
Abstract
Background
Platelet-rich plasma (PRP) is widely used to promote healing and improve function in various musculoskeletal injuries. However, the efficacy and safety of PRP for meniscal injury remain unclear.
Purpose:
To evaluate the effects of PRP in patients with meniscal injury.
Study Design:
Systematic review; Level of evidence, 2.
Methods:
A comprehensive search was conducted in PubMed, Embase, Cochrane Library, Web of Science, Wanfang, and CNKI databases. Randomized controlled trials comparing PRP with placebo or no additional treatment in adult patients with meniscal injury were included. Outcome measures included the visual analog scale for knee pain, Lysholm score, Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), Knee injury and Osteoarthritis Outcome Score (KOOS), treatment failure, and complications. Data were pooled using a random-effects model by incorporating the influence of heterogeneity.
Results:
This meta-analysis included 18 randomized controlled trials involving a total of 1143 patients. The mean follow-up duration ranged from 3 to 12 months. PRP significantly reduced knee pain (mean difference [MD], −0.73; 95% CI, −0.91 to −0.55) and improved knee function, as indicated by higher Lysholm scores (MD, 6.77; 95% CI, 5.35 to 8.20) and KOOS (MD, 4.34; 95% CI, 1.35 to 7.32), and lower WOMAC scores (MD, –5.33; 95% CI, −8.10 to −2.56). Subgroup analyses suggested similar results in patients with and without concurrent knee osteoarthritis, with single and multiple PRP injection, and with follow-up duration of <12 and ≥12 months. In addition, PRP also reduced treatment failure rates (odds ratio, 0.26; 95% CI, 0.12 to 0.59), with no significant difference in complications.
Conclusion:
PRP is effective in reducing pain and improving knee function in patients with meniscal injury.
Registration:
CRD42024601679 (PROSPERO)
Meniscal injury is one of the most common knee injuries, particularly among athletes and active individuals.22,31 Physiologically, meniscus plays a crucial role in knee joint stability, shock absorption, and load transmission. 30 Meniscal tears can lead to pain, swelling, and functional impairment, significantly affecting an individual’s quality of life. 3 If left untreated or inadequately treated, meniscal injuries can result in long-term complications, such as osteoarthritis (OA) and cartilage degeneration, contributing to further disability and chronic knee pain. 35 While nonoperative treatments, including physical therapy and nonsteroidal anti-inflammatory drugs, are often the first line of management, surgical interventions such as partial meniscectomy or meniscal repair are considered for more severe cases. 28 However, these treatments have their limitations, as surgical procedures may not fully restore the normal function of the meniscus and can increase the risk of early-onset OA. 48 Consequently, there is a growing interest in finding alternative therapies that can enhance meniscal healing and improve long-term outcomes.
Platelet-rich plasma (PRP) has emerged as a promising biological treatment for musculoskeletal injuries, including meniscal injuries.10,54 PRP is an autologous concentration of platelets derived from the patient's own blood, which is rich in growth factors and bioactive proteins. These growth factors, including platelet-derived growth factor, transforming growth factor beta, and vascular endothelial growth factor, promote tissue regeneration, reduce inflammation, and enhance the healing of injured tissues.38,39 The rationale for using PRP in meniscal injuries lies in its ability to accelerate the healing process by stimulating cellular proliferation, collagen synthesis, and angiogenesis in the meniscus. 5 Furthermore, the anti-inflammatory properties of PRP may help reduce pain and improve knee function. 6 Given these biological features, PRP has been proposed as a minimally invasive therapeutic option to treat meniscal injuries and prevent subsequent knee degeneration.
