
Abstract
Background:
Previous evaluations in adult pitchers have noted discrepancies in pitchers’ rate of perceived effort (RPE) versus actual effort when pitching.
Purpose:
To discern a relationship between RPE with objective measures of effort including ball velocity, maximal elbow varus torque, torque loading rate, and cumulative elbow varus torque in high school (HS) and professional (PRO) baseball pitchers.
Study Design:
Descriptive laboratory study.
Methods:
A total of 38 HS pitchers (age, 16.9 ± 0.9 years; height, 183.3 ± 6.0 cm; weight, 78.1 ± 9.2 kg) and 24 PRO pitchers (age, 24.0 ± 2.3 years; height, 188.8 ± 5.2 cm; weight, 90.9 ± 7.3 kg) were analyzed using 3-dimensional motion capture (480 Hz) while throwing fastballs. HS pitchers threw at 50%, 75%, and 100% effort; PRO pitchers threw at 75% and 100% effort. Elbow varus torque, loading rate, cumulative torque, and ball velocity were used to assess intra-pitcher relationships with a linear mixed-effects model.
Results:
HS pitchers significantly differed (Pall < .001) at 50%, 75%, and 100% RPE for, respectively, ball velocity (30.2 ± 1.0 vs 32.2 ± 0.6 vs 35.1 ± 0.5 m/s), elbow varus torque (53.3 ± 4.4 vs 59.0 ± 3.3 vs 69.1 ± 2.8 N·m), cumulative torque (1919.0 ± 115.9 vs 2033.3 ± 85.5 vs 2339.2 ± 87.6 N·m*s), and torque loading rate (360.3 ± 53.3 vs 421.1 ± 38.6 vs 532.6 ± 53.1 N·m/s). Similar results were observed for PRO pitchers at 75% and 100% effort (P < .001). A strong correlation was found between the RPE and the measured torque parameters (all R2 > 0.85). The observed change in measured variables did not correspond to the change in RPE for all metrics for both pitching populations (ie, HS at 50% effort threw at 86% ball velocity, 75% maximal elbow varus torque, 80% cumulative torque, and 67% torque loading rate). In PRO pitchers, variance did not differ between effort groups for all variables. In HS pitchers, there was greater variance in lower effort pitches for ball velocity between 50% and 100% (P < .001) and 50% and 75% (P < .001) and for torque loading rate for 75% to both 50% and 100% (P < .001).
Conclusion:
Although throws from HS and PRO pitchers at lower prescribed RPE showed lower observed effort, the reduction in observed efforts decreased disproportionately less compared with perceived efforts. PROs appear to be more adept at maintaining consistency during submaximal effort pitches compared with HS pitchers.
Clinical Relevance:
Interval throwing programs commonly rely on pitchers self-regulating intensity through RPE. Reductions in RPE do not consistently translate into proportional decreases in ball velocity or elbow varus torque, especially in HS pitchers who show greater variability at submaximal efforts. Simply asking pitchers to “throw easier” may not reliably reduce joint loading and could expose healing tissue to higher-than-intended stress. Clinicians should recognize the limitations of RPE-based workload progression, particularly in younger pitchers, and consider integrating objective monitoring tools (e.g., velocity tracking, wearable sensors, or biomechanical assessments) to ensure safer and more consistent return-to-throw rehabilitation.
