 suture anchors were inserted in the over-the-top position in this patient. The appropriate number of suture anchors may be controversial; however, we believe that at least 3 to 4 anchors are required for proper capsulolabral repair and rotator interval closure. Boileau et al 5 also mentioned that an inappropriate anchor position on the glenoid and using fewer than 3 anchors are important causes of recurrent instability after primary ACR. Hyperlaxity is also considered to be a risk factor for clinical failure after primary ACR. Voos et al 46 reported 3 times higher recurrent instability in patients with hyperlaxity. In the current study, 2 patients in the revision group had hyperlaxity. These patients had no reason for recurrence, such as new trauma, other than hyperlaxity. Inherent hyperlaxity is related to plastic deformation of the capsule. 37 Persistent damage to the capsule and labrum after repeated dislocations and surgery can affect the normal structure of the capsulolabral complex. Although hyperlaxity in the primary group in the current study was not related to a positive persistent apprehension sign, evaluating preoperative hyperlaxity is important.
Millar and Murrell 30 compared primary and revision ACR, revealing good functional outcomes and recurrence rates, although none of their patients had glenoid bone defects. Stein et al 43 reported that revision Bankart repair showed good to excellent clinical outcomes, but they were inferior to those after primary Bankart repair. They performed postoperative MRI and showed that revision Bankart repair can restore adequate anteroinferior labral joint congruency. Krueger et al 23 reported poorer subjective outcomes after revision ACR (vs primary ACR), although there was no difference in the positive apprehension sign. Thus, they suggested that the poorer subjective outcomes after revision arthroscopic surgery might be related to increased arthropathy or emotional concerns regarding the shoulder. In contrast, the present study identified no arthropathy in either group, and revision and primary ACR provided comparable functional outcomes for patients with moderate glenoid bone defect sizes. Patel et al 36 reported a mean ASES score of 81.1 and good to excellent quality of life scores at a mean follow-up of 36 months after revision ACR in 40 patients with failed primary surgery. In their study, a mean number of 2.43 (range, 1-3) anchors were used for revision ACR. It is thought that such a small number of anchors used may have contributed to the lower ASES score in contrast to the current study’s ASES score of 97.6. Bartl et al 2 reported good results with a mean Constant score of 87 and a mean simple shoulder test score of 11 points after revision arthroscopic stabilization surgery in 56 patients. They showed the usefulness of at least 3 anchors and a portal at the 5:30 clock position in revision surgery. 2 In the current study, the revision group showed excellent results with an ASES score of 97.6 using ≥3 anchors without a portal at the 5:30 clock position.
A systematic review by Abouali et al 1 revealed that 69.1% of patients were able to return to sports after revision arthroscopic surgery, which agrees with the rate of 65.2% in our revision group. Returning to sports at the preoperative level in overhead-throwing athletes typically requires the recovery of external rotation capability and the shoulder’s capacity for proprioception. 6 However, revision surgery could cause additional damage to the many neuronal structures of the anteroinferior capsule–labrum–ligament complex, 50 which might impair the recovery of proprioception. We speculate that this mechanism might explain the poorer rate of return to sports in the revision group relative to the primary group (65.2% vs 80.6%, respectively). However, in the present study, the sports level was classified into only high (dynamic or contact sports), medium (static sports), and low (limited sports activity), and throwing sports could not be compared and analyzed. Further studies on returning to throwing sports in patients undergoing revision ACR will be needed.
The results of isokinetic muscle strength testing revealed that internal rotation strength was improved at 1 year after surgery, although external rotation strength did not improve to the same extent. The PTR can be a useful indicator of rotator muscle balance and stability, 14,19 with population-specific ratios of 0.57 to 1.19, because internal rotation strength is generally greater than external rotation strength. 44 Ellenbecker and Davies 14 have also suggested that a PTR of 0.66 to 0.75 (2:3-3:4) is needed to prevent shoulder injuries, and the present study revealed significantly improved PTR values at 1 year after surgery in the revision group (0.78) and the primary group (0.74). In the present study, external rotation strength in both groups relative to the preoperative value for the involved shoulder was also recovered at 1 year after surgery, although it was still weaker than in the uninvolved shoulder. Internal rotation strength in both groups, on the other hand, recovered similarly to that of the uninvolved shoulder at 1 year after surgery. Rhee et al 38 reported that patients with weak internal and external rotation strength showed a positive apprehension sign at 1 year after surgery. These results inform orthopaedic surgeons on the importance of the external rotation/internal rotation power ratio, and external rotator strengthening exercises should be emphasized. Long-term follow-up studies using isokinetic muscle strength testing are also needed to evaluate external rotation recovery.