Despite the increasing use of PRP in clinical settings, the efficacy of PRP for meniscal injuries remains controversial. 10 Previous clinical studies have reported mixed results regarding its effectiveness. Some studies have shown significant improvements in pain relief, knee function, and reduced treatment failure rates after PRP injections.1,18-20,32,52 while others found no significant differences compared with conventional treatments.7,8,13 These discrepancies may be attributed to variations in study design, patient populations, and PRP preparation protocols. The lack of standardized treatment protocols and inconsistent results in the literature have raised concerns about the generalizability and reliability of the findings, leading to uncertainty regarding the optimal use of PRP for meniscal injuries. 4 Although several previous meta-analyses have attempted to synthesize the available evidence, their results were also inconsistent.24,33,47,51 Moreover, these meta-analyses were based on limited studies and involved both the randomized controlled trials (RCTs) and non-RCTs, which may introduce bias and weaken the strength of the conclusions.24,33,47,51 Furthermore, these analyses did not thoroughly explore the potential effect of study characteristics, such as the presence of concurrent knee OA, the number of PRP injections, and the follow-up duration, all of which may affect treatment efficacy. In view of the newly published RCTs in recent years, ¶ the aim of the current meta-analysis is to evaluate the efficacy and safety of PRP for meniscal injury by systematically reviewing and analyzing data from RCTs. This study focuses on key outcomes such as knee pain, function, treatment failure, and complications. Additionally, the meta-analysis explore the possible effect of study characteristics, particularly the presence of concurrent knee OA, the number of PRP injections, and the duration of follow-up, on treatment outcomes.
Methods
During the design and implementation of this study, we followed the guidelines set forth by PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses)36,37 and the Cochrane Handbook. 15 The protocol of the meta-analysis has been registered at PROSPERO with the identifier CRD42024601679.
Study Inclusion and Exclusion Criteria
This meta-analysis included studies that met the inclusion criteria specified in the PICOS principle.
P (patients): Adult patients (aged ≥18 years) diagnosed with meniscal injury, confirmed via clinical assessment or magnetic resonance imaging (MRI). Studies involving pediatric populations were excluded. No restriction was placed on the etiology of the tear (traumatic vs degenerative) or on participants’ physical activity levels (eg, professional athletes), to reflect a broad and generalizable population. However, most included studies did not specify these characteristics in sufficient detail to allow subgroup analyses.
I (intervention): PRP treatment (injection during surgery or postoperatively), without restrictions to the dose, frequency, or treatment duration. PRP therapy was defined as any PRP injection administered intraoperatively or postoperatively, without restrictions on dose, frequency, or preparation method. Most included studies used preparations consistent with pure PRP (P-PRP), but specific classification (eg, leukocyte content) was not reported in the majority of trials. Postoperative rehabilitation protocols were accepted as long as they were applied equally to intervention and control groups.
C (control): Including placebo, no additional treatment.
O (outcome): The primary outcomes were knee pain measured by the visual analog scale (VAS) and knee function assessed using the Lysholm score and Knee injury and Osteoarthritis Outcome Score (KOOS). The Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) was included as a supplementary functional outcome, reported in a limited number of studies, and primarily used for elderly patients or those with concurrent degenerative changes. The Lysholm score is a patient-reported outcome measure used to assess knee function. It evaluates aspects such as pain, instability, and the ability to perform daily activities, with higher scores indicating better knee function. 21 The WOMAC measures pain, stiffness, and physical function, with a lower score indicating better knee function. 43 The KOOS evaluates knee function across 5 domains—Pain, Symptoms, Activities of Daily Living, Sport and Recreation, and Quality of Life—making it suitable for both knee injuries and osteoarthritis. A higher KOOS indicates a better knee function. 43 The secondary outcomes are the rate of treatment failure and the incidence of complications. Typically, treatment failure was defined as the unhealed meniscal tear that needed additional interventions after surgical repair as detected by MRI or during the second-look arthroscopy. Any complications that may potentially be related to the treatment were recorded, such as knee hematoma, infection, and the incidence of deep vein thrombosis, and so forth.
S (study design): RCT.
Excluded from the analysis were reviews, editorials, meta-analyses, preclinical studies, studies not designed as RCTs, studies involving pediatric patients, studies without the intervention of PRP, or studies that did not report the outcomes of interest. If studies with overlapped patients were retrieved, the one with the largest sample size was analyzed in the meta-analysis.
Database Search
The Medline (PubMed), Embase (Ovid), and CENTER (Cochrane Library), Web of Science, Wanfang, and CNKI (China National Knowledge Infrastructure) databases were searched using the combination of the following terms: (1) “platelet-rich plasma” OR “platelet rich plasma” OR “PRP”; (2) “meniscus” OR “menisci” OR “meniscal”; and (3) “random” OR “randomly” OR “randomized” OR “randomized” OR “placebo” OR “allocated” OR “control,” limited to clinical studies in human. Only studies that included human participants and were published as full-length articles in peer-reviewed journals were considered. We included studies published in English or Chinese. The full search strategy for each database is shown in the Appendix. Additionally, references to related reviews and original articles were screened as part of the final database search. The final database search was conducted on August 31, 2024.