The rising prevalence of elbow injuries among baseball pitchers has drawn attention to the ulnar collateral ligament (UCL).6,21 While UCL reconstruction surgery was once reserved for professional (PRO) pitchers, there is concern about the increasing number of high school (HS) pitchers undergoing this procedure. 3 Recent studies indicate that adolescents and young adults aged 15 to 19 years represent the greatest population of athletes undergoing UCL reconstruction 11 and now account for over 54% of total UCL injuries across the United States. 25
To address this growing trend, alterations in throwing workload have been used both to protect the healthy and to rehabilitate the injured pitcher. Rehabilitation strategies like interval throwing programs (ITP) have been a longstanding staple in helping pitchers safely return to sport. 8 ITPs are structured into 2 distinct phases: flat-ground throwing and mound throwing. 22 During the flat-ground phase, athletes are supposed to throw a baseball with only enough effort for it to travel the prescribed distances. The mound phase incorporates throws at varying rates of perceived effort (RPEs)—namely, 50%, 75%, and 100%—which is a commonly used subjective measure that indicates how hard an individual exerts himself during activity. These submaximal throws are prescribed with increasing volume and intensity until the athlete can perform maximal effort throws, asymptomatically. This progression is designed to allow healing tissues to strengthen with incremental sport-specific loading while avoiding loading regimens that would be prone to causing injury. In short, this progression allows pitchers to build tolerance to pitching stresses that are otherwise challenging to replicate through traditional exercises. 2
While RPE is widely used to guide ITPs, research has shown that perceived effort levels do not correlate proportionally with reductions in ball velocity or elbow varus torque. Melugin et al 20 reported that while throwing on flat ground at 36.6 m (120 ft) with an RPE of 75%, HS and college pitchers demonstrate a ball velocity reduction to 86% of maximum, while elbow varus torque only decreases to 93% of maximum. Similarly, mound-based studies in collegiate pitchers revealed no proportional decrease in velocity or elbow varus torque with submaximal RPE levels. 23 These findings raise concerns about the efficacy of RPE-guided rehabilitation, particularly given the role of elbow varus torque in UCL injuries. 12 While changes in maximal elbow varus torque have been reported, there is a lack of published data on the torque loading rate, as well as the cumulative elbow varus torque throughout a given pitch between different RPEs. Furthermore, no studies have examined whether PRO pitchers exhibit better RPE perception and more proportional change compared with HS pitchers.
Therefore, the purpose of this study is to evaluate the influence of different perceived effort levels on key pitching variables including ball velocity, maximal elbow varus torque, torque loading rate, and cumulative elbow varus torque in HS and PRO baseball pitchers. This study seeks to determine whether reductions in RPE correspond proportionally to changes in pitching variables across both HS and PRO pitchers. We hypothesize that reductions in pitching variables will not align proportionally with RPE, with PRO pitchers exhibiting closer alignment compared with HS pitchers.
Methods
This was a retrospective review of pitchers who were previously tested. Data were deidentified before distribution, thus qualifying for exempt institutional review board review under federal guidelines. High school (HS; n = 38; age, 16.9 ± 0.9 years; height, 183.3 ± 6.0 cm; weight, 78.1 ± 9.2 kg; 29 right-handed/9 left-handed) and professional pitchers (PRO; n = 24; age, 24.0 ± 2.3 years; height, 188.8 ± 5.2 cm; weight, 90.9 ± 7.3 kg; 20 right-handed/4 left-handed) previously evaluated were included in this study. Inclusion requirements for PRO pitchers were (1) at the time of testing, pitchers were on the major league or minor league (low A or high A, AA, and AAA) roster; (2) pitchers had no record of serious injury (requiring >2 weeks of rest or rehabilitation) in the past 6 months, and (3) pitchers had been cleared by team clinicians to participate in baseball activities. Inclusion requirements for HS pitchers were (1) at the time of testing, pitchers were on a HS or club team, (2) pitchers had no record of serious injury (requiring >2 weeks of rest or rehabilitation) in the past 6 months, and (3) pitchers had been cleared to participate in baseball activities by their physician.
Pitching evaluations were conducted as previously described.9,16 Demographic data were self-reported by the pitcher, including age, preferred throwing arm, experience level, and history of injury. Research staff measured and recorded the pitcher's height and weight. Before pitching, 46 reflective markers were positioned on anatomic landmarks as previously described.9,16 Positional coordinate data of the reflective markers were collected using an 8-camera Raptor-E motion analysis system (Motion Analysis Corp) at 480 Hz. The global coordinate system was established based on International Society of Biomechanics standards: Y was vertically upward, X was from the pitching rubber toward home plate, and Z was the cross-product of X and Y. 29
After an unlimited warm-up period with the pitcher's preferred routine, the pitcher was instructed to throw fastballs at varying levels of effort. Because the pitcher warmed up throwing 100% effort, he was able to adjust down to 50% having thrown 100% as a guide. The HS pitcher threw 3 fastballs in the order of 50%, 75%, and 100% effort, while the PRO pitcher threw 3 fastballs at the 75% and 100% effort conditions (not 50%). The pitches were thrown from a regulation turf mound to 9-hole screen and home plate at regulation distance (18.4 m/60.5 ft). Pitchers were allowed to pitch at their own pace and were not given instruction on where to aim in the strike zone. Ball flight data (eg, ball velocity, spin rate, true spin, efficiency) were collected using a portable TrackMan B1 located behind the catcher.