Glenoid bone defects are important in patients with anterior shoulder instability. 5,20 Shin et al 42 reported that glenoid bone defects of >17.3% were associated with recurrent instability after arthroscopic Bankart repair. Yamamoto et al 51 also reported that anterior stability decreased with glenoid bone defects of >20% in the 3-o’clock position in their cadaveric study. Shaha et al 41 reported that the WOSI score was poor in patients with more than subcritical bone loss of 13.5%. The mean glenoid bone defect sizes in the revision group (17.3%) and primary group (15.4%) in the current study were greater than a subcritical bone loss of 13.5%. At the final follow-up, the mean WOSI score was 636.7 in the revision group and 551.1 in the primary group, which were better than 839.5 in the subcritical bone loss group reported by Shaha et al. 41 Unlike our study, Shaha et al 41 analyzed patients by quartiles according to the percentage of bone defects; the patients included in that study were active-duty military and had a higher WOSI score than that of the civilian population, even without recurrent instability.
Regarding the threshold of glenoid bone defects, there is no generally accepted definition of “moderate” or “severe” glenoid bone defects. However, in general, 20% to 25% is considered as the threshold for “severe” bone loss. 25 We set a moderate bone loss threshold of 10% to 25%, which is commonly used. In the present study, the mean glenoid bone defect size was considered moderate in the primary group (15.4% ± 5.1%). The mean number of dislocations before surgery in the primary group was 9.6 ± 11.4. Repetitive dislocations increase micro–impaction fractures of the anterior glenoid rim, which can lead to greater glenoid bone defects. 42 In the revision group, the mean glenoid bone defect size was 17.5% ± 5.2% (range, 11%-25%) (Figure 1). Interestingly, we observed that all patients in the revision group with a positive apprehension sign also had a glenoid bone defect of >20%. In contrast, patients in the revision group with glenoid bone defect sizes of 11% to 20% did not exhibit any positive apprehension sign. Moreover, in the current study, the cutoff value for glenoid bone defects to predict a positive apprehension sign after revision ACR was 20.5%. The cutoff value for glenoid bone defects in revision ACR has not been suggested so far, and it seems to be an important indicator for determining the surgical strategy for revision.
This study has several limitations. First, retrospective single-center studies with short follow-ups are prone to have various sources of selection bias. In addition, the characteristics of the 2 groups were not completely matched, although we did not detect significant differences regarding sex and hand dominance. There was a statistical difference in age between the 2 groups. Patients in the revision group underwent revision surgery at a mean of 3.4 years after primary surgery, and this may explain why the revision group was older than the primary group. These older patients were likely to have lower activity levels and might have contributed to the excellent results in the revision group. Furthermore, the results of primary ACR are already known to be excellent, and we do not believe that any imbalances would have substantially influenced our results. Second, we did not directly compare bony revision procedures (eg, the Latarjet procedure) and arthroscopic surgery. We are only aware of one retrospective cohort study that directly compared revision arthroscopic surgery and revision Latarjet procedures, 13 although that study did not consider preoperative glenoid bone defects. The present study revealed that revision and primary ACR provided comparable results in patients with moderate glenoid bone defects, although further studies are needed to compare bony procedures and arthroscopic surgery as revision strategies. Third, a glenoid bone defect is important in determining the surgical method. The revision group showed a positive apprehension sign in patients with glenoid bone defects of >20%. However, because the sample size of the revision group is small (n = 23), a large cohort study would be needed to identify the cutoff value of glenoid bone defects that can affect the outcomes of revision surgery. Fourth, in the current study, a positive apprehension sign was considered as a failure of surgery. However, even though a physical examination was performed by the same examiner, a positive apprehension sign can appear differently according to the subjective feeling of the patient, so it may be difficult to evaluate it as real failure. Finally, the present study did not identify any patients with recurrent dislocations probably because of the small sample size; therefore, a larger cohort of patients is needed to clarify the true recurrence rate of dislocations. Moreover, the follow-up rate was only 55.2% of eligible patients. It is possible that patients with worse outcomes (eg, recurrent dislocations, pain, etc) were the ones lost to follow-up. More follow-up patients would be required to clarify the interpretation of our results.
Conclusion
In patients with moderate glenoid bone defects of 10% to 25%, we found that clinical outcomes after revision ACR were comparable to those after primary ACR. However, significant glenoid bone loss was related to a positive remaining apprehension sign in the revision group. Surgeons should consider these findings when selecting their revision strategy for patients with failed anterior shoulder stabilization. An alternative revision procedure should be considered when the glenoid bone defect is >20%.
Footnotes
Final revision submitted August 8, 2021; accepted August 24, 2021.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Seoul National University Bundang Hospital (No. B-2103/670-102).