Data Collection and Quality Evaluation
Two authors (J.L. and M.T.) conducted independent database searches, data collection, and quality assessment. No automated tools were used for data extraction. Two reviewers (J.L. and H.L.) independently extracted the data using a standardized Excel spreadsheet developed for this review, and discrepancies were resolved through discussion or consultation with a third reviewer. The data collected encompassed various aspects, including overall study information (such as first author, publication year, and study country), study design (double-blind, single-blind, or open-label), patient characteristics (diagnosis, number of patients, mean age, and sex), if patients with knee OA were included, concurrent treatment (arthroscopic surgery, rehabilitation, or other treatments), PRP preparation and administration (timing, frequency, and times of injections), controls (placebo or no additional treatment), follow-up durations, and outcomes reported.
The quality of the included RCTs was assessed using the Cochrane risk-of-bias tool. 15 This tool evaluated various aspects such as random-sequence generation, allocation concealment, blinding of participants and outcome assessment, addressing of incomplete outcome data, selective reporting, and other sources of bias.
Statistical Analysis
The influences of PRP on VAS for pain, Lysholm score, WOMAC, and KOOS were summarized as mean difference (MD) and corresponding 95% CI. 15 The influences of PRP on the rate of treatment failure and the incidence of complication were presented as odds ratio (OR) and corresponding 95% CI. 15 Heterogeneity was assessed using the Cochrane Q test. 15 The I2 statistic was also calculated, with I2 > 50% indicating significant statistical heterogeneity. 16 A random-effects model was used to pool the results because this model could incorporate the potential influence of heterogeneity. 15 For the primary outcome, subgroup analyses were also conducted to evaluate the study characteristics on the outcomes by comparing the efficacy of PRP in patients with or without concurrent knee OA, in studies with single or multiple injections of PRP, and in studies with the follow-up duration of <12 or ≥12 months. A sensitivity analysis limited to studies of patients with concurrent arthroscopic surgery was also performed. An evaluation of the publication bias was conducted via a visual inspection using funnel plots and by performing the Egger regression asymmetry test. 9 A P < .05 was considered statistically significant. Statistical analyses were conducted using RevMan (Version 5.1; Cochrane) and Stata software (Version 17.0; Stata Corporation).
Results
Literature Search
Figure 1 depicts the flowchart that outlines the process of database searching and study identification, ultimately leading to the selection of studies for inclusion. Initially, a total of 336 articles were obtained through the database search, which was subsequently reduced to 234 after eliminating duplicate records. A total of 199 articles were excluded based on an evaluation of their title and abstract, primarily because of their lack of relevance to the objective of the present meta-analysis. Then, 17 out of the remaining 35 articles were excluded after full-text review for reasons outlined in Figure 1. Ultimately, 18 RCTs # were deemed suitable for quantitative analysis.