All data processing was performed using custom MATLAB scripts (Version R2021b; MathWorks) as previously described.9,16 Data from the markers were filtered by a low-pass filter (fourth order, zero-lag Butterworth filter; 18-Hz cutoff frequency). Elbow varus torque was calculated over the course of the entire pitch (from maximal knee height to maximal internal shoulder rotation). Peak elbow varus torque (N·m) was reported as the maximum that occurred between foot contact and ball release. Torque loading rate (N·m/s) was calculated as the peak varus torque divided by the time to reach peak torque starting at foot contact. Cumulative torque (N·m*s) was calculated as the integral of the torque curve, from foot contact to ball release.
To assess intra-pitcher relationship between the RPE conditions, elbow varus torque measures, and ball velocity among pitchers, a linear mixed-effects model with random intercepts was used. To establish variance at each condition, the standard deviation for each parameter of all pitches in a RPE group was calculated. Repeated-measures analysis of variance with post hoc Tukey Honestly Significant Difference was used to compare variance within each RPE group. For all analyses, statistical significance was set with a Bonferroni corrected alpha value of .05. R2 < 0.3 indicated a weak correlation, 0.31 < R2 < 0.7 indicated a moderate correlation, R2 > 0.71 indicated a strong correlation. All data analyses were performed using MATLAB with the Statistics and Machine Learning Toolbox.
Results
For the HS group, within an individual pitcher, there were significant differences between all RPE groups, 50% to 75%, 50% to 100%, and 50% to 75%, for ball velocity (m/s), elbow varus torque (N·m), cumulative torque (N·m*s), and torque loading rate (N·m/s) (P < .001) (Table 1). For each parameter, a strong correlation was found between RPE and ball velocity (R2 = 0.85), elbow varus torque (R2 = 0.91), cumulative torque (R2 = 0.93), and torque loading rate (R2 = 0.85). In the PRO group, within an individual pitcher, significant differences were found between the 75% and 100% effort groups for all parameters (P < .001) (Table 2).
Pooled Means for Varying Pitching Efforts in High School Pitchers a

Data are presented as mean ± SD.
Statistically significant difference 50% and 75% effort, 50% and 100% effort, and 75% and 100% effort.
Pooled Means for Varying Pitching Efforts in Professional Pitchers a

Data are presented as mean ± SD.
Statistically significant difference between 75% and 100%.
The observed change in measured variables was not identical to the change in RPE for all metrics (Table 3, Figure 1). For HS pitchers, for every 25% decrease in RPE, ball velocity decreased 2.44 m/s (β = 0.098), elbow varus torque decreased 8.42 N·m (β = 0.34), torque loading rate decreased 89.56 N·m/s (β = 3.58), and cumulative torque decreased 238.06 N·m*s (β = 9.52). In PRO pitchers, with the 25% decrease in RPE, ball velocity decreased 3.95 m/s (β = 0.16), elbow varus torque decreased 18.23 N·m (β = 0.73), torque loading rate decreased 233.75 N·m/s (β = 9.35), and cumulative torque decreased 3.95 N·m*s (β = 14.74).
Percentage of Maximal Effort in High School and Professional Pitchers a
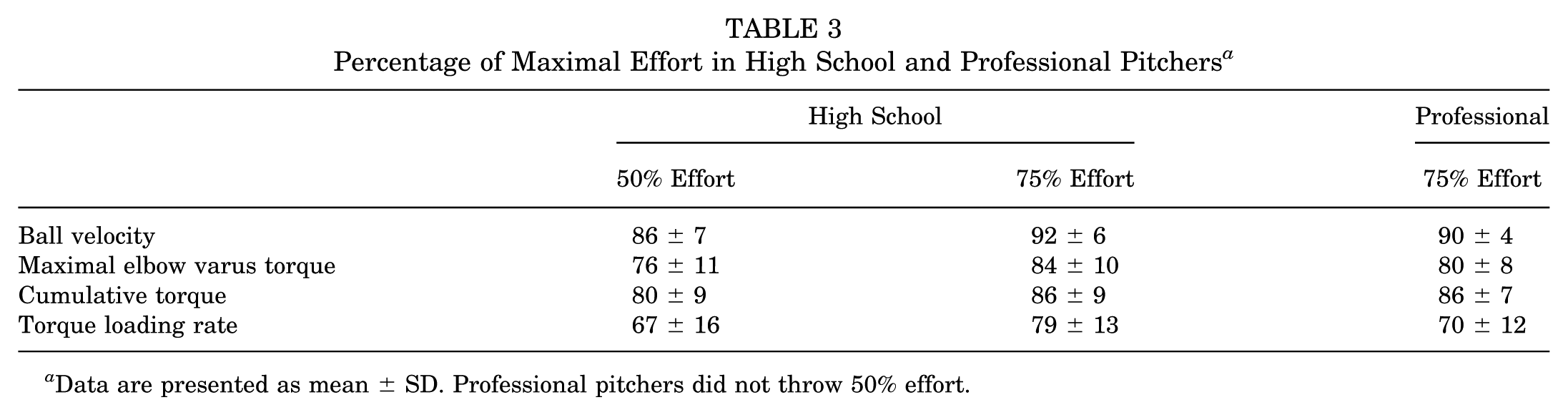
Data are presented as mean ± SD. Professional pitchers did not throw 50% effort.