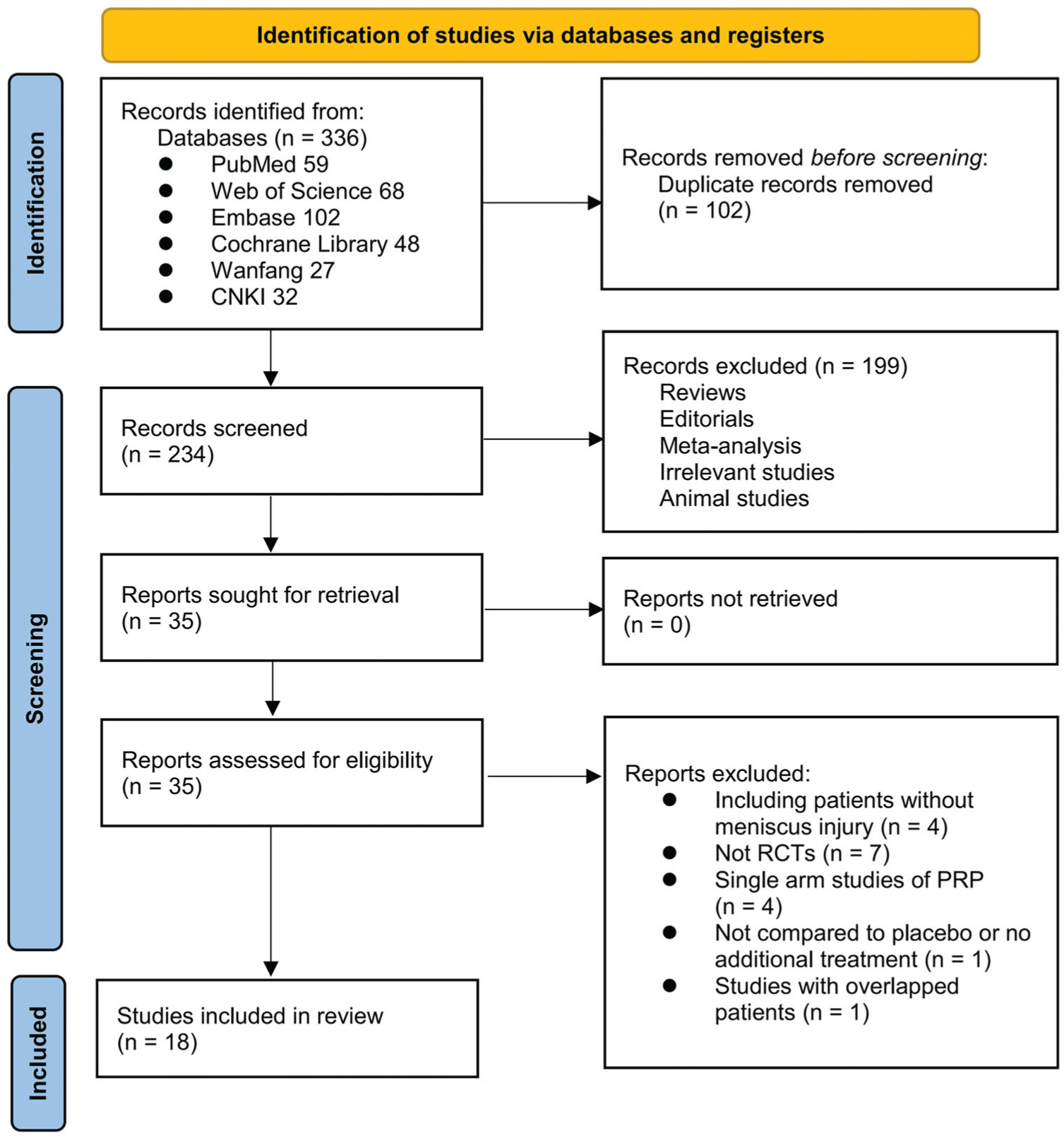
Flowchart of database search and study identification. None of the included studies was conducted in the United States; hence, none was performed under Food and Drug Administration oversight. PRP, platelet-rich plasma; RCT, randomized controlled trial.
Study Characteristics and Data Quality
An overview of the included studies can be found in Table 1. These studies were performed in China, Poland, Egypt, and Iraq and were published between 2015 and 2024. It is worth noting that all included RCTs were conducted outside the United States and thus were not subject to US Food and Drug Administration (FDA) regulatory oversight. All of the studies enrolled patients with meniscal injury, with1,18,25,29,49,50 and without ** knee OA. The sample size of the included studies was 26 to 130, and a total of 1143 patients with meniscal injury were included in the meta-analysis. The mean ages of the patients were 21.6 to 70.3 years. In 16 †† of the 18 included studies, all patients received arthroscopic meniscal repair surgery, while not for the other 2 studies.18,20 Autologous PRP was all used, which was injected into the repair site during or after the arthroscopic meniscal repair surgery. Single-time injection of PRP was performed as intervention in 12 studies, ‡‡ while multiple injections of PRP (2-6 times) was performed in the other 5 studies.1,11,42,45,46,53 Placebo was injected as control in 1 study, 19 while in the other studies, no additional treatment was used in the control group. The follow-up duration was 3 to 42 months after treatment. Outcome of knee pain was observed in 12 studies, §§ and the outcome of the Lysholm, WOMAC, and KOOS scores were reported in 12, ‖‖ 8,1,18-20,25,40,42,50 and 511,19,20,27,50 studies, respectively. Three studies14,19,20 reported the outcome of treatment failure, and 4 studies1,46,49,50 reported the incidence of complications. The details of study quality evaluation for the RCTs are shown in Table 2. Four studies were double-blind,11,19,20,27 1 was single-blind, 18 and another 13 studies were open-label. ¶¶ Fifteen studies reported the details of random sequence generation, ## while only 2 studies19,20 reported allocation concealment. No bias related to incomplete outcome data or selective reporting was suspected.