Mean percentage change of measured effort versus perceived effort in (A) high school and (B) professional pitchers.
When comparing the variance between RPE groups for HS pitchers, there were significant differences in ball velocity variance in the comparisons of 50% to 100% (P < .001) and 50% to 75% (P < .001), but not 75% to 100% (P > .05) (Table 4). A significant difference was also found in the torque loading rate between groups 50% to 75% (P < .001) and 75% to 100% (P < .001). No significant difference was found in variance for elbow varus torque (P = .15) or cumulative torque (P = .39). Comparing variances in the PRO pitchers, there were no significant differences found between effort groups for all variables: ball velocity (P = .22), maximal elbow varus torque (P = .79), cumulative torque (P = .95), and torque loading rate (P = .11).
Standard Deviation for Varying Pitching Efforts Within High School and Professional Pitchers a

Data are presented as mean ± SD.
Statistically significant difference (P < .001) at 50% and 75% effort.
Statistically significant difference (P < .001) at 50% and 100% effort.
Statistically significant difference (P < .001) at 75% and 100% effort.
Discussion
RPE remains a fundamental tenant of altering throwing workload, especially during an ITP to return to play after baseball injury. Our hypothesis that both HS and PRO pitchers do not have proportional changes in measured variables for a given RPE was confirmed. PRO pitchers were better able to adjust their effort levels to mirror a prescribed RPE as compared with HS pitchers, likely secondary to pitching experience and more efficient biomechanics.
Previous literature has shown that pitchers struggle with the ability to accurately adjust their effort compared with the prescribed RPE. Wilk et al 28 reported that pitchers undergoing return to throw programs threw at faster velocities compared with the RPE prescribed. When throwing at 120 ft, elbow varus torque and ball velocities in HS and collegiate pitchers did not decrease to the magnitude of the prescribe RPE. 20 Melugin et al 20 noted that 25% reductions in RPE lead to decreases in elbow varus torque by 7% and ball velocity decreased by 11%. In a study in adult pitchers throwing on the mound at 18.4 m (60.5 ft), Slenker et al 23 found at a 60% RPE, elbow varus torque decreased to 75% and ball velocity only decreased to 84% of the maximal respective values. When looking at HS pitchers, Fiegen et al 11 reported that for every 25% decrease in RPE, elbow varus torque decreased 13% and ball velocity decreased by 7.5%. Similarly, in the current study for HS pitchers, a 25% RPE reduction resulted in a 16% reduction in elbow varus torque and 8% reduction in ball velocity. PRO pitchers were better at more appropriately adjusting their ball velocity and elbow varus torque in attempts to mirror a given RPE in comparison with the HS pitchers. If a pitcher were to appropriately decrease his velocity to meet the prescribed 50% RPE, it is possible that at the decreased velocity the pitcher would have difficulty maintaining proper mechanics as well as accuracy/command with getting the ball to the intended target. Ball velocity is likely a poor indicator of shoulder and elbow load and pitchers are throwing with greater intensity than prescribed and/or intended. Altered pitching mechanics during these submaximal throws is a probable mechanism by which pitchers decrease their RPE but future research should investigate the exact change in mechanics due to decreased RPE and its potential influence on load at the elbow.
Previous research has positively linked fastball velocity to elbow varus torque17,24 as well as increased elbow varus torque to elbow injuries.1,12,15,26 Utilizing maximal elbow varus torque is a valuable metric to represent load experienced at the elbow; however, it only represents a single maximal value and does not appropriately quantify the cumulative load on the elbow or the tissue loading rate about the elbow. Higher cumulative torque could cause prolonged exposure to the medial elbow and lead to increased tissue fatigue. Hodakowski et al 14 reported higher cumulative torque in 100% RPE fastball pitches thrown by PRO pitchers (3015 N·m*s) compared with this study's PRO and HS pitchers (2890 and 2339 N·m*s, respectively). Because only 1 previous study has examined cumulative torque, comparing values is difficult, especially between competition levels. For both HS and PRO pitchers, cumulative load and torque loading rate decreased at lower throwing effort, which bolstered the case of variable-effort pitching during the rehabilitation process, as lower subjective throwing intensities impart less load on the shoulder and elbow. Incidentally, the torque loading rate among PRO pitchers was the only pitching variable that demonstrated a greater reduction in magnitude compared with the relative reductions in perceived effort across all pitching conditions.
The current study highlights that HS pitchers struggle to maintain consistent effort levels at lower RPE, as shown by larger variability in ball velocity and loading rate at 50% RPE compared with 100%. In contrast, PRO pitchers demonstrated consistent variability across all RPE conditions, suggesting a greater ability to regulate effort and deliver more uniform throws. This discrepancy suggests that achieving consistent outputs at prescribed RPEs, particularly when using ball velocity as a proxy for effort, may be unrealistic for developing pitchers. Coaches, physical therapists, athletes, physicians, and trainers should consider these limitations when designing throwing programs for adolescent pitchers. A recently published ITP by Dowling et al 8 addressed discrepancies in RPE by adjusting workload progression through volume and distance, yet variability in effort at non-PRO levels remains a concern. However, the present findings underscore that substantial variability still exists in non-PRO populations, even under controlled conditions. Interestingly, while ball velocity varied significantly among HS pitchers at 50% RPE, elbow varus torque did not—raising the possibility that pitchers may alter their mechanics to achieve reduced output (ie, slower pitch velocity) without a corresponding reduction in joint loading. This mechanical compensation may involve adjustments in segmental sequencing, stride length, or trunk contribution, allowing for lower velocities to be achieved with relatively stable torque levels. This also suggests that variability in perceived effort may not only reflect cognitive calibration issues but also biomechanical adaptations. Future research should examine whether these adjustments are adaptive, aiming to preserve mechanics under lower output demands, or potentially maladaptive, introducing new movement inefficiencies or injury risks. Additionally, research should explore individualized ITPs tailored to HS and PRO athletes, taking into account their respective capacity to regulate effort and the possible downstream effects of effort variability on recovery, performance, and joint health.
These findings emphasize the value of incorporating lower-intensity throws in ITPs, but they also highlight a critical risk: the disproportionate gap between perceived effort and actual observed effort. If pitchers unintentionally throw with greater effort and torque than instructed, particularly at 50% and 75% RPE, they may be exposing healing tissues to loads higher than intended, increasing the risk of reinjury. This concern is especially pressing given the established link between elevated elbow varus torque, higher fastball velocities, and increased injury rates in PRO pitchers.1,4,6,7,18,19,29 These discrepancies suggest that traditional, subjective RPE targets may not provide a reliable framework for safely progressing throwing workloads, particularly in adolescent or inexperienced populations. Tailoring ITPs to account for individual variability in effort regulation is critical. Programs should integrate objective monitoring tools such as motion capture and wearable sensors, to more accurately assess both velocity and joint torque. These technologies enable real-time feedback and better alignment between intended and actual effort, ensuring safer and more effective workload progression. Incorporating regular biomechanical assessments or video analysis can further support mechanical consistency, particularly during lower-intensity phases where compensatory movement patterns may emerge. As motion capture systems and wearable technology become increasingly accessible, they offer a practical, data-driven path to more precisely track elbow loading and optimize return-to-throw protocols. Widespread adoption of these tools represents a key opportunity to reduce reinjury risk and address the growing elbow injury epidemic in baseball.