Characteristics of Included RCTs a

DB, double-blind; KOA, knee osteoarthritis; KOOS, Knee injury and Osteoarthritis Outcome Score; MRI, magnetic resonance imaging; NR, not reported; OL, open-label; PC, placebo controlled; PRP, platelet-rich plasma; R, randomized; RCT, randomized controlled trial; SB, single-blind; VAS, visual analog scale; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Study Quality Evaluation via the Cochrane Risk-of-Bias Tool

Influence of PRP on Knee Pain
Pooled results of 12 studies a showed that compared with control, PRP injection significantly reduced the knee pain of patients with meniscal injury as evaluated by the VAS (MD, –0.73; 95% CI, −0.91 to −0.55; P < .00001; I2 = 68%) (Figure 2). Further subgroup analyses showed similar results in patients with or without concurrent knee OA (subgroup difference, P = .07) (Appendix Figure A1A), in studies with single or multiple injection of PRP (subgroup difference, P = .51) (Appendix Figure A1B), and in studies with follow-up duration of <12 or ≥12 months (subgroup difference, P = .20) (Appendix Figure A1C). The sensitivity analysis limited to studies of patients with concurrent arthroscopic surgery showed consistent results (MD, −0.69; 95% CI, −0.88 to −0.50; P < .001; I2 = 67%).

Forest plots for the meta-analysis evaluating the influence of platelet-rich plasma (PRP) on visual analog scale–evaluated knee pain in patients with meniscal injury.
Influence of PRP on Knee Function
Further meta-analyses with 12, b 8,1,18-20,25,40,42,50 and 511,19,20,27,50 studies showed that PRP significantly improved knee function of patients with meniscal injury as compared with controls, as evidenced by a higher Lysholm score (MD, 6.77; 95% CI, 5.35 to 8.20; P < .00001; I2 = 46%) (Figure 3A), a lower WOMAC (MD, −5.33; 95% CI, −8.10 to −2.56; P = .0002; I2 = 80%) (Figure 3B), and a higher KOOS (MD, 4.34; 95% CI, 1.35 to 7.32; P = .004; I2 = 72%) (Figure 3C). Further subgroup analyses showed similar results between patients with or without concurrent knee OA, in studies with single or multiple injection of PRP, and in studies with follow-up duration of <12 or ≥12 months (subgroup difference, all P > .05) (Appendix Figures A2, A3, and A4). For the outcome of the Lysholm score, all the involved studies included patients with concurrent arthroscopic surgery. c In addition, the sensitivity analyses limited to studies of patients with concurrent arthroscopic surgery showed consistent results of the WOMAC (MD, −5.64; 95% CI, −8.75 to −2.53; P < .001; I2 = 82%) and KOOS (MD, 3.53; 95% CI, 0.59 to 6.46; P = .02; I2 = 70%).

Forest plots for the meta-analysis evaluating the influence of platelet-rich plasma (PRP) on knee function in patients with meniscal injury. (A) Knee function as evaluated by the Lysholm score. (B) Knee function as evaluated by the Western Ontario and McMaster Universities Osteoarthritis Index score. (C) Knee function as evaluated by the total Knee injury and Osteoarthritis Outcome Score. IV, inverse variance.
Influence of PRP on Rate of Treatment Failure and Incidence of Complications
Finally, pooled results of 3 studies4,19,20 suggested that PRP significantly reduced the treatment failure rate (OR, 0.26; 95% CI, 0.12 to 0.59; P = .001; I2 = 0%) (Figure 4A) for patients with meniscal injury. Meta-analysis of 4 studies1,46,49,50 showed that the incidence of complications was not statistically different between patients in the PRP and control groups (OR, 0.47; 95% CI, 0.21 to 1.03; P = .06; I2 = 0%) (Figure 4B).
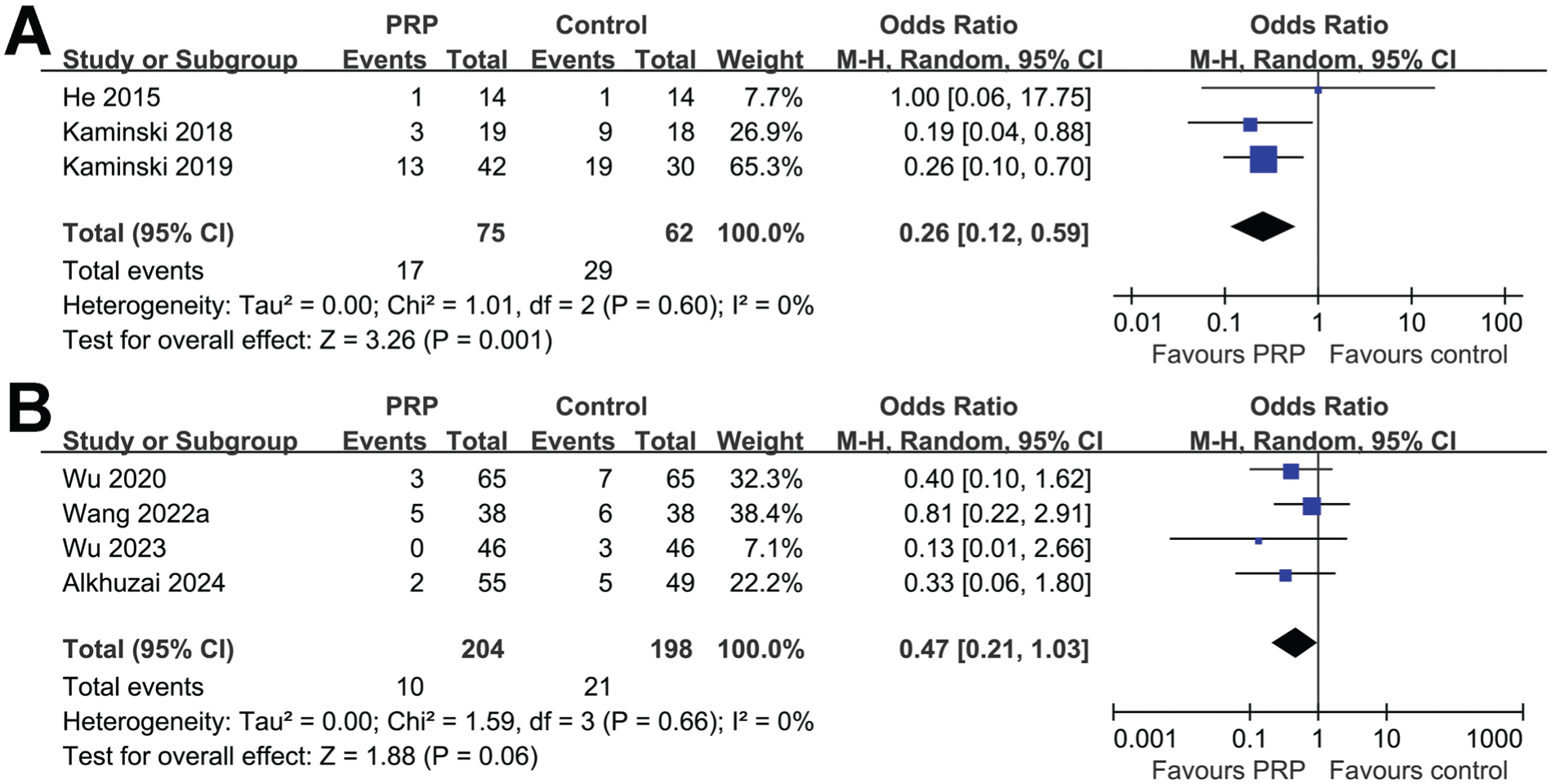
Forest plots for the meta-analysis evaluating the influence of platelet-rich plasma (PRP) on the treatment failure rate and the incidence of complications in patients with meniscal injury. (A) Treatment failure rate. (B) Incidence of complications. M-H, Mantel-Haenszel.