Limitations
Limitations of the study are as follows: Healthy pitchers were used in this assessment, which does not adequately represent the typical ITP cohort of injured or deconditioned pitchers attempting to return to play. Pitchers were also instructed to throw <20 pitches total, which does not account for workloads where fatigue can alter perceived efforts. Although the method of data collection for the HS and PRO was nearly identical, these data were provided retrospectively and we did not have the ability to retrospectively ask for pitching conditions. Therefore, we only have 2 RPE conditions for the PRO and 3 for the HS pitchers. As there were no PRO data collected at 50% RPE, it is possible that the PRO pitchers might display increased variation at lower levels of RPE similar to the HS pitchers; future research should investigate the ability of PRO pitchers to consistently throw at reduced efforts. It is unclear how fatigue influences a pitcher's ability to replicate perceived efforts and may be an area for additional research. This study evaluated pitching efforts from a mound at 18.4 m (60.5 ft); however, other ITP simulation biomechanical studies have attempted at varying distances on the flat-ground.5,13 Given many ITPs incorporate throwing at prescribed distances with varying RPE as a staple to the program, this is an important parameter lacking from the current paper that can be investigated in future studies for more comprehensive analyses of perceived efforts for ITP. The actual amount of torque experienced at the elbow is unknown with metrics collected here acting as estimated surrogates. Though the values here likely derive the highest value when comparing throws among a single pitcher as conducted in the current study.
Conclusion
Although both HS and PRO pitchers demonstrated lower observed effort during throws performed with reduced perceived effort, the magnitude of reduction in observed effort was disproportionately smaller than the decrease in prescribed effort. This discrepancy was more pronounced in HS pitchers, suggesting PRO pitchers are better at modulating their perceived effort. Additionally, HS pitchers exhibited greater variability with reduced RPE, suggesting difficulty in consistently modulating their effort within submaximal ranges. These findings indicate that PRO pitchers are more adept at controlling effort output, while HS pitchers may lack the control or experience to reliably adjust intensity. These findings raise concerns about the effectiveness of instructing pitchers, particularly HS pitchers, to simply “throw easier” as a strategy to reduce elbow varus torque or overall biomechanical load, and could potentially lead to inconsistent or unintended loading patterns. Alternative methods or more precise monitoring may be necessary to achieve the intended reduction in joint loading.
Footnotes
Final revision submitted May 19, 2025; accepted June 16, 2025.
Presented as a poster at the annual meeting of the AOSSM, Nashville Tennessee, July 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.R. is a paid consultant for Acumed LLC, Encore Medical, Zimmer Biomet Holdings Inc, Bioventus LLC, Restor3d Inc, RTI Surgical Inc, Flower Orthopedics Corp, ExosMed Corp, MedShape Inc, and Medical Device Business Services Inc; is a paid presenter or speaker for Acumed LLC, Medartis Inc, Bioventus LLC, and TriMed Inc; has received hospitality payments from Acumed LLC, Encore Medical, Zimmer Biomet Holdings Inc, and Medartis Inc; has received royalties from Pioneer Surgical Technology Inc; has received honoraria from Encore Medical and Medartis Inc; and has received support for education from Southtech Orthopedics. G.P.N. has received hospitality payments from Stryker, Anika Therapeutics, and Wright Medical Technology; consulting fees from Stryker, Anika Therapeutics, KCI USA Inc, Azurmeds, and Wright Medical Technology; speaking fees from Wright Medical Technology and Arthrosurface Inc; and royalties from Anika Therapeutics, Stryker, Wright Medical Technology, and Arthrosurface Inc. N.N.V. is a paid consultant for Arthex Inc, Medacta USA, and Stryker; is a paid presenter or speaker for Arthrex Inc; has received research support from Arthrex Inc; has received hospitality payments from Arthrex Inc, Stryker, Breg, Nevro Corp, Pacira Pharmaceuticals, Relievant Medsystems, and Spinal Simplicity; has received nonconsulting fees from Arthrex Inc; has received consulting fees from Smith & Nephew; has received support for education from Medwest Associates; and has received royalties or a license from Arthrex Inc, Smith & Nephew, and Graymont Professional Products. G.E.G. is a paid consultant for Encore Medical, Medical Device Business Services, Wright Medical Technology, DePuy Synthes Sales, DePuy Synthes Products, and Bioventus LLC; has received consulting fees from Stryker Corp; has received hospitality payments from Encore Medical, Wright Medical Technology, Smith & Nephew, Arthrex, and Exactech Inc; is a paid presenter or speaker for Encore Medical and Wright Medical Technology; has received support for education from Medwest Associates; and has received royalties or a license from Stryker Corp, Encore Medical, and Wright Medical Technology. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by Rush University Medical Center (ORA No. 25010307-IRB01).