Publication Bias
The funnel plots for the meta-analyses of the influences of PRP on VAS evaluated knee pain and the Lysholm, WOMAC, and KOOS scores of patients with meniscal injury are shown in Figure 5. These plots are symmetrical on visual inspection, suggesting a low risk of publication bias. The Egger regression tests for the outcome of the VAS and Lysholm score also suggested a low risk of publication bias (P = .38 and 0.35, respectively). The Egger regression tests for the outcome of WOMAC and KOOS were not performed because <10 studies were included. The publication biases underlying the outcomes of treatment failure rate and the incidence of complications were unable to determine because only 3 and 4 studies, respectively, were included.

Funnel plots for the meta-analyses. (A) Funnel plots for the meta-analysis evaluating the influence of platelet-rich plasma (PRP) on visual analog scale–evaluated knee pain. (B) Funnel plots for the meta-analysis evaluating the influence of PRP on knee function as evaluated by the Lysholm score. (C) Funnel plots for the meta-analysis evaluating the influence of PRP on knee function as evaluated by the Western Ontario and McMaster Universities Osteoarthritis Index score. (D) Funnel plots for the meta-analysis evaluating the influence of PRP on knee function as evaluated by the total Knee injury and Osteoarthritis Outcome Score. MD, mean difference.
Discussion
The results of our meta-analysis demonstrate that PRP significantly reduces knee pain and improves function in patients with meniscal injury. PRP was found to be superior to control treatments across various clinical outcomes, including the VAS for pain, the Lysholm score, the WOMAC, and the KOOS. Additionally, PRP reduced treatment failure rates and did not result in a higher incidence of complications compared with control groups, further supporting its safety profile. These findings suggest potential benefits of PRP in managing meniscal injuries, although limitations in study quality and lack of placebo controls in most trials warrant cautious interpretation.
The mechanisms underlying PRP’s positive effects on meniscal injury likely involve its high concentration of platelets and growth factors, which promote tissue repair and reduce inflammation. 10 Indeed, a previous study utilizing a rabbit model showed that PRP treatment of meniscal injuries increases catabolic molecules and promotes fibrosis rather than meniscal cartilage regeneration, particularly in inflammatory conditions. 23 Growth factors such as platelet-derived growth factor, transforming growth factor beta, and vascular endothelial growth factor are key players in this process, enhancing cellular proliferation, matrix synthesis, and angiogenesis. 44 PRP may also modulate inflammatory pathways by suppressing proinflammatory cytokines and upregulating anti-inflammatory mediators, thereby creating an environment that facilitates healing. 17 Additionally, the ability of PRP to enhance collagen production may contribute to the structural integrity of the meniscus, promoting recovery from injury. 2 The key molecular mechanisms underlying the benefits of PRP for meniscal injury remain to be determined in the future.
Our subgroup analyses offer further insights into the efficacy of PRP under various conditions. We observed that the benefits of PRP were consistent across patients with and without concurrent knee OA, suggesting that PRP can be effective regardless of the degenerative state of the joint. This is important because injection of PRP has been confirmed to be effective for reducing pain and improving knee function in patients with knee OA, 34 which may confound its efficacy of meniscal injury. Moreover, this finding is particularly relevant given the high prevalence of OA in patients with meniscal tears, highlighting PRP as a viable option for a broader patient population. Similarly, the benefits of PRP were observed whether single or multiple injections were administered, although some studies suggest that multiple injections may enhance outcomes because of sustained delivery of bioactive factors. Moreover, the efficacy of PRP was evident in both short-term (<12 months) and long-term (≥12 months) follow-up, indicating that the therapeutic effects are durable over time.
Strengths and Limitations
The strengths of the meta-analysis include an extensive literature search across 6 English and Chinese databases, the inclusion of RCTs only to minimize bias from observational designs, and the conduct of multiple subgroup analyses to validate findings. However, the lack of placebo controls in nearly all included studies may still introduce performance bias. In addition, our meta-analysis has some other limitations. First, although etiology of meniscal injury and patient activity level may influence treatment outcomes, most included studies did not distinguish between traumatic and degenerative tears or classify participants by athletic status. As such, subgroup analyses by these variables were not possible. This clinical heterogeneity should be taken into account when interpreting our findings, which aim to provide a comprehensive overview of PRP efficacy across diverse patient populations. In addition, the lack of standardized classification of PRP preparations (eg, P-PRP vs Leukocyte-rich Platelet-Rich Plasma) across studies limited our ability to perform subgroup analyses by PRP type. Most studies appeared to use P-PRP, but leukocyte content and activation protocols were often not reported. Additionally, while all studies applied rehabilitation protocols, detailed descriptions were often missing, and variation across protocols may have influenced functional outcomes. However, most trials applied similar rehabilitation strategies to both study arms, reducing the likelihood of major bias. Moreover, variations in platelet concentration, the presence or absence of leukocytes, and activation methods may contribute to differences in treatment efficacy. 12 However, to the best of our knowledge, a standardized protocol for preparing autologous PRP remains to be determined. Standardization of PRP preparation protocols is needed to ensure consistency and reproducibility of results. As for the outcome, although the WOMAC score is more commonly used in osteoarthritis research, a few included studies applied this scale in older adults with meniscal injuries, possibly because of overlapping degenerative changes. In this meta-analysis, WOMAC was used as a supplementary outcome and was not central to our primary functional evaluation, which relied on meniscus-relevant scales such as Lysholm and KOOS. Furthermore, although the number of included RCTs was adequate, the sample sizes of some individual studies were small, potentially limiting the generalizability of our findings. Larger RCTs with more uniform methodologies are necessary to confirm the observed benefits of PRP in meniscal injuries. Another limitation is the relatively low quality of the included studies. Thirteen of the 18 studies were open-label, and only 1 of the included studies was placebo controlled. Therefore, the results should be validated in large-scale, high-quality RCTs.
From a clinical perspective, PRP represents a nonsurgical option for the treatment of meniscal injuries, offering a potential alternative to traditional therapies such as surgery or nonoperative management with physical therapy. Given the growing interest in biologic therapies, PRP could play an important role in the management of meniscal tears, particularly for patients seeking less invasive treatment options. Moreover, the low risk of complications observed in our analysis supports the safety of PRP, making it a viable treatment choice for a wide range of patients, including those with comorbidities or contraindications to surgery. Future research should focus on addressing the limitations of current studies and further exploring the role of PRP in meniscal injury treatment. In particular, well-designed, large-scale RCTs with standardized PRP protocols are needed to confirm the efficacy and safety of this treatment. Additionally, studies should investigate the long-term effects of PRP on meniscal healing and knee function, as well as its potential to delay or prevent the progression of OA in patients with meniscal injuries. Furthermore, the exploration of molecular mechanisms and signaling pathways involved in PRP-mediated tissue repair could provide deeper insights into optimizing its therapeutic potential. It should be noted that although PRP therapy has shown promising results in improving meniscal healing and knee function, its use for meniscal injuries remains an off-label indication according to the FDA. Clinicians using PRP in this context must ensure informed consent is obtained, explaining the investigational nature of the treatment, its potential benefits, and uncertainties regarding long-term safety and efficacy. Further regulatory guidance and high-quality RCTs are needed to establish standardized protocols and broaden the approved clinical applications of PRP. Additionally, there is currently no specific Current Procedural Terminology code approved for PRP injection in the treatment of meniscal injuries. This coding gap contributes to a lack of reimbursement by many insurance providers, potentially limiting patient access to PRP therapy despite emerging evidence of benefit. These financial and policy considerations should be taken into account when discussing PRP as a treatment option.
Conclusion
In conclusion, this meta-analysis provides pilot evidence that PRP may be an effective and safe treatment for meniscal injuries. PRP significantly reduces pain, improves knee function, and lowers the risk of treatment failure, with benefits observed across different patient populations and treatment protocols. Despite some limitations, these findings highlight the potential of PRP as a nonsurgical option for meniscal injury management, and future research will be key to refining its use and maximizing its clinical benefits.
Footnotes
Appendix
Final revision submitted May 27, 2025; accepted June 8, 2025.